
Abstract
Individuals with schizophrenia (SCZ) form less accurate mental representations of the self and others, which contributes to social dysfunction. It remains unclear, however, whether such deficits extend to metaperception (MP), the ability to understand how others view one’s own personality. In Phase 1 of this study, 30 individuals with SCZ and 30 healthy controls (HCs) had a videotaped conversation with an experimenter and then completed a Big Five trait questionnaire, with the goal of predicting how strangers who view their videos would rate them on the five personality traits. In Phase 2, separate participants watched the videos and rated targets’ personalities. These ratings served as “The Truth” to which Phase 1 MPs were compared for Tracking Accuracy (i.e., extent to which The Truth predicts MPs) and Directional Bias (i.e., extent to which MPs overestimate or underestimate the truth). Tracking Accuracy was weaker in SCZ than in HC for Openness, Conscientiousness, and Agreeableness. Moreover, Tracking Accuracy and Directional Bias of MPs in SCZ were unrelated to mentalizing abilities and clinical insight. Our results suggest that the capacity to understand how others view one’s own personality is impaired in SCZ and may be a distinct component of the social cognitive system.
Metacognition (i.e., thinking about thinking) is impaired in people with schizophrenia (SCZ) relative to healthy controls (HCs) (Dimaggio & Lysaker, 2015; Lysaker, Dimaggio, & Brüne, 2014). First defined by Flavell (1976), metacognition is broadly considered the superordinate of second-order cognitive processes, such as perceptions about perceptions and reflections about actions (Overschelde, 2008). A key component of metacognitive capacity in SCZ is impaired introspection (Gould et al., 2015; Lysaker et al., 2001; Mishara, Lysaker, & Schwartz, 2014), and these impairments can span both nonsocial and social domains (Harvey & Pinkham, 2015). In nonsocial domains, deficits include reduced introspective knowledge of one’s memory capacities and preferred learning style (Koren et al., 2004; Koren, Seidman, Goldsmith, & Harvey, 2006; Peters, Hauschildt, Moritz, & Jelinek, 2013). Deficits in socially relevant domains include reduced introspective knowledge of one’s feelings to cope with psychological challenges (Lysaker et al., 2011) and one’s ability to recognize self-generated emotions (Demily, Weiss, Desmurget, Franck, & Baudouin, 2011). Deficits are also evident in social cognitive domains such as emotion perception (Moritz, Woznica, Andreou, & Köther, 2012) and mental state attribution (Köther et al., 2012).
In the social domain, the larger concept of metacognition, which includes introspective knowledge, is often regarded as the synthesis of information about emotions, thoughts, and intentions into a coherent understanding of the self and others that guides behavior (Bruno, Sachs, Demily, Franck, & Pacherie, 2012; Dimaggio, Lysaker, Carcione, Nicolò, & Semerari, 2008; Hamm et al., 2012; Koren & Harvey, 2006; Lysaker et al., 2013). This notion accommodates early (Bleuler, 1911) and modern (Lysaker & Lysaker, 2010) theories of SCZ as a disorder of the self, wherein experience of the self and the distinction between the self and others are compromised (Hur, Kwon, Lee, & Park, 2014; Mishara et al., 2014; Park & Nasrallah, 2014). For instance, work in source monitoring errors indicates that those with SCZ often confuse their own actions and thoughts with those of others (Keefe, Arnold, Bayen, & Harvey, 1999). Such an inability to create a clear self-other distinction might render differential evaluation of one’s own and others’ cognitive experiences problematic and exacerbate social functioning difficulties (Penn, Corrigan, Bentall, Racenstein, & Newman, 1997). Supporting this idea, metacognitive performance has been found to account for 10–15% of the variation in social outcomes above and beyond that accounted for by other forms of cognitive performance (Brüne, Dimaggio, & Lysaker, 2011; Gould et al., 2015; Lysaker et al., 2010, 2013; Mitchell et al., 2012). Additionally, targeting metacognitive deficiencies has proven beneficial for improving social functioning, with researchers noting the unique role that metacognition plays in monitoring and regulating one’s social behavior (Dodell-Feder, Tully, & Hooker, 2015; Moritz et al., 2014; Moritz, Veckenstedt, Bohn, Köther, & Woodward, 2013; Ottavi et al., 2014; Rocha & Queirós, 2013; Schaub, Abdel-Hamid, & Brüne, 2010).
An important aspect of understanding the self and others is perception of personality traits, the dispositional properties that make us distinct social entities (Funder, 2012). Judgments of these traits are frequently made and are socially consequential, helping us find suitable friends and romantic partners, explain past behavior, predict future behavior, and navigate our social world (Funder, 1991, 1999). Perceptions about how others view one’s own personality are called metaperceptions (MPs) because they entail forming perceptions about others’ perceptions (Cook & Douglas, 1998; Laing, Phillipson, & Lee, 1966). Requiring a coherent perception of the self and why others may perceive oneself differently, MP is considered a metacognitive process that underlies social judgments (Briñol & DeMarree, 2012; Petty, Briñol, Tormala, & Wegener, 2007) and relates to self-perceptions. In the general population, the correlation between MPs and self-perceptions of personality is around .70 (Kenny & DePaulo, 1993); that is, people believe that others view them fairly similarly to how they view themselves (Campbell & Fehr, 1990; Kenny & West, 2008; Malloy, Albright, Kenny, Agatstein, & Winquist, 1997; Vazire & Carlson, 2010). This may be because people self-perceive their behavior and assume that others see it the same way, or because they internalize how they think others view them based on feedback (Felson, 1992; Kenny & DePaulo, 1993).
