
Abstract
Some studies suggest Imagery Rescripting (ImRs) may be more effective than Imaginal Exposure (IE) for processing trauma when non-fear emotions are predominant. ImRs has been proposed to work through positive memory revaluation and increasing mastery, while IE focuses on fear toleration through inhibitory learning. We present standardized ImRs and IE analogues to explore their impact on non-fear emotions and underlying mechanisms. Forty-one participants selected an autobiographic event and were randomly assigned to ImRs, IE, or a control condition. Core elements of ImRs and IE were delivered via audio. We repeatedly assessed event-related emotions, distress, mastery, and tolerance for negative emotions. Participants in ImRs showed greater reductions in distress, fear, and anger, but not in self-conscious emotions, compared to IE. Unexpectedly, IE participants experienced increased negative emotions, including fear, with no specific advantage for increasing tolerance. Reductions in negative emotions were also observed in the control group. We found tentative indications for positive revaluation following ImRs. In conclusion, the ImRs analogue largely facilitated expected changes, while IE led to adverse effects. We discuss potential reasons for these findings and suggest improvements for the analogues and overall procedure.
Keywords
Introduction
Research has shown that exposure-based treatments effectively improve post-traumatic stress disorder (PTSD, Bradley et al., 2005; Lewis et al., 2020; Watkins et al., 2018). However, approximately 40% of PTSD patients still show clinically significant symptoms following gold-standard treatment with cognitive behaviour therapy (Semmlinger et al., 2024). It has been suggested that ‘non-fear’ emotions like shame, guilt, or anger play an important role in the development, maintenance, and treatment outcomes of PTSD (Andrews et al., 2000; Dillon et al., 2020; Kubany & Watson, 2003; Saraiya & Lopez-Castro, 2016).
Imagery Rescripting (ImRs; Schmucker & Köster, 2017) may be a promising therapy approach for addressing non-fear emotions associated with autobiographical (traumatic) events. Imaginative techniques are particularly applicable when direct confrontation with distressing situations is impractical or harmful, such as in conditions related to trauma or other negative interpersonal experiences.
A growing body of research has shown that ImRs is effective across a range of psychological disorders (for a meta-analytic review, see Kip et al., 2023; Kroener et al., 2023). An ImRs-session, according to the protocol by Schmucker and Köster (2017), 1 starts with an exposure phase focusing on the most distressing part (the ‘hotspot’) and progresses to rescripting the original scene. At first, the patient imagines the current self entering the scene, mastering or resolving the situation in a way that the former, traumatized self feels safe (e.g. imagining the police arriving to apprehend the perpetrator). In the second phase, the therapist guides the current self to provide compassion and comfort to the former self. The rescripting process allows personalized modification of the situation, addressing the maladaptive cognitions and emotions. Some clinical studies with PTSD patients reported larger reductions in non-fear emotions after ImRs compared to an exposure-based intervention (Arntz et al., 2007) or improvements for patients who did not respond well to CBT (Grunert et al., 2007). They put forward the hypothesis that trauma patients who experience primarily non-fear emotions may not optimally benefit from mere exposure but profit from alternative approaches like ImRs.
One theoretical explanation may be that rescripting and exposure operate through different mechanisms. The most widely recognized mechanisms for exposure therapy are habituation and inhibitory learning. According to Emotional Processing theory (EPT; Foa & Kozak, 1986), repeated exposure to threatening stimuli (e.g. to aspects of the trauma during imaginal exposure) results in a reduction of the negative emotional response within and across exposure sessions. This reduction (or habituation) is incompatible with the fear memory and is assumed to weaken the association between stimulus and response elements. Yet EPT also recognized that repeated exposure without the anticipated negative outcome (e.g. escalating fear) corrects exaggerated threat probabilities, a process referred to as extinction learning in experimental research (Hermans et al., 2006).
Contemporary models extended this concept by positing that the central mechanism of fear extinction is inhibitory learning. Through repeated pairings of the conditioned stimulus (CS) without the expected unconditioned stimulus (US), a new, inhibitory meaning is formed that competes with and inhibits the original excitatory meaning (Brewin, 2006). Within this approach, being able to tolerate elevated levels of fear is emphasized over fear reduction and seen as an adaptive emotion regulation skill (Craske et al., 2008).
In the context of imaginal exposure to traumatic (or other disturbing) memories, an expectancy mismatch may involve a patient realizing her ability to tolerate increased levels of anxiety and distress while recalling details of the event. However, the mechanisms may be more complex when addressing non-fear emotions. Self-conscious emotions like shame and guilt involve maladaptive cognitions about oneself (e.g. ‘I am fundamentally flawed’; ‘It is all my fault’) that may require active correction. Anger and guilt can serve as avoidance mechanisms, interfering with the confrontation of other painful trauma-related emotions during exposure (Dillon et al., 2020). Emotion-focused therapy, for example, differentiates between primary and secondary emotions, suggesting that secondary emotions (e.g. shame about symptoms) may obstruct access to primary maladaptive emotions rooted in negative experiences where fundamental needs have been neglected (Greenberg & Pascual-Leone, 2024). Further, the emotion-focused approach posits that while it is crucial to access and reduce maladaptive emotions, it is equally important to transform these emotions into adaptive ones, such as empowering anger and self-compassionate sadness through fulfilling formerly unmet needs (Herrmann et al., 2016). In summary, when multiple (non-fear) emotions are involved, simply learning that emotions decrease on their own or can be tolerated may be insufficient; instead, transforming negative emotions into more positive and adaptive ones might be crucial.
