
Abstract
Objective
This study reports clinical characteristic of moderate–severe obsessive–compulsive disorder (OCD) among school students in China.
Methods
We examined 153 patients for the distribution of OCD symptoms using the Yale-Brown Obsessive Compulsive Scale Symptoms Checklist, the severity of anxiety and depression symptoms using the Hamilton Anxiety Scale and the Hamilton Depression Scale-24, respectively, and impairment in learning, family and social functions using the Pediatric Quality of Life Enjoyment and Satisfaction Questionnaire.
Results
The number of total OCD, obsession and compulsion symptoms was 6.71 (standard deviation [SD] = 2.25), 3.77 (SD = 1.32) and 2.94 (SD = 1.59), respectively. The incidence of moderate and severe depressive symptoms for junior high school students was significantly higher than for primary and high school students. The number of children and adolescents with OCD increased with age, reaching a peak in the senior high school stage.
Conclusion
The most common symptoms in children and adolescent OCD patients are miscellaneous obsessions, aggressiveness, religiousness, checking, miscellaneous compulsions, cleaning-washing and repeating. These patients show a relatively high co-occurrence rate of anxiety symptoms and depressive symptoms, which impairs their learning, as well as their family and social functions.
Keywords
Background
Obsessive–compulsive disorder (OCD) is a relatively common and distressing mental disease characterised by time-consuming, impairing obsessions or compulsions, often accompanied by avoidance behaviours. 1 OCD affects approximately 2% of the general population.2,3 It affects 0.25% to 4% of children and adolescents,4,5 and at least 50% of patients with a first diagnosis experience a chronic course of symptoms that last to adulthood.6,7 OCD is associated with major functional disruption in multiple situations and leads to substantial impairment in several important areas of daily life. 8
The peak OCD incidence occurs in early adolescence and early adulthood. 9 Patients with OCD usually have a reduced quality of life, similar to patients with schizophrenia, 10 and have a heavy personal and socioeconomic burden. 11 OCD symptoms are often manifested internally rather than externally; many patients believe that their thoughts or behaviours are shameful or embarrassing and are unwilling to disclose them. 1 Owing to lack of awareness, parents may not realise that their children’s obsessive symptoms signify OCD. Parents also want to protect their children from the adverse effects of a label of OCD. OCD is often overlooked12–14 for several reasons: (1) patients are often reluctant to reveal their thoughts and behaviours to their parents or doctors out of fear that they will be considered strange; (2) medical staff, especially in general hospitals, lack awareness of the multiple manifestations of OCD symptoms; (3) misdiagnosis: clinically, two in three patients with OCD have a history of major depressive disorder (MDD), sometimes accompanied by generalised anxiety disorder (GAD). These mixed symptoms often lead to misdiagnosis as MDD or GAD instead of OCD; (4) in a standard psychiatric checkup, doctors seldom ask about OCD symptoms, such as compulsive hand-washing; and (5) parents often lack awareness of the multiple manifestations of OCD symptoms and thus do not recognise them. Altamura found that initial drug treatment takes almost 8 years from the onset of OCD.15,16 There are few large-scale and systematic studies on OCD in children and adolescents.
Although OCD symptoms affect children and adolescent patients’ daily life, learning and family interactions, doctors, parents and patients themselves still lack sufficient knowledge of OCD symptoms. 1 This study investigated OCD symptoms in children and adolescent patients. The comorbidity of obsessive–compulsive symptoms and depression and anxiety in different age groups were analysed. The identification of OCD symptoms is necessary to provide a theoretical basis for early diagnosis, and to promote healthy mental development in children and adolescents.
Materials and methods
The survey was conducted in the OCD Medical Center in Tongde Hospital of Zhejiang Province, P.R. China, from September 2009 to December 2017. The institutional review board approved the study protocol. All participants and/or their guardians participated voluntarily and provided written informed consent prior to the investigation.
All the children and adolescent patients who visited the OCD Medical Center were screened using the Short OCD Screener (SOCS) to increase the rate of OCD detection. Outpatients and inpatients were invited to participate in the study. Inclusion criteria were as follows: (1) a first diagnosis of OCD as defined by the World Health Organization’s International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10, 1995); (2) aged 6 to 18 years, regardless of gender; (3) OCD symptom severity of ≥16 on the Yale-Brown Obsessive Compulsive Scale (Y-BOCS). 17
Patients with any of the following conditions were excluded: (1) OCD was a comorbid symptom, not the primary mental disorder; (2) history of brain injury or surgery; (3) drug treatment or other psychiatric non-drug treatment in the past 4 weeks; (4) history of alcohol or drug abuse in the past 12 months.
