
Abstract
Impaired insight in patients with schizophrenia results in less satisfactory clinical outcomes. This study was conducted to investigate the relationship between insight and individual psychopathological dimensions in inpatients with schizophrenia using a self-report questionnaire. In this study, 90 patients with schizophrenia aged 18–75 years admitted in the acute psychiatric ward of a medical center in Taiwan were enrolled. Patient insight was measured using the Self-Appraisal of Illness Questionnaire (SAIQ), and psychopathological dimensions were measured using the Positive and Negative Syndrome Scale (PANSS) and its five-factor structure model. A higher SAIQ score indicates greater insight. In bivariate correlation analyses, statistically significant correlations were observed between age, single marital status, educational level, and positive, excited, and depressed symptom factor of the PANSS and SAIQ score. In regression analyses, age and excited and depressed symptom factors were significantly associated with SAIQ score. No significant association was observed between insight and neurocognitive functions. Considering demographic characteristics, psychopathology, and neurocognition, in the acute phase of schizophrenia, younger patients with less severe excited symptoms and more severe depressive symptoms had greater insight.
Introduction
The concept of insight comprises awareness of illness, attitude toward psychotic experiences, the process of judging one’s self-experience, and the exploration of the causes and reasons of experiences (David, 1990). Insight is not an all-or-none phenomenon; it is thought to be a capacity that includes multiple dimensions of awareness of the illness, the need for treatment, and the consequences associated with the illness (Amador et al., 1993). Impaired insight in patients with schizophrenia causes nonadherence to treatment and poor clinical outcomes (Erol et al., 2015).
Studies on insight in patients with schizophrenia have more often used researcher-rated insight scales instead of self-report measurements. A trained researcher might provide a more valid assessment using an objective rating scale. However, self-rated scales for assessing insight, such as the Birchwood Insight Scale (Birchwood et al., 1994), Insight and Treatment Attitudes Questionnaire (McEvoy et al., 1989), and Self-Appraisal of Illness Questionnaire (SAIQ) (Marks et al., 2000), have been used in clinical practice. Some objective researcher-rated insight scales have been used as the gold standard tool for comparison and shown acceptable validity and reliability. Moreover, a self-report may reduce some researcher biases, such as participant–researcher interaction problems and the tendency to categorize patients with low intelligence and weak communication skills as having poor insight (Marks et al., 2000). This issue cannot be ignored in patients with schizophrenia who have marked psychopathology and difficulties with social interaction.
Many symptoms of schizophrenia, such as delusions, are false judgments that are presented with extraordinary conviction and are unshakeable by other experiences and counterargument. Patients with a delusional thinking process are often unable to judge the difference between the real and fantasy worlds. Therefore, patients may be unaware of their symptoms and, thus, are unaware of the need for medical assistance. Studies have found a significant association between insight and positive symptoms (Amador et al., 1993), negative symptoms (Mingrone et al., 2013; Zhou et al., 2015), disorganization (Smith et al., 2000), and excitement (Pousa et al., 2017). However, studies on the relationship between insight and depression are controversial (Cohen et al., 2019; Zhou et al., 2015).
Taiwan is situated in Southeast Asia and has developed according to its traditional cultural backgrounds. Until now, certain beliefs and preconceptions toward people with schizophrenia exist in Taiwan (Kurumatani et al., 2004). Stigma may result in insight leading to despair, and individuals may consider meaningful life as no longer a viable possibility. Studies have reported that clinical insight and stigma interact in a manner that results in the experience of reduced meaning and self-clarity in life (Hasson-Ohayon et al., 2014; Or et al., 2013). These subjective experiences may be assessed better using a self-rating scale. The SAIQ used in this study includes dimensions of worry, need for treatment, and outcome of illness. For example, the worry dimension focuses on whether the patient is concerned about the surrounding environment due to their mental illness, such as looking for jobs and making friends. The questionnaire may have different results due to different social and cultural backgrounds. To date, in Taiwan, few studies have explored clinical insight in patients with schizophrenia measured using a self-report questionnaire. Thus, this study was conducted to use a self-rated scale to evaluate clinical insight from the perspective of the patient; in addition, we assume that the insight of patients with schizophrenia is related to psychiatric symptoms in a Chinese or Taiwanese cultural context. Moreover, we investigated the relationship between clinical insight and clinical variables, cognitive function and executive function in inpatients with schizophrenia.
