
Abstract
Objective:
In Arabic-speaking countries, most individuals with depression or obsessive–compulsive disorder (OCD) do not seek or receive evidence-based treatment due to a dearth of facilities, shame/self-stigma, or religious concerns. The feasibility and effectiveness of “Western” psychotherapeutic concepts have rarely been evaluated for Arabic-speaking populations. The present study examined the efficacy of My Metacognitive Training (myMCT), a trans-therapeutic self-help manual, in a mixed sample of participants with depression and/or OCD. We considered both participants with depression and/or OCD because a number of cognitive biases and dysfunctional beliefs are shared by the two disorders.
Method:
The myMCT manual was translated into Arabic. A total of 160 individuals with either self-reported OCD and/or self-reported depression were recruited. Individuals were assessed at baseline and then randomized either to myMCT (n = 84) or to a wait-list control condition (n = 76). Six weeks later, individuals were invited to the post assessment. The Beck Depression Inventory (BDI-II) served here as the primary outcome. Secondary outcomes were the Obsessive–Compulsive Inventory–Revised (OCI-R) and the self-rating version of the Yale-Brown Obsessive Compulsive Scale (OCD patients only). Individuals were reimbursed with a 17€ voucher.
Results:
Completion rates were similarly low in the two groups (myMCT: 37%, controls: 35%). Presumably because of the high rate of noncompletion and nonadherence (29%), the intention-to-treat analyses failed to yield a significant effect. Those who had at least started the myMCT intervention improved significantly on the BDI-II at a large effect size. A significantly larger improvement among those who had started or completed the myMCT intervention was also seen on the OCI-R at a large effect size.
Conclusions:
Individuals who studied the myMCT manual showed large improvement on the BDI-II, irrespective of their primary symptomatology. However, the results are seriously compromised by the low completion rates in both conditions. Importantly, evaluations using the same manual in other language populations (and with other background cultures) produced good to excellent retention rates. The study demonstrates that self-help manuals may not represent a suitable medium for large-scale dissemination of evidence-based self-help material in an Arab population and corroborates prior findings suggesting low adherence in this population. Whether smartphone apps and Internet interventions represent more viable alternatives than self-help manuals needs to be tested, as well as specific barriers preventing dissemination and completion in this population.
Introduction
Treatment gap in obsessive–compulsive disorder and depression
Obsessive–compulsive disorder (OCD) and depression are serious psychiatric disorders. Although effective therapies are available (see the next section), a large subgroup still does not receive (adequate) treatment due to a number of reasons, including fear of stigma, financial constraints, and poor service availability (García-Soriano, Rufer, Delsignore, & Weidt, 2014; Kohn, Saxena, Levav, & Saraceno, 2004; Marques et al., 2010; Moritz, Schröder, Meyer, & Hauschildt, 2013; Rebello, Marques, Gureje, & Pike, 2014; Schwartz, Schlegl, Kuelz, & Voderholzer, 2013; Stein, 2002; Veldhuis et al., 2012; Wahl, Ertle, Bohne, Zurowski, & Kordon, 2011). If treatment is sought at all, initiation of proper therapy is often delayed by many years. The situation is especially grave in low- and middle-income countries (Andrade et al., 2013; Eaton et al., 2011; Kohn et al., 2004; World Health Organization, 2011).
Narrowing the treatment gap
Cognitive-behavioral therapy (CBT) and variants thereof have proved effective in OCD (Olatunji, Davis, Powers, & Smits, 2013; Öst, Havnen, Hansen, & Kvale, 2015) as well as depression, notwithstanding that, at least for depression, the effects of CBT might have been overestimated and are less strong in more recent studies (Cuijpers et al., 2013; Johnsen & Friborg, 2015). Yet, as mentioned, these treatments are only available to a minority of patients. The treatment gap may be narrowed with low-threshold interventions such as bibliotherapy (self-help books; see the next section), remote therapy (Wootton, 2016), interactive Internet interventions, and self-help websites (Dèttore, Pozza, & Andersson, 2015; Mataix-Cols & Marks, 2006; McIngvale, Bakos-Block, Hart, & Bordnick, 2012). The present study is concerned with bibliotherapy. In our view, on a global scale such a medium has some advantages over online tools as not all individuals in lower income countries have a smartphone or a personal computer in their homes. As we have argued previously (Moritz et al., 2018), e-books and pdf documents are often less costly than commercial online programs and can be easily downloaded as well as printed (e.g., in outpatient facilities or offices of nongovernmental organizations). If registration is mandatory, online devices have lingering problems with data confidentiality, especially in countries with a poor information technology infrastructure and nonadherence to democratic standards (Lawlor-Savage & Prentice, 2014). Although a recent meta-analysis demonstrated that effects for Internet-delivered interventions are larger than effects for other media, the effectiveness of the various interventions might be equal if the content is similar (Mayo-Wilson & Montgomery, 2013).