Measures
The Yale-Brown Obsessive Compulsive Scale Symptoms Checklist (Y-BOCS-SC)18,19 and the Yale-Brown Obsessive Compulsive Scale (Y-BOCS) 17
The Y-BOCS-SC comprises 58 items that assess two types of obsessive–compulsive symptoms: 1) compulsive thoughts: aggressiveness, contamination, sex, hoarding-saving, religiousness, symmetry-exactness, body-related and miscellaneous obsessions (eight categories, 37 items); 2) compulsions: cleaning-washing, checking, repeating, counting, ordering-arranging, hoarding-collecting and miscellaneous compulsions (seven categories, 21 items). The Y-BOCS severity scale 17 consists of 10 questions scored on a scale of 0 to 4 that assess the severity of obsessions and compulsions. Total severity scores are usually assumed to indicate the following levels of OCD: subclinical (0–7), mild (8–15), moderate (16–23), severe (24–31) and extremely severe (32–40). A mild level of OCD is generally considered clinically significant, but previous studies have tended to consider scores ≥16 points as the inclusion criteria for OCD. 20
The Hamilton Depression Scale-24 (HAMD-24) 21 was developed by Max Hamilton in 1960 and is the most commonly used scale for clinical assessment of MDD. A total HAMD score >35 indicates severe depression (score level 4), 21 to 35 indicates moderate depression (score level 3), 8 to 20 indicates mild depression (score level 2) and <8 indicates no depressive symptoms (score level 1). 22 This scale has been used in some adolescent studies.23–25 A Chinese version of the scale suitable for teenagers was used in this study. 26
The Hamilton Anxiety Scale (HAMA) 27 is a classic anxiety rating scale compiled by Hamilton in 1959. It consists of 14 items rated on a 5-point scale. A HAMA total score ≥29 indicates severe anxiety (score level 4); 14 to 28 indicates moderate anxiety (score level 3); 7 to 13 indicates mild anxiety (score level 2); <7 indicates no anxiety symptoms (score level 1). Factor analysis of the HAMA has shown two major factors: physical factors and mental factors. The HAMA has been used in some adolescent studies.23,24 A Chinese version of the scale suitable for teenagers was used in this study. 28
The Pediatric Quality of Life Enjoyment and Satisfaction Questionnaire (PQ-LES-Q) 29
The PQ-LES-Q is a parent-reported questionnaire used to assess patients’ life quality. This questionnaire is suitable for person aged 6 to 17 years. It has good internal consistency and sufficient concurrent validity. The parent-reported items are used under the condition that parents can provide a relatively reliable authorised rating. The scale consists of 15 questions about current satisfaction with life, including health, mood/feelings, school, helping out at home, getting along with friends, getting along with family, play/free time, getting things done, sense of love for life, having enough money, place of residence, ability to pay attention, energy level and overall course of life. Each item is rated from 1 (very poor) to 5 (very good). The total score is the sum of each item score.
Research procedure
All the research members watched videos before the study began to train them in standardised questionnaire assessment. The reliability of the researchers’ results was statistically examined to ensure the authenticity and reliability of the collected data. The intraclass correlation coefficient was above 0.8.
Interviews were conducted with patients (accompanied by their parents); each interview lasted 1 hour. The researchers who participated in the study were doctors from Tongde Hospital of Zhejiang Province, and Zhejiang Chinese Medical University. The interview began with an introductory discussion of the patients’ problems. Patients then completed the Y-BOCS-SC, Y-BOCS, HAMD, HAMA and PQ-LES-Q with their parents’ assistance. The data were independently evaluated by psychologists. To ensure the reliability of the collected data, videos of rating interviews were recorded and randomly selected weekly (>20% of interviews were selected). Evaluators were retrained if the consistency rate fell below 80%.
To ensure the integrity of the data, patients with missing data were followed up by telephone. The quality control measured used in this study ensured the accuracy of data collation. The researchers conducted unified training and tests using the questionnaires, and conducted presurveys of the questionnaires after assessment to ensure consistency in understanding and operation among researchers.
The researchers conducted daily random checks on the questionnaire data to determine whether there were any missing/incorrect items and completed a quality control result record form.