Material and method
Participants and study design
This study adopted a cross-sectional design. The study subjects included patients with schizophrenia who were hospitalized on an acute psychiatric ward of a medical center in Taiwan from December 2017 to May 2019. Patients who met the following inclusion criteria were invited to participate in the study: (a) age between 18 and 75 years, (b) a primary clinical diagnosis of schizophrenia, (c) able to cooperate with interviews, and (d) stable medication and dosage for 2 weeks. Because the number of older patients with schizophrenia and their proportions in the general population are rising as the life expectancy globally increased (Liao et al., 2020), we recruited older participants in this clinical study. The diagnosis of schizophrenia was made according to the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (APA, 2013) and based on the clinical interviews and review of medical records by two senior psychiatrists. Those who had any substance use disorder (e.g. alcohol, tobacco, and betel nut use) and neurological or medical conditions that can impair cognitive functions, including head injuries and intellectual disabilities, were excluded from the study. In this study, 90 patients were recruited. During the investigation period, all participants received their usual daily treatment. All patients received antipsychotics, including first-generation antipsychotics (n = 8, 8%), risperidone (n = 10, 11.1%), paliperidone (n = 11, 12.2%), aripiprazole (n = 5, 5.6%), olanzapine (n = 12, 13.3%), quetiapine (n = 9, 10%), clozapine (n = 10, 11.1%), long-acting injection antipsychotics (n = 21, 23.3%), and others (n = 4, 4.4%). The questionnaire and methodology for this study were approved by the Institutional Review Board of Changhua Christian Hospital. Written informed consent was obtained from all patients.
Insight assessment
The Taiwanese version of the SAIQ (Kao & Liu, 2010; Marks et al., 2000) is a 17-item self-report tool for investigating and measuring attitudes toward psychiatric illness. The participants rate each item using a 4-point scale ranging from 0 (do not agree at all) to 3 (agree completely). Higher SAIQ scores indicate greater insight. The SAIQ contains three-factor structures, which are defined as worry, need for treatment, and presence/outcome of illness. The items of the worry subscale include how much a patient tends to worry, worry about their conditions, worry about getting into trouble, worry about losing friends, worry about being unable to work or not recovering, and worrying thoughts that interfere with getting things done. The worry subscale can be used to measure the dimension of social consequences associated with illness in the patient’s insight. The items in the subscale of the need for treatment include how a patient feels about other people’s recommendation for their treatment, whether they believe the current treatment to be necessary, how a patient thinks they would be doing without treatment, whether the patient is gaining a lot from being treated, and whether their condition requires psychiatric intervention. The items in the presence/outcome of illness subscale comprise whether a patient thinks that their conditions will go away without treatment, whether a patient believes that they will be better someday without treatment, whether they would do fine if treatment is discontinued, whether they have symptoms of mental illness, and how ill the patient thinks they are. In this study, the internal consistency was acceptable, and Cronbach’s α was 0.896 for the entire scale, 0.866 for the worry subscale, 0.819 for the need for treatment subscale, and 0.801 for the presence/outcome of illness subscale.
Clinical evaluation
Positive and Negative Syndrome Scale (PANSS)
We evaluated the patients’ psychopathology using the PANSS, a 30-item scale scored using a 7-point scale from 1 to 7 for each item (Kay et al., 1987). Higher total scores indicate more severe symptoms. We adopted the five-factor structure based on the National Institute of Mental Health consensus model (Wallwork et al., 2012). This model uses 20 of the 30 items of the PANSS, including positive, negative, disorganized, excited, and depressed factors. The positive factor comprises items of delusion, hallucination, grandiosity, and unusual thought content; the negative factor comprises items of blunted affect, emotional withdrawal, poor rapport, passive social withdrawal, lack of spontaneity, and motor retardation; the disorganized/concrete factor comprises items of conceptual disorganization, difficulty in abstraction, and poor attention; the excited factor comprises items of excitement, hostility, uncooperativeness and poor impulse control; and the depressed factor comprises items of anxiety, guilt feelings, and depression.
Clinical Global Impressions Scale–Severity (CGI-S)
The overall severity of patients was assessed using the CGI-S and Clinical Global Impressions Scale–Improvement (CGI-I) (Guy, 1976).
