
Abstract
Background:
Since the onset of coronavirus disease 2019 (COVID-19) in the world, healthcare workers have been exposed to this virus due to their important roles and responsibilities in the care and treatment of patients with COVID-19. In this regard, doing risk assessments in healthcare centres helps significantly to control and reduce COVID-19. Therefore, this study aimed to assess COVID-19 risk and its association with clinical symptoms among healthcare workers in Neyshabur.
Methods:
This cross-sectional study was conducted among 483 healthcare workers of Neyshabur medical centres in 2020. In order to collect the data, a checklist consisting of three sections of demographic variables, risk assessment and clinical symptoms was used. Statistical analyses were performed by using the STATA software version 14. The significance level was set at P<0.05.
Results:
The mean ± standard deviation age of the study population was 34.2 ± 8.4 years. Out of 483 participants, 55 (11.4%) were identified as high-risk exposure category, 52 (10.8%) as medium-risk category and 77 (15.9%) as low-risk category. According to multiple logistic regression models, it was observed that cough (odds ratio (OR)=2.2; P=0.001), running nose (OR=3.3; P<0.001), suffocation (OR=3.2; P<0.001), shivering (OR=3.4; P=0.001), nausea (OR=3.3; P=0.001), vomiting (OR=7.2; P=0.025), diarrhoea (OR=3.0; P=0.001), muscular pain (OR=2.1; P=0.005), joint pain (OR=2.2; P=0.005) and fatigue (OR=2.1; P=0.003) were significantly associated with risk assessment.
Conclusions:
The findings showed that more than one-fifth of studied healthcare workers were at high or medium-risk exposure of COVID-19. Cough and fatigue had the most frequencies in healthcare workers with high or medium-risk exposure, and also, vomiting and shivering had a stronger association with risk assessment status.
Introduction
Coronavirus disease 2019 (COVID-19) was first identified following cluster reports of viral pneumonia in Wuhan City, Hubei Province, China. On 30 January 2020, the World Health Organization (WHO) declared the COVID-19 outbreak a global health emergency and announced that as a pandemic in early March.1, 2 The COVID-19-related diseases have ranged from a mild illness such as a common cold to severe respiratory problems. 3 An increasing number of studies have reported that the clinical characteristics of infected patients at the onset of illness were fever, cough, fatigue, myalgia, diarrhoea, headache, vomiting and shortness of breath. In some cases, the infected patients have suffered from the severe respiratory syndrome, and pneumonia caused the death.4–8 According to the Centers for Disease Control and Prevention (CDC), the risk of severe disease with COVID-19 increases with age, thus older people, especially those with a weak immune system and some underlying conditions, have a greater chance of experiencing infection with COVID-19 and severe symptoms. 9 Even so, people of any age may be more prone to COVID-19 through close contact with an infected person. 10 Until now, several outbreak investigation reports11–14 have documented that not only the general community increases the risk of contracting and spreading the new respiratory pandemic, but healthcare workers (HCWs) have the potential for direct and indirect exposure to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and can have an important role in hospital transmission because of the nature of their work.15, 16 HCWs have been continuously on the frontline of medical emergencies, treatments and intensive care, and in the provision of care for COVID-19 patients. Earlier studies have shown that a large number of frontline medical workers were at direct risk of contracting the infection and died by the end of February 2020.17, 18 The greater risk observed among HCWs may reflect a higher infection rate due to work intensity, long-term exposure to large numbers of SARS-CoV-2-infected patients, insufficient rest and shortage of personal protective equipment (PPE).4, 8, 15, 19 This fact has been proved that transmission can be particularly effective in crowded medical wards, inadequately ventilated spaces, lack of a single and isolated room, and the pollution of the physical and consensual environment. 20
Devastating viral infection is known to have a major effect on HCWs. Therefore, considering that healthcare providers as a vulnerable population have helped to control the prevalence of viral diseases such as COVID-19, which is currently spread, they have to adopt the required biosafety measures strictly so as to stay safe from the disease and should be perceived as a discrete population. 19 Therefore, doing risk assessments in healthcare centres helps significantly to control and reduce viral infection such as COVID-19. 21 Given the high importance of this epidemic and its growing statistics in Iran, this study aimed to assess the risk of COVID-19 and its association with clinical symptoms among HCWs in Neyshabur in 2020.