Evidence suggests that MPs are not simply projected self-perceptions but rather that they require intricate social information processing. MPs (e.g., how Mark thinks Sue perceives him) agree more with others’ perceptions (e.g., how Sue actually perceives Mark) than do self-perceptions (e.g., how Mark views himself; Albright, Forest, & Reiseter, 2001; Carlson, Vazire, & Furr, 2011; Oltmanns, Gleason, Klonsky, & Turkheimer, 2005). Such keen MPs likely require objective evaluation of one’s own behavior and an ability to interpret others’ feedback in response to that behavior (Albright & Malloy, 1999; Carlson & Furr, 2009; Stopfer, Egloff, Nestler, & Back, 2014; Wyer, Henninger, & Wolfson, 1975). For example, those higher in mindfulness (i.e., awareness of the present moment and unbiased observation of one’s own experience) and interpersonal adjustment (i.e., social competence) produce MPs that relate more strongly to others’ actual perceptions (Carlson, 2013, 2016). Increased understanding of the self and others, therefore, seems important to MP, which is further supported by studies showing that people who report higher confidence in the agreement between their MPs and others’ perceptions produce greater such agreement (Carlson & Furr, 2013; Carlson, Furr, & Vazire, 2010). Perhaps unsurprising then, MPs appear influential across the social domain (Anderson, Srivastava, Beer, Spataro, & Chatman, 2006; Schlenker, 2003; Tice & Wallace, 2003). In romantic relationships, for instance, targets whose MPs more closely match their partners’ perceptions of them have more satisfied partners (Carlson, 2016), and targets’ beliefs that their partners view them as insecure, regardless of their veracity, are associated with destructive relationship beliefs and behavior (Lemay & Dudley, 2009).
Despite this extensive literature in the general population, very little is known about MP of personality in individuals with SCZ. To the best of our knowledge, only one study has approached this topic by assessing the correspondence between personality self-perceptions and others’ perceptions in SCZ. Klein, Altinyazar, and Metz (2013) asked target participants and their first-order relatives to rate the targets’ everyday personalities on 60 trait adjectives. The average correlation between ratings by patients and their relatives (r = .316) was significantly smaller than the correlation between ratings by HCs and their relatives (r = .659). This suggests that people with SCZ may exhibit reduced introspective knowledge of their personalities; however, as individuals were not asked specifically to rate how they believe that others perceive them, MP was not directly evaluated.
Because personality judgments are so commonly made, guide our behavior, and are important for understanding the social self and others (Funder, 1999), additional work is needed to develop a comprehensive understanding of how people with SCZ view their own personalities and how closely these views adhere to those of both familiar and non-familiar others. Although personality MP has been demonstrated to demand complex social information processing and relate to social functioning in the general population (Carlson, 2013, 2016; Lemay & Dudley, 2009), it has yet to be systematically investigated in SCZ. Doing so would illuminate whether the impaired metacognitive system that underlies distorted mental representations of the self and others (Bora, Sehitoglu, Aslier, Atabay, & Veznedaroglu, 2007; Fisher, McCoy, Poole, & Vinogradov, 2008) is implicated in personality perception, which might have important consequences for the social dysfunction so common in the disorder (Hooley, 2015; Mueser & Bellack, 1998). Findings of inaccurate MPs in SCZ may contribute to metacognitive training programs aimed at improving social functioning by encouraging behavioral self-awareness, utilization of behavioral feedback, and impression management related to personality perception.
The aim of the current study was therefore to determine whether people with SCZ are less accurate and more biased than healthy individuals at predicting how others view their personalities. We adopt the Truth and Bias Model of Judgment (West & Kenny, 2011) in the present work to help address these questions. In this model, perceiver judgments of some criterion are assumed to be pulled toward the truth to some extent, as well as other values distinct from the truth, which the model labels bias (West & Kenny, 2011). Using this model, we operationalized the accuracy and bias of MPs with two components: (1) Tracking Accuracy, the extent to which others’ actual perceptions predict MPs, and (2) Directional Bias, the extent to which MPs overestimate or underestimate others’ actual perceptions (i.e., the signed difference between individual MPs and the average value of others’ actual perceptions). In addition, we evaluated assumed similarity as an additional source of bias in MPs as well as other metacognition variables as moderators of Tracking Accuracy and Directional Bias.
To test the accuracy and bias of MPs in SCZ, a two-phase design was employed. In Phase 1, individuals with SCZ and HCs had a videotaped “get to know you” conversation with an experimenter and then completed a personality questionnaire with the goal of predicting how strangers who view that videotape would rate their personalities. In Phase 2, undergraduates unfamiliar with Phase 1 target participants watched the videos and rated targets’ personalities. These ratings served as “The Truth” to which Phase 1 MPs were compared for accuracy and bias. Given previous findings of poor introspective accuracy in SCZ and reduced neural activation in the rostrolateral prefrontal cortex, a region that is specifically linked to metacognitive ability (Pinkham, Klein, Hardaway, Kemp, & Harvey, 2018), we hypothesized weaker Tracking Accuracy of MPs in SCZ relative to HC. Additionally, as patients disproportionately overestimate their functioning and often deny that they have a mental illness (Bedford & David, 2014; Dickerson, Ringel, & Parente, 1997; Moritz et al., 2012), we anticipated larger positive Directional Bias (e.g., overestimation of positive traits) in SCZ relative to HC.
Method
Participants
All participants provided written informed consent, and the study was approved by The University of Texas at Dallas (UTD) Institutional Review Board.