Imagery Rescripting (ImRs) has been hypothesized to facilitate a positive revaluation of the original memory using the principles of reconsolidation (Arntz, 2012). In contrast to inhibitory learning, where a new, no-threat memory is formed, the rescripting process is assumed to directly change the emotional meaning of the original memory in a positive way. Research by Kindt et al. (2009) has demonstrated that fear memories can be altered on a neuronal level when reconsolidation principles are applied. When a memory is reactivated, it becomes malleable, allowing the integration of new information. This may also occur in an IE session, for example, when disclosing shameful aspects of the traumatic situation and receiving empathy from the therapist. However, in ImRs, this process is more deliberate. During the second phase of ImRs, patients are guided to actively modify the course of the event, ensuring that fundamental needs, such as the needs for control, safety, and self-worth, are met while the memory is in an active state. Results from a study with nightmare patients, indeed, revealed an increase in feelings of mastery (i.e. feeling in control of the nightmare content) as the only significant mediator in the rescripting group, whereas, in the exposure group, an increased tolerance for negative emotions mediated treatment effects (Kunze, Lancee, et al., 2019). The advantages of memory revaluation include more rapid generalization across situations and lower rates of symptom reinstatement as the original memory is being changed.
Experimental analogue studies offer an effective and economical way to explore mechanisms and effects of treatment components (Waters et al., 2017). In a classical conditioning experiment with 70 healthy participants, Dibbets et al. (2012) demonstrated that adding ImRs during the extinction phase reduced fear reinstatement and aversiveness of the unconditioned stimulus (US; i.e. indicating revaluation). The fear memory was created using scripts about a car accident, followed by presenting a rescripted or an expectancy-mismatch ending. Another experiment compared mere extinction with ImRs and Eye Movement Desensitization and Reprocessing (EMDR) and found reductions in US aversiveness across all conditions, including extinction-only (Dibbets et al., 2018).
Several studies have employed the trauma-film paradigm (TFP, Holmes & Bourne, 2008), which involves the creation of a traumatic memory with a highly disturbing film scene followed by a memory consolidation phase of 30 minutes (Dibbets & Arntz, 2016; Hagenaars & Arntz, 2012; Siegesleitner et al., 2020), or 1 day (Siegesleitner et al., 2019; Woelk et al., 2022). After that, the memory is reactivated, and an intervention is employed. Results on whether ImRs is superior to IE in altering emotional meanings, including transforming negative (non-fear) emotions into positive feelings, were mixed. In a study by Dibbets and Arntz (2016), ImRs was not superior in reducing non-fear emotions (disgust, anger, and sadness). Siegesleitner et al. (2019) found reduced levels of fear, horror, anger, and disgust compared to IE but no differences in shame, guilt, and sadness. Woelk et al. (2022) found changes in US expectancy ratings in IE and IE + ImRs but not in ImRs-only. However, US aversiveness did not change in the ImRs conditions, and the authors suggested that changes may occur in memory-associated cognitions of beliefs rather than the US itself. In line with that, Hagenaars and Arntz (2012) found that ImRs led to fewer negative cognitions about the world and less self-blame compared to IE, though, with similar changes after positive imagery. Siegesleitner et al. (2020) reported a steeper increase in sense of mastery and positive emotions following ImRs compared to IE and a control condition. No differences between conditions were observed in negative emotions. The study noted the limitations of the TFP for assessing treatment effects on self-related emotions and cognitions, as a trauma film may not impact the self-beliefs of healthy participants, thus calling for experimental paradigms that allow for the investigation of personally relevant memories.
Recognizing this limitation, Strohm et al. (2019; 2021) and Çili et al. (2017) chose to study the effects of ImRs on personal memories of distressing autobiographic events in healthy subjects. Strohm and colleagues (2019, 2021) compared ImRs to a no-intervention control condition (2019) and positive imagery (2021), finding reductions in sadness and helplessness, as well as increased mastery after ImRs (2019). Meanwhile, Çili et al. (2017) reported positive emotional changes; however, the lack of an exposure-based control group limits the interpretability of these results. Given that studies with an exposure-based control group reported revaluation effects in the exposure condition (Dibbets et al., 2018) – along with theoretical explanations that could account for such findings – it is crucial to include an exposure-based control group when investigating differential mechanisms.
Study aims
This pilot study presents an analogue approach to investigate the effects and mechanisms of Imagery Rescripting (ImRs) and Imaginal Exposure (IE) using autobiographical memories, hereby adapting the methodology of Strohm et al. (2019) and Çili et al. (2017). To specifically examine self-conscious emotions, participants were asked to select experiences involving humiliation or rejection associated with feelings of shame and guilt. H. Watson et al. (2016) demonstrated that various versions of rescripting could be effectively delivered through pre-recorded audiotapes to victims of recent bullying behaviour. To ensure standardization, ease of administration, and replicability, we similarly recorded audiotapes featuring the core elements of ImRs and repeated IE (see supplemental online material). Following a brief memory reactivation, both intervention conditions began with a rehearsal of the selected situation. Participants in the IE condition were instructed to re-experience the situation a second time, whereas participants in the ImRs condition were guided to confront the ‘perpetrator’ and comfort their former selves. Participants in the control condition (CC) also listened to an audiotape about a neutral topic. Throughout the experiment, we measured event-related emotions, distress, sense of mastery, and tolerance for negative emotions as potential mechanisms underlying the effects of ImRs and IE.
Consistent with previous findings (Hagenaars & Arntz, 2012; Siegesleitner et al., 2019), we hypothesized that ImRs would be more effective than both IE and the control condition in reducing non-fear emotions, while IE and ImRs would yield similar reductions in fear. Furthermore, we anticipated that ImRs would increase sense of mastery and positive emotions, whereas IE would improve tolerance for negative emotions (Kunze, Lancee, et al., 2019; Siegesleitner et al., 2019; Strohm et al., 2019).