Methods
Design and sample
This cross-sectional study was conducted among 483 HCWs that were selected via convenience sampling from Neyshabur medical centres (22 Bahman and Hakim hospitals) between February and April 2020. To calculate the sample size, the power of the study and the alpha level are considered to be 80% and 5%, respectively. The objective of the study was described to all participants and verbal consent was obtained from all of them to participate in the study.
Measures
Data collection was performed by using a three-part checklist. The first part of the checklist included demographic questions (age, gender, marital status, job category, job tenure, weight, height and current place of living). The second part included a checklist of COVID-19 risk assessments in HCWs. The risk assessment tool had nine questions that measured the healthcare providers’ exposure to patients with COVID-19 or their secretions/excretions in the healthcare setting over the past 14 days (Table 1). 22 After completed checklists by HCWs, risk assessment was done by an epidemiologist. HCWs, who were classified as high or medium-risk exposure category, were notified to perform a COVID-19 test (Table 1). The third part included a checklist of clinical symptoms (fever ⩾38°C, cough, running nose, suffocation, sore throat, shivering, nausea, vomiting, diarrhoea, muscular pain, joint pain and fatigue). The present study has been approved by the ethics committee of Neyshabur University of Medical Sciences, ethical code: IR.NUMS.REC.1398.037.
Items of risk assessment questionnaire.

The data obtained from the checklist were codified and entered into the statistical software package (STATA, version 14). Frequencies, percentages, ranges, means and standard deviations (SDs) were used as descriptive statistics. Two risk assessment categories were constructed: (a) high or medium-risk exposure category; (b) low or no identifiable risk exposure category. The chi-square test was used to investigate the relationship between clinical symptoms and risk assessment status. In order to establish whether there was a significant association between the clinical symptoms and risk assessment status after adjusting for covariates, a multiple logistic regression model was performed. The significance level was set at P<0.05.