Cognitive functions
The Frontal Assessment Battery (FAB) (Dubois et al., 2000) and Montreal Cognitive Assessment (MoCA) (Nasreddine et al., 2005) were used to evaluate executive and cognitive functions, respectively, by a senior psychiatrist. The FAB measures six domains of executive function: conceptualization, mental flexibility, motor programming, sensitivity to interference, inhibitory control, and environmental autonomy. The total scores of the FAB range from 0 to 18, with a higher score indicating a better function. The MoCA measures seven cognitive domains: visuospatial/executive functions, naming, verbal memory registration and learning, attention, abstraction, 5-min delayed verbal memory, and orientation. The total scores of the MoCA range from 0 to 30, with a higher score suggesting a better cognitive function.
The rater of clinical evaluation, including the PANSS, CGI, MoCA, and FAB, was blinded to each participant’s response to the SAIQ.
Statistical analysis
The correlation between the SAIQ score and variables was assessed using the Pearson correlation coefficient and independent t-test. With respect to the small sample size, we determined the factors associated with insight using multiple linear regression analyses wherein the variables that reached statistical significance in the bivariate analyses were used as independent variables. We used the Enter method for multiple linear regression analyses. Considering that the patients’ cognitive function deteriorated with ageing, we used the partial correlation in which patients’ ages were controlled when examining the relationship of the individual subscales in the SAIQ with the researcher-rated insight (item G12 in the PANSS, lack of judgment and insight) and neuropsychological variables. For all analyses, p-values of less than .05 were used to denote statistical significance.
Results
Demographics of the participants
Of the 90 patients, 51 (56.7%) were male. The average age of the patients was 44.4 ± 11.7 years. The average age at the onset of schizophrenia was 27.0 ± 10.7 years. The average duration of illness was 17.4 ± 11.0 years. The mean total score of the CGI-S was 4.0 ± 0.7, and that of the PANSS was 73.4 ± 10.0 (Table 1).
Demographics and clinical features of patients with schizophrenia, mean ± standard deviation.

Note. CGI-S = Clinical Global Impressions Scale–Severity; CGI-I = Clinical Global Impressions Scale–Improvement; PANSS = Positive and Negative Syndrome Scale; MoCA = Montreal Cognitive Assessment; FAB = Frontal Assessment Battery; SAIQ = Self-Appraisal of Illness Questionnaire.
Correlation between clinical variables and insight
Table 2 shows the statistically significant correlations between age, marital status, and educational level and insight. Moreover, significant correlations were observed between higher positive, lower excited, and higher depressed factor scores of the PANSS and higher SAIQ scores. In addition, a positive correlation was found between the scores of the FAB and SAIQ. We further examined the correlation between the patients’ clinical variables and the item G12 in the PANSS (researcher-rated insight). The correlation matrix of the SAIQ, PANSS factors, neurocognition, and other variables is presented in Table 3.
Correlations of clinical features of patients with schizophrenia and insight scale (SAIQ and PANSS G12).

Note. CGI-S = Clinical Global Impressions Scale–Severity; CGI-I = Clinical Global Impressions Scale–Improvement; PANSS = Positive and Negative Syndrome Scale; PANSS G12 = item G12 in PANSS rating lack of judgment and insight (researcher-rated insight); MoCA = Montreal Cognitive Assessment; FAB = Frontal Assessment Battery; SAIQ = Self-Appraisal of Illness Questionnaire; higher SAIQ score indicates greater insight.
† Coefficient of the Pearson correlation analysis.
‡ t-Value of independent t-test.
*p < .05; **p < .01.
Correlation matrix of SAIQ, PANSS factors, neurocognition, and other variables.

Note. Coefficient of the Pearson correlation analysis; Marriage (0 = single, 1 = married); Edu = educational years; PAN-T = total score of Positive and Negative Syndrome Scale; PAN-T = total score of PANSS; PAN-P = positive factor score of PANSS; PAN-N = negative factor score of PANSS; PAN-Dis = disorganized factor score of PANSS; PAN-E = excited factor score of PANSS; PAN-Dep = depressive factor score of PANSS; MoCA = Montreal Cognitive Assessment; FAB = Frontal Assessment Battery; SAIQ = Self-Appraisal of Illness Questionnaire; higher SAIQ score indicates greater insight.
*p < .05; **p < .01.