Methods
Participants
Fifty-six undergraduate psychology students completed session 1 in exchange for course credit. The sample size was determined for practical reasons and aimed at economic pilot testing of our procedures. Figure 1 displays a flow chart of study participation, dropout, and exclusion processes. Three participants dropped out after session 1. Fifty participants reported at least one psychological symptom; however, no exclusion symptoms (psychotic symptoms, suicidal thoughts, or self-harming behaviour). Five participants reported to be affected strongly by their symptoms and were excluded from further participation. However, two of them ignored the instructions on the screen to retreat from further participation and came to their laboratory appointment (session 2), which we only noticed during data analysis. We included them in the analysis, although there was some missing data at t0. None of the participants exceeded the cut-off value for PTSD suggested by Maercker and Schützwohl (1998) for the IES-R. Two participants completed the online assessments in the wrong order. We excluded another seven participants from the analysis because we had to assume that the experimental procedure did not work properly for them; they did not listen to the complete memory reactivation task (3 participants) and/or showed no changes or even decreases in arousal after MRT (4 participants). We concluded that they failed to recall a sufficiently distressing event or avoided the emotions associated with the memory. Five participants did not complete the follow-up online assessment 1 day later. We included participants with missing data at baseline (t0) and follow-up (t4) in the analysis sample to have maximum power for the analysis of the data collected at the laboratory assessment (session 2: t1-t3).The sample size for session 1 (Day 1: t0) was N = 39; for session 2 (Day 2: t1-t3) it was N = 41, n (IR) = 12, n (IE) = 15, n (CC) = 14; for session 3 (Day 3: t4) it was N = 36, n (IR) = 10, n (IE) = 14, n (CC) = 12. Mean age of participants at study participation (t0) was 22.59 years (Min = 19, Max = 30). Basic participants’ characteristics separated for condition are provided in Table 1. Flow chart of sample formation with dropouts and exclusions. Notes. DO = Drop out; FAC = Failed attention checks; WO = Completion in wrong order; ImRs = Imagery rescripting; IE = Imaginal exposure; CC = Control condition. Participants’ characteristics in session 1 (t0). Notes. IES-R = Impact of Events Scale-revised; ImRs = imagery rescripting; IE = imaginal exposure; CC = control condition. aThe third option ‘gender diverse’ was not selected.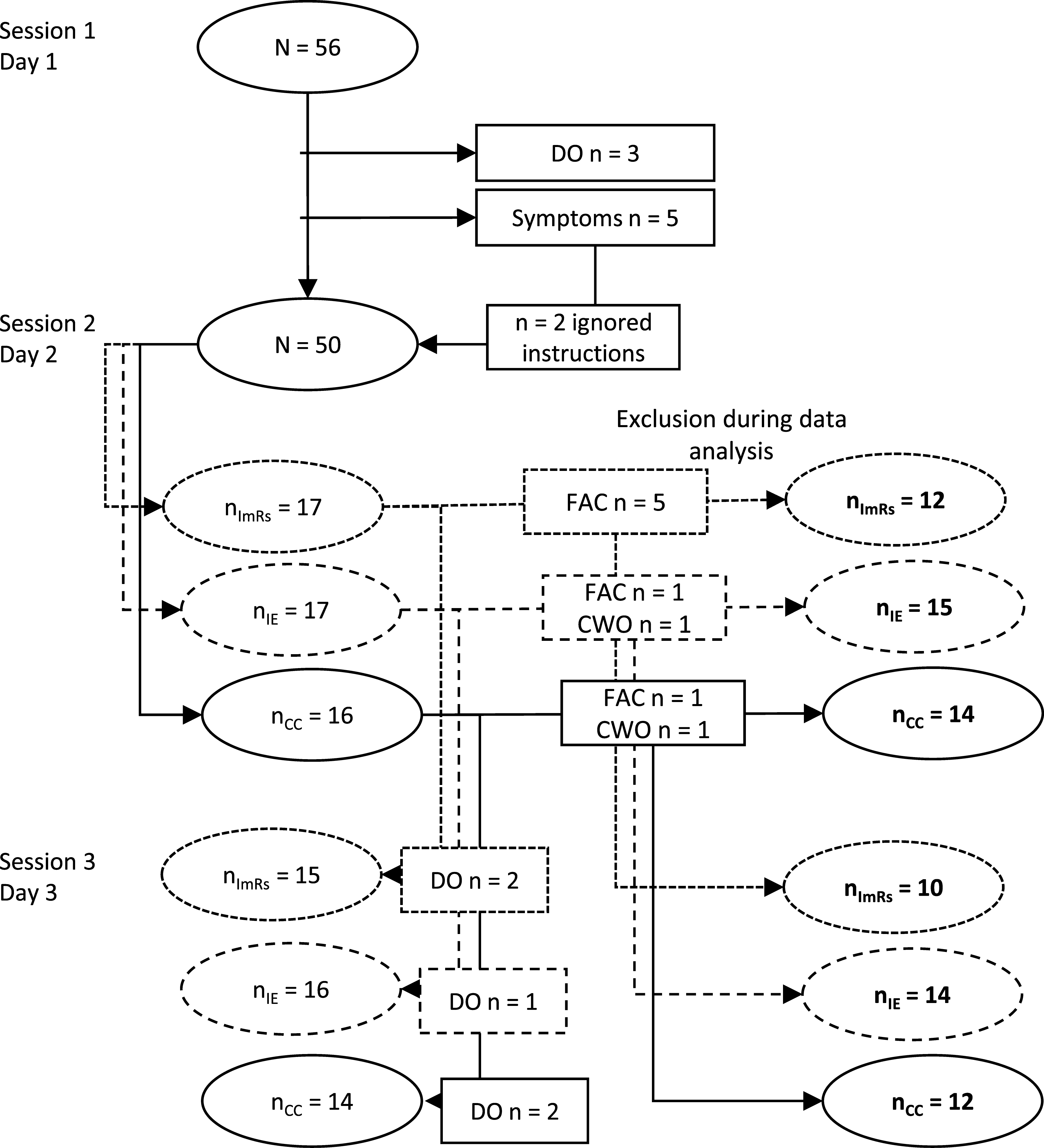

Audio recordings
We recorded audio instructions for memory reactivation and for all three experimental conditions and delivered them via headphones. Participants could go through the audios at their own pace by pressing a foot lever. The audio files and an English transcript are publicly accessible on the first authors’ OSF repository (https://osf.io/5tgaf/). Prior to the memory activation, participants selected a distressing autobiographical event for the use of this study.