Guided and unguided treatment concepts (i.e., self-help programs such as online portals designed for use with or without the assistance of a therapist), which are mainly derived from research in Western societies, have rarely been examined rigorously as to their efficacy in other cultures. It is thus unclear whether evidence obtained from trials mainly conducted in Europe or North America (Mayo-Wilson & Montgomery, 2013) can be transposed to other parts of the world (for a discussion, see Gearing et al., 2013).
CBT-based self-help interventions yield good results in depression, OCD, and other disorders, especially when set up as guided interventions, and they sometimes equal results obtained with face-to-face therapy (Andersson et al., 2012; Dèttore et al., 2015; Herbst et al., 2012; Karyotaki et al., 2017; Mahoney, Mackenzie, Williams, Smith, & Andrews, 2014; Moritz, Kersten, Dietl, Aardema, & O’Connor, 2015; Richards & Richardson, 2012; Tolin et al., 2007; Wootton, Dear, Johnston, Terides, & Titov, 2013). The present study investigated whether My Metacognitive Training (myMCT), a self-help manual that has been positively evaluated in German-, English-, and Russian-speaking populations (Hauschildt, Schröder, & Moritz, 2016; Moritz et al., 2011, 2018; Moritz, Stepulovs et al., 2016), is effective in an Arab population, given that many parts of the Arabic-speaking world have reservations about “the West” in general (Pew Research Center, 2006) and psychological interventions in particular (Gearing et al., 2013).
myMCT: A self-help manual for OCD
We evaluated the Arabic version of the treatment manual myMCT (Moritz & Hauschildt, 2011, 2016), which is available in several other languages as well. The manual and worksheets (see the Method section) can be downloaded at no cost via www.uke.de/mymct. The intervention takes an integrative (trans-therapeutic) approach with a clear focus on metacognitive techniques that imparts to patients metacognitive knowledge about cognitive phenomena (e.g., thoughts cannot be fully controlled; thought–action fusion is impossible) and corrects false beliefs (e.g., the belief that thought suppression helps to dilute negative cognitions). This approach is derived from and inspired by metacognitive training (MCT) for psychosis, which aims at “straightening” the cognitive biases of psychosis such as jumping to conclusions and overconfidence (Moritz et al., 2014). MCTs have been developed for different disorders (e.g., depression, borderline personality disorder), each targeting different biases that are implicated in the pathogenesis of the target psychopathology. At the core of myMCT are the six cognitive biases (e.g., perfectionism and inflated responsibility) and dysfunctional coping patterns (e.g., thought suppression) highlighted by the Obsessive–Compulsive Working Group as likely pathogenetic mechanisms of OCD (Obsessive Compulsive Cognitions Working Group, 1997, 2003, 2005). One chapter also addresses the false metacognitive belief that OCD is an incurable brain disorder that is not amenable to psychotherapeutic treatment (Hauschildt, Jelinek, Randjbar, Hottenrott, & Moritz, 2010). In addition, myMCT incorporates techniques from different therapeutic “schools,” such as exposure with response prevention (ERP), the most effective technique for OCD (Rosa-Alcazar, Sanchez-Meca, Gomez-Conesa, & Marin-Martinez, 2008; for a study on self-directed ERP, see Tolin et al., 2007), acceptance and commitment therapy (ACT; Hayes, Masuda, & DeMey, 2003), and mindfulness-based approaches (Hofmann & Asmundson, 2008; Kahl, Winter, & Schweiger, 2012; Öst, 2014). The manual also conveys the metacognitive strategy of association splitting (Moritz & Jelinek, 2007), which has been successfully evaluated as a single technique (Moritz, Jelinek, Klinge, & Naber, 2007; Moritz & Russu, 2013). The association-splitting technique teaches patients how negative thoughts may turn into strong obsessions that increasingly dominate consciousness. Patients are familiarized with the cognitive principle of the “fan effect” and are encouraged to generate neutral and positive associations for OCD-laden cognitions to weaken the associative strength of OCD cognitions (e.g., black–chocolate rather than black–death).
myMCT was developed as an integrative treatment approach as most researchers agree that OCD is a multifaceted and multicausal disorder (Abramowitz, Taylor, & McKay, 2009), which may explain why even the most evidence-based single technique, ERP, is not efficacious in all patients (Abramowitz et al., 2012). Moreover, because preferences, specific needs, and worries vary across individuals, we aimed to provide a “tool kit” for readers to choose from. As some of the approaches amalgamated in myMCT derive from traditions with different (and sometimes opposing) treatment recommendations (Hofmann & Asmundson, 2008), we aimed to provide a synergic combination of the techniques in order not to confuse readers. To illustrate, we agree with Needleman and Cushman (2010), who argue that change-oriented CBT and acceptance-oriented ACT share important features and can thus be effectively combined despite remaining differences (“the goal of traditional CBT is to reduce symptoms, whereas, the goal of ACT is valued living irrespective of symptoms,” p .168). We reconciled CBT and ACT using the following philosophy: “If you cannot change the thought, accept the fact that you have the thought and realize that it is a thought only.”