Results
The participants’ demographic characteristics are presented in Table 2. The mean ± SD age of the study population was 34.2 ± 8.4 years (range 21–64) and 58% of them were men (Table 2). Among 483 participants, 11.39% were identified as high-risk exposure category (Table 3). The mean ± SD age of the population in the high-risk exposure category was 35.6 ± 9.7 years (range 23–61), and 54.6% of them were men. The characteristics of the study population across the risk exposure categories are presented in Table 3. The results of COVID-19 test showed that 22 (40%) and one (1.3%) of the participants in the high-risk and medium exposure categories had a positive test, respectively.
Characteristics of the study population, (n=483).
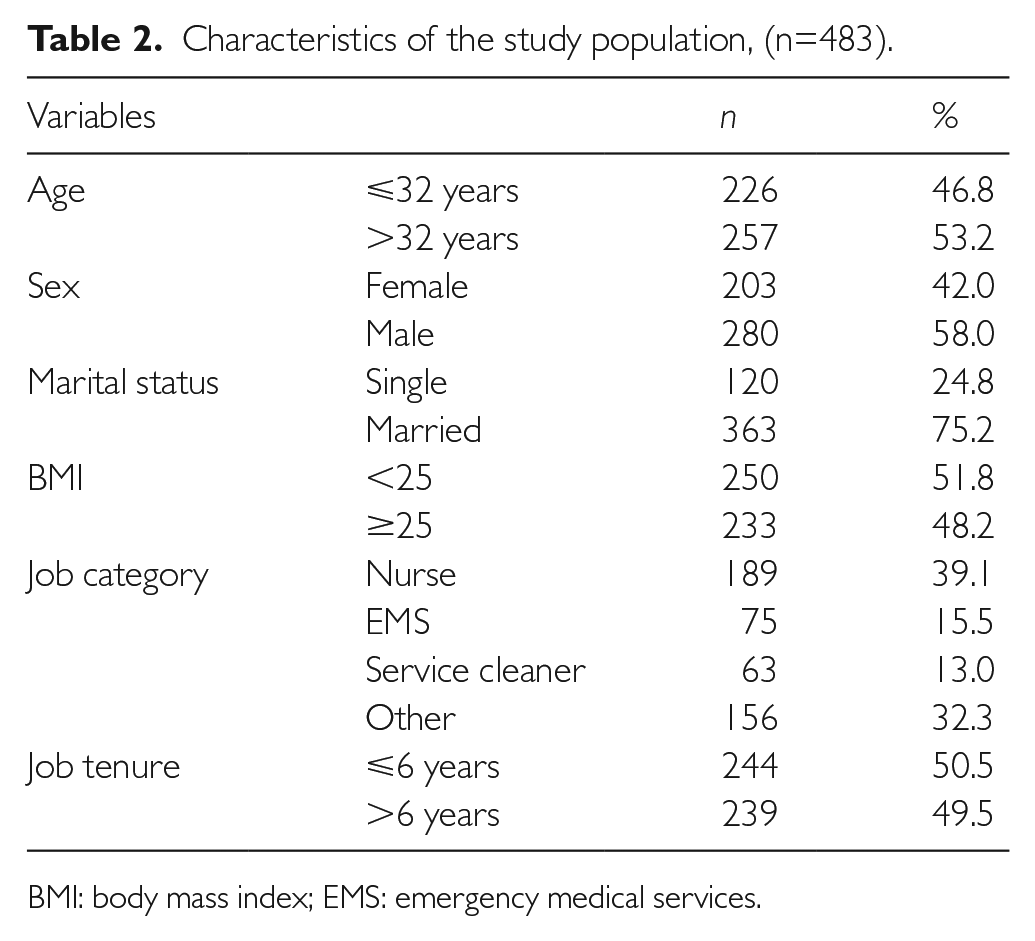
BMI: body mass index; EMS: emergency medical services.
Status of risk assessment based on demographic characteristics in participants.
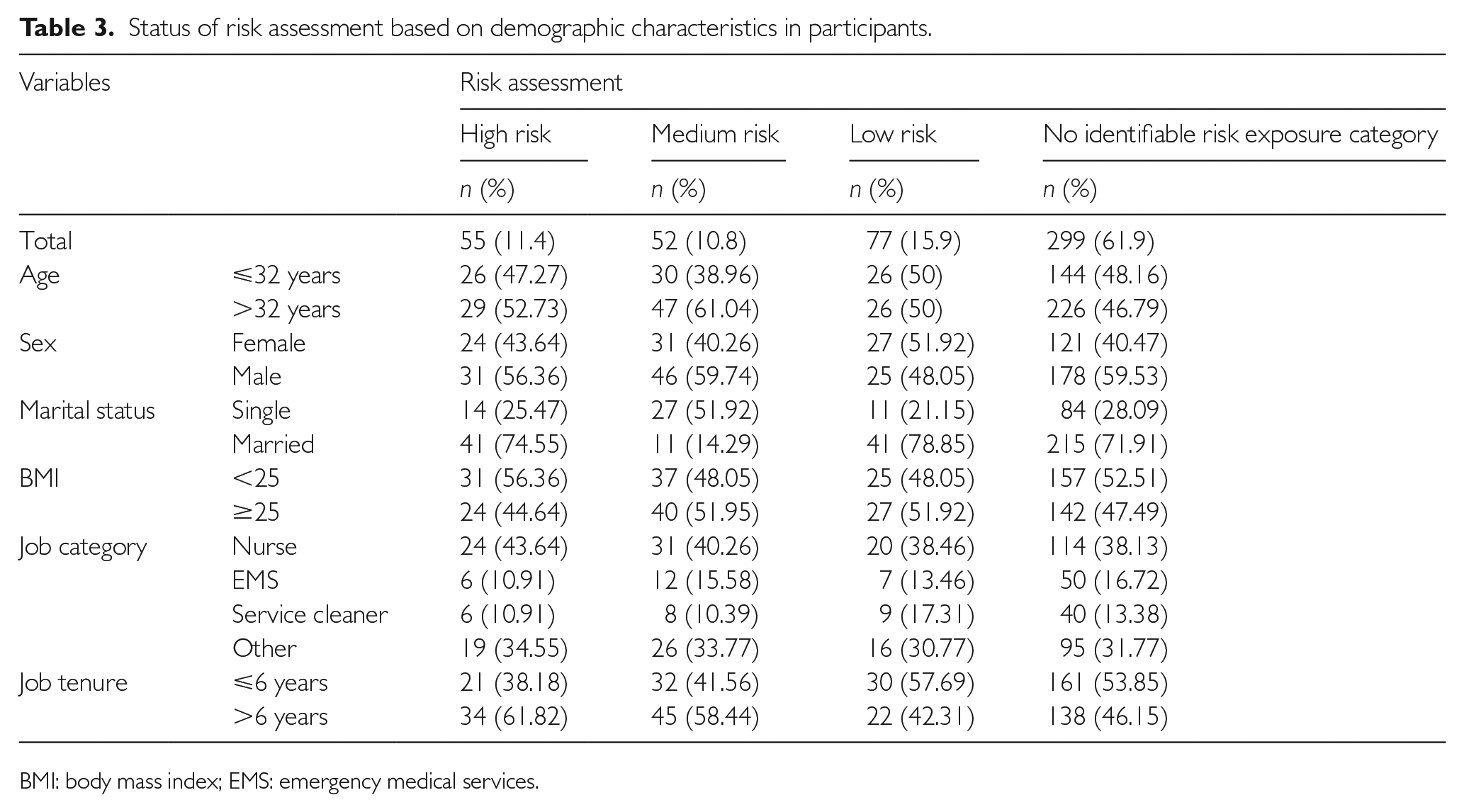
BMI: body mass index; EMS: emergency medical services.
We observed that cough and fatigue have the most frequencies among the different evaluated clinical symptoms. Table 4 summarises the results of the unadjusted association between risk assessment status (high or medium-risk exposure, low or no identifiable risk exposure) and clinical symptoms. A significant association was observed between risk assessment status and most of the clinical symptoms including cough, running nose, suffocation, shivering, nausea, vomiting, diarrhoea, muscular pain, joint pain and fatigue in the unadjusted analysis (Table 4). Table 4 displays the results of the adjusted association between risk assessment status and clinical symptoms based on the multiple logistic regression models. According to these models, when they were adjusted