Memory reactivation task (MRT)
The MRT was developed for the purpose of this study and consisted of three sequences. First, we led participants to picture the scene with their eyes closed to give rise to associated feelings. The second recording led participants to identify and dwell on the hotspot and to imagine the scene like a film. Several questions stimulated the recall of sensory information to facilitate a vivid imagination of the scene (i.e. ‘What do you see, hear, and smell’?). Thirdly, they were instructed to open their eyes and to proceed with answering the questionnaires. On average, participants needed 3.59 minutes (SD = 1.38) for the MRT. After the MRT, participants were randomly assigned by the online survey tool to IE, ImRs, or CC.
Imaginal exposure (IE)
During IE (based on Foa et al., 2014), we instructed participants to re-experience the situation twice. This included five audio recordings simulating different steps of an imaginal exposure session: (1) Finding a starting point of the situation; (2) Narration of the situation vocally or mentally from the beginning to the end in present tense and in first person; (3) Short grounding instructions (i.e. ‘Remember that the situation is over now and that you are here in our laboratory’); (4) Repetition of the situation narrative; and (5) positive reinforcement and instruction to open the eyes.
Imagery rescripting (ImRs)
During ImRs (based on Schmucker & Köster, 2017), participants were told to re-experience the situation once and then imagine the present self striking back at the perpetrator and showing compassion towards the younger self. This included ten audio recordings, of which the first two and the last one differed from the IE condition only in the way how the younger self was being addressed 2 . After the rehearsal (2) followed a concentration on the hotspot from the former self’s perspective (3) and the introduction of the present self (4). Recordings (5), (6) and (7) instructed the actual self to address and strike back at the perpetrator in a way that (s)he would not be able to do any more harm. They could also imagine helpers (e.g. police or a friend) to assist them in the process. Recordings (8) and (9) instructed the present self to show compassion and comfort to the younger self. We gave examples of possible actions (i.e. ‘Maybe s (he) would like to get a hug or be brought to a safe and nice place’?). Participants needed significantly more time for completion of ImRs compared to IE (8.8 vs. 4.7 minutes; F (1, 25) = 59.41, p < .01).
Control condition (CC)
Participants in the control group listened to a 6-minute informational text about amber (based on an article from Wikipedia). They were debriefed and got the option to receive ImRs to process their distressing event after post-assessment.
Measures
Demographics and mental health screening (t0)
After basic demographics (age, gender), we screened for mental health symptoms and traumatic experiences using the trauma list of the Composite International Diagnostic Interview (Wittchen & Pfister, 1997). Participants who reported a trauma completed the German version of the Impact of Events Scale-revised (IES-R, Maercker & Schützwohl, 1998; Weiss & Marmar, 1996).
Selection of the autobiographical event (t0)
Participants were instructed to choose a negative interpersonal experience from their childhood or adolescence where they had felt humiliated or rejected as we were particularly interested in investigating event-related feelings of shame and guilt and wanted to ensure high enough levels of shame and guilt. The situation should include at least one person who had caused the negative feelings to fit the standardized audio instructions. We gave some examples to stimulate memory recall and asked participants to describe characteristics of the event in an open-text format. We categorized the events and evaluated their appropriateness based on the open-text information (e.g. humiliation, being bullied, etc.).
State emotions and distress (t1, t2, and t3)
State emotions were assessed using the German version of the Positive and Negative Affect Schedule (PANAS, Breyer & Bluemke, 2016; D. Watson et al., 1988). To get more meaningful outcome measures from PANAS items, we derived four subscales via factor analyses: fear (items: afraid, jittery, scared, nervous, strong (i)), anger (items: irritable, hostile, upset), self-conscious emotions (items: guilty, ashamed), and positive emotions (items: enthusiastic, excited, proud; for more detail about scale formation, see supplemental material Figure S1). Cronbach’s alpha ranged from .76 to .88 at t2. PANAS items and subjective units of distress (SUD) were rated on a visual analogue scale (VAS) ranging from ‘0-not at all’ to ‘100-extremely’.
Event-related shame and guilt (t0, t2, and t4)
Event-related shame and guilt were assessed with the Event-Related Shame and Guilt Inventory (ERSGI, Kulla et al., 2021). In the current study, we administered a preliminary version with 40 items but used only the 12 items as in the latest version (see appendix). Cronbach’s alpha in the current sample was .89 for shame and .84 for guilt.
Mastery and tolerance (t0, t2, and t4)
We assessed feelings of mastery (i.e. feeling in control of the situation vs. feeling helpless and weak) and tolerance for negative emotions as possible working mechanisms in ImRs and IE with three items each. For mastery, participants posed a slide control between three pairs of adjectives: (1) weak – strong; (2) helpless – superior; (3) powerless – powerful. Due to a spelling error, we could not use item 3. For tolerance, participants rated three items on a VAS from ‘not at all true’ to ‘absolutely true’: (1) ‘I think I can handle the feelings triggered by the situation’; (2) ‘I would like to turn off the feelings triggered by the situation (i)’; (3) ‘I find the feelings I have about the situation terrifying (i)’. Cronbach’s alpha was .90 for mastery and .83 for tolerance. Low values (0) indicate low mastery/tolerance, and high values (max. 100) indicate high mastery.
Experimental procedure and manipulation
All procedures were approved by the university ethics committee. Written informed consent was provided from all participants. We used the CONSORT-SPI checklist when writing our report (Grant et al., 2018). The study comprised several measurements in three sessions that took place on three consecutive days (see Figure 2). Sessions 1 and 3 were an online survey that was completed at home. Session 2 took place in our laboratory. Experimental procedure. Notes. ERSGI = Event-Related Shame and Guilt Inventory; SUD = Subjective Units of Distress; PANAS = Positive and Negative Affect Schedule; ImRs = Imagery Rescripting; IE = Imaginal Exposure; CC = Control Condition; t1-t3 took place in the laboratory; t0 and t4 were an online survey to be completed on the day before and after.
Session 1
Participants completed session 1 at home, one day before their laboratory appointment. It included demographic questions and the screening procedure. Participants who fulfilled the inclusion criteria continued with selecting an autobiographical event for the study. It ended with baseline assessments of mastery, tolerance and event-related shame and guilt (t0).