Empirical evidence for the efficacy of myMCT
Four randomized controlled studies on the myMCT have been conducted so far (N = 86–128 participants). For the beta version and the first edition, the effects of the treatment were most convincing for obsessive thoughts at a medium to strong effect size, while the effects on compulsive behavior are less established (Hauschildt et al., 2016; Moritz et al., 2011; Moritz, Stepulovs et al., 2016). The manual has therefore been recently complemented by exercises targeting compulsions. A recent study on 70 patients showed a good retention rate (80%) as well as large effect sizes for both obsessive and compulsive symptoms on the Yale-Brown Obsessive Compulsive Scale (Y-BOCS; see Methods) for myMCT relative to the control condition (Moritz et al., 2018). Depression and cognitive biases also declined and (metacognitive) knowledge acquisition was enhanced. Interestingly, poor insight emerged as a risk factor for nonresponse. To improve adherence, the third edition of the manual aims to enhance motivation for change by various exercises (e.g., writing a letter to one’s disorder, imagining overarching life values and goals). A recent meta-analysis shows that unguided myMCT exerts an average effect size of .40 (Hedges’ g; Philipp et al., 2018) relative to control conditions, which is slightly higher than for other unguided self-help interventions (Pearcy, Anderson, Egan, & Rees, 2016).
Mental health in Arab countries
Results of studies on treatment compliance in Arab countries are mixed. While one study found better medication adherence in Arab patients with hypertension (Al-Ramahi, 2015) when indirectly compared to a U.S. population, some studies suggest that adherence to evidence-based (medical) treatment is lower among Arab people. This finding has been linked with preference for “traditional therapy” and expectations of severe side effects (Yoel et al., 2013). Interestingly, low adherence to treatment and preventive medical approaches have also been found among Arabs who have immigrated to the U.S. (Talaat, 2015).
Gearing and colleagues (2013) posit that efficacious psychosocial evidence-based interventions may fail when adapted from one culture to another. Translation necessitates a deep understanding of the respective culture (including within-culture differences), established practices, and obstacles. In their systematic review encompassing 22 psychosocial or mental health studies in Middle East Arab countries, they identified more barriers (68%) than promoters (32%) to the effective translation and adaptation of empirically supported psychosocial interventions. Poor or questionable acceptability of the intervention within the cultural context (54%), community and system difficulties (27%), and problems with clinical engagement processes (19%) were noted as the most frequent barriers.
In Arab countries with a predominantly Muslim population, mental disorders are often attributed externally to the will of God, divine punishment, evil spirits, or sorcery (Gearing et al., 2013). Common barriers to treatment are a lack of general public awareness of mental illness as well as psychosocial treatment in Arab countries (Al-Darmaki, Thomas, & Yaaqeib, 2016; Eapen & Ghubash, 2004; Karam et al., 2006), personal financial constraints (Eapen & Ghubash, 2004; Karam et al., 2006; Murray et al., 2006), gender norms that impede women’s access to health services (Al-Krenawi & Graham, 1999), and poor local transportation (Eapen & Ghubash, 2004). Furthermore, social shame is strongly associated with mental illness (Eapen & Ghubash, 2004; Karam et al., 2006) and with the utilization of mental health services (Eapen & Ghubash, 2004; Shalhoub-Kevorkian, 2005). Families of individuals with mental illness or those seeking treatment are at risk of diminishing their social status in their community (Shalhoub-Kevorkian, 2005). Treatment from religious and traditional healers is perceived as less stigmatizing (Al-Krenawi & Graham, 1999; Wahass & Kent, 1997). In a recent study on Emirati college students, social stigma represented the strongest barrier to seeking help for mental health problems. Many students endorsed religious practices to cope with mental health problems and to maintain mental health (Al-Darmaki et al., 2016). “Westernized” professional mental health services are often viewed as not respecting Arab values (Al-Krenawi & Graham, 1999; Al-Krenawi, Graham, Al-Bedah, Kadri, & Sehwail, 2009; Savaya, 1998). Initial engagement of Arabs with mental health services is accordingly low.
The most recent WHO Mental Health Atlas that includes country profiles (World Health Organization, 2014) shows that psychiatric treatment in Arab countries is tenuous. Even in high-income countries such as Qatar, there are only 2.95 psychiatrists per 100,000 people compared to 12.4 in the U.S. (in Iraq [upper-middle income]: 0.4; in Jordan [upper-middle income]: 0.51; in Syria [lower-middle income]: 0.0 per 100,000 people). For psychologists, the discrepancy is even greater (U.S.: 29.62; Qatar: 1.28; Iraq: 0.1; Jordan: 0.27; Syria: 0.12 per 100,000 people). The U.S. has 648 psychiatric hospitals, but there is only one in Qatar (Iraq: 3; Jordan: 3; Syria: 5). For psychiatric units in general hospitals, the discrepancy is also large (US.: 1,170; Qatar: 0; Iraq: 22; Jordan: 3; Syria: 3). Overall, the budget for mental; health in the Arab world is low (Okasha, Karam, & Okasha, 2012).