Phase 1 of the study included 30 individuals with SCZ or schizoaffective disorder and 30 HCs who received monetary compensation in exchange for participating. Participants with SCZ were recruited from Metrocare Services, a nonprofit mental health services provider in Dallas County, Texas, USA. HCs were recruited through community advertisements. Groups were matched on age (p = .913), years of education (p = .411), maternal education (p = .863), paternal education (p = .146), and intellectual ability as estimated by the WRAT-3 reading subscale (p = .963). The distribution of sex, race, and ethnicity was also identical between groups. Sample characteristics are presented in Table 1.
Demographic and clinical information.

Note. HC = healthy control. SD = standard deviation. SCZ = with schizophrenia. PANSS = Positive and Negative Syndrome Scale. Symptom severity is presented as the sum of PANSS items for positive, negative, and general symptom clusters. Estimated IQ is presented as a standard score from the reading subscale of the WRAT-3.
aData unavailable for three patients and one control.
bData unavailable for seven patients and four controls.
For both groups, exclusion criteria were (1) presence or history of pervasive developmental disorder or mental retardation by DSM-IV criteria, (2) presence or history of medical or neurological disorders that may affect brain function (e.g., seizures), (3) presence of sensory limitation including visual or hearing impairments that interfere with assessment, (4) no proficiency in English, (5) presence of substance abuse in the past month, (6) presence of substance dependence not in remission for the past 6 months, and (7) age under 18 or over 45. Furthermore, controls could not meet criteria for any major DSM-IV Axis I or II disorders. Participants with SCZ could not have any psychiatric hospitalizations within the 2 months leading up to participation and had to be on a stable medication regimen for a minimum of 6 weeks, with no dose changes for a minimum of 2 weeks. Diagnoses were confirmed with the Mini International Neuropsychiatric Interview (Sheehan et al., 1998) and the Structured Clinical Interview for DSM Disorders Psychosis Module (First, Spitzer, Gibbon, & Williams, 2002), and symptom severity was assessed with the Positive and Negative Syndrome Scale (PANSS) (Kay, Opler, & Fiszbein, 1992).
For Phase 2 of the study, 120 undergraduate students (50 males; mean age: 23.42, standard deviation (SD) = 5.10) were recruited and received class credit for participating. Exclusion criteria for Phase 2 were (1) presence or history of self-reported medical or neurological disorders that may affect brain function (e.g., seizures), (2) presence of sensory limitation including visual or hearing impairments that interfere with assessment, (3) no proficiency in English, and (4) age under 18 or over 45.
Measures
Videotaped “Get To Know You” conversation
The videotaped task was a 5-min conversation between each Phase 1 participant and an experimenter. Participants were told that the purpose of the conversation was to get to know one another and that they could discuss anything. All Phase 1 participants conversed with the same experimenter who was blind to their diagnostic status, asked questions from a set of memorized prompts (e.g., “What do you usually do for fun?”), offered concise answers to questions, and allowed the participant to talk a majority of the time. Letzring, Wells, and Funder (2006) found that interjudge consensus, agreement between self-perceptions and others’ perceptions, and knowledge of conversation partner were maximized by using conversations with the instruction to get to know one another, compared to conversations with no instructions and more structured tasks. Consensus was also increased by longer conversation times.
Mini international personality item pool
The Mini international personality item pool (Mini-IPIP) (Donnellan, Oswald, Baird, & Lucas, 2006) is a 20-item version of the International Personality Item Pool—Five-Factor Model measure (Goldberg, 1999). Its five domains, each consisting of 4 items, are Extraversion (e.g., “I am the life of the party”), Agreeableness (e.g., “I feel others’ emotions”), Conscientiousness (e.g., “I like order”), Neuroticism (e.g., “I get upset easily”), and Openness to Experience (e.g., “I have a vivid imagination”). Here, Openness to Experience comprises ratings of intelligence and imaginativeness. Participants indicate how accurate each statement is in describing them on a scale from 1 = Very inaccurate to 5 = Very accurate, with higher scores indicating more presence of the trait. An analysis using a large, nationally representative sample of young adults found that the Mini-IPIP had good reliability, acceptable validity, and a five-factor structure (Baldasaro, Shanahan, & Bauer, 2013). In addition, Credé, Harms, Niehorster, and Gaye-Valentine (2012) found that, among 6 measures with 20 or fewer items, the Mini-IPIP had the highest criterion-related validity and external validity.
Procedure
In Phase 1, participants first engaged in the videotaped “Get to Know You” conversation with the trained experimenter. Immediately thereafter, they completed the Mini-IPIP with the aim of predicting how unfamiliar strangers who watch their videotape would rate them. Participants additionally indicated the extent to which their everyday personalities were accurately represented in the conversation on a scale from 0 = Not at all accurate to 10 = Extremely accurate. These ratings were collected to ensure that groups did not differ on how well their everyday personalities were portrayed during the conversation, as such differences could disproportionately affect the MPs of each group and confound subsequent results.
In Phase 2, raters each watched six Phase 1 videos, three of patients and three of controls. Thus, each video was watched and rated by 12 undergraduate raters. Thirty pairs of Phase 1 videos were created with one patient and one control matched on sex, race/ethnicity, and age; pairs were then randomly assigned to 10 groups consisting of 3 pairs each. Within each group, the order of videos was counterbalanced using a balanced Latin Square design, so every 10th Phase 2 rater watched the same group of videos but in a different order. After seeing a video, Phase 2 raters completed the Mini-IPIP for how they perceived the participant in that video. No Phase 2 raters reported any acquaintance with people whom they viewed in the Phase 1 videotapes.