Multiple linear regression analyses
The patients’ age; educational year; marital status; positive, negative, disorganized, excited, and depressed factor scores of the PANSS; and FAB score were entered into the regression analyses. Age (standardized β = −.224; T = −2.007; p = .048), the excited factor score of the PANSS (standardized β = −.434; T = −4.945; p < .001) and depressed factor score of the PANSS (standardized β = .340; T = 3.903; p < .001) showed a statistically significant association with the SAIQ. The regression model explained 37.8% (F = 7.017; p < .001) of the variance in the SAIQ (Table 4). The regression model to predict PANSS G12 as a dependent variable was also performed. The results revealed that the patients’ educational year, family history, and excited and depressed factor scores of the PANSS reached significance.
Associative factors of clinical insight (SAIQ) of patients with schizophrenia according to multiple linear regression analysis.
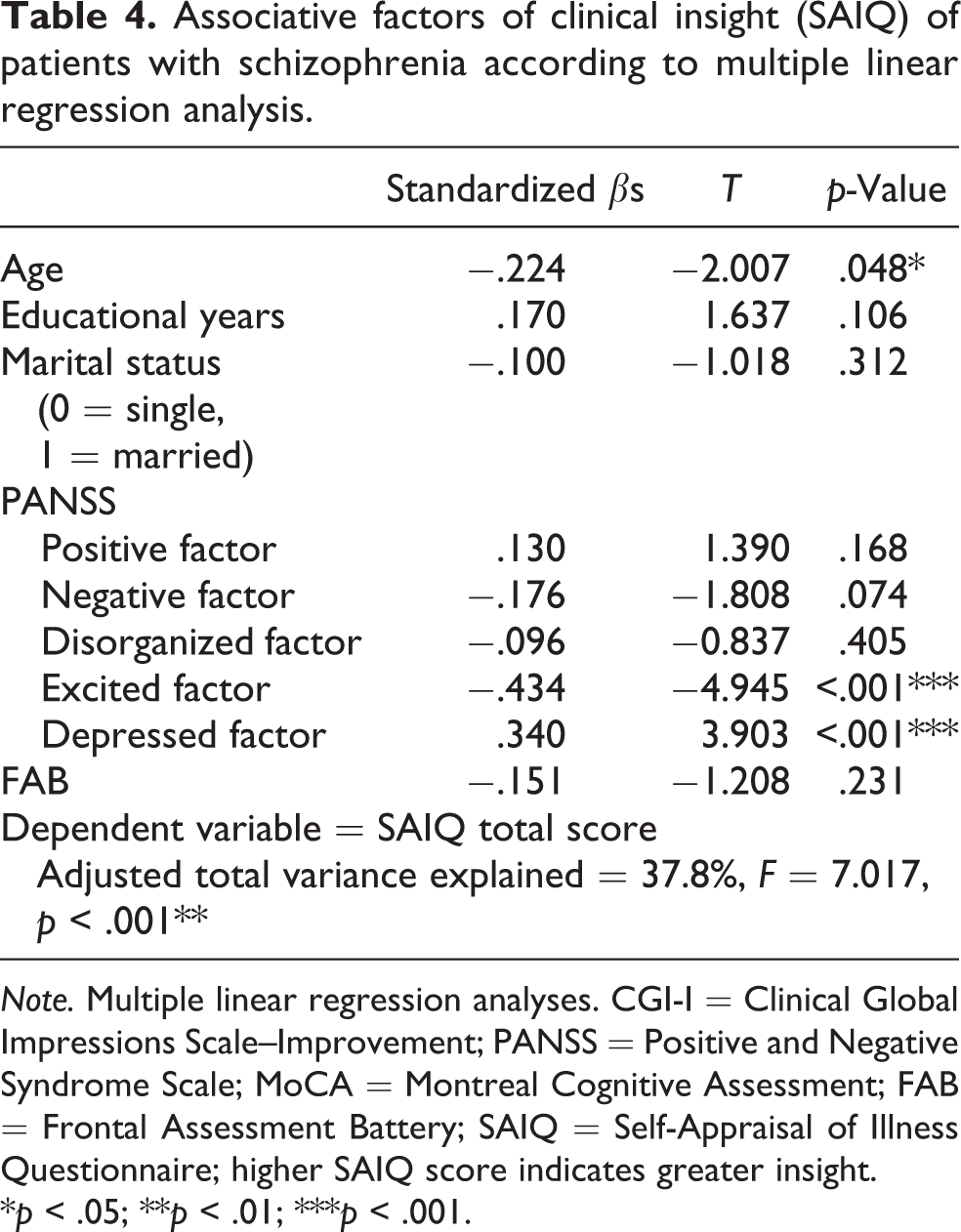
Note. Multiple linear regression analyses. CGI-I = Clinical Global Impressions Scale–Improvement; PANSS = Positive and Negative Syndrome Scale; MoCA = Montreal Cognitive Assessment; FAB = Frontal Assessment Battery; SAIQ = Self-Appraisal of Illness Questionnaire; higher SAIQ score indicates greater insight.