Session 2
In our laboratory, participants were seated in single, soundproof PC booths to answer baseline state emotions and distress (t1). Then, they received audio instructions via headphones to activate memories of the selected autobiographical event (MRT). After that, they rated state emotions, distress, mastery and tolerance as well as event-related shame and guilt (t2). Participants were randomly assigned to one of three conditions: imagery rescripting (ImRs), imaginal exposure (IE), or a control condition (CC). The laboratory assessment ended with a post-assessment of state emotions and distress (t3).
Session 3
On the following day, participants completed follow-up assessments at home for mastery, tolerance and event-related shame and guilt (t4). For ethical reasons, the control group was debriefed and offered to receive ImRs as we assumed this intervention to be most effective.
Statistical analysis
We used RStudio 4.0.5 for all analyses. Randomization checks included several one-way ANOVAs and Fisher’s exact tests to test whether experimental groups differed in age, gender, mental health problems, characteristics of the chosen autobiographical event, and levels of outcome variables at baseline.
For manipulation checks and hypothesis testing, we used a linear mixed-effects model approach using lmerTest (Bates et al., 2015) with condition as between factor (3 levels: ImRs, IE, and CC) and time as within-factor. All models were fitted with random intercept at the participant level. Estimation method was REML; denominator degrees of freedom were approximated with the Kenward–Roger’s method. Checks for normality and homogeneity of the residual’s variances indicated violations in some dependent variables, but visual inspection with Q-Q-plots showed that violations were not extreme. We conducted an omnibus test with stats::anova and reported the fixed effects’ interaction estimates and respective t- and p-values using either CC or IE as reference groups to compare impact of the condition on time (base::summary). For evaluating reactions to the MRT, we used values from before to after MRT (t1-t2). We further explored gender-specific reactions to the MRT (between factor gender, within factor time). For evaluating changes through the interventions, we used values from before to after intervention phase (t2-t3 for state emotions and distress; t2-t4 for event-related shame and guilt, mastery and tolerance). Here, we controlled for gender, baseline levels, and the duration of the interventions. We calculated marginal (variance explained by fixed factors, that is, condition and time) and conditional (variance explained by fixed and random factors, that is, individual contribution of each subject) R2 for multilevel models (Nakagawa & Schielzeth, 2013) and effect sizes for t-values derived from the fixed-effects estimate using the R package DSUR.noof (Field et al., 2012).
Results
Randomization checks
About 64% of the sample was male. Randomization resulted in a slightly uneven gender distribution over groups with more female participants in the control condition (Fisher’s test, p = .11). There were no significant between-group differences in mental health (all ps > .56).
According to the instructions, participants selected most frequently a humiliating experience for the study (41.5%; e.g. being laughed at because of poor performance in front of the class or being cheated on by a girlfriend), an experience of physical assault (14.6%) and bullying (e.g. by (class)mates; 12.2 %). There were no significant group differences in event categories (Fisher’s test, p = .33).
The majority (83.3%) reported an event from age 18 or younger, as was asked in the instructions. We included the remaining four participants in the analysis since the priority was to choose the event that still bothered them the most at present. Mean age at the time of the distressing event was 13.53 years (SD = 4.51). There was no difference between conditions (F (2, 36) = .00, p > .99).
Means and standard deviations of outcome measures at baseline (t0), before (t1) and after memory reactivation (t2), immediately after intervention (t3), and at follow-up 1 day later (t4).
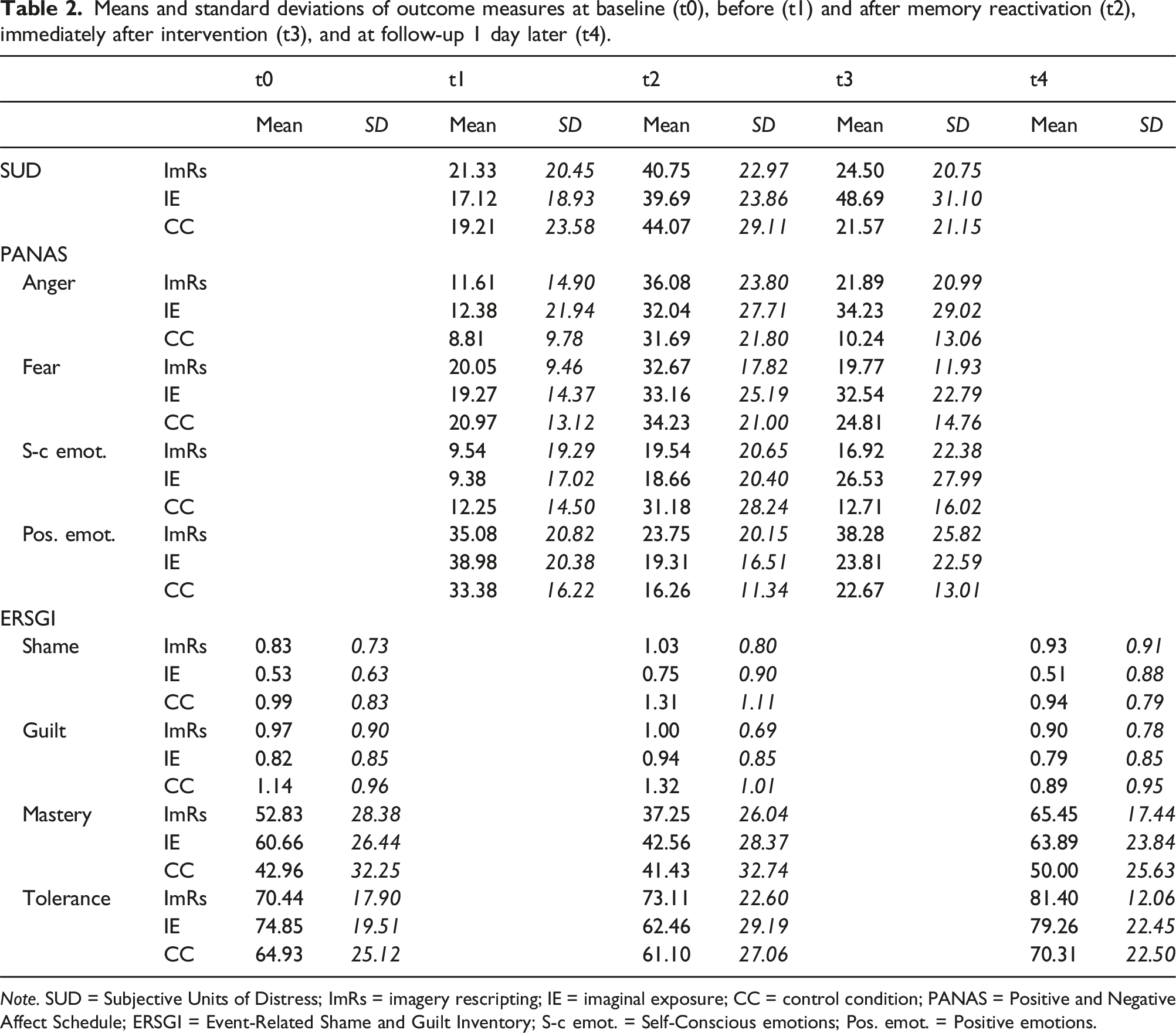
Note. SUD = Subjective Units of Distress; ImRs = imagery rescripting; IE = imaginal exposure; CC = control condition; PANAS = Positive and Negative Affect Schedule; ERSGI = Event-Related Shame and Guilt Inventory; S-c emot. = Self-Conscious emotions; Pos. emot. = Positive emotions.