Statistical analyses
Phase 1 MPs were averaged across the 4 items of each Big Five domain on the Mini-IPIP to yield one score per domain. Phase 2 perceptions were averaged across the 12 undergraduates who rated each video and across the 4 items of each Big Five domain; these ratings served as “The Truth” to which Phase 1 MPs were compared for accuracy and bias. Consistency was high among Phase 2 raters with Intraclass Correlation Coefficients (ICCs) > .86 for each Big Five domain. All analyses were run separately for each Big Five domain and based on The Truth and Bias Model of Judgment (West & Kenny, 2011). Here, linear regression models predict Phase 1 MPs as a function of The Truth, subtracting The Truth’s grand mean from Phase 1 MPs and The Truth (i.e., centering them with The Truth’s mean). Thus, the dependent variable is the difference between individual Phase 1 MPs and the average value of The Truth, and the intercept is the predicted value of this difference at average levels of The Truth. We evaluated regression diagnostics for each model (e.g., normality of residuals, presence of outliers), and note any instances of problems and their consequences throughout the text. Interested readers can access copies of the data, IPIP questionnaires, and syntax for the analyses on the Open Science Framework page for this project: https://osf.io/jmx6f/.
Discrepancy scores (e.g., Mark’s MP minus The Truth for Mark) are often used as outcome variables in accuracy research (e.g., Sabbag et al., 2012); however, despite their ubiquity, they have received some criticism for their methodological limitations (Cronbach, 1958; Edwards, 1994; Johns, 1981; Wall & Payne, 1973). For these reasons, we utilized the Truth and Bias Model of Judgment (West & Kenny, 2011), which allows for the simultaneous examination of Tracking Accuracy (the linear association between the judgment and the truth) and Directional Bias (the mean-level difference between the judgment and the truth). In addition, the model permits researchers to easily investigate moderators of Directional Bias and Tracking Accuracy, such as diagnostic status. The model also accommodates the investigation of additional sources of bias in MPs, such as assumed similarity.
We initially estimated baseline levels of Directional Bias and Tracking Accuracy in participants’ MPs of the Big Five traits by computing Cohen’s ds (i.e., the mean-level difference between participants’ Phase 1 MPs and the Truth divided by the average of the two standard deviations across the two measures) and correlations (i.e., the zero-order Pearson correlation between participants’ Phase 1 MPs and the Truth), respectively. We then investigated participants’ diagnostic status as a moderator of Directional Bias and Tracking Accuracy by specifying models that predicted Phase 1 MPs as a function of The Truth, Group (effect codes: SCZ = 1; HC = −1), and The Truth × Group interaction. Here, Tracking Accuracy (i.e., the degree to which The Truth predicts Phase 1 MPs) was assessed by the regression coefficient for The Truth (i.e., the change in Phase 1 MPs expected for every unit increase in The Truth), and The Truth × Group interaction assessed group differences in Tracking Accuracy. Directional Bias (i.e., the signed difference between individual MPs and the average value of The Truth) was assessed by the intercept such that a positive intercept shows that Phase 1 MPs overestimated The Truth on average, whereas a negative intercept shows that Phase 1 MPs underestimated The Truth on average. The group effect assessed group differences in Directional Bias (i.e., whether the difference between Phase 1 MPs and The Truth’s grand mean differed by group). Subsequent analyses investigated participants’ assumed similarity to others as an additional source of bias in their MPs of the Big Five traits. Finally, we performed post hoc analyses to evaluate whether additional variables related to metacognition may help to explain the results. To account for multiple comparisons, we adopted an alpha level of .01 for all tests. Findings not meeting this threshold, but with p values below .05, are reported as marginally significant.
Power analyses
We performed power analyses using the Monte Carlo simulation capabilities of Mplus version 7.4 to determine our ability to detect our principal effects of interest across two sets of analyses: (a) basic Truth and Bias model analyses (i.e., models without moderators) and (b) Truth and Bias model analyses containing moderators of Tracking Accuracy and Directional Bias. All analyses assumed a sample size of 60 participants and used 5,000 replications to evaluate our levels of power to detect small-, medium-, and large-sized effects. Broadly speaking, the analyses suggested that we should have adequate-to-high levels of power to detect medium effects (power estimates ranging from .68 to .97) and large effects (all power estimates = .99) but low levels of power to detect small effects (power estimates ranging from .13 to .35).
Results
Phase 1 participants thought that the conversations accurately portrayed their everyday personalities (M = 8.13, SD = 2.41, scale from 0 = Not at all accurate to 10 = Extremely accurate), with no difference (p = .597) between SCZ (M = 8.30, SD = 2.34) and HC (M = 7.97, SD = 2.51). Figure 1 presents mean and SDs for Phase 1 MPs and The Truth, and Table 2 presents the baseline effect sizes for Directional Bias and Tracking Accuracy in participants’ MPs of the Big Five traits. For illustrative purposes, Figure 2 presents the distribution of signed discrepancy scores. As can be seen in Table 2, participants significantly overestimated others’ perceptions of their openness to experience, conscientiousness, and agreeableness and underestimated others’ perceptions of their neuroticism. Moreover, with the exception of extraversion, estimates of Directional Bias were typically medium in size. Table 2 further shows that baseline levels of Tracking Accuracy were quite strong across all the traits.