To conclude, the mental health infrastructure in Arab countries is poor, especially in rural areas and areas affected by armed conflicts. In these areas, self-help interventions are perhaps the only available treatment. Yet, despite examples of successful implementation of CBT-oriented mental health interventions in Arab countries (Hamdan-Mansour, Puskar, & Bandak, 2009; Knaevelsrud, Brand, Lange, Ruwaard, & Wagner, 2015), reservations concerning evidence-based (Western) treatment remain strong.
Shared cognitive biases in OCD and depression
Depression and OCD are closely related, and depression is the most frequent comorbid disorder in OCD (56%; Rickelt et al., 2016). It thus comes to no surprise that they share a number of important cognitive and affective biases as well as dysfunctional coping styles such as thought suppression and rumination when dealing with negative emotions and low self-esteem (Abramowitz, Storch, Keeley, & Cordell, 2007; Brown, Antony, & Barlow, 1992; Dar & Iqbal, 2015; Exner, Martin, & Rief, 2009; Ghamari Kivi, Mohammadipour Rik, & Sadeghi Movahhed, 2013; Halvorsen et al., 2015; Hansmeier, Exner, Rief, & Glombiewski, 2016; Hezel & McNally, 2016; Jacoby, Leonard, Riemann, & Abramowitz, 2014; Moradi, Fata, Ahmadi Abhari, & Abbasi, 2014; Moritz, Jahns et al., 2016; Motivala et al., 2018; Shaw, Carbonella, Arditte Hall, & Timpano, 2017; Sun, Zhu, & So, 2017; Yap, Mogan, & Kyrios, 2012). These cognitive biases are targeted in the treatment of both depression (e.g., Jelinek, Otte, Arlt, & Hauschildt, 2013) and OCD (e.g., Jelinek, Moritz, & Hauschildt, 2017). Clark (2004) postulates that intrusive thoughts in patients with OCD often lead to depressive cognitions. For example, when a patient with OCD thinks he has to control an intrusive thought, this may trigger worry and ruminative thinking as a strategy for dealing with the distressing thought. In line with this, an influential cognitive model of obsessions (Rachman, Thordarson, Shafran, & Woody, 1995) suggests that when patients with OCD have shameful obsessions, they see themselves as having poor moral values. This may lead to cognitive biases that are typical for patients with depression, such as a negative self-view and rumination as well as negative self-interpretations. Therefore, it is plausible that some treatments for depression may be helpful for patients with OCD as well (and vice versa).
The present study
For the present study, we addressed the question raised in our last trial on myMCT (Moritz et al., 2018) regarding whether culturally adapted translations of the manual are feasible and efficacious in nonindustrialized countries. We chose to translate the myMCT manual into Arabic because it is a world language spoken in many countries with a primarily Muslim population that often lives in areas with a poor mental health infrastructure. A self-help tool may be an alternative treatment for those who fear stigma and negative consequences when seeking face-to-face treatment for mental health problems.
We did not confine recruitment to patients with OCD for two reasons. First, some patients may not know the correct label/diagnosis of their symptoms and may experience these instead as somatic disorders (Al-Darmaki et al., 2016; Al-Krenawi, 2005; Eapen & Ghubash, 2004; Karam et al., 2006). Second, as discussed above in greater detail, depression and OCD share a number of important cognitive and affective biases as well as dysfunctional coping styles that can be addressed by the same therapeutic approach.
We hypothesized that myMCT would be equally effective with OCD and depressed patients and that satisfaction with the manual would be comparable to that of other language samples. We also explored possible moderators of change.
Method
Study design
We set up an Internet-based randomized wait-list controlled trial (the assessment was done online; the self-help training was bibliotherapeutic and conveyed via a pdf document). Participants in the intervention condition received the Arabic translation of the myMCT manual immediately after randomization, whereas participants in the wait-list condition received the manual upon completion of the post assessment. The study was set up as an unguided treatment; participants did not receive any therapeutic advice or counseling. Participants were mainly recruited via Google AdWords between October 2017 and March 2018. A lower number of participants were recruited via Facebook online forums. Study participation was anonymous. Inclusion was not restricted to particular countries, but fluency in Arabic was mandatory.
A total of 506 persons accessed the introductory webpage (multiple entries were possible), 230 exited after the first page, 11 participants declined the electronic informed consent, and 105 participants exited later in the survey. The total sample thus consisted of 160 individuals with either self-reported OCD symptoms (with or without depression, n = 68) or depression without OCD (n = 92) who completed the baseline survey and were allocated to either myMCT (n = 84) or the wait-list control group (n = 76); 36% completed the assessments 6 weeks later (treatment group: n = 31, 37%; control group: n = 27, 35%). The assessments were set up using the online software Questback/Unipark®; no IP addresses were stored. Ethical approval was obtained prior to the start of the trial.
