
Abstract
Objective
This study aims to investigate the prevalence of multimorbidity in Cyprus and the extent to which citizens are satisfied with the currently provided healthcare and to provide recommendations on the basis of findings.
Design
A nationally based survey conducted through personal interviews, using a structured questionnaire designed for this survey.
Setting
Cyprus rural and urban areas (excluding Turkish occupied areas).
Participants
Four hundred and sixty-five Cypriot adults, average age 53 years.
Main outcome measures
Lifetime prevalence of self-reported non-communicable diseases.
Results
This study demonstrated initial evidence for a high prevalence of non-age specific multimorbidity among Cypriots and dissatisfaction with their doctors, especially for the time allocated to discuss their general state of health. Recommendations focus on a new cost-effective, person-centred model of healthcare. The model prioritizes prevention rather than treatment, targeting the determinants of complexity before their influences create conditions that demand high-cost interventions, and it is based on three fundamental principles: (1) tackling health as a political issue, (2) empowering the patient and (3) introducing Applied Nutrition in the system.
Conclusions
This study threw light into the issue of patient complexity and revealed unmet people’s needs and expectations for a more person-centred care, providing a first challenge to the single disease-based system of healthcare in Cyprus. The findings of the study may have important implications for government policies and highlight the need for more research in this area to inform policy makers, particularly in view of the fact that a new Health System is currently being designed.
Introduction
The onset of the 21st century coincides with a global awareness of the rising numbers of chronically ill people with multimorbidity at increasingly younger ages. 1 Health systems are criticised for failing to respond effectively to the new challenges, 1 –3 which can be only partially addressed by single disease-based models, 3 and for focusing disproportionately on specialist care 1 away from the values of health equity and people-centred care declared at the Alma-Ata. Criticisms pinpoint the low focus on cost-effectiveness of public health strategies, 4 the low responsiveness to people’s needs and expectations 4 and low proportion of health expenditure on prevention. 2
Cyprus follows closely the global trends, with an ageing population 5,6 and a high incidence of chronic disease. 7 National health priorities include cardiovascular disease (CVD), diabetes, obesity, hypertension, hypercholesterolaemia and neuropsychiatric disorders, 2,5 –7 all shown to be associated with the socioeconomic status of citizens. 7,8 The Cypriot health system – the only one in Europe that relies heavily on private spending 2 – is criticised for fragmentation, lack of universal coverage and inequalities in access to healthcare services. 6 Hospitals focus mainly on acute care, without health planning mechanisms, no referral system, long waiting lists and no universal electronic medical record to facilitate continuity of care. 6 Out of the 2218 doctors in Cyprus, two-thirds work in the private sector and are mainly specialists 6 and of the rest in the public sector only about a fifth are general practitioners (GPs). 9 Spending on prevention programmes is the lowest in Europe (0.7%), 2 while existing policies on childhood obesity, smoking and healthy diet have not demonstrated any results so far. 6
In view of above, this study aims to investigate the prevalence of multimorbidity in Cyprus and the extent to which citizens are satisfied with the currently provided system of care and to provide recommendations on the basis of findings. To our knowledge, no previous studies have examined the issue of multimorbidity in Cyprus, which was defined for this study as ‘the presence of at least two chronic health problems reported by the same individual’.
Methods
Questionnaire design
The questionnaire was developed in Greek with 28 questions classified in two categories: Part A: Demographic data (questions 1–14) requesting personal and lifestyle data and Part B: Methods of prevention and treatment of chronic health problems (questions 15–28) focusing on lifetime prevalence of chronic diseases, methods, success and satisfaction of treatment. All questions were clearly defined and mutually exclusive, so that respondents could find exactly what they wanted to answer in one of the choices. Several alterations were made until a satisfactory questionnaire was formed with a good potential to obtain answers to all research questions. Coding, numbering, listing of questions, type and sequence of answers, etc. were clearly designed so that answers could be easily converted to variables and effectively subjected to statistical analysis. Three pilot studies were conducted which led to further modifications on the basis of the feedback obtained.
Data collection
This door-to-door survey was fielded from October 2008 to December 2008, resulting in 465 completed interviews. Interviewing was conducted by the Center for European and International Affairs of the University of Nicosia. All interviews were carried out by 18 interviewers working throughout the areas under the control of the Republic of Cyprus (urban and rural). Eligible respondents were household members, men or women, aged between 18 and 88 years. Respondents were selected using the most recent birthday method. There was no substitution of respondents within households. Data on the population were taken by the latest census (2002).