*p < .05; **p < .01; ***p < .001.
Partial correlations of the SAIQ subscales and variables
After age was controlled, the worry, need for treatment, and presence/outcome of illness subscale scores in the SAIQ exhibited a significantly negative correlation with PANSS item G12 (lack of judgment and insight) score. There was no significant correlation between the three aforementioned subscales and FAB or MoCA (Table 5).
Correlations of the SAIQ subscales with researcher-rated insight, neuropsychological functions, and psychopathology.

Note. Partial correlation, age was controlled; higher SAIQ score indicates greater insight. SAIQ = Self-Appraisal of Illness Questionnaire; PANSS = Positive and Negative Syndrome Scale; MoCA = Montreal Cognitive Assessment; FAB = Frontal Assessment Battery.
*p < .05; **p < .01; ***p < .001.
Discussion
Insight and educational level
In the bivariate analysis, patients with more years of higher education had greater insight, as shown in either the SAIQ or PANSS G12 as the outcome. The educational level was significantly associated with PANSS G12 in the regression model. These findings are inconsistent with some studies (Bayard et al., 2009; Xiang et al., 2012). The inconsistent results might be attributed to the heterogeneous sample and could be possibly influenced by the stage of illness in the study population. Less-educated patients have lesser understanding of the illness and no knowledge of available services and, therefore, seek traditional healers (Basu et al., 2015). Well-educated patients may have more access to information regarding mental illnesses than less-educated ones. Early interventions targeted at the less-educated patients are necessary to help them understand psychiatric symptoms and for them to receive immediate treatment.
Insight and age
The results of this study revealed that age was negatively correlated with the SAIQ score, indicating that older patients have worse clinical insight. This finding appears not only in the bivariate correlation analysis but also in the linear regression analysis. Since we also included the scores of patient cognitive function (MoCA), executive function (FAB), and psychopathology (PANSS) in the regression analysis and the age variable was still considered a significant contributor, older age can be considered a factor independently associated with poorer insight. Studies from Western countries (Cohen et al., 2019; Gerretsen et al., 2014) have found similar results. Due to the chronic course of schizophrenia, older patients are receiving medical care for many years. With the ageing process, patients must deal with the changes in their physical condition, social support and family issues. In our inpatient study, since the Taiwanese or Chinese traditionally expect the children to take responsibility for caring for their parents, placing parents in a psychiatric ward would be regarded as abandonment by their families (Fung et al., 2008). We suggest that hospitalization results in some psychodynamic changes in older patients, such as defense mechanisms of denial or regression to cope with these life changes, and therefore, poorer adherence or impaired insight may develop.
Insight and family history
In contrary to the SAIQ, either in correlational or regression analysis, patients with a family history of mental illness were associated with greater insight measured by PANSS G12. Some studies have reported that the psychoeducational program for family caregivers can improve the patient’s sense of illness and awareness of self-symptoms (Ema Komala et al., 2018). We believe that since patients with a family history of mental illness and their family members have past experiences of the symptoms, manifestations, and treatment, they can be aware of the changes in their own mental and psychiatric symptoms. A patient with a family history of schizophrenia may teach their family how to manage a relative with schizophrenia. In addition, the physician may discuss with the patient and their family how the patient is not to be blamed for the illness and how to help the patient and family understand the need for treatment and signs of relapse so that the patient’s awareness of illness can be enhanced (Navidian et al., 2012).