for other covariates, it was observed that cough, running nose, suffocation, shivering, nausea, vomiting, diarrhoea, muscular pain, joint pain and fatigue were significantly associated with risk assessment (Table 4). Based on Table 4, vomiting and shivering had a stronger association with the risk assessment status.
Unadjusted and adjusted relationship of clinical symptoms with risk assessment in study population.

OR: odds ratio; CI: confidence interval.
Adjusted for age, sex, marital status, body mass index, job category, and job tenure.
Discussion
The outbreak of coronavirus has posed a significant challenge for the workplaces and had several different physical and psychological effects on the workforces.23, 24 Because of the established continuous communication of employees in the high-risk work environments such as hospitals and medical centres with different people including colleagues and clients during the duration of work shifts, many people in these workplaces are at heightened risk of catching COVID-19. 25
With this subject in mind, we have attempted to assess the risk of the transmission of COVID-19 to HCWs who are working in medical centres. A checklist was prepared for subjects involving three sections to assess the health and safety risk faced by HCWs during the coronavirus pandemic. Among 483 HCWs, we identified 15.9% at low risk and 61.1% without risk exposure to COVID-19. Likewise, we found that the highest exposure (11.4%) occurred for HCWs who had a longer duration and intimacy of exposure to provide direct care for infected people. This finding is to some extent similar to that of Ashinyo et al., 26 in that 14% of the exposed HCWs were at high risk of COVID-19 virus infection. In addition, our study reported that the medium-risk category in the HCWs is also estimated at 10.8%. This supports our finding that HCWs have a considerably higher risk of COVID-19 infection. 13 The attention is intended to keep on analysing high and medium-risk exposures associated with COVID-19 in medical centres.