Manipulation checks
Manipulation checks revealed that state emotions (PANAS) and SUD-values changed significantly in the expected directions in reaction to the MRT (t1-t2; main effects time all ps < .01) with no differences between conditions (main effect condition: all ps > .43) and no interaction effects (all ps > .21), meaning that participants reacted to the MRT with increased levels of negative emotionality (increase in estimated means across conditions between 12 and 22 units) and that randomization worked well beyond memory reactivation. There was a non-significant tendency for female participants to show larger increases in PANAS self-conscious emotions and event-related shame and guilt after MRT (ps between .09 and .28) which was not observed for fear and anger. Noticeably, although participants were instructed to choose an event associated with shame and guilt, they reported more anger and fear compared to self-conscious emotions after MRT (see Table 2).
Effects of interventions on event-related emotions (PANAS and ERSGI)
For SUD, we found a main effect for time (F (1, 42) = 10.56, p < .01) as well as for condition (F (2, 42) = 5.58, p < .01), and a significant interaction of time and condition (F (2, 42) = 11.11, p < .01). The amount of variance explained by the fixed effects (i.e. condition and time; marginal R2) was R2(m) = .48. The amount of variance explained by the entire model (i.e. conditional R2) was R2(c) = .75. In IE, SUD levels increased significantly as compared to CC (β = 31.83, t (38) = −3.43, p < .01, r = .59) and to ImRs (β = −25.58, t (38) = −3.43, p < .01, r = .49). Slopes of ImRs and CC did not differ significantly (β = 6.25, t (38) = 0.83, p = .41, r = .13).
For fear, we found a significant main effect of time (F (1, 42) = 10.17, p < .01) and a (non-significant) interaction of time and condition (F (2, 42) = 2.79, p = .07; R2(m) = .50, R2(c) = .71). Participants in ImRs experienced a significantly steeper decrease of fear compared to IE (β = −13.19, t (38) = −2.23, p = .03, r = .34) but slopes of ImRs and CC were similar (β = −3.49, t (38) = −0.58, p = .56, r = .09). Participants in CC also experienced a decrease but less pronounced and not significantly different to IE (β = 9.71, t (38) = −2.23, p = .09, r = .27). See Figure 3 for a graphical display of intervention effects on the main outcome variables fear, anger, self-conscious and positive emotions, as well as mastery and tolerance. Before and after intervention: Changes in PANAS fear, anger, self-conscious and positive affects (t2-t3) as well as mastery and tolerance (t2-t4) depending on condition. Notes. ImRs = Imagery Rescripting; IE = Imaginal Exposure; CC = Control condition.
For anger, there was a significant interaction between time and condition (F(2, 42) = 6.26, p < .01), revealing a significantly steeper decrease in anger for ImRs (β = −16.84, t (38) = −2.31, p = .03, r = .35) but also for CC (β = −24.1, t(38) = −3.45, p < .01, r = .49) compared to IE. Slopes of ImRs and CC were very similar (β = 7.26, t(38) = 0.98, p = .33, r = .16).
For self-conscious emotions, we found a significant interaction of time and condition (F(2, 42) = 4.35, p = .02, R2(m) = .38, R2(c) = .50). Surprisingly, participants in CC experienced a steep decrease of self-conscious emotions, while participants in IE experienced a slight increase (β = 26.1, t(38) = 2.93, p < .01, r = .43). Participants in ImRs did not change from pre- to post-intervention and did not differ from IE (β = −10.26, t(38) = −1.11, p = .28, r = .18) or CC (β = 15.84, t (38) = 1.68, p = .10, r = .26).
For positive emotions, we found a significant main effect of time (F(1, 42) = 10.05, p < .01) and condition (F(2, 42) = 3.62, p = .04), but no interaction effect (F(2, 42) = 1.10, p = .34, R2(m) = .43, R2(c) = .62). In Figure 3, participants in ImRs seem to have experienced a unique increase in positive emotion. However, the difference was not significant when compared to CC and IE (IR/CC: β = 8.12, t(38) = 1.18, p = .24, r = .19; IR/IE: (β = 9.44, t(38) = 1.40, p = .17, r = .22). A post-hoc contrast analysis of differences between ImRs and all other participants (Helmert contrast) controlling for values at t1 and t2 indicated significantly higher levels of positive emotions for ImRs (β = 4.22, t (36) = 2.16, p = .04, r = .34) at post-intervention (t3).