Invitation and baseline survey
The google AdWords campaign, as well as the posts connected to the baseline survey, informed participants about the study’s rationale. Participants were guaranteed delivery of a manual either immediately or after a 6-week delay (i.e., for the wait-list control group). Only individuals 18 years or older who reported having OCD and/or depression were included, but this was not formally verified via, for example, a diagnostic telephone interview. Concurrent treatments (e.g., medication, psychotherapy) did not represent exclusion criteria. Unlike prior self-help studies on myMCT and on single concepts incorporated in myMCT such as association splitting, a financial incentive was provided (an Amazon voucher sent via e-mail with a $17 value). Moreover, all participants received another self-help manual upon completion as an incentive. Electronic informed consent was mandatory. Then, questions on demographic background (e.g., age, sex, level of education) were posed as well as questions on medical history (e.g., onset of disorder, prior experience with psychotherapy or self-help related to OCD). Next, psychopathological scales were administered (see the Measures section). As in prior studies on myMCT, we asked participants whether they had answered the questions truthfully, and we requested an e-mail address and a personal code word. Participants were then randomized to one of the two conditions (allocation was according to the date of participation as displayed in the so-called trigger e-mail). Due to the online setup of the study, concealed allocation was different from the standard case in which team members perform enrollment. Our procedure is best described as centralized assignment. The risk of bias was low as the person allocating individuals to conditions had no information about the participants other than the date they entered the study.
Intervention and post assessment
Participants in the myMCT condition were e-mailed the self-help manual and worksheets as two separate pdf attachments within 24 hr following completion of the baseline survey. The Arabic myMCT manual can be downloaded at no cost via www.uke.de/mymct. It contains 14 chapters; the translated Arabic version is 177 pages long (including 97 pictures and 26 worksheets containing exercises). We instructed participants to work through the material over the next few weeks. After 6 weeks, participants in the myMCT and the control group received a personal invitation via e-mail to take part in the post assessment. First, participants were requested to reenter the e-mail address they had used for the baseline assessment as well as their personal code word (to match pre- and post data). The same set of questionnaires was administered as before (we again asked whether patients had OCD; the Y-BOCS was administered only to those who affirmed having OCD). For those who received the manual and claimed that they had at least started to read the myMCT, we asked for their subjective appraisal. In addition, we asked about important changes in their treatment and recent incidents that might have impacted their symptomatology. Up to three reminders for participation were sent.
Measures
All measures were translated by Schaimaa Irshaid.
Beck Depression Inventory II (BDI-II)
The BDI-II (Beck, Steer, & Brown, 1996) served as the primary outcome as depression is a common denominator in both depression and OCD. The BDI-II contains 21 items that tap into cognitive, behavioral, and somatic symptoms of depression. Items have to be endorsed on a 4-point Likert-type scale. Consistent with current diagnostic criteria in the DSM-5, the assessment interval encompassed the previous 2 weeks. The psychometric properties are good (Kühner, Bürger, Keller, & Hautzinger, 2007). For the test–retest reliability of the Arabic translation, see the Results section.
Obsessive–Compulsive Inventory–Revised (OCI-R)
The OCI-R (Foa et al., 2002) served as a measure for OCD symptom severity in all participants. The OCI-R is a self-report scale capturing frequent OCD symptoms (e.g., washing, checking, ordering during the last week). Previous studies have shown good to excellent psychometric properties (Abramowitz & Deacon, 2006; Foa et al., 2002; Huppert et al., 2007). Internet administration of the scale (Coles, Cook, & Blake, 2007) has been found to be equivalent to paper-and-pencil administration. For the test–retest reliability of the Arabic translation, see the Results section.
Yale-Brown-Obsessive-Compulsive Scale (Y-BOCS)
The self-report version of the Y-BOCS (Baer, Brown-Beasley, Sorce, & Henriques, 1993; Goodman, Price, Rasmussen, Mazure, Delgado et al., 1989; Goodman, Price, Rasmussen, Mazure, Fleischmann et al., 1989) was administered to those who indicated having OCD. The Y-BOCS shows high agreement with the original interview version (Schaible, Armbrust, & Nutzinger, 2001; Steketee, Frost, & Bogart, 1996). Five items assess the severity of obsessive thoughts and compulsions. Two additional questions tap illness insight (Item 11) and avoidance (Item 12). To avoid potential misunderstandings, examples of obsessive thoughts and compulsive behavior were provided as part of the instructions (e.g., cognitive compulsions are sometimes confused by patients with obsessions; Federici et al., 2010). The questions related to the previous week. We then calculated the total score (Items 1–10). The test–retest reliability of the online version of the instrument is good (Moritz, Jelinek, Hauschildt, & Naber, 2010; Moritz & Russu, 2013). For the test–retest reliability of the Arabic translation, see the Results section.