The assessment of the scales was supervised by Zhejiang Chinese Medical University. The data management and statistical analysis was conducted by the Medical College of Zhejiang University. The study was regularly supervised by the Data and Safety Supervisory Committee, and supervision conferences were held every 6 months during the study.
Statistical analysis
Statistical analysis was performed using Dynamic Data Exchange (DDE) software (Beijing Jinshan Office Software Co., Ltd., Beijing, China) for data entry and exported using the SPSS database. SPSS version 19.0 (IBM Corp., Armonk, NY, USA) was used to organise and analyse the data. Count data were described using mean and standard deviation (SD). Differences between means were compared using the independent t-test. The interclass difference was compared using one-way analysis of variance, and the intraclass difference was compared using Student’s t-test. Measurement data were described using frequency and percentage. The interclass difference was compared using the chi-squared test. Possible influencing factors were screened using unconditional multivariate logistic regression analysis.
Results
Participant demographic and clinical characteristics
Of 675 patients with OCD, 163 declined to participate, 170 did not meet the inclusion criteria and 186 met the exclusion criteria. 153 cases were included in the survey: 99 boys and 54 girls. These were aged 8 to 18 years (mean age = 15.36 years, SD = 2.40 years) and had 2 to 12 years of education (mean = 9.59 years, SD = 2.25 years): primary school (group A, 6–12 years old) 23 cases (15.03%); junior high school (group B, 13–15 years old) 42 cases (27.45%); senior high school (group C, 16–18 years old) 88 cases (57.52%).
The mean age at OCD onset was 13.47 (SD = 2.59) years, the mean age at first visit to the medical centre was 15.36 (SD = 2.40) years and mean OCD duration was 21.95 (SD = 20.24) months. There was no significant difference in gender distribution between the three groups. There were significant differences in the age at first visit, age at onset, and duration of disease between the three groups (all P < 0.05), as shown in Table 1.
Participant demographic and clinical characteristics.

Values are means and standard deviations. A: primary school; B: junior high school; C: senior high school.
At the baseline, 56.21% of patients were not diagnosed with OCD and had never received medication or other treatment. Of the other 67 subjects who had received medication or other treatment, 13.04% (3/23) were in the primary school group, 42.86% (18/42) in the junior high school group and 52.27% (46/88) in the senior high school group. There was a significant difference between these three groups (x2 = 11.421, P = 0.003). The response rate of the primary school group was significantly lower than that of the junior high school group (x2 = 6.04, P = 0.025) and senior high school group (x2 = 11.381, P = 0.001). There was no significant difference between the junior high school group and senior high school group. Only 50.75% of subjects were correctly diagnosed with OCD out of the 67 subjects who had received treatment (medication or other treatments): 33.33% (1/3) in the primary school group, 44.4% (8/18) in the junior high school group and 54.35% (25/46) in the senior high school group. There was no significant difference in correct diagnosis between these three groups.
Analysis of obsessive–compulsive symptoms
The mean number of obsessive symptoms was 3.77 (SD = 1.32), the mean number of compulsion symptoms was 2.94 (SD = 1.59) and the total number of obsessive–compulsive symptoms was 6.71 (SD = 2.25). A total of 96.08% (147/153) of patients had more than one type of obsession and 83.66% (128/153) of patients had more than one type of compulsion. Of the total patients, 4.58% (7/153) had only obsessions and no corresponding compulsions, whereas 0.65% (1/153) of patients had only compulsions and no obsessions.
Table 2 shows the number and proportion of the 15 types of Y-BOCS-SC obsessive–compulsive symptoms for the whole sample and for the three groups. The three most frequently reported obsessions were miscellaneous obsessions (87.58%), aggressiveness (72.55%) and religiousness (62.75%). The four most frequently reported compulsive behaviours were checking (88.24%), miscellaneous compulsions (75.16%), cleaning-washing (47.71%) and repeating (47.71%).
Distribution of symptoms.

Y-BOCS-SC: Yale-Brown Obsessive Compulsive Scale Symptoms Checklist; A: primary school; B: junior high school; C: senior high school. *Comparison between groups A, B and C.
There were significant between-group differences in the obsessions religiousness (P < 0.01), symmetry-exactness (P < 0.05), miscellaneous (P < 0.01) and body-related (P < 0.05), and in the compulsion checking (P < 0.01) (Table 2).