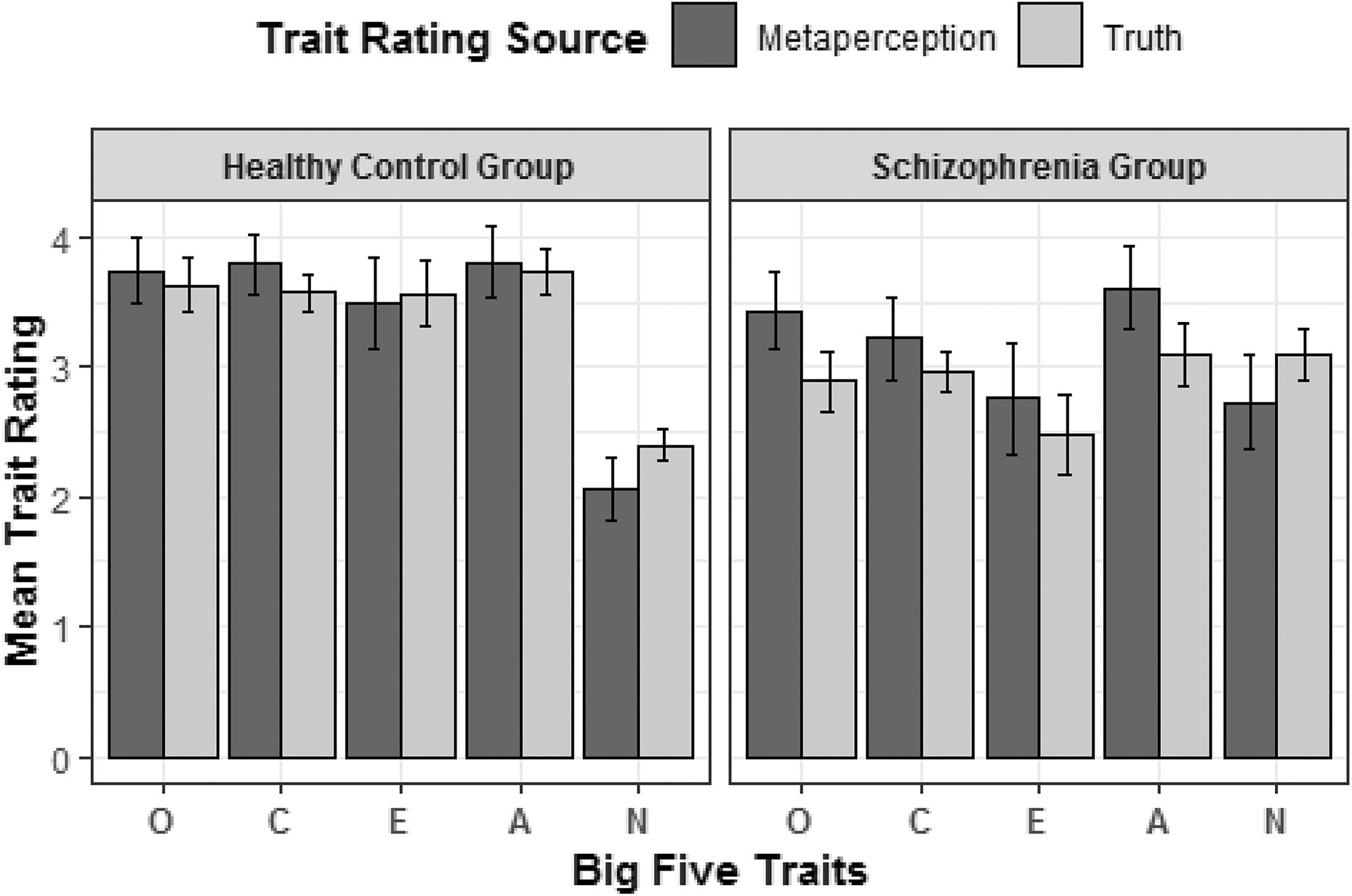
Average values for The Truth and Phase 1 MPs between groups. Error bars represent 95% CIs. O = Openness. C = Conscientiousness. E = Extraversion. A = Agreeableness. N = Neuroticism. CI = confidence interval; MP = metaperception.
Baseline effect sizes for Directional Bias and Tracking Accuracy in MPs of Big Five traits.

Note. MP = metaperception. CI = confidence interval. Unbiased Cohen’s ds (i.e., d unb’s; Hedges & Olkin, 1985) were used to estimate the magnitude of Directional Bias; these estimates use the average of the standard deviations across the two measures as the standardizer. Pearson correlations were used to estimate the magnitude of Tracking Accuracy.
**p < .01.

Discrepancy scores between MPs and other ratings of personality for each group. MP = metaperception.
Diagnostic status as a moderator of Tracking Accuracy and Directional Bias
Table 3 presents the regression coefficients for the Truth and Bias Model analyses with diagnostic status as a moderator of Tracking Accuracy and Directional Bias. As can be seen, the Truth × Group interaction terms were statistically significant for three of the domains: Openness to Experience, Conscientiousness, and Agreeableness. Follow-up simple slopes analyses showed that Tracking Accuracy was stronger in HC than in SCZ for those traits: Openness to Experience (HC: b = 1.21, 95% confidence interval (CI) [0.87, 1.55], SE = 0.17, p < .001, β = 1.12, 95% CI [0.80, 1.44]; SCZ: b = 0.59, 95% CI [0.29, 0.89], SE = 0.15, p < .001, β = 0.55, 95% CI [0.26, 0.83]), Conscientiousness (HC: b = 1.51, 95% CI [0.86, 2.17], SE = 0.33, p < .001, β = 0.95, 95% CI [0.54, 1.36]; SCZ: b = 0.34, 95% CI [−0.21, 0.90], SE = 0.28, p = .22, β = 0.22, 95% CI [−0.13, 0.56]), and Agreeableness (HC: b = 1.27, 95% CI [0.70, 1.84], SE = 0.28, p < .001, β = 1.00, 95% CI [0.55, 1.45]; SCZ: b = 0.29, 95% CI [−0.11, 0.70], SE = 0.20, p = .15, β = 0.23, 95% CI [−0.09, 0.55]).
Regression models for diagnostic status as a moderator of Tracking Accuracy and Directional Bias in MPs of Big Five traits.