Patient Satisfaction Questionnaire/Fragebogen zur Patientenzufriedenheit (ZUF-8)
To assess general satisfaction with the manual, we administered the ZUF-8 (Schmidt & Wittman, 2008) to those who had read the manual in part or in whole. This scale was originally derived from the Client Satisfaction Questionnaire (Attkisson & Zwick, 1982) and was adapted for a bibliotherapeutic intervention. Its psychometric properties are good (Kriz, Nübling, Steffanowski, Rieger, & Schmidt, 2008; Schmidt, Nübling, Lamprecht, & Wittmann, 1994). Furthermore, individuals who had begun to read the myMCT manual were asked for their appraisal of the intervention (e.g., usefulness, comprehensibility, symptom reduction, side effects; see Tables 3 and 4). Items had to be rated on a 4-point Likert-type scale (1 = not at all, 2 = a little, 3 = a lot, 4 = absolutely).
Strategy of data analysis
We performed an analysis of variance with time as the within-subject variable and group as the between-subject factor. For the intention-to-treat analyses (i.e., considering all patients randomized to conditions irrespective of adherence and completion status), we used multiple imputation with 100 iterations and entered all demographics listed in Table 1 and baseline psychopathological variables (BDI-II, OCI-R, Y-BOCS; see Table 2) as predictors.
Demographic and psychopathological baseline characteristics of the sample.

myMCT = My Metacognitive Training; OCD = obsessive–compulsive disorder.
Differences between the myMCT and control groups across time; per protocol and intention-to-treat analyses with means and standard errors.a

myMCT = My Metacognitive Training; ANOVA = analysis of variance; BDI-II = The Beck Depression Inventory; WL = wait-list; OCI-R = Obsessive–Compulsive Inventory–Revised; Y-BOCS = Yale-Brown Obsessive-Compulsive Scale.
a Post scores refer to raw data (not imputed).
We also looked at completer data and whether group differences occurred when comparing participants in the myMCT group who had started to read the manual versus control participants (per-protocol analysis). Potential moderators of treatment outcome were examined using the PROCESS macro by Hayes (Model 1); parameters were set to default mode.
Results
Sample characteristics and comparisons
Table 1 confirms that both groups were comparable with regard to demographic and psychopathological baseline characteristics. The sample showed OCD and depressive symptom severity on the brink of moderate–to-severe symptoms. OCI-R scores cannot be compared to prior studies since we used a 5-point Likert-type scale to allow greater variability in regard to our mixed sample. Most patients were males in their late 20s and were rather well-educated. Few participants were currently receiving medication and even fewer were receiving psychotherapy.
Group comparisons on main outcomes
The CONSORT flowchart is displayed in Figure 1. Only 36% of the participants responded to our multiple invitations to participate in the post assessment; rates were similar for both groups. Moreover, only 29% (n = 9) of the myMCT sample who responded to our invitation reported that they had read or started to read the book.

CONSORT chart diagram.
The regression models of the intention-to-treat analyses indicated a nonsignificant effect of the sample on symptom improvement (BDI-II: 0.12, p = .905; Y-BOCS: b = 2.82, p = .394; OCI-R: 0.09, p = .336). Table 2 presents results of the completer and per-protocol analyses, which yielded very different findings because the poor retention rate and treatment adherence lowered the power to detect effects with intention-to-treat analyses. Although for the completer (BDI-II, Y-BOCS) and per-protocol analyses (all indexes), the effect of time was significant, suggesting large improvements over the 6 weeks, only the per-protocol analyses yielded interactions in favor of myMCT at a medium-to-large (nonsignificant for Y-BOCS) or large (significant for BDI-II, OCI-R) effect size (see Table 2).
Prediction and moderation
We tested demographic and psychopathological variables as potential moderators of treatment outcome using the PROCESS macro by Hayes (Model 1). For all analyses, the BDI-II difference score served as the outcome variable. The interaction was not significant for any of the variables. The only significant effects were related to symptom decline across time. Having read fewer self-help books in the past (b = −2.72, SE = 1.23, t = −2.22, p = .0031, LLCI = −5.18, ULCI = −0.26) and having a higher baseline motivation (b = 3.85, SE = 1.39, t = 2.77, p = .008, LLCI =1.07, ULCI = 6.63) were related to better outcomes.
Subjective appraisal (ZUF-8 and additional questions)
Results of the ZUF-8 (Table 3) and other qualitative questions (Table 4) were compared with data obtained from a prior study on patients with OCD in an English-speaking sample (Moritz et al., 2018). Relative to the evaluation of myMCT in this previous study, ratings were worse (i.e., the difference was 10% or more) related to quality, whether the participants received the intervention they expected to receive, and participants’ happiness with the extent of help received. Moreover, only a few participants were able to use the manual on a regular basis. Most participants, more than in the prior study, endorsed that the manual would make more sense if it were used together with psychotherapy.