Insight and psychopathological dimensions
Our results revealed that the overall severity of psychopathology (PANSS total score) did not correlate with the patients’ insight. This finding differs from those of some studies (David et al., 1995; Johnson et al., 2012, 2014). We speculate that the overall severity of psychopathology is partly related to the patient’s inpatient status. Due to the self-rating questionnaire used in this study, patients may be inclined to fill in a more acceptable reply for the psychiatric staff because they want to be discharged earlier, resulting in a finding of insignificant correlation. However, some trends and associations were still observed in individual psychopathological dimensions and insight. In addition, the positive symptom factor of schizophrenia was correlated with insight in the bivariate analyses, but not in the regression analyses. This finding indicates that the association of positive symptoms with insight is less significant than that of excited and depressed symptom factors with insight. Some studies support this result (McEvoy et al., 1989), and others have different results (Pousa et al., 2017; Zhou et al., 2015). Psychotic phenomenology is thought to be heterogeneous, and the awareness into each positive symptom is affected by the nature of symptoms and might be influenced by different cultural and psychological factors. Many studies have explored the relationship of lack of insight and psychopathology using the three-factor model of the PANSS (positive, negative, and general). Using a more detailed classification to investigate the relationship between insight and psychopathology may be more appropriate. We speculate that patients with positive factors on the PANSS, such as P1 delusions, P3 hallucinations, and G9 unusual thought content, have different symptom contents. Therefore, the patients have different explanations and coping strategies toward their positive symptoms and demonstrate various degrees of reality testing and awareness of the illness. The mechanisms for the production of positive symptoms and impaired insight may be independently developed and are not causally related (David et al., 1995; McEvoy et al., 1989).
Contrary to positive, negative, and disorganized symptom dimensions, either in bivariate or regression analysis, our results revealed that patients with more severe excited symptoms had poorer insight of the disease. This finding is similar to those of some other studies (Volavka et al., 2016; Zhou et al., 2015). This indicates that the observations of excitement, hostility, uncooperativeness, defensive attitude, or provocation of patients may indicate their currently poorer insight. To achieve greater insight, decreasing the patient’s excited symptoms should be emphasized more in the acute phase of schizophrenia.
Many studies have reported that the depressed symptoms of patients with schizophrenia are associated with their insight. Patients with more severe depression have greater insight (Murri et al. 2015), a finding supported by our results. In the regression analysis that considered multiple patient variables, the association between depressive symptoms and disease insight became more pronounced than that in bivariate analysis. The causal relationship between depression and clinical insight has been suggested to be a complex and mutual influence. The attribution theory has been developed within a cognitive framework and suggests that higher levels of depression in patients are associated with better awareness and attribution of mental illness (Lincoln et al., 2007). Conversely, the defense theory suggests that increased insight results in symptoms of depression. The process is understood as the depressive symptomatology being formed after the defense mechanism against lower self-esteem by the consequence of realizing that one has become ill and been diagnosed with schizophrenia. Depression and demoralization are considered outcomes of the reacquisition of insight (Cavelti et al., 2014).
In this study, the relationship of the three subscales of the SAIQ with the five psychopathology factors in the PANSS was investigated (Table 5). In the analysis of the worry subscale and total SAIQ score, patients with milder excited symptoms and more severe depressed symptoms had greater insight. We speculate that a patient’s emotional symptoms, such as excitement or depressive symptoms, significantly contribute to their insight. In addition, this result reflects the study strength. We used a five-factor structure model of the PANSS that could investigate the excited and depressed symptomatology in people with schizophrenia. This finding conforms to that of another study in Taiwan (Kao & Liu, 2010), which has used three psychopathological dimensions (positive, negative, and general) measured by the PANSS and found no correlation between insight and psychopathology. With respect to the need for a treatment subscale, patients with milder negative, disorganized, and excited symptoms had greater insight. When the patients had been effectively treated, they had fewer negative symptoms, better cognitive status, and a more stable mood and experienced gains from treatment. Therefore, they could express their feelings through the self-rating questionnaire process and report positive feedback regarding psychiatric treatment. With respect to the presence/outcome of illness domain, patients with more severe positive symptoms, milder excited symptoms, and more severe depressed symptoms had greater insight. This finding suggests that patients express their self-imagination and expectation of their disease in answering the questionnaire. When their positive symptoms are reduced, patients do not feel that they are sick and may tend to deny their illness.