Note. MP = metaperception. CI = confidence interval. SE = standard error. b represents unstandardized coefficients. Directional Bias is denoted by the intercept, with group differences in Directional Bias denoted by the regression coefficient for Group. Tracking Accuracy is denoted by the regression coefficient for Truth, with group differences in Tracking Accuracy denoted by the regression coefficient for Truth × Group.
aThere was evidence of two influential observations. After removing these two observations, the intercept became marginally significant (b = 0.23, 95% CI [0.02, 0.44], SE = .10, p = .0305) as did the effect of Group (b = 0.24, 95% CI [0.03, 0.45], SE = .10, p = .0232).
bThere was some evidence of heteroscedasticity, χ2 (1) = 7.23, p = .007. Using sandwich estimators to account for heteroscedasticity resulted in a marginally significant interaction between Truth and Group, b = −0.24, SE = 0.11, p = .035.
cThere was evidence of two influential observations. After removing these two observations, the intercept became nonsignificant (b = −0.20, 95% CI [−0.48, 0.08], SE = .14, p = .17).
*p < .05; **p < .01.
Groups were also marginally significantly different in their mean-level Directional Bias for Openness. Results revealed that the SCZ group significantly overestimated their level of Openness (intercept = 0.40, 95% CI [0.18, 0.62], SE = 0.11, p < .001). In contrast, the HC group did not display any significant mean-level Directional Bias (intercept = 0.04, 95% CI [−0.19, 0.27], SE = 0.11, p = .72), suggesting that the overall effect was driven by primarily by the SCZ group.
Assumed similarity as an additional source of bias in MPs
We next sought to determine whether patients’ MPs were less accurate and/or more biased because they thought that Phase 2 raters would view them the same way they view themselves generally. To this end, before the 5-min conversation, Phase 1 participants rated how they viewed their own everyday personality with the Mini-IPIP, the same questionnaire used for the MPs and Phase 2 ratings. A Truth and Bias regression model with these general self-perceptions and The Truth as predictors of MPs was conducted for each of the Big Five traits (see Table 4). Results revealed statistically significant evidence of assumed similarity for openness (β = 0.51, 95% CI [0.41, 0.62]), extraversion (β = 0.45, 95% CI [0.25, 0.65]), and agreeableness (β = 0.59, 95% CI [0.41, 0.77]), and marginally significant evidence for neuroticism (β = 0.43, 95% CI [0.09, 0.78]) and conscientiousness (β = 0.39, 95% CI [0.02, 0.76]).
Regression models for assumed similarity as an additional source of bias in MPs of Big Five traits.
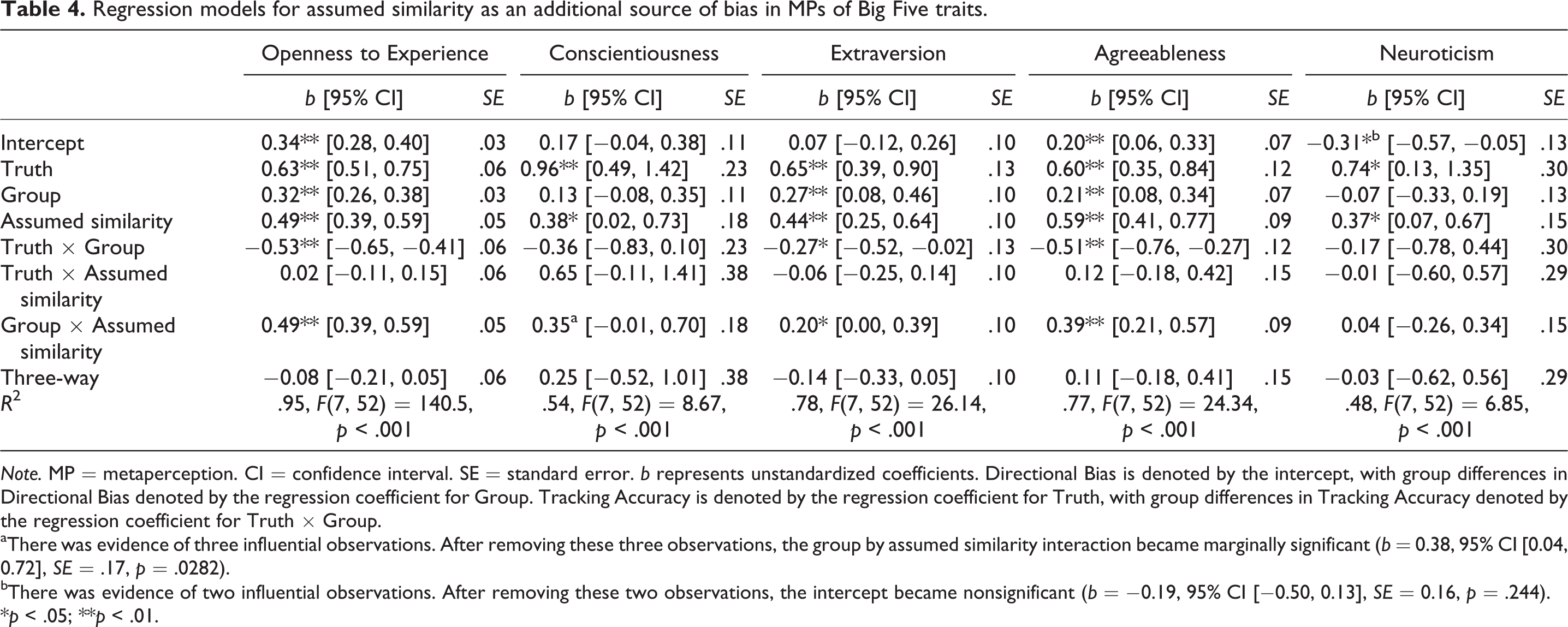
Note. MP = metaperception. CI = confidence interval. SE = standard error. b represents unstandardized coefficients. Directional Bias is denoted by the intercept, with group differences in Directional Bias denoted by the regression coefficient for Group. Tracking Accuracy is denoted by the regression coefficient for Truth, with group differences in Tracking Accuracy denoted by the regression coefficient for Truth × Group.
aThere was evidence of three influential observations. After removing these three observations, the group by assumed similarity interaction became marginally significant (b = 0.38, 95% CI [0.04, 0.72], SE = .17, p = .0282).
bThere was evidence of two influential observations. After removing these two observations, the intercept became nonsignificant (b = −0.19, 95% CI [−0.50, 0.13], SE = 0.16, p = .244).