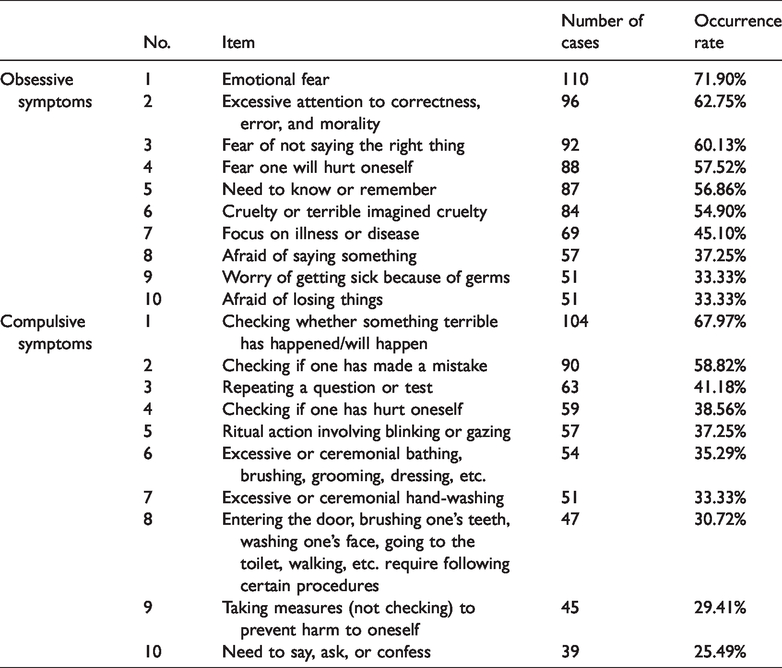
The five most frequently reported obsessive symptoms for the whole sample of 153 patients were emotional fear; excessive attention to correctness, error, and morality; fear of not saying the right thing, fear of hurting oneself; and need to know or remember (Table 3). The five most frequently reported compulsive symptoms were checking whether something terrible has happened/will happen; checking if one has made a mistake; repeating a question or repeating a test; checking if one has hurt oneself; or ritual action involving blinking or gazing (Table 3). Of the 10 most frequently reported obsessive and compulsive symptoms, the symptom overlap rate was low for primary school patients compared with junior high school and high school patients, but the symptoms of junior high school and senior high school patients overlapped. After examination, there was no statistical difference in OCD severity between the three groups.
Most frequently reported obsessive and compulsive symptoms.
Comorbidity of OCD and anxiety/depression symptoms
Of 153 patients with OCD, 107 (69.93%) had depression symptoms and 101 (66.01%) had anxiety symptoms (Table 4). There was a significant difference in the severity of depressive symptoms between the three groups (P = 0.001). The incidence of moderate to severe depressive symptoms in junior high school and high school students was 30.95% and 6.82%, respectively. The incidence of moderate and severe depressive symptoms in junior high school students was significantly higher than that in primary and high school students (P < 0.01). There was no significant difference in symptom severity distribution (Table 4).
Distribution of severity of comorbid anxiety and depression symptoms.

A: primary school; B: junior high school; C: senior high school; HAMA: Hamilton Anxiety Scale; HAMD-24: Hamilton Depression Scale. *Comparison between groups A, B and C.
OCD severity analysis
Using OCD severity as the dependent variable (0 = moderate, 1 = severe), a multivariate logistic regression analysis was performed with four independent variables: age, gender, severity of HAMD symptoms and severity of HAMA symptoms. The results showed that greater severity of HAMA symptoms was associated with more severe OCD (Table 5).
Multivariate logistic regression analysis of factors influencing OCD severity.

OCD: obsessive–compulsive disorder; HAMA: Hamilton Anxiety Scale; HAMD-24: Hamilton Depression Scale; OR: odds ratio; CI: confidence interval.
Of the 153 patients with OCD, 125 (81.70%) showed a decline in academic performance. The analysis of life quality (PQ-LES-Q scores) is shown in Table 6. There was a statistically significant difference in decline in academic performance and family functions between the three groups of patients (Table 6) (both P < 0.001). As education level increased, decline in academic performance and family function decreased, whereas the absenteeism rate increased.
Outcomes of Pediatric Quality of Life Enjoyment and Satisfaction Questionnaire.