For event-related shame, there was only a significant main effect of time (F (1, 32.37) = 12.16, p = .00), but no main effect of condition or interaction effects (all ps > .18, R2(m) = .69, R2(c) = .89). For event-related guilt, there was a significant interaction effect (F(2, 32.13) = 5.34, p < .01, R2(m) = .66, R2(c) = .90). Contrary to our hypotheses, that was caused by participants in CC who showed a significantly steeper decrease in guilt compared to IE (β = −0.48, t(31.97) = 3.18, p < .01, r = .49) and ImRs (β = −0.34, t(32.36) = 2.17, p = .04, r = .36). ImRs and IE did not differ (β = −0.14, t(32.07) = −0.87, p = .39, r = .15).
Effects of interventions on mastery and tolerance
For mastery, there was a significant main effect of time (F (1, 33.19) = 28.03, p < .01), but no significant interaction between time and condition (F(2, 33.15) = 1.79, p = .18, R2(m) = .52, R2(c) = .72). In Figure 3, participants in ImRs seemed to have experienced a steeper increase in mastery compared to IE and CC, but the differences were not significant (IR/CC: β = 16.79, t(33.55) = 1.88, p = .07, r = .31; IR/IE: β = 10.76, t(33.1) = 1.2, p = .24, r = .20), and levels at t3 were not higher when compared to all other participants (Helmert contrast: β = 2.78, t(29) = 1.40; p = .17, r = .25)
For tolerance, there was only a significant main effect of time (F(1, 32.74) = 19.25, p < .01), but no main effect of condition or interaction effects (all ps > .66, R2(m) = .54, R2(c) = .79).
Discussion
This study presented an alternative analogue approach to investigate and compare emotional processes and underlying mechanisms of imaginal exposure (IE) and imagery rescripting (ImRs), specifically focusing on self-conscious emotions. To enhance standardization, we used pre-recorded audio instructions. Participants selected a distressing interpersonal experience associated with feelings of shame and guilt. After memory reactivation (MRT), participants were randomly assigned to ImRs, IE, or a control condition. Immediately after the intervention phase, we assessed state emotions and distress, and, one day later, event-related shame and guilt, as well as feelings of mastery and tolerance for negative emotions as potential underlying mechanisms, and compared values to pre-intervention levels.
Evaluation of the memory reactivation task
Overall, memory reactivation appeared to have worked successfully, though levels of negative event-related emotions, particularly shame and guilt, were moderate, mainly remaining within the lower third of the scale. Distress and state emotions measured before and after MRT differed significantly and in the expected directions, with changes of about 10–20 units (VAS from 0–100). Only four participants showed no change or a decrease in distress following MRT; these participants had been excluded from further analysis. The findings suggest that our audio-taped MRT effectively reactivated the memory of the autobiographical event. However, despite instructions to select an event associated with shame and guilt, participants reported higher levels of anger and fear than self-conscious emotions after MRT. This may be unsurprising given the healthy and predominantly male sample. Nevertheless, insufficient memory activation can lead to measurement issues and violation of statistical assumptions, which underscores the challenge of studying clinical phenomena through analogue experiments (Waters et al., 2017). Future research should explore methods to intensify the reactivation process or implement more careful participant selection based on the intensity of event-related emotions.
Evaluation of the interventions
Imagery rescripting
Emotional changes following the ImRs analogue generally aligned with our expectations. Compared to IE, ImRs resulted in significantly greater reductions in distress, fear, and anger. However, this pattern was less pronounced for PANAS self-conscious emotions and event-related shame and guilt, where we had anticipated the largest divergence. The expected means of PANAS self-conscious emotions remained almost stable from pre- to post-intervention in ImRs. Additionally, we observed a decrease in self-conscious emotions and event-related guilt in the control group, which differed significantly from changes observed in ImRs (for event-related guilt) and IE (for both). While these results correspond to the findings from Siegesleitner et al. (2019), our analogue design specifically aimed to observe changes in self-conscious emotions.
How can these results be interpreted? First, they may suggest that ImRs does not have a superior effect in reducing feelings of shame and guilt. However, given the small pilot sample, we should be cautious in generalizing this finding; more research is required to draw more definite conclusions here. Another potential explanation is that we observed a floor effect in the ImRs group, who had the lowest pre-intervention levels of PANAS self-conscious emotions (about 15 units lower than the control group) but showed almost the same post-intervention levels as the control group. A similar effect may explain the results for event-related guilt.
Moreover, we found hints of a unique increase in positive emotions and feelings of mastery in the ImRs group, consistent with the results of Siegesleitner et al. (2020). However, these results were not statistically significant and require further investigation.
Imaginal exposure
While we expected ImRs to change event-related emotions more strongly than IE, we did not anticipate the adverse effects observed in the IE condition. Other experiments have similarly reported high levels of distress and fear in exposure conditions (Dibbets & Arntz, 2016; Siegesleitner et al., 2019). An initial increase in distress and anxiety is part of exposure therapy; however, these levels are also expected to decrease over time. It is possible that the IE analogue was too short to fully unfold its effects. Although we controlled for the duration of the intervention phase, this only accounts for a linear relationship between imagination time and outcome variables. In reality, emotional responses to exposure typically follow an inverted-U or parabolic trajectory, that is, rising first and then attenuating. Another explanation could be that the formation of the inhibitory memory marked by lower fear levels was not complete immediately after the intervention phase and would have become evident at a follow-up measurement (Kunze, Arntz, & Kindt, 2019). The increase in tolerance for negative emotions and sense of mastery that was also observed in the IE group supports this notion. Future studies should consider extending the exposure phase or adding a consolidation phase and measuring all variables afterwards.
So far, we have not observed a specific increase in tolerance for negative emotions following IE; instead, tolerance increased across all conditions. It is possible that exposure through the MRT alone was sufficient to increase tolerance, but this needs further investigation.