*p < .05; **p < .01.
Table 4 also shows that group status significantly moderated the degree of assumed similarity for openness and agreeableness. The effect for extraversion was also marginally significant. Simple slope analyses indicated that whereas SCZ demonstrated assumed similarity for openness (b = 0.98, 95% CI [0.88, 1.08], SE = 0.05, p < .001, β = 1.03, 95% CI [0.92, 1.13]), extraversion (b = 0.64, 95% CI [0.36, 0.92], SE = .14, p < .001, β = 0.65, 95% CI [0.37, 0.94]), and agreeableness (b = 0.98, 95% CI [0.77, 1.20], SE = .11, p < .001, β = 0.98, 95% CI [0.77, 1.20]), the HC group did not (openness: b = −0.00, 95% CI [−0.17, 0.17], SE = 0.08, p = .996, β = −0.00, 95% CI [−0.18, 0.18]; extraversion: b = 0.24, 95% CI [−0.03, 0.52], SE = .14, p = .079, β = 0.25, 95% CI [−0.03, 0.53]; agreeableness: b = 0.20, 95% CI [−0.08, 0.49], SE = .14, p = .16, β = 0.20, 95% CI [−0.08, 0.49]).
Post hoc analyses
Given the heterogeneity of SCZ (Maglione, Vahia, & Jeste, 2015), we conducted additional, post hoc analyses in an attempt to explain (1) what might underlie patients’ less accurate MPs and (2) the variation of overestimation and underestimation (i.e., Bias) in patients. Here, depressive symptoms, insight into illness, and Theory of Mind were of interest, as previous work has shown that each is related to self-assessment in SCZ (Chakraborty & Basu, 2010; Harvey, Twamley, Pinkham, Depp, & Patterson, 2017; Lysaker, Hasson-Ohayon, Kravetz, Kent, & Roe, 2013). Depression was assessed via the total score from the self-report Beck Depression Inventory-II (BDI-II) (Beck, Steer, Ball, & Ranieri, 1996), insight into illness was assessed via the PANSS G12 item, and Theory of Mind was assessed via the total score from the performance-based TASIT (McDonald, Flanagan, Rollins, & Kinch, 2003), all of which were administered in the same study session as the Phase 1 MPs. Three Truth and Bias regression models were run separately for the BDI-II, PANSS G12 item, and TASIT, with HC participants also included in the BDI-II and TASIT analyses.
Due to large group differences in depression and theory of mind, analyses including these variables as moderators of accuracy and bias tended to have problems with multicollinearity. With this limitation in mind, results revealed that Tracking Accuracy and Directional Bias were largely unrelated to depression, insight into illness, and Theory of Mind (all ps > .08). One exception was a marginally significant association between higher depression scores and overestimation of neuroticism (b = 0.06, 95% CI [0.002, 0.11], SE = .03, p = .04). In addition, after removing two influential observations in another analysis, we found that participants with greater levels of insight into their illness displayed significantly more overestimation (b = 0.42, 95% CI [0.18, 0.67], SE = 0.12, p = .002) in their MPs of openness but also marginally improved Tracking Accuracy (b = 0.45, 95% CI [0.07, 0.83], SE = 0.18, p = .02). Although relationships did not differ between groups on the BDI-II and TASIT for any Big Five domain (all ps > .08), there was one case in which adjusting for the presence of heteroscedasticity resulted in a marginally significant three-way interaction between Truth, Group, and TASIT for MPs of conscientiousness (b = 0.09, SE = 0.04, p = .017).
Discussion
We examined the ability of individuals with SCZ to understand how others view their personalities (i.e., MPs). After completing a “get to know you” conversation with an experimenter, participants with SCZ and HCs predicted how strangers who watch their conversations would rate them on the Big Five traits, and these MPs were compared to strangers’ actual ratings of them for accuracy and bias. Here, the accuracy and bias of the MPs comprised two components: (1) Tracking Accuracy, the extent to which strangers’ perceptions predict MPs and (2) Directional Bias, the signed difference between individual MPs and the average of strangers’ perceptions. Participants with SCZ generally exhibited more inaccurate MPs, as Tracking Accuracy was weaker in SCZ than in HC for Openness to Experience, Conscientiousness, and Agreeableness. Directional Bias also appeared larger in SCZ than in HC for Openness to Experience such that patients overestimated strangers’ perceptions more than controls did, although this difference did not survive our stringent family-wise error correction. Our results suggest that the robust impairments of self-awareness and introspective knowledge in SCZ extend to personality perception, which may be relevant to the social dysfunction common in people with SCZ.