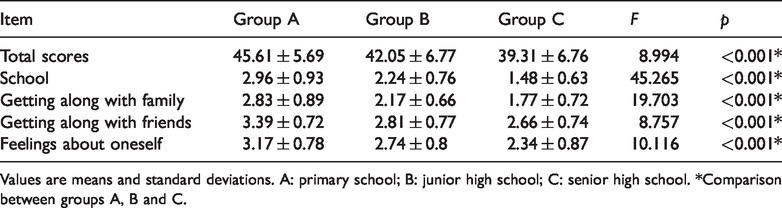
Values are means and standard deviations. A: primary school; B: junior high school; C: senior high school. *Comparison between groups A, B and C.
Ethics approval
Before the data collection, ethical clearance was obtained from Tongde Hospital of Zhejiang Province, and formal permission was obtained from the drug prevention and rehabilitation centres. Written informed consent was obtained from the individuals with OCD and their guardians. Participants were informed about the purpose and voluntary nature of the study, and informed that there was no foreseeable risk or harm from participating in the study.
Discussion
OCD is a neurotic disorder characterised by uncontrollable obsessive and compulsive behaviours that often affect an individual’s social function and have a negative impact on their family. 30 As a subtype of mood disorder in children and adolescents owing to its special aetiology, clinical manifestations, treatment and prognosis, OCD in children and adolescents has received increasing attention. According to one survey, approximately one-third to one-half of adult OCD cases occur before the age of 15 years or even before school age. 31 The average age of onset in this study was 13.47 years, and disease duration increased with age. The number of children and adolescents with OCD reached a peak in the senior high school stage. The average course of the disease in this study was 21.95 months, and the disease course continued to increase with age. Epidemiological studies show that approximately 0.6% of adolescents have OCD. 32 Prepubescent boys have a slightly higher OCD prevalence rate, but there is only a slight difference in OCD prevalence in pubescent boys and girls. 33 In this study, boys accounted for 64.7% of OCD cases, which is consistent with epidemiological results.
This study showed that the comorbidities of depressive symptoms and anxiety symptoms in 153 patients with OCD were, respectively, 69.93% and 66.01%, and the number of patients with comorbid anxiety symptoms and depressive symptoms reached a peak in the junior high school stage. The incidence of moderate and severe depressive symptoms in junior high school students was significantly higher than that in primary and high school students. Higher HAMA scores indicated more severe OCD symptoms.
The findings showed that the three most frequently reported obsessions (as assessed by the Y-BOCS-SC) were miscellaneous obsessions, aggressiveness and religiousness. The five most frequently reported obsessive symptoms were emotional fear, excessive attention to correctness, error, morality, fear of not saying the right thing, fear of hurting oneself, and need to know or remember. These latter five symptoms are related to learning pressure experienced by the patient.
The three most frequently reported compulsions were checking, miscellaneous compulsions, cleaning-washing and repeating. The five most frequently reported compulsive symptoms were checking whether something terrible has happened/will happen, checking if one has made a mistake, repeating a question or repeating a test, checking if one has hurt oneself and ritual action involving blinking or gazing. Of these five symptoms, checking whether something terrible has happened/will happen, checking if one has made a mistake, repeating a question or repeating a test, and ritual action involving blinking or gazing are also related to learning processes and habits.
Most of the children and adolescent OCD patients in this study had more than one type of obsession or compulsion. Most patients showed obsessions and compulsive behaviour, a finding consistent with the results of Matsunaga. 34 The five most frequently reported obsessive and compulsive symptoms were similar to Juckel et al.’s findings 35 (“enhanced feeling of responsibility,” “exact attention concerning details,” “difficulties with decisions,” and “repetitive controlling”). In the present study, the distribution of obsessive and compulsive symptoms in primary school students was significantly different from that in junior high school and senior high school students. There was no significant difference in the distribution of symptoms between junior high school and high school students. This may be because of changes related in academic stage and accommodation in patients with OCD. Most primary school students are day students, and the family environment has a greater impact on them. Most junior high school and high school students are resident students. These students are more affected by the school and other students, and when they suddenly experience greater academic pressure, their obsessive and compulsive symptoms change.