Control condition
Lastly, the control condition resulted in decreases across all negative emotional states. Similar effects were observed in other experiments comparing ImRs and IE to a control condition (Dibbets & Arntz, 2016; Kunze, Arntz, & Kindt, 2019; Siegesleitner et al., 2019). It is likely that the control group was distracted by listening to the informational text. Since we did not apply the MRT a second time after the intervention, we may have measured participants’ ability to disengage from adverse emotions rather than the intensity of feelings during (or shortly after) active recall. However, this does not fully explain the decrease in event-related guilt in the control group 1 day later. Another possibility is that the MRT alone initiated a revaluation process or created an inhibitory memory with the post-intervention measurements (t3) capturing these effects. The relatively high anger scores reported after MRT may indicate a surge of righteous anger toward the perpetrator, marking the beginning of a revaluation process. Developing control conditions that keep the memory in an equally active state without resulting in inhibition learning or revaluation remains a challenge.
Strengths and limitations
The strengths of this study include its experimental design, featuring both an exposure condition and a no-intervention control condition. We introduced a novel design utilizing personally relevant memories but maintaining a high level of standardization which facilitates easy administration and replicability for future researchers. In future, the interventions may be used as an online therapy tool, for example, as blended care or to bridge the waiting period for a therapy spot.
However, the study has several limitations and results should be interpreted cautiously. First, the sample was a very small and homogeneous student sample. The randomization resulted in a slightly unbalanced gender distribution across experimental groups (more females in the control group). Female participants tended to show stronger reactions in self-conscious emotions after MRT, which may have contributed to floor effects in the predominantly male intervention groups. Despite this, our results add value as most previous studies were mainly conducted with female participants (e.g. Strohm et al., 2019: 81.5% females; Siegesleitner et al., 2019: 100% females). No data was collected to identify participants’ racial and ethnic identity or cultural background. Future studies should aim for larger, gender-balanced samples and consider possible gender effects.
Second, we used a preliminary version of the ERSGI to improve the measurement of event-related shame and guilt beyond a single-item assessment. However, initial validity checks suggest it may be more appropriate for use in clinical populations (Kulla et al., 2021). Third, we did not include a measure of PTSD symptom severity or an analogue, such as tracking intrusions over the following week. Including these measures would have allowed for comparisons of symptom improvement in IE and ImRs, especially since some studies report similar effectiveness in (analogue) symptom reduction but differences in emotional changes (Arntz et al., 2007; Siegesleitner et al., 2019, 2020). Fourth, comparisons with existing studies may be limited, as we did not follow the ImRs protocol by Arntz and Weertman (1999). We cannot rule out that the patient’s perspective in the third phase produces different effects. Fifth, due to data privacy concerns, we did not record verbalizations during the imagination tasks. Thus, we have no knowledge about the content of the imagery processes and if participants followed the audio instructions. Sixth, the study was not pre-registered.
Conclusion
In summary, the emotional changes following the ImRs analogue were largely consistent with our expectations and previous findings. ImRs led to greater reductions in distress, fear, and anger compared to IE, but there were no significant reductions in PANAS self-conscious emotions and event-related shame and guilt. Interestingly, the control group also showed reductions in all negative emotions, including self-conscious emotions and guilt that differed significantly from IE. Contrary to our expectations, the IE analogue resulted in increased levels of negative emotions including fear. We found (non-significant) hints for positive revaluation in ImRs, indicated by increased levels of positive emotions and sense of mastery post-intervention; there was no specific increase in tolerance for negative emotions following IE.
To conclude, the ImRs analogue performed well, yielding largely anticipated effects. However, refinements to the control and IE conditions seem necessary to ensure a more accurate comparison between well-matched analogues.
To enhance the analogue interventions and overall procedure, we recommend the following: extending the duration of IE to better align with ImRs and ensure the completion of inhibitory memory processes (e.g. by adding another repetition or a focused section on the hotspot, and including a consolidation phase); repeating the MRT before post-assessments to reactivate the memory specifically in the control group; incorporating measures for PTSD analogue symptoms; and considering the collection of real-time physiological data. Emphasis should be placed on the robust induction of analogue symptoms and event-related emotions to prevent floor effects, for example, through careful sample selection based on the intensity of event-related emotions.
Supplemental Material
Supplemental Material - An analogue approach to investigate non-fear emotions and working mechanisms in imagery rescripting and imaginal exposure: Preliminary findings
Supplemental Material for An analogue approach to investigate non-fear emotions and working mechanisms in imagery rescripting and imaginal exposure: Preliminary findings by Jessica Schlünzen, Patricia Kulla, and Joachim Kruse in Journal of Experimental Psychopathology.
Supplemental Material
Supplemental Material - An analogue approach to investigate non-fear emotions and working mechanisms in imagery rescripting and imaginal exposure: Preliminary findings
Supplemental Material for An analogue approach to investigate non-fear emotions and working mechanisms in imagery rescripting and imaginal exposure: Preliminary findings by Jessica Schlünzen, Patricia Kulla, and Joachim Kruse in Journal of Experimental Psychopathology.
Footnotes
Author contributions
Jessica Schlünzen: Conceptualization, Methodology, Formal analysis, Investigation, Data curation, Writing - Original draft, Visualization, Project administration; Patricia Kulla: Conceptualization, Methodology, Investigation, Writing – Review & Editing, Project administration; Joachim Kruse: Conceptualization, Validation, Resources, Writing – Review & Editing, Supervision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge financial support from the University of the Bundeswehr, Munich, for covering publication fees (FORScience - Open Access Fund for Journals).
Transparency and openness statement
A detailed trial protocol, materials (i.e. audio recordings), and analysis code are available on the OSF repository of the first author (![]() ). Unpublished questionnaires (i.e. ERSGI) and methods for scale formation (i.e. PANAS subscales) are available as supplemental material. Data was collected from students of the University of the Bundeswehr Munich and cannot be made public due to restrictions of the German Ministry of Defense. The university ethics committee granted ethical approval.
). Unpublished questionnaires (i.e. ERSGI) and methods for scale formation (i.e. PANAS subscales) are available as supplemental material. Data was collected from students of the University of the Bundeswehr Munich and cannot be made public due to restrictions of the German Ministry of Defense. The university ethics committee granted ethical approval.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.