Subjective appraisal.a
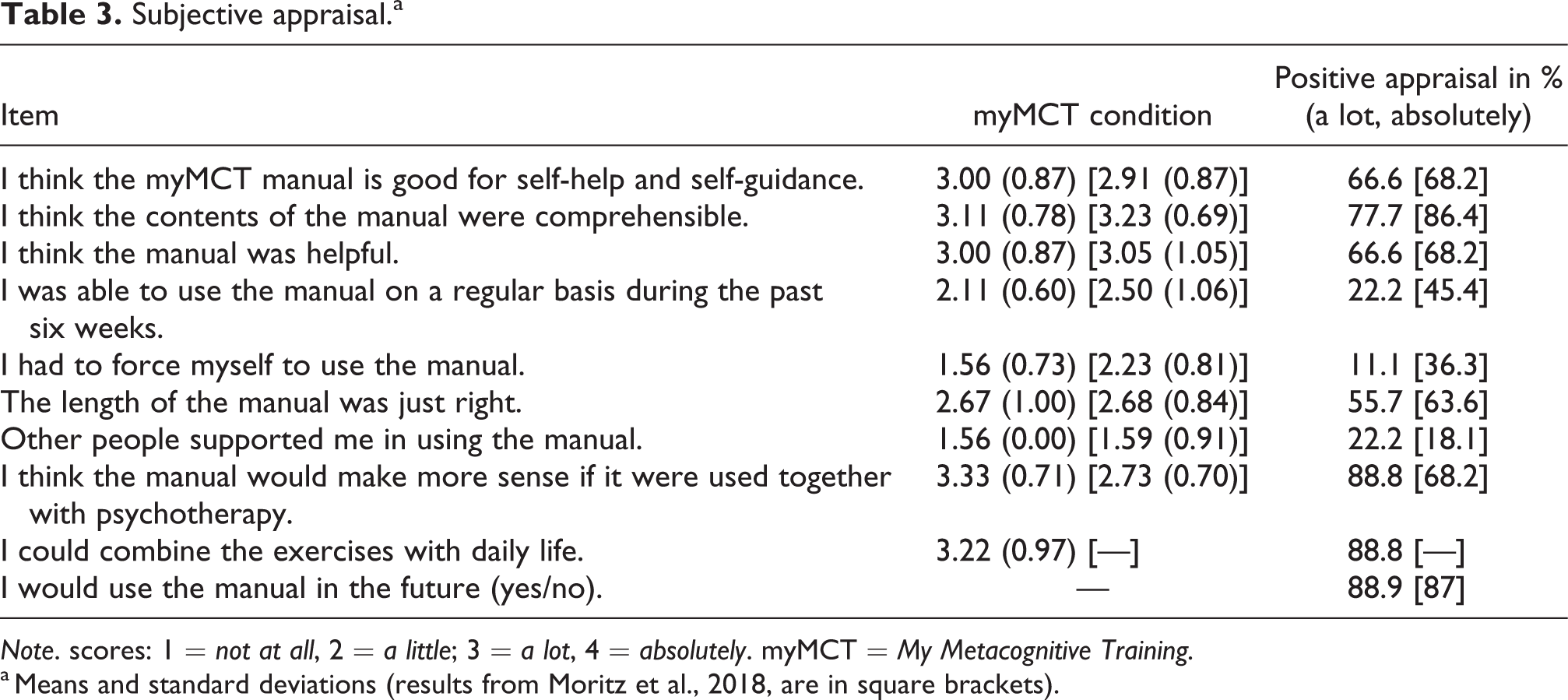
Note. scores: 1 = not at all, 2 = a little; 3 = a lot, 4 = absolutely. myMCT = My Metacognitive Training.
a Means and standard deviations (results from Moritz et al., 2018, are in square brackets).
Subjective appraisal of myMCT (adapted from the ZUF-8).a

Note. myMCT = My Metacognitive Training; ZUF-8 = Patient Satisfaction Questionnaire/Fragebogen zur Patientenzufriedenheit.
a Means and standard deviations (results from Moritz et al., 2018, are in square brackets).
Better ratings were obtained on the questions concerning whether the participants would recommend the manual to a friend with similar symptoms and whether they would use the manual again. Fewer individuals than in the prior study had to force themselves to use the manual (see Tables 3 and 4).
Ratings were comparable for appropriateness for self-help, helpfulness, comprehensibility, satisfaction with the manual, and length of the manual. Ratings were similar for the question as to whether the participants had received support from others.
Noncompletion
Noncompleters (i.e., participants who did not engage in the post assessment) did not differ from completers on any of the pathological or demographic background characteristics apart from lower motivation, t(158) = 2.37, p = .019.
Reliability
For the total sample, internal consistency was good to excellent (BDI-II: α = .84, Y-BOCS: α = .78; OCI-R: α = .89) and the test–retest reliability was satisfactory (BDI-II: r = .70, p < .001; Y-BOCS: r = .68, p = .004; OCI-R: r = .75, p < .001). For the wait-list control group, test–retest reliability was slightly better (BDI-II: r = .75, p < .001, Y-BOCS: r = .88, p = .006, OCI-R: r = .80, p < .001).