The academic performance of subjects in this study showed a declining trend (as assessed by the PQ-LES-Q). This study assumed a subtle relationship between learning and adaptability and the family environment. Individuals who score <8 on the PQ-LES-Q usually show the characteristic of perfectionism. They work hard and learn well. Individuals who score ≥16 or above probably experience OCD; their learning and adaptation abilities may be impaired and they may show declining test scores. These results indicate that even students with minor obsessive symptoms can achieve good academic results. However, if their condition worsens, they may show a sharp decline in performance. Doctors are unlikely to diagnose mild symptoms that do not affect an individual’s daily study, work and social intercourse as OCD. In fact, individuals who strive for perfection may learn and work better. Checking of house doors, car doors, windows and gas switches increases safety. Keeping one’s body and household goods clean increases comfort. These tendencies do not indicate a morbid state as long as the individual feels no distress. However, when such symptoms affect an individual’s daily activities, they become a problem. Parents will not seek medical advice if a child is functioning well in daily life. In China, primary hospitals are unlikely to provide adequate psychiatric treatment. In addition, parents may be unwilling to consult a doctor because of a sense of shame. When they finally choose to visit a hospital, the problems are usually moderate to severe.
The mental states of children and adolescents continue to develop as their age, physical development, family and social environment change. 36 Currently, Chinese children and adolescents face huge pressure from entrance examinations at the end of each academic stage. This is a challenge for the whole family, and every family member plays a role in preparing the child for the examinations. As a result, students, families and schools experience enormous invisible pressures. 36 In the present study, the incidence of moderate to severe depressive symptoms in junior high school and high school students was 30.95% and 6.82%, respectively. In childhood and adolescence, OCD often co-occurs with other mental disorders, most commonly neuropsychiatric disorders, including anxiety and depression symptoms. 37 Comorbidities interfere with the course of OCD treatment and affect its efficacy.
Research suggests that family accommodation contributes to higher levels of functional impairment in child and adolescent OCD patients, 38 particularly day students. Many OCD patients engage their caregivers in their OCD symptomatology, such as asking them to directly participate in compulsions. 39 Studies have shown that scores on family intimacy and emotional expression factors perceived by adolescent OCD patients are lower than those of normal volunteers, and scores on contradictory factors are higher than those of normal volunteers, indicating that the communication and emotional expression of family members of adolescent OCD patients are often problematic and contradictory. 40 There are many contradictions in the family environment, 41 and some young people may not experience a family atmosphere of care, warmth and lightheartedness. Adolescent obsessive–compulsive patients believe that parents are less likely to be warm and understanding, and more likely to be punishing, harsh and refusing. 42 Przeworski et al. 42 found that in OCD patients, both the parents’ emotional expression and the patient’s subjective perception of the parents’ emotional expression were critical and accusatory, and this tendency was related to OCD severity. Therefore, even if young people with OCD seek help from parents or teachers in the early stages of OCD, they often feel uncomfortable or harshly treated because of their mild symptoms and the heavy academic pressure they are under. OCD is often detected after a long course of illness, which means that the best time for treatment is often missed.
Conclusion
Teenage patients usually show obsessive thinking in the initial OCD stages. OCD problems are usually internal and seldom exhibited externally. Most patients consider OCD symptoms to be shameful and embarrassing and are thus unwilling to seek medical help. However, when the patient has a greater knowledge of their OCD, they find it easier to understand some symptoms, such as uncontrollable touching, repeating some sentences, and patting and beating some parts of the body when taking off the clothes. If the patient feels no pain or anxiety from these uncontrollable behaviours, and if the behaviours eventually disappear, then the problem is not OCD. However, if the behaviours affect various aspects of the patient’s life, they may indicate OCD.
Symptom analysis should be used to determine whether a patient has OCD and needs to consult a doctor when the following symptoms appear: emotional fear, excessive attention to right and wrong, excessive morality, fear of not saying the right thing, fear of hurting oneself, need to know or remember, checking if something terrible has happened/will happen, checking to see if one has made mistakes, repeating questions or tests, checking if one has hurt oneself and ritual action involving blinking or gazing. The present findings indicate that the number of children and adolescents with OCD increases with age, reaching a peak in the senior high school stage. The number of patients who have comorbid anxiety symptoms and depressive symptoms reaches a peak in the junior high school stage. Once an individual has developed OCD, with or without comorbidities (e.g. depression and anxiety symptoms, as found in this investigation), their abilities may be impaired. In conclusion, greater awareness of OCD symptoms and comorbid depression and anxiety symptoms will help with early diagnosis and timely treatment of OCD.
Footnotes
Acknowledgements
We would like to thank Tongde Hospital of Zhejiang Province, for accepting our proposal and providing ethical clearance. We acknowledge Zhejiang Chinese Medical University for providing the assessment tools Y-BOCS-SC, Y-BOCS, HAMD, HAMA and PQ-LES-Q. We owe our thanks to all the individuals who participated in this study.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.