Relationship of the SAIQ subscales with neurocognitive functions
Patient cognitive function (MoCA score) was not correlated with disease insight (Table 2). In the regression analysis and the partial correlation analysis, no association was observed between the patients’ executive function (FAB score) and their insight (Tables 3 and 4). These results are consistent with those of some published studies (Zhou et al., 2015). However, some studies have found a weak association between neurocognition and insight (Nair et al., 2014). Insight impairment may be related to deficits in multiple neurocognitive domains in a patient with schizophrenia. Metacognition and social cognition play significant roles in insight (Koren et al., 2004). The two aforementioned factors could not be assessed by the measurements used in this study. Moreover, we propose that the inconsistent results obtained in different studies are related to methodological differences, including the use of different instruments, and differences in the participants’ clinical course and disease stages. Another possible reason is that the number of samples in this study is too small to show statistical differences. Future research should investigate the relationship of the subitems of executive and cognitive functions with clinical insight.
Associations between poor cognitive function and schizophrenia were reported (Maccabe, 2008). In addition, age would reduce the cognitive function across time (Li & Hsu, 2015). Therefore, in this study, when analyzing the correlation between the SAIQ and PANSS G12, the MoCA and the FAB, the variable of age was controlled. When the age factor was controlled, the three subscales of the SAIQ were negatively correlated with the researcher-rated insight scale (item G12 of the PANSS, lack of judgment, and insight) (Table 5). This result differs from those of the studies from Western countries (Marks et al., 2000) but is similar to the findings of another study in Taiwan (Kao & Liu, 2010). In a Western country study (Marks et al., 2000), the worry subscale was not significantly correlated with item G12 of the PANSS. The author even recommended the exclusion of this subscale when screening for patient insight. We believe that the difference between this study and the study by Marks et al. (2000) reveals the differences between Eastern and Western cultures. Studies have suggested that stigmatizing attitudes against people with psychosis are much stronger in Chinese culture than those in European or American culture (Hsiao et al., 2006). People from cultures in which strong social stigma exists against people with mental illness have a psychosocial incentive to minimize their illness, presumably to avoid social rejection and devaluation (Mohamed et al., 2014). As the findings of this study in Taiwan, patients with schizophrenia apparently worry about getting into trouble, losing friends, or being unable to work. Those issues are also relevant to the subscales of some researcher-rated insight scales assessing patient awareness of the social consequences of mental disorders (Amador et al., 1993). The participants recruited in the study by Marks et al. (2000) were from the community. Patients living in the community may have milder symptoms and higher acceptance by the population; thus, they may have fewer issues to worry about. Therefore, we speculate that the worry domain in a patient’s overall insight assessment has a higher proportion and importance in Taiwanese or Eastern society background than in Western societies. In addition, the worry dimension reflects the internal worry and emotional state. Therefore, such things to worry about are relatively difficult to be visible in the scale evaluated by the researcher. Therefore, it may be difficult to show an association between the two scores (the worry subscale of the SAIQ and PANSS G12) in the correlational analysis. Interestingly, some positive findings in correlational and regression analyses have shown discrepancies between self-reported and observer-rated instruments as the dependent variable. Thus, the conjunct use of self-reports and observer-rated tools for a more comprehensive assessment of a patient’s insight is recommended.
This study had several limitations. First, a cross-sectional design in this study could examine the causal relationship between variables and insight. Second, the patients were recruited in an inpatient setting. Thus, the results may not be generalizable to all patients. The psychopathology and insight in patients of the outpatient department, day hospital, and chronic inpatient ward and those under psychiatric home care may be different. Third, the prescription patterns of medications, such as first- and second-generation antipsychotics and long-acting injections of antipsychotic drugs, and subtypes of schizophrenia may have various effects on a patient’s insight. Fourth, the sample size of this study was small. However, even with these limitations, we consider the results of this Asian study to be a valuable reference for comparison with Western studies.
Conclusions
In the acute phase of schizophrenia, younger patients with less severe excited symptoms and more severe depressive symptoms had greater insight. Higher educational level and a family history of schizophrenia might also be significant factors of greater insight. No significant correlation was observed between neurocognitive functions and insight. To promote the insight of acutely ill patients, we suggest addressing the patients’ psychiatric symptoms, especially excited symptoms, along with pharmacological and non-pharmacological treatments. In addition, patients with depressed symptomatology may require supplementary treatment with appropriate psychosocial intervention to improve their depression and simultaneously maintain their clinical insight. A longitudinal study tracking changes in the relationship between psychopathology and insight over time might be important and useful in clinical practice.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
The questionnaire and methodology for this study were approved by the Institutional Review Board of Changhua Christian Hospital. Written informed consent was obtained from each patient.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.