The study used a classic cluster sample design aiming at estimating household views/opinions across the island. The sample was designed to specifically represent the adult population residing in occupied residential housing units and, by definition, excluded residents of institutions and group housing. As a consequence of this sampling design, the objective was to obtain a confidence level of 95% and a confidence interval of ±4.5%. Based on the target population size, the sample size was estimated to be 474 people. In addition, a set of instructions were also given to them on how to approach each interviewee and on how to perform the interview. The overall response rate for this study was 61.26%.
Data analysis
The data were analysed with the use of SPSS 16. Both descriptive statistics (means, standard deviations and percentages) and inferential statistics (phi-coefficients, ϕ, that show the relationship between dichotomous variables) were used for the analyses. Further analysis was carried out in order to obtain deeper insights from the survey. A number of variables were subjected to cross tabulation. This paper was based on the part of the results related to multimorbidity and participants’ satisfaction with the provision of healthcare.
Results
The sample was composed of 465 adults, average age 53 years (SD = 15.52), of which 43.2% were men and 56.8% were women. In terms of education, 54.8% of participants were middle level (high school) graduates, 24.9% university/college graduates and 20.2% had elementary education. Age was determined with 2012 as a reference.
As shown in Figure 1, the majority of the participants (61.5%) report as suffering now, or have suffered in the past, from at least one health problem.
Health problems and percentages of the population reporting as suffering now (or in the past) from a health problem.
Cross tabulation of the results revealed strong positive correlations between many diseases in support of the ‘multimorbidity case’. Apart from the well-established associations between metabolic risks and CVD, significant associations were also shown between many common health problems, of both physical and psychological nature, such as cardiovascular disorders with cancer (ϕ = 0.137, p = 0.003) and arthritis (ϕ = 0.111, p = 0.016); and depression with obesity (ϕ = 0.281, p = 0.000), bowel problems (ϕ = 0.222, p = 0.000), skin problems (ϕ = 0.199, p = 0.000) and hypercholesterolaemia (ϕ = 0.184, p = 0.000). (All significant associations are included in Appendix 1.)
Number of health problems among the population.
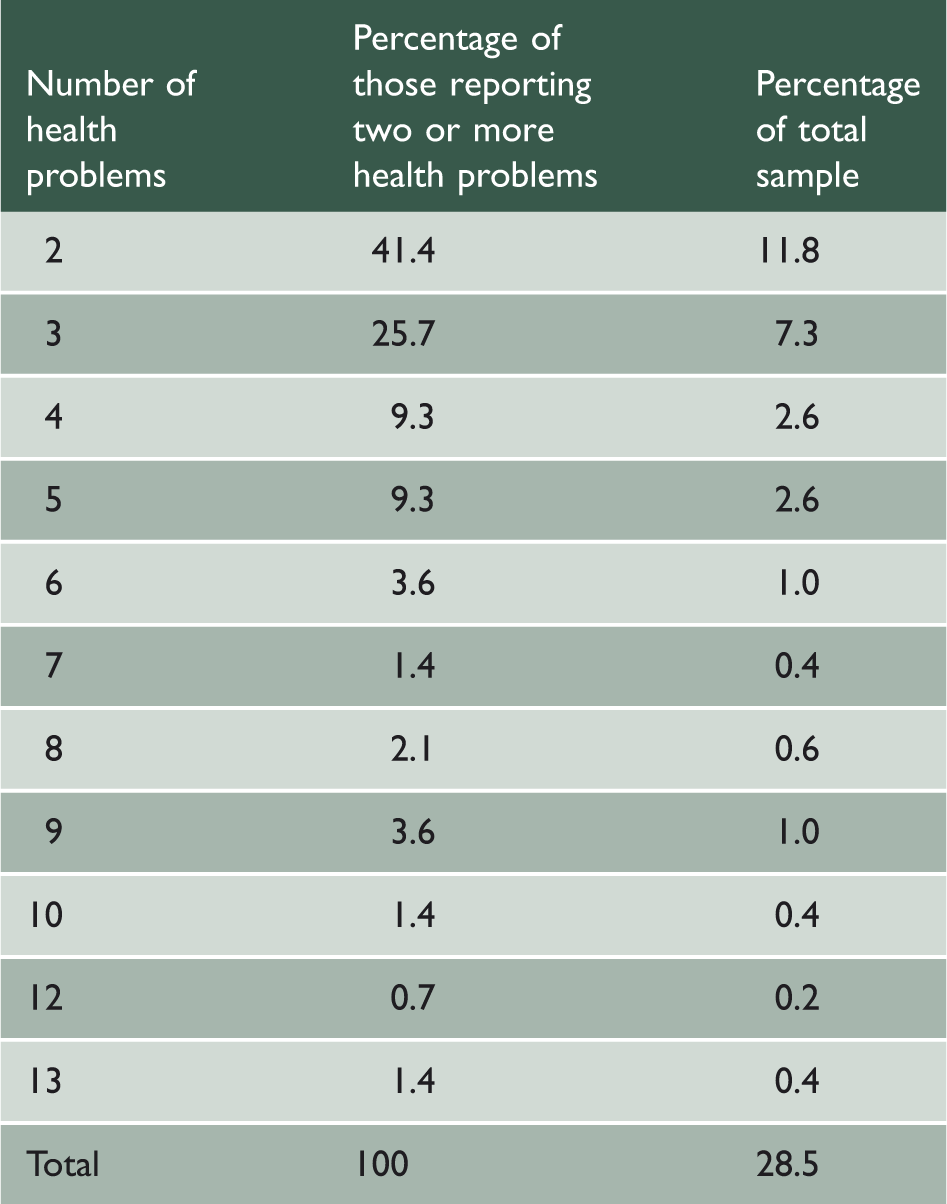
Age analysis of persons reporting two or more health problems.

A significant degree of dissatisfaction was also shown, with the time allocated by doctors to discuss both patients’ specific health problems (Figure 2(a)) and their general state of health (Figure 2(b)).
(a) Time allocated to patients by their doctor to discuss in detail the particular health problem for which they visited him/her and (b) time allocated to patients by their doctor to discuss in detail their general state of health, apart from the particular health problem for which they visited him/her.
Just over a fifth (21.7%) of the population felt that their doctor allocated ‘much’ (11.6%) or ‘very much’ (10.1%) time to discuss in detail a particular health problem, whereas 32.9% believe that they were allowed ‘little’ (29.0%) or ‘no time’ (3.9%) (Figure 2(a)).
To the question if doctor allows time to discuss their general state of health, apart from the particular problem for which they visited him/her, only 20.4% of the population stated that they were allowed ‘much’ (11.8%) or ‘very much’ time (8.6%), whereas 43.4% believe they were given ‘little time’ (27.3%) or ‘no time’ (16.1%) (Figure 2(b)).
Discussion
This study in line with research elsewhere, 1,10,11 highlights the issue of patient complexity, demonstrating evidence for a high prevalence of non-age-specific, multimorbidity and low fulfilment of citizens’ expectations for more person-centred approaches. Whereas multimorbidity rises with age, the vast majority of multimorbid participants are younger than 65. Furthermore, several common diseases appear to occur over time in the same individual. These not only include diseases of the metabolic syndrome family – already shown to have common deeper pathophysiological links based on web-like metabolic abnormalities 11 – but also diseases, seemingly unrelated – and as a rule medically treated independently from each other – such as CVD with cancer and arthritis; and hypercholesterolaemia with cholelithiasis, skin problems and fungal infections. A strong psyche–body interconnectedness was revealed with neuropsychiatric disorders occurring in the same individual with hypercholesterolaemia, obesity, bowel problems, skin problems, fungal infections and cholelithiasis. Unfulfilled expectations for more person-centred approaches were also expressed, with almost half of the population expressing dissatisfaction with the time allowed by their doctor to discuss their general state of health, apart from the specific problem for which they visited him/her. Time, however, may not be the only missing value as the vast majority (76.5%) of Cypriots never in their life visited a GP, 12 who traditionally focuses on the persons and the particular circumstances of their lives. 10, It is highly probable that those visiting GPs are even less, as the terms General Pathologist, Specialist Pathologist and often the Cardiologist are synonymous with the GP in Cyprus. 12 Evidently, limited choice forces resort to specialists who, as a rule, even with more time, would not be in a position to discuss all the diseases of a patient.
Based on the above findings, and in view of the burden of the economic crisis on the country’s resources, we propose a cost-effective model of care, highly responsive to citizens’ needs and expectations, on the basis of European ideals for longer and healthier lives. 4,13 The model draws from the philosophy that underpins integrated healthcare paradigms which demands multidisciplinary and crossdisciplinary teamwork 14 on the basis of common goals, inter-professional relationships and collective learning within communities of practice. 3 Aiming at tackling the determinants of complexity before their influences create conditions that demand high-cost interventions, the proposed model is founded on three fundamental principles: (1) tackling health as a political issue, (2) empowering the patient and (3) introducing Applied Nutrition (AN) in the system.
Tackling health as a political issue
Tackling health as a political issue – a major WHO strategic aim 4,14 – requires cross-government policy coherence and coordination 14,15 in health strategies, laws and regulations. Under the burden of the evidence that the actual determinants of health exist well beyond the narrow boundaries of the health sector, 8,11,14 the new health system needs to focus on the persons and the multitude of web-like interactions with their environments. 11 Taking into account that every aspect of the government and the economy has the potential to affect health and health equity, including finance, education, housing, employment, transport and health, 14 the focus should be on strengthening ‘health governance’ 16 through harmonisation of health aims and objectives, both at horizontal and vertical levels of management, so that these do not cut across ministerial and other organisational boundaries. 15 Lack of policy coherence and coordination is evident, for example, in the Cypriot Ministry’s of Commerce policy for unrestricted trading, production and consumption of trans fats in spite of WHO’s calls to all Ministries of Health for a global ban of trans fats. 17 Government leadership to balance public and private sector interests and to effectively control the relationship between the market and health equity is important, as the marketplace can generate serious negative conditions for health, including the increased availability of, and access to, health-damaging commodities. 14 In view of the well-established beneficial effects of the Mediterranean diet and the abundance of these foods on the island (e.g. olive oil), the government should establish mechanisms (e.g. subsidies to producers, educational programmes to citizens, and so on) to support and encourage their production and consumption, and proceed to ban harmful foodstuffs (as already did Denmark and Austria with trans fats).
Furthermore, based on official estimates that healthcare spending could be halved if people can remain healthy as they live longer, 18 the focus should be on reinvesting resources to low-cost, high-impact interventions, 4 such as prioritising illness-prevention rather than illness-management. 13 For the past decades, the emphasis was rather on high-cost, low-impact interventions, creating a health system suffocated by expensive diagnostic equipment, 6 predominantly used for the diagnosis of symptoms after they appear and by specialists 6 who deal with single disease care. In an interview with HIO officials by the first author, it was revealed that the European guidelines to focus on prevention rather than treatment 13 were translated as more diagnostic laboratory and other tests, despite that these have not been shown to reduce morbidity or mortality. 19 These views may be related to the fact that the Cypriot health sector, in general, has an overcapacity of expensive medical technology – largely underutilized, 6 which place Cyprus at the very top of the list among European countries on number of CT scanners and hospital MRI units per capita. 2
Empowering the patient
Patient empowerment, a core principle of 21st century anthropocentric health strategies, 13,14,16,18 aims at reinforcing citizens’ psychosocial skills, 20 including their self-efficacy, assertiveness, self-awareness, sense of autonomy and, in general, their ability to influence the state of their health. 14,20,21 Researchers found that patients expect and demand a higher level of health literacy and involvement in clinical decision making than they feel they have. 10,22 Patient empowerment can be a highly cost-effective long-term strategy as it decreases dependence on healthcare services. 21 Empowering interventions draw from the principles of self-determination and self-reflection 20,21 and are characterised by continuity of care, patient centeredness, mutual acknowledgement and adequate time to allow patients to negotiate treatment options and make their own decisions. 20 The ‘empowerment-oriented approach’, 20 which considers patients as self-determining agents responsible for the consequences of their choices, is seen as an alternative to the traditional ‘compliance-oriented’ approach, 20 a basic principle of the paternalistic paradigm, 21 which views patients as passive recipients of medical decisions and prescriptions, 20 submitting to the authority of their healthcare provider. 21 Policy makers need to be aware of the importance of ensuring self-awareness and choice in patient empowerment policies, to help patients develop self-efficacy and guide decisions regarding disease and treatment availability and safety. 13,20 Patient empowerment is one of the areas not adequately addressed yet by policy makers in Cyprus. 6 Citizens, for example, have a very narrow range of choices, 6 leading to dissatisfaction, as shown by this study. Establishing a policy for increasing GPs and creating an institutional framework for complementary and alternative medicine (CAM) modalities, 6 using the technical support offered by WHO within the context of its global strategy on CAM, 16 will increase citizens’ informed and safe choices in line with EU policies. 13 Furthermore, the development and implementation of a coherent national e-Health strategy following WHO guidelines 16 will significantly add to citizen health literacy and self-efficacy and will reduce the burden on the system.
Introducing Applied Nutrition
Nutrition is widely acknowledged as a major determinant of health 16,18 with a much more complex relation to illness than commonly believed, as it incorporates a multitude of intricately complicated interactions between several parameters which influence an individual’s choice of food, including biological, economic, physical, social, psychological and behavioural factors. 11,23 At the moment, evidence-based nutritional therapeutic interventions – such as those used by Nutritional Therapists, Clinical Nutritionists and other Applied Nutrition professionals 24,25 – are largely absent from mainstream healthcare practice in Cyprus. While government statistics demonstrate that only 4.5% of the population visited a nutrition professional in the past year, and these were mainly women aged 15–44, 12 our study found that 75% of patients with multimorbidity are aged above 45. Apparently, these patients do not receive professional nutritional counselling, as this is not normally offered within the context of routine medical practice. 26 Nutritional science appears to be a victim of overloaded curricula in medical schools. As evidence demonstrates, with the rapid growