
Abstract
Metabolic syndrome (MetS), a constellation of central obesity, hypertension, dyslipidaemia and glucose intolerance, is highly prevalent in individuals with schizophrenia and conveys significant cardiovascular risk and mortality. Associated risk factors are female sex, some ethnic groups, advanced age, long duration of illness, smoking and exposure to antipsychotic agents. The prevalence of MetS varies across countries and psychiatric populations, and its development can be very rapid. Regular monitoring of all features of MetS is the cornerstone of its early detection and management. Future research needs to focus more on genetic determinants of MetS in the context of schizophrenic illness. This review aims to update the reader with the latest knowledge about the prevalence of MetS in schizophrenia and what might be the underlying pathophysiological mechanisms.
Keywords
Metabolic syndrome: introduction
The metabolic syndrome (MetS, also known as syndrome X, syndrome of chronic cardiovascular disease and Reaven’s syndrome) is a constellation of different conditions, including abdominal obesity, insulin resistance, dyslipidaemia and elevated blood pressure. All components of the MetS (with obesity holding a central role in its development) have been recognized as independent risk factors for cardiovascular disease and so the presence of MetS is associated with other comorbidities such as the prothrombotic state, proinflammatory state, nonalcoholic fatty liver disease and reproductive disorders [Cornier et al. 2008]. Owing to its multiple components, many definitions have been given to MetS: by the World Health Organization (WHO) in 1985, by the European Group for the Study of Insulin Resistance in 1999, by the National Cholesterol Education Program’s Adult Treatment Panel III (NCEP-ATP III) in 2001 (modified in 2003), by the American Association of Clinical Endocrinologists in 2003 and finally by the International Diabetes Federation (IDF) in 2006 (Table 1). In an attempt to unify criteria of MetS proposed by various organizations, a joint statement of the IDF, the National Heart, Lung and Blood Institute, the American Heart Association, the World Heart Federation, the International Atherosclerosis Society and the International Association for the Study of Obesity suggested a revision of central obesity criteria to account for ethnic differences [Alberti et al. 2009]. According to the above, the diagnosis of MetS should be established if any three of the five criteria described below are present:
Elevated waist circumference, according to population- and country-specific definitions (usually high thresholds for North America and North Europe, moderate thresholds for Asia, the Middle East, the Mediterranean, Africa, Central and South America and low thresholds for China and Japan).
Elevated triglycerides (≥150 mg/dl) or drug treatment for dyslipidaemia.
Reduced high-density lipoprotein (HDL) (<40 mg/dl) or drug treatment for hypercholesterolaemia.
Elevated blood pressure (systolic ≥130 mmHg, diastolic ≥85 mmHg) or a history of hypertension or drug treatment for hypertension.
Elevated fasting glucose (≥100 mg/dl) or drug treatment for hyperglycaemia.
Criteria for the metabolic syndrome definition (adapted from Cornier et al. 2008, International Diabetes Federation, 2006).

AACE, American Association of Clinical Endocrinologists; BMI, body mass index; BP, blood pressure; EGIR, European Group for the Study of Insulin Resistance; HDL, high-density lipoprotein; IDF, International Diabetes Federation; NCEP ATP III, National Cholesterol Education Program Adult Treatment Panel III; WHO, World Health Organization.
The prevalence of MetS is increasing throughout the world but is partly dependent on the definition that is used to determine inclusion as well as the composition of the population being studied (i.e. sex, age, race and ethnicity) [Cornier et al. 2008]. Using the modified NCEP-ATP III criteria, the National Health and Nutrition Examination Survey (NHANES) compared data from a US cohort of 6423 adults (1988–1994) with a similar one of 6962 participants (1999–2006) and concluded that there has been an increase in age-adjusted MetS prevalence from 29.2% to 34.2% respectively over the years [Mozumdar and Liguori, 2011]. Efforts to control specific cardiovascular risk factors, such as blood pressure or total serum cholesterol levels, worldwide appear to have been partially effective since the 1980s (especially for countries with high income) [Danaei et al. 2011; Farzadfar et al. 2011]. Despite this, the mean body mass index (BMI) of the world’s population has shown a constant increase in the last three decades, both in developed and developing countries [Finucane et al. 2011]. Although this increase in BMI is likely to be a positive thing in developing countries, as it indicates that more people have better nutrition, in developed countries this is giving rise to the so-called ‘obesity epidemic’.
So it appears that MetS is common and increasing in the general population regardless of definition. Increased calorie intake and sedentary lifestyles have been implicated in the development of MetS worldwide, and without doubt constitutes a major public health risk. However, it is worth noting that certain population groups and more importantly certain patient groups have an even greater predisposition to developing MetS.
Metabolic parameters of schizophrenia
Schizophrenia is a highly heritable condition, which is associated with a dramatic reduction in lifespan; a meta-analysis of existing data has revealed a substantial gap between the health of people with schizophrenia and the general community [Saha et al. 2007]. Mortality in patients with schizophrenia is largely due to cardiovascular disease [Tandon et al. 2009]. Sudden cardiac death, often resulting from cardiac arrhythmias, is also an important cause of mortality [Koponen et al. 2008].
Schizophrenia has been associated with an increased risk of diabetes since the nineteenth century [Maudsley, 1979]. Henry Maudsley was one of the first psychiatrists to notice an association between diabetes and schizophrenia. This was prior to the development of antipsychotic treatments. Even today, a significant number of studies have demonstrated that antipsychotic naïve patients have impaired glucose tolerance, increased insulin resistance and increased visceral fat distribution compared with normal controls [Thakore et al. 2002; Venkatasubramanian et al. 2007; Fernandez-Egea et al. 2009]. More importantly, other studies have shown increased glucose intolerance in the siblings of people with schizophrenia and an increased prevalence of type II diabetes in the parents of subjects with nonaffective psychosis [Fernandez-Egea et al. 2008a, 2008b]. Recently, a Danish study found that having schizophrenia is associated with an at-risk allele for type II diabetes located in the TCF7L2 gene [Hansen et al. 2011]. These findings suggest that diabetes and schizophrenia may share familial risk factors or common genetic predisposition.
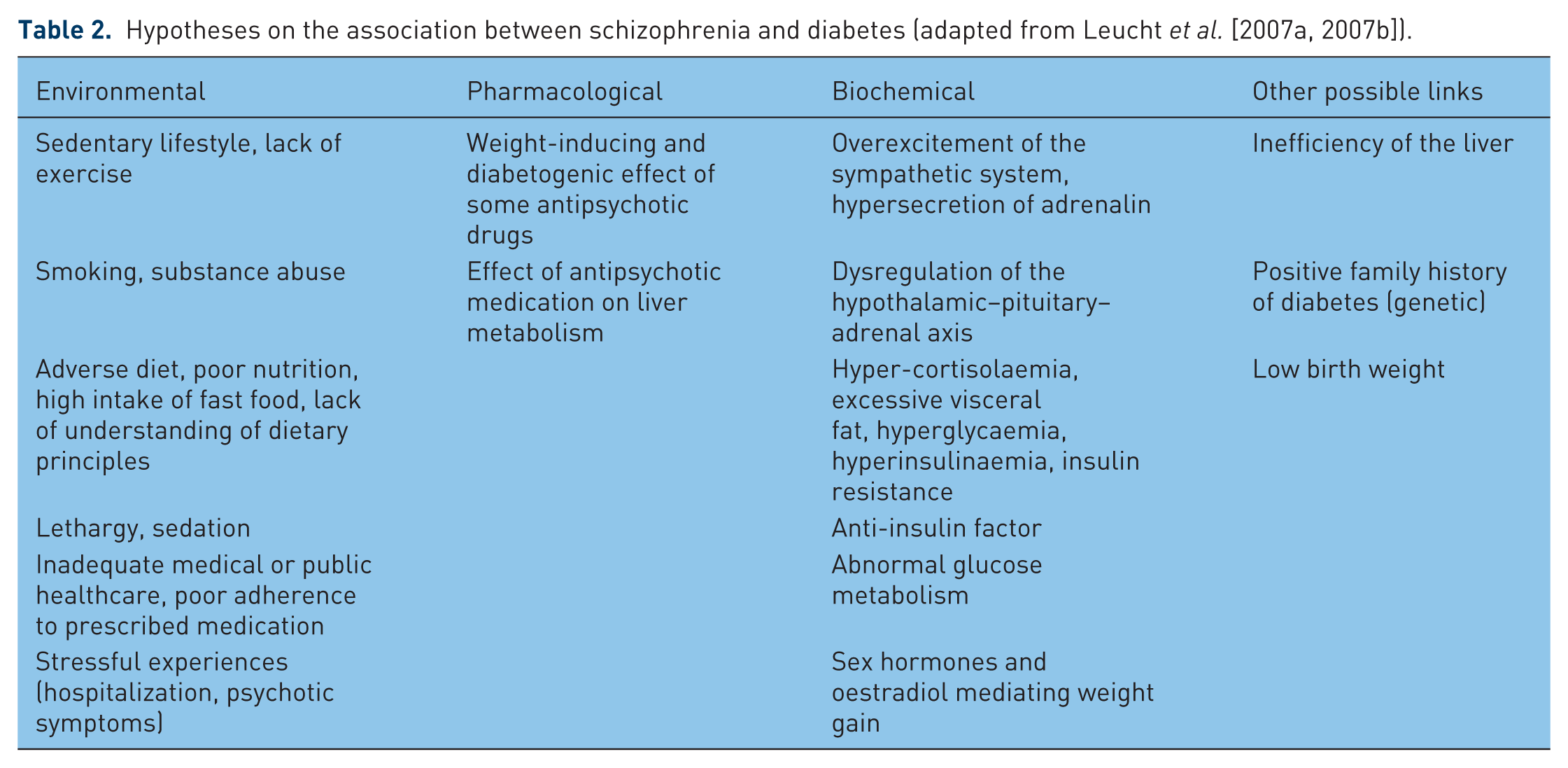
It has been estimated that in the USA as many as 60% of people with schizophrenia meet the criteria for MetS, as opposed to 30% for the general population [Mendelson, 2008]. Numerous studies have shown that overweight and diabetes are in general increased in people with schizophrenia, with a two- to fourfold increase in the risk of diabetes compared with the general population [Leucht et al. 2007a, 2007b]. This association, possibly predating the introduction of antipsychotic medication, has raised multiple hypotheses to account for the association between schizophrenia and diabetes by making reference to a number of intrinsic and extrinsic factors (Table 2).
Hypotheses on the association between schizophrenia and diabetes (adapted from Leucht et al. [2007a, 2007b]).
Rationale and objectives
In this review we provide an update about MetS in schizophrenia. We aim to present data from original studies, which consider the MetS as an entity using any of the established definitions.
We set the following objectives at the beginning of our review:
To provide a current estimate of the extent of MetS, with reference to its prevalence and incidence in populations of patients with schizophrenia.
To identify factors that are associated with the development and presence of MetS; these could be either related to the environment (health habits, use of antipsychotic medication) or to characteristics of the individual patients (sex, age and duration of illness).
Review methodology
Eligibility criteria
Eligibility criteria were original articles published in English language until 2011. Studies were included on the basis of making reference to any established definition of MetS and excluded if they only described individual features of MetS. We included studies that adopted an adequately robust design, either cohorts, case-control, cross-sectional or randomized controlled trials (RCTs).
Information sources
Information was obtained from the ISI Web of Knowledge platform (by Thomson Reuters), a comprehensive database that incorporates the Web of Science (1970 to present) and MEDLINE (1950 to present) and also includes articles from PsychINFO and the Cochrane Review Database.
Search
We searched articles using the terms: Title = (schizophrenia) AND Title = (metabolic syndrome), published until year 2011. Our initial search generated 119 hits. We completed our search by checking against previously published reviews and extracting additional articles (Table 3).
Published descriptive reviews of metabolic syndrome (MetS) in schizophrenia.

Study selection
Screening of articles was based on titles and abstract reading. Only articles fulfilling our eligibility criteria were included, and full texts were subsequently obtained. Special care was taken to avoid duplications and group together different articles describing the same study population.
Outcome
A total of 47 original studies were identified (Table 4).
Original observational studies on metabolic syndrome and schizophrenia.

FGA, first-generation antipsychotics (conventional or typical); IDF, International Diabetes Federation; MD, affective disorders (including bipolar disorder): MS, mood stabilizers; NCEP-ATP III, National Cholesterol Education Programme – Adult Treatment Panel III; NCEP-ATP III mod, modified National Cholesterol Education Programme criteria, fasting glucose reduced from over 110 mg/dl to over 100 mg/dl; PSYCH, other psychotic disorders; RCT, randomized controlled trial; SCZ, schizophrenia; SCZA, schizoaffective disorder, SGA, second-generation antipsychotics (atypical).
Several researchers have tried to summarize the current evidence on MetS in schizophrenia in numerous systematic or selective reviews. Most reviews focus on studies of epidemiological interest but also attempt to address the pathophysiological connections between MetS and schizophrenia. A group of reviews focus particularly on studies of metabolic features associated with the use of second-generation antipsychotics. A significant number of reviews that focus on behavioural and pharmacological interventions targeting metabolic disturbances in schizophrenia and severe mental illness are also available, but they are not mentioned here as they are beyond the scope of this article.
Description/discussion of studies
Observational studies on prevalence and incidence of MetS were conducted in several countries, and the most numerous publications come from the USA, followed by Belgium and Finland. The great majority of studies employed a cross-sectional design, and fewer were case-control and cohort studies. Only two RCTs were included, the first comparing the incidence of MetS among patients treated with aripiprazole versus olanzapine and placebo [L’Italien et al. 2007] and the second comparing prevalence rates of MetS developed following 6 weeks of treatment of young unmedicated drug-naïve patients with haloperidol, risperidone or olanzapine [Saddichha et al. 2008]. The composition of the study group varied, however male patients appeared to be over represented. In most studies the mean age of participants in the study group was over 40 years of age, and only a few studies referred to patients with first episode schizophrenia [Attux et al. 2007; Saddichha et al. 2007; De Hert et al. 2008b; Saddichha et al. 2008; Curtis et al. 2011]. The predominant diagnosis of patients studied was schizophrenia, however a great number of studies also included patients with schizoaffective disorder and other psychotic disorders. In almost all studies, patients were medicated with first- and second-generation antipsychotic drugs (FGAs, SGAs) and only one cross-sectional and two case-control studies referred to drug-naïve patients [Saddichha et al. 2007, 2008; Padmavati et al. 2010]. Most studies used the NCEP-ATP III definition while some studies also calculated MetS rates by using the IDF definition.
Overall prevalence rates
Prevalence rates varied largely across studies. This possibly reflected the epidemiological versatility of the groups of patients studied, and factors such as age, sex, ethnicity, medication status, smoking, duration of illness and country of origin affected the final outcome. The lowest prevalence rate reported was 3.9%, originating from an Indian population of 51 unmedicated, drug-naïve young outpatients (mean age 26.9) with chronic schizophrenia, and was based on the IDF definition of MetS [Padmavati et al. 2010]. The highest prevalence rate reported, 68%, derived from a study of 221 psychotic inpatients and outpatients (mean age 37.9) from a New Zealand rehabilitation setting, who were treated with a combination of FGAs and SGAs (authors used the IDF criteria) [Tirupati and Chua, 2007]. Those two studies clearly showed how MetS rates vary between two completely different populations of patients with psychosis, who can be placed at the extremes of a spectrum in terms of their epidemiological features and medication status.
When different criteria were used to calculate MetS in the same population, outcome rates also varied, with IDF criteria usually generating the highest rates and NCEP-ATP III modified criteria the lowest [McEvoy et al. 2005; Correll et al. 2006, 2008; De Hert et al. 2006a and 2006b, 2007; Meyer et al. 2006; Bobes et al. 2007; Cerit et al. 2008; Rejas et al. 2008; Saddichha et al. 2008; Rezaei et al. 2009; Sugawara et al. 2010; Yazici et al. 2011]. Those studies that also included a control group revealed that the rates of MetS in patients with schizophrenia were at least twice as high compared with the general population [Cohn et al. 2004; McEvoy et al. 2005; Saari et al. 2005; Lamberti et al. 2006; Mackin et al. 2007; Sugawara et al. 2010]. This effect was usually more prominent in younger age groups and tended to be attenuated or even reversed in older age groups [McEvoy et al. 2005; Lamberti et al. 2006; Sugawara et al. 2010; Yazici et al. 2011]. Only one study from India reported a higher prevalence rate in the general population compared with patients with schizophrenia [Padmavati et al. 2010].
Metabolic syndrome and sex
Numerous studies compared prevalence rates between men and women. Most studies revealed substantially increased prevalence rates of MetS in women [Cohn et al. 2004; Kato et al. 2004; McEvoy et al. 2005; Correll et al. 2006; De Hert et al. 2006b; Hagg et al. 2006; Lamberti et al. 2006; Meyer et al. 2006; Bobes et al. 2007; Teixeira and Rochal, 2007; Cerit et al. 2008; Rejas et al. 2008; Sicras-Mainar et al. 2008; Huang et al. 2009; Rezaei et al. 2009; Yazici et al. 2011], up to threefold compared with men [Rezaei et al. 2009]. Fewer studies reported a slight predominance of male sex in MetS rates or no significant differences in rates of MetS across sexes [Heiskanen et al. 2003; Basu et al. 2004; Tirupati and Chua, 2007; Correll et al. 2008; Koponen et al. 2010; Kraemer et al. 2010; Sugawara et al. 2010, 2011].
Metabolic syndrome and age
The prevalence of MetS increases with age in the general population and a similar trend was generally observed in patients with schizophrenia. Quite a few studies have included cluster analysis of age groups, and an association between rates of MetS and age of participants was usually demonstrated [Cohn et al. 2004; McEvoy et al. 2005; Hagg et al. 2006; Lamberti et al. 2006; Bobes et al. 2007; Suvisaari et al. 2007; Cerit et al. 2008; Rejas et al. 2008; Huang et al. 2009; Sugawara et al. 2010, 2011; Kang et al. 2011; Yazici et al. 2011]. The pattern of this association was not always clear and depends on the level of age clusters studied by researchers. Some studies though revealed a peak of MetS rates in the third, fourth or fifth decade of life with subsequent decline in MetS rates in later life [Hagg et al. 2006; Sugawara et al. 2010]. This effect was not consistent through all studies, and it was not present in the same way in both sexes. A single study showed that women with schizophrenia tended to reach a peak in MetS rates in the forth decade of life, while men reach a peak in the third decade [Sugawara et al. 2010]. This finding could also reflect the fact that men tend to have an earlier onset of schizophrenia than women and so are exposed longer to this condition. It is of interest though that when age-cluster analysis was applied to the same population, considering the type of psychiatric setting, more complex patterns were revealed. Both male and female inpatients showed a peak in MetS rates in their fourth decade of life with a further decline, while outpatients presented an atypical pattern of MetS prevalence changes, with men scoring higher in their third, fifth and seventh decades and women in their fourth and seventh decades [Sugawara et al. 2011]. However, one should be very cautious in trying to interpret the kind of data that stem from a single study.
Metabolic syndrome and medication
Only three studies included antipsychotic-naïve patients and reported rates of MetS lower than the rates described in the majority of studies. It is of note that two of these studies referred to drug-naïve patients who had been medicated for only 6 weeks with antipsychotic agents, and they developed MetS in response to this [Saddichha et al. 2007, 2008], and the third study referred to a very rare population of drug-naïve, unmedicated patients with an extremely low prevalence of MetS, as discussed above [Padmavati et al. 2010]. A German study explored the prevalence of MetS in patients with treated or untreated schizophrenia at baseline and at 3 months after initiation or switch of antipsychotic treatment. The authors reported an increase from 44.3% to 49.6%, and also described the lowest baseline MetS prevalence (24.7%) in previously unmedicated patients [Kraemer et al. 2011]. The lack of further studies on drug-naïve patients is an anticipated source of bias in any effort to explore the role of antipsychotic medication in the development of MetS. However, numerous studies attempted to compare various antipsychotics or groups of antipsychotics (FGAs versus SGAs) in terms of their contribution to MetS [Almeras et al. 2004; Kato et al. 2004; Straker et al. 2005; Correll et al. 2006, 2007; Hagg et al. 2006; L’Italien et al. 2007; Suvisaari et al. 2007; Tirupati et al. 2007; Cerit et al. 2008; De Hert et al. 2008b; Meyer et al. 2008; Saddichha et al. 2008; Huang et al. 2009; Rezaei et al. 2009; Schorr et al. 2009; Lee et al. 2011]. Consistent findings across these studies found that MetS was more likely with SGAs over FGAs, polypharmacy over monopharmacy and high-potency over low-potency agents. For individual antipsychotics, clozapine and olanzapine appeared to be related to higher MetS rates than other antipsychotic agents.
Metabolic syndrome and ethnicity
Very few studies attempted to address the issue of ethnicity when MetS rates are calculated [Basu et al. 2004; Kato et al. 2004; McEvoy et al. 2005; Straker et al. 2005; Correll et al. 2006; Lamberti et al. 2006]. Black African and Hispanic patients appeared to present with higher rates of MetS, however some studies found rates to be similar to white populations. However, outcomes appeared to be quite inconsistent. It is of note that despite Indian and Asian populations having a predisposition to develop diabetes, studies of patients with schizophrenia originating from these populations usually reported lower prevalence rates of MetS compared with white and black patients. Of course this observation can also reflect the lower rates of prescribing atypical antipsychotics in developing versus developed countries.
Metabolic syndrome and duration of pscyhotic illness or type of psychiatric setting
Only three studies were identified which looked at duration of psychotic illness in the calculation of MetS rates. One prospective cross-sectional study calculated MetS prevalence across four clusters of illness duration and demonstrated a clear association: the longer the participants had had psychosis, the higher the rates of MetS [De Hert et al. 2006a]. Two more studies (referring to the same population) failed to reveal an association between chronicity of illness and higher prevalence of MetS [Bobes et al. 2007; Rejas et al. 2008]. A recent study from Japan revealed substantial differences in rates of MeS between inpatients and outpatients with schizophrenia, with outpatients presenting with almost threefold the prevalence of MetS compared with inpatients (48.1% versus 15.8%). This remarkable difference possibly reflects the fact that schizophrenia inpatients in Japan typically have long hospital stays, during which they receive controlled diets and occupational therapy [Sugawara et al. 2011].
Metabolic syndrome and lifestyle habits
Though some studies described lifestyle characteristics of their population, only a few chose to describe how these reflected MetS rates. Only four studies distinguished between smokers and nonsmokers when MetS rates were calculated [Lamberti et al. 2006; Cerit et al. 2008; Rezaei et al. 2009; Schorr et al. 2009]. In three of these, smokers appeared to have higher rates of MetS compared with either nonsmokers or the whole study population, while only one study showed similar rates between the two groups [Cerit et al. 2008].
Incidence of metabolic syndrome
A minority of studies calculated incidence rates of MetS [Attux et al. 2007; L’Italien et al. 2007; Saddichha et al. 2007; Srisurapanont et al. 2007; De Hert et al. 2008b; Meyer et al. 2008; Kim et al. 2010; Kraemer et al. 2010]. The results were hardly comparable in this field as incidence rates were calculated for various time periods, from 6 weeks up to 1 year. One of these studies referred to a population of 30 young drug-naïve women who were medicated with an antipsychotic agent for 6 weeks, and provided MetS incidence estimates at the beginning and the end of the trial period (3.33–31.81%) [Saddichha et al. 2007]. This was a clear and rare example of how quickly and extensively MetS can develop as a response to antipsychotic administration in an otherwise healthy population.
Framingham 10-year risk
A few studies calculated Framingham 10-year cardiovascular risk rates for their patients [Cohn et al. 2004; Correll et al. 2006, 2008; Bobes et al. 2007; Rejas et al. 2008; Yazici et al. 2011]. When controls were also included, study populations scored substantially higher [Cohn et al. 2004]. Men scored higher than women in all studies that calculated rates according to sex. When cardiovascular risk rates were calculated for age clusters, the highest values were observed in the fifth and sixth decade of life.
Findings from other reviews
Our findings build on those from other reviews: first it is clear that there is an association between metabolic risk factors and antipsychotic use; second it seems that antipsychotic use alone is not sufficient to explain the increased metabolic risk seen in schizophrenia.
In a thorough systematic review of atypical antipsychotics and weight gain, Taylor and colleagues discussed a total of 74 papers (6 on amisulpride, 27 on clozapine, 8 on olanzapine, 7 on quetiapine, 13 on risperidone, 7 on sertindole, 3 on ziprasidone and 3 on zotepine) [Taylor and McAskill, 2000]. They concluded that with the exception of ziprasidone, all medications have been associated with weight gain; however aripiprazole was not included in this review.
Jin and colleagues reviewed studies on the effect of atypical antipsychotics (clozapine, risperidone, olanzapine, quetiapine, ziprasidone and aripiprazole) on glucose dysregulation [Jin et al. 2004]. They included four extensive case series and summaries, 13 epidemiological studies from prescription and drug safety monitoring databases and 10 clinical studies on glucose intolerance and atypical antipsychotics. Despite individual differences noted among various antipsychotics, they noted that patients with known risk factors for type II diabetes mellitus, such as ethnicity, first-degree family history of diabetes mellitus and baseline obesity, appear to be at increased risk for the development of glucose dysregulation during treatment.
Meyer and Koro reviewed 48 studies and focused on the effects of FGAs and SGAs on serum lipids [Meyer and Koro, 2004]. They stated that high-potency conventional antipsychotics (haloperidol) and some atypicals (ziprasidone, risperidone and aripiprazole) are associated with lower risk of dyslipidaemia, whilst low-potency conventional antipsychotics (chlorpromazine, thioridazine) and some other atypicals (quetiapine, olanzapine and clozapine) are related to higher risk of dyslipidaemia.
Newcomer, in a massive and comprehensive literature review, gathered data from more than 200 studies on the metabolic effects of atypical antipsychotics, with special focus on weight gain and glucose and lipid dysregulation [Newcomer, 2005]. He extensively discussed eight antipsychotic medications, specifically clozapine, olanzapine, risperidone, quetiapine, zotepine, amisulpride, ziprasidone and aripiprazole, and provided a detailed account of the metabolic profile of each. Clozapine and olanzapine were associated with the highest risk for causing clinically significant weight gain; risperidone, quetiapine, amisulpiride and zotepine a moderate risk; ziprasidone and aripiprazole a lower risk. He also noted that this ranking reflected the relative risk for insulin resistance, dyslipidaemia and hyperglycaemia.
In a systematic review and meta-analysis Smith and colleagues compared FGAs and SGAs with regards to their risk for type II diabetes mellitus [Smith et al. 2008]. The atypical antipsychotics included in this review (clozapine, olanzapine, risperidone and quetiapine) appeared to have a small increased risk only for development of diabetes compared with typical antipsychotics.
Simon and colleagues attempted to investigate whether weight gain and metabolic side effects of atypical antipsychotics are dose dependent in a systematic review of 45 original articles [Simon et al. 2009]. Among the medications included (clozapine, olanzapine, risperidone, quetiapine, ziprasidone, sertindole, amisulpiride and aripiprazole) a dose–response relationship between serum concentrations and metabolic outcomes was suggested only for clozapine and olanzapine, although the association between daily dose and metabolic measures was not clear.
Meyer and colleagues summarized the information available about MetS in patients with schizophrenia and proposed mechanisms for the increased prevalence of MetS in this population [Meyer et al. 2005a]. They suggested that the vulnerability to developing MetS among patients with schizophrenia derives from the concept that the phenotype of MetS resembles that of Cushing’s disease, and thus is related to an inherent dysregulation of the hypothalamo-pituitary-adrenal (HPA) axis.
Meyer and Stahl returned with a second review in which they focused on the prevalence of MetS in schizophrenia, presenting data from the latest studies [Meyer and Stahl, 2009]. They also attempted to address the great debate about whether the development of MetS is an environmental epiphenomenon related to health habits seen in schizophrenia, or a fundamental part of this disease. Special emphasis was placed on the importance of the fasting serum triglyceride to HDL ratio in predicting insulin resistance better than fasting serum glucose. The authors also discussed the issue of metabolic monitoring in patients with schizophrenia and made appropriate reference to a number of behavioural and pharmacological interventions. They concluded that because of lifestyle, disease and medication effects, patients with schizophrenia have significant risk for cardio-metabolic disease. They also recommended routine monitoring, preferential use of metabolically neutral antipsychotics, antidiabetic medication and lifestyle education as ways to minimize risk.
In a review of MetS and psychiatric illness, Mendelson emphasized the pathophysiological links between the development of MetS and the emergence of psychotic symptoms in schizophrenia by investigating the role of asymmetrical dimethylarginine (ADMA), homocysteine, s-adenosylmethionine (SAMe) and N-methyl-D-aspartate receptors (NMDAR) [Mendelson, 2008]. He highlighted the presence of increased levels of ADMA as a common feature between MetS and schizophrenia. ADMA is an endogenous inhibitor of nitric oxide, which is a major intracellular mediator of NMDAR activation. Thus ADMA might contribute to decreases in NMDAR activity that, in turn, may increase the psychotic symptoms in schizophrenia.
Lindley and colleagues provided a detailed account of the insulin-resistance syndrome in schizophrenia, referring to a number of endogenous and exogenous factors [Lindley et al. 2008]. They emphasized the strong links between insulin resistance and lifestyle characteristics (including weight, diet, exercise, energy expenditure) and discussed the role of stress and HPA axis dysregulation in antipsychotic-induced metabolic disturbances. They also noticed that significantly higher fasting glucose levels are observed in drug-naïve patients with schizophrenia, suggesting an integral role of insulin resistance in this disorder. Following this path of thought they introduced the hypothesis that insulin resistance shares genetic risk factors with schizophrenia and mood disorders.
Among the most comprehensive reviews is without doubt that of Leucht and colleagues [Leucht et al. 2007a, 2007b]. In their impressive work, the authors performed a pedantic review of 52 original articles since 1919, the majority of which describe individual features of MetS in patients with schizophrenia. This is definitely one of the most systematic attempts to present both the extent and the nature of this condition. The authors provided a detailed account of numerous estimations of the prevalence of MetS in schizophrenia, showing almost unanimously increased rates compared with the general population.
In a review, De Hert and colleagues summarized all estimates of the prevalence and incidence of MetS in schizophrenia from 2003 onwards [De Hert et al. 2009]. They also provided suggestions for screening and monitoring of MetS in patients with schizophrenia and emphasized the importance of a multidisciplinary assessment of psychiatric and physical conditions. The authors returned in 2012 with two more meta-analyses on metabolic and cardiovascular adverse effects associated with antipsychotic drugs [De Hert et al. 2012a, 2012b]. They concluded that the potential of SGAs to induce or trigger metabolic dysregulation, including type II diabetes mellitus and MetS, is firmly established. They ranked SGAs from high to low in terms of cardiovascular adverse effects as follows: clozapine = olanzapine > quetiapine ≥ risperidone = paliperidone > amisulpride > aripiprazole ≥ ziprasidone. They noted that, for the FGAs, the low-potency agents have the highest potential and the high-potency agents the lowest potential to induce metabolic dysfunction. The risk profiles of the FGAs are comparable to those of the high- and low-risk SGAs. They also recommended regular monitoring as part of the management of patients receiving antipsychotic drugs.
The most recent meta-analyses on this topic come from Mitchell and colleagues [Mitchell et al. 2011, 2012b]. The authors provided a very comprehensive review of prevalence and predictors of MetS in adults with schizophrenia and related disorders, accounting for subgroup differences. The overall rate of MetS was calculated at 32.5% and they were only minor differences according to different definitions, treatment setting, country of origin and no appreciable differences between men and women. Older age had a modest influence on the rate of MetS, while the duration of illness had the strongest influence. Waist circumference proved to be the most useful measure in predicting high rates of MetS. The highest rates of MetS were seen in those prescribed clozapine (51.9%) and the lowest rates in those who were unmedicated (20.2%).
There was a significantly lower cardiovascular risk in early compared with chronic schizophrenia. Diabetes and prediabetes appeared uncommon in the early stages, especially in unmedicated patients.
Overall all the reviews already published agree that MetS is increasingly present in patients with schizophrenia. Most authors emphasized the importance of extrinsic factors (antipsychotic medication, increased calorie intake, sedentary lifestyle) in its development, however the concept of intrinsic factors being implicated (genetic links between schizophrenia and diabetes) is also supported.
Discussion
Summarizing the findings
MetS is over represented in SMI, and patients with schizophrenia usually have a twofold (or more) risk of developing it compared with the general population. Its prevalence varies largely (3.9–68%) across various countries and studies: it is least likely in young, unmedicated, drug-naïve patients and most likely to be seen in chronically ill and long-term medicated patients. Women tend to present with increased rates of MetS compared with men, and some ethnic groups, such as black Africans and Hispanics show a possible predisposition to the condition. Prevalence of MetS in patients with schizophrenia generally increases with age, as in the general population, and the highest rates for Framingham 10-year cardiovascular risk are observed in men and in the fifth and sixth decades of life. It is of note that women tend to have higher rates of MetS and men higher rates of Framingham 10-year cardiovascular risk; at first glance, this looks like a paradoxical observation. However, we should consider that MetS reflects the current metabolic profile of an individual (based on a variety of physiological measures) while the Framingham 10-year risk describes the likelihood of a cardiovascular event in the future and is calculated by using metabolic measures (HDL, total cholesterol, systolic blood pressure) and epidemiological data (age, smoking status, treatment for hypertension) [D’Agostino et al. 2008]. So men are still at higher risk of developing cardiovascular disease (possibly due to a combination of unhealthy life habits, lack of medical input and abnormal metabolic status) while women show a higher point prevalence of MetS, which can reflect a gender-specific metabolic profile. SGAs, high-potency antipsychotic agents (both FGAs and SGAs) and polypharmacy are risk factors for the development of MetS. Other risk factors include the length of exposure to psychotic illness and lifestyle habits, such as smoking. The incidence of MetS in schizophrenia is hard to calculate but it can develop quickly, even within 6 weeks of starting antipsychotic medication.
Directions for future research: the genetics
In this review, we emphasized the importance of extrinsic factors in the development of MetS. However, we cannot remain oblivious to the large and growing amount of evidence suggesting that MetS also has a strong genetic component. Numerous genome wide association studies (GWAS) have identified various single nucleotide polymorphisms (SNPs) associated with the different components of MetS. These SNPs are usually found in the vicinity of genes that play various roles in one or more metabolic pathways. Relevant literature provides a wealth of evidence:
BMI: in a large GWAS of 249,706 individuals, Speliotes identified 18 new loci associated with BMI, in addition to 14 SNPs previously associated with BMI and waist and weight measurements [Speliotes, 2010].
Hypertension, blood pressure
Type II diabetes: Zeggini and colleagues reviewed the literature on loci associated with type II diabetes and identified six additional susceptibility loci in a large-scale replication study of 53,795 individuals [Zeggini et al. 2008].
Dyslipidaemia: a large-scale GWAS of more than 100,000 individuals identified 95 loci associated with both normal variation in blood lipid traits and extreme blood lipid phenotypes [Teslovich et al. 2010]. Two more studies of 5414 and 132 individuals respectively identified SNPs associated with blood cholesterol levels and hypertriglyceridaemia [Kathiresan et al. 2008; Wang et al. 2008].
Recently a number of GWAS also focused on MetS as an entity. Kraja and colleagues in their analysis including 22162 samples identified 29 common variants associated with MetS or a pair of its traits [Kraja et al. 2011]. Zabaneh and Balding analysed 4794 samples and identified nine loci associated with the development of MetS in Asian men, not substantially different from MetS determinants in other populations [Zabaneh and Balding, 2010].
A number of studies have also implicated several genes in the development of MetS. Polymorphic variants of the gene encoding 5,10-methylenetrahydrofolate reductase (MTHFR gene) appear to infer an increased risk for metabolic abnormalities, especially in response to antipsychotic medication [Van Winkel et al. 2010; Kuzman and Mueller, 2012]. A polymorphism of the gene encoding the adrenergic α1A receptor (ADRA1A gene) is found to be a risk factor for severe metabolic abnormalities [Cheng et al. 2012]. Similarly, another polymorphism of the gene encoding serotonin 2C receptor (HTR2C gene) is also associated with increased risk of MetS in patients taking antipsychotics, particularly those using clozapine or risperidone [Mulder et al. 2007, 2009]. Polymorphic variants of the cannabinoid type 1 receptor gene (CNR1 gene) are associated with obesity-related phenotypes in women [Milewicz et al. 2010]. Finally, variations in genes implicated in circadian regulation (clock genes) may be important in the regulation of metabolic parameters in schizophrenia, during long-term treatment with SGAs [Moons et al. 2011].
These studies indicate that the cardiovascular risk factors associated with MetS are to a certain extent genetically determined. This means that there is likely a genetic aspect to the cardiovascular risk seen in people with schizophrenia. Future research should address this emerging concept of the genetic predisposition to develop MetS in schizophrenia. Thus we could potentially develop diagnostic tools that will inform us of the risks carried by a particular individual of developing MetS, even before the initiation of antipsychotic medication. This would allow appropriate medication choices to be made early in the course of illness and adequate health interventions to be implemented sooner rather than later. Hopefully more research in the future will be able to clarify these complex metabolic pathways and provide proactive management of all these metabolic disturbances.
The importance of monitoring for the prevention of metabolic syndrome
The cornerstone of early detection and effective management of MetS in patients with schizophrenia is comprehensive monitoring, and a variety of guidelines provide structured schedules for this. Despite the introduction of guidelines for metabolic screening in schizophrenia, metabolic monitoring in routine clinical practice is still low. In their impressive meta-analysis of 48 studies, Mitchell and colleagues reviewed changes in monitoring screening of patients receiving antipsychotics before and after the implementation of relevant guidelines [Mitchell et al. 2012a]. They concluded that although guidelines can increase monitoring, most patients still do not receive adequate testing. Similar results come from another group of researchers who found that glucose and lipid screening is underutilized in patients starting on SGAs [Morrato et al. 2008], and the introduction of the American Diabetes Association’s Consensus Statement on antipsychotic drugs and diabetes was not associated with an increase in screening rates [Morrato et al. 2009].
Apart from the basic features of MetS (BMI, fasting plasma glucose, fasting plasma lipids, blood pressure), other tests such as electrocardiography and routine blood tests (urea and electrolytes, liver function tests, full blood count, prolactin levels) can complement the laboratory and physical checks of patients with schizophrenia, especially those in receipt of antipsychotic medication. A medical and family history should also be included in this monitoring, and in most cases it is meaningful to accompany the whole process with regular advice on healthy living. The frequency of monitoring can vary and be adapted to the individual needs of patients. However, it is more important that this process is incorporated into regular psychiatric follow up. The findings that certain ethnic groups, female sex, family history and type of medication all increase the risk of developing MetS can be used by practitioners to identify and target certain individuals who are likely to be at greater risk of life-threatening cardiovascular disease should they develop schizophrenia.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors
Conflict of interest statement
The authors declare that there is no conflict of interest.