Given the extensive literature on reduced social understanding of the self and others in SCZ (Brüne et al., 2011; Dimaggio & Lysaker, 2015; Lysaker et al., 2013; Mitchell et al., 2012; Penn, Sanna, & Roberts, 2008), our findings of impaired personality MP in SCZ were anticipated. They also are consistent with and build upon those of Klein et al. (2013), in which the correlation between targets’ personality self-perceptions and relatives’ ratings of targets was weaker in SCZ than in HC. Fisher, McCoy, Poole, and Vinogradov (2008) posited that the impaired metacognitive system in the social domain “provide[s] a parsimonious explanation for the disturbances in the sense of self and other that characterize schizophrenia” (p. 1465). To the best of our knowledge, the present study is the first to indicate that people with SCZ are poorer at understanding how others view their personalities, which may be a unique product of this metacognitive system implicated in forming less accurate mental representations of the self and others. Indeed, our results support the distinctiveness of personality MPs from some of the other forms of metacognition, as Tracking Accuracy and Directional Bias were unrelated to insight into illness and Theory of Mind. This suggests not only that metaperceiving personality entails unique abilities (e.g., awareness of one’s own behavior and what it implies about one’s disposition) but also that improvements in personality MP in SCZ likely could not arise by simply targeting metacognition more broadly.
Such improvement, however, does not appear warranted for all traits, as MPs were less accurate in our participants with SCZ only for those traits higher in evaluativeness (i.e., when social values largely influence a trait’s desirability; John & Robins, 1993)—Openness to Experience, Conscientiousness, and Agreeableness. Self-serving positivity biases (Dunning, 1999; Kruger, 1999) compromise one’s ability to accurately introspect on socially desirable traits and has been demonstrated in the general population by less accurate MPs and self-perceptions for highly evaluative traits (Carlson & Kenny, 2012; Vazire, 2010). The finding that patients marginally overestimated Openness more than HCs suggests that individuals with SCZ may be less aware of self-serving biases and less likely to appropriately adjust for them in relevant social situations. For example, if Mark overestimates how intelligent others think he is, then he may not seek out all of the necessary experience to be a competitive applicant for employment. Such findings are also consistent with previous reports that individuals with SCZ disproportionately overestimate their cognitive and social functioning and often believe that they do not have a mental illness (Bedford & David, 2014; Dickerson et al., 1997; Moritz et al., 2012; Silberstein, Pinkham, Penn, & Harvey, 2018).
For the other highly evaluative traits, Conscientiousness and Agreeableness, patients’ and controls’ MPs tended to overestimate others’ perceptions (although not significantly so), with no group differences in this Directional Bias. For these traits, however, Tracking Accuracy was weaker in SCZ, suggesting that patients’ MPs were more discrepant from The Truth in both directions. That is, individual patients exhibited more extreme overestimation or underestimation that averaged at the group level to moderate overestimation, whereas control individuals exhibited less extreme overestimation or underestimation that also averaged at the group level to moderate overestimation (see Figure 2). It therefore appears that underestimation and overestimation of socially desirable traits occur in people with SCZ, which is consistent with research on other forms of introspective knowledge (Harvey et al., 2017; Sabbag et al., 2012).
Further analyses found that while the Tracking Accuracy and Directional Bias of MPs were not generally associated with depression, clinical insight, or mentalizing abilities, self-perceptions of personality did significantly predict MPs for each trait. This was particularly pronounced in patients, but not in controls, for Openness and Agreeableness. These findings coincide with research showing that people with SCZ tend to have difficulty creating a clear self-other distinction and understanding why others’ mental experiences may differ from their own (Hur et al., 2014; Lysaker & Lysaker, 2010; Mishara et al., 2014; Park & Nasrallah, 2014; Penn et al., 1997). They likewise coincide with research showing that people in the general population, on the other hand, are often capable of accurately understanding when their MPs should differ from their general self-perceptions (Albright et al., 2001; Albright & Malloy, 1999; Carlson et al., 2011; Carlson & Furr, 2009; Oltmanns et al., 2005; Wyer et al., 1975). This overemphasis on self-perceptions may therefore provide a mechanism for MP inaccuracies.
The current study has limitations that require consideration. First, although well matched on relevant demographic and cognitive variables, Phase 1 groups included only 30 participants each. Thus, the current investigation is insufficiently powered to detect small effects (e.g., a link between depressive symptoms and underestimation or overestimation in patients), especially with tests run at an alpha level of .01. Replication of these results is therefore warranted. Second, limitations of the study paradigm should also be considered. We restricted analyses to MPs for the Big Five traits and in the context of a brief conversation with a stranger. Future work may wish to investigate personality MPs across different contexts (e.g., understanding how a romantic partner views oneself) and different socially relevant traits (e.g., trustworthiness) in people with SCZ. It is possible that MPs may align more closely with the perceptions of others if longer or repeated interactions were used. Further, the current paradigm demonstrates impaired MP in SCZ and suggests that overreliance on self-perceptions may play a role, but the full mechanisms of this impairment remain unknown. It is possible that poor self-knowledge drives difficulties in MP, but poor personality perception may play a role as well. Additional studies should assess whether patients would differ from controls when rating how one individual (person a) would rate another individual who is not the self (person b). It may also be beneficial to concurrently examine cognitive biases that are common in SCZ (e.g., jumping to conclusions) to determine whether such biases impact self- and meta-perception.
In conclusion, we demonstrated that individuals with SCZ are generally less accurate at understanding how others view their personalities based on a conversation with a stranger. We additionally found that personality MPs appear to be distinct from some other forms of metacognition in SCZ, such as clinical insight and mental state attribution. These findings suggest that personality MP may be an important and unique component of the impaired metacognitive system that underlies social dysfunction in SCZ.
Footnotes
Authors’ note
Amy E. Pinkham and Jonathon R. Shasteen are co-first authors.
Acknowledgement
The authors would like to thank Shonaali Sarode for her assistance with data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by internal funding from the University of Texas at Dallas.