By carrying out the coronavirus tests, we found that 40% of HCWs who were categorised as high risk had a positive test for COVID-19. This finding is to some extent similar to that of Nguyen et al., 13 in which frontline HCWs had a high-risk magnitude (12–23.7%) during the early period of the COVID-19 pandemic. In line with findings by Lan et al. 27 and Chadeau-Hyam et al., 28 we revealed that the essential workers (including HCWs) involved in high-risk workplaces with significant direct exposure to patients have been at an increased risk of developing COVID-19 infections. Also, in a study by Sharma et al., 29 exposure to patients with COVID-19 (duration of exposure) resulted in a positive test for COVID-19. In this account, HCWs dealing with patients during an infectious period of disease by performing certain treatment procedures such as intubation and nebulisation were recognised as having a significant risk of infection.30–32 Hence, it may be concluded that due to the high contagiousness of the coronavirus, as well as the occupational fit in which treatment staff have close and long-term exposure to patients with coronavirus, a positive test is not unexpected.
In terms of signs and symptoms, we represented fatigue (37.7%), cough (36.5%) and running nose (32.7%) as the most frequent in high-risk and medium-risk categories. These values correlated reasonably well with the study of Lai et al., 33 in which infected HCWs presented with fever (60.91%). Our laboratory findings were consistent with previous studies including fever, cough, and fatigue. In a study by Liu et al., 34 it was shown that cough (83%), fever (76.7%) and fatigue (70%) were frequent symptoms which made patients seek care in a medical centre. Also, the results of the study by Huang et al. 35 pointed out fever (98%), cough (76%) and fatigue (44%) as the main complaints of patients with COVID-19. Despite this, the extent and severity of symptoms seem to vary depending on the length of exposure to the virus and the usage of PPE.13, 16
Meanwhile, it was interesting to find that our subjects have been shown to develop some atypical and less common symptoms affecting their digestive systems. We found that some patients experienced diarrhoea (16.8%), nausea (15.9%) and vomiting (3.7%).
A multiple logistic regression analysis was conducted to examine to what extent risk assessment predicts the clinical presentations. The evidence from this study implies that there is a significant relationship between risk assessment status and most of studied clinical symptoms (cough, running nose, suffocation, shivering, nausea, vomiting, diarrhoea, muscular pain, joint pain and fatigue), when adjusting for other covariates, whereas fever and sore throat presented a non-significant relationship with risk assessment status. Notably, in our study, we recorded that vomiting had a stronger association with risk assessment status (OR=7.2). Only a few studies have been conducted so far to assess how risk exposure is related to clinical symptoms. In agreement with our findings, Nguyen et al., 13 in a symptom-based study in which HCWs reported at least one clinical symptom and suggested a great association between the symptoms and risk exposure. Looking into the literature, it has now been suggested that among HCWs who reported being in close contact with a patient with confirmed COVID-19 in a medical setting, the risk of severe COVID-19 symptoms increased.36,37
Conclusions
The findings showed that more than one-fifth of studied HCWs were at high or medium-risk exposure of COVID-19. Cough and fatigue had the most frequencies in HCWs with high or medium-risk exposure and, also, vomiting and shivering had a stronger association with risk assessment status. Given that HCWs are one of the most important groups facing COVID-19, identifying and reducing the risk in HCWs by continuous training, using PPE properly can help to maintain HCWs immunity against infection.
Footnotes
Acknowledgements
The author(s) gratefully acknowledge the Neyshabur HCWs who willingly participated in this study.
Authors’ contributions
Ahmad Ghasemi, Ali Gholami and Hamid Abasi researched the literature and conceived the study. Seyed Morteza Shamshirgaran, Nayyereh Aminisani, Ensieyh Mollanoroozy, Masoud Mohammad Malekzadeh and Ali Gholami were involved in protocol development, gaining ethical approval and patient recruitment. Ali Gholami analysed the data. Hadi Fazel, Fatemeh Khorashadizade, Ghasem Moshar-Movahed, Amir Sadegh Alimardani, Ali Gholami and Hamid Abasi wrote the first draft of the paper. All authors reviewed and edited the paper and approved the final version of the paper.
Availability of data and materials
The datasets generated are available from the corresponding author.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The present study was approved by the ethics committee of the Neyshabur University of Medical Sciences (IR.NUMS.REC.1398.037).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Neyshabur University of Medical Sciences.
Informed consent
At the beginning of the study, the aims of the study were explained to the participants, and after obtaining informed consent, participants completed the self-report questionnaire.