Discussion
The present study aimed to assess the efficacy of a trans-therapeutic (integrative/eclectic) manual for an Arabic-speaking population with OCD and/or depression. Unlike prior trials on the myMCT, we did not restrict the inclusion to participants with OCD only because depression and OCD share a number of metacognitive beliefs and dysfunctional coping mechanisms (see Introduction section). Moreover, we suspected that many individuals might not know their exact diagnosis in view of the poor awareness of mental illness and its treatment in Arab countries (Al-Darmaki et al., 2016; Al-Krenawi, 2005; Eapen & Ghubash, 2004; Karam et al., 2006). In the invitation, therefore, we described the core symptoms of OCD and depression to allow the participation of people who were unsure about the proper label for their problems.
We evaluated a self-help manual via an online study because the mental health infrastructure in most Arabic-speaking countries is poor (Okasha et al., 2012; World Health Organization, 2014) and, even if “Western” mental health treatment is available, other traditional or religious help is often sought, particularly due to stigma and knowledge gaps (see the Introduction). Although face-to-face therapy is usually recommended for standard treatment, several guidelines advocate media-delivered approaches or guided self-help if standard therapist-guided treatment is not available (for OCD, see, e.g., Hohagen, Wahl-Kordon, Lotz-Rambaldi, & Muche-Borowski, 2015; NCCMH, 2006) in view of promising findings related to this new line of treatment delivery.
As hypothesized, patients who had at least started reading the myMCT manual benefited from the intervention at a medium-to-large (Y-BOCS) or large (BDI-II; OCI-R) effect size relative to controls. Results are compromised by a number of factors, however, that raise strong questions about the feasibility of bibliotherapy in this language population. The completion rate (36%) was far lower than in prior trials of myMCT although the interval was the same. Moreover, this was the first unguided study on myMCT in which a financial incentive was provided in addition to another treatment manual at the end of the post assessment. Even worse, only 29% of those allocated to the intervention group read the manual. However, the retention rate was comparable for the two conditions, which tentatively speaks against dissatisfaction with the manual as the cause of the poor response rate (but does not prove it). If dissatisfaction were the cause, loss to post should have been largest for the myMCT condition.
Almost 90% of the individuals who read the manual reported they would use it again and would recommend it to a friend. Yet ratings were lower in comparison to a prior study (Moritz et al., 2018) for quality and happiness with the extent of the help received. Importantly, few patients used the manual on a regular basis, and most patients endorsed that the approach would make more sense if combined with psychotherapy. At least two thirds endorsed that the manual is good for self-help, helpful, comprehensible, and satisfactory. Few received support from other people.
As an interim conclusion, the approach seems to be effective, but the medium is suboptimal. We have recently developed an online tool for myMCT; the portal consists of different modules with many exercises and allows patients to access information on a secure website. It needs to be tested whether such a medium would be more successful in terms of dissemination and adherence despite some disadvantages mentioned in the Introduction. Prior research showed that online intervention is feasible and successful in an Arab population when used in a guided fashion (Knaevelsrud et al., 2015). At the moment, we can only speculate about the reason for the low adherence. For example, technical problems (not having a pdf reader despite instructions on how to download one) could have been a contributing factor. Reservations against psychological treatment because of fear of stigma or religious affiliation may have also played a role (see Introduction). We do not think that the contents were problematic because the few participants who had begun to read the manual showed clear improvements.
Subsequent analyses showed no moderating effects of any of the variables, including diagnostic status (OCD vs non-OCD). A lower number of self-help books read previously and higher motivation predicted a larger decline on the BDI-II, irrespective of condition.
The study suffers from a number of limitations, some of which have already been acknowledged. Retention rate and treatment adherence were extremely poor relative to studies on myMCT in Western populations (Hauschildt et al., 2016; Moritz et al., 2010, 2018) but also relative to a Russian population (Moritz, Stepulovs et al., 2016), to whom much of its content was probably unknown to a similar degree. The low retention rate is especially problematic for the intention-to-treat analyses. Because of the low retention rate and treatment adherence, we did not conduct a follow-up, which would have likely yielded unreliable findings.
Although the approach seems to have been effective for the few who used or began to use it, we think a different medium should be attempted, such as a smartphone app or an online tool. In emerging and developing countries, 37% of the population were in possession of a mobile device in 2015 compared to 68% in developed countries (Poushter, 2016). For Internet usage, the figures are higher (54% versus 87%), and the numbers have likely risen since then.
Conclusion
Our results indicate that, in its present form, the myMCT manual represents an effective but not very pragmatic or feasible treatment program for obsessions, compulsions, and depression in an Arabic-speaking population. Other forms of treatment delivery may improve the rate of use of the intervention.
Footnotes
Authors’ Note
Steffen Moritz and Schaimaa Irshaid are joint first authors; Marit Hauschildt and Franziska Miegel are joint senior authors.
Author contributions
All authors contributed to the study concept and design. Steffen Moritz and Marit Hauschildt wrote the original self-help manual My Metacognitive Training. Schaimaa Irshaid translated the manual and made cultural adaptations. She was also in charge of data collection and correspondence with participants. All authors contributed to data interpretation. Steffen Moritz drafted the manuscript, and Marit Hauschildt and Schaimaa Irshaid corrected the different versions. All authors approved the final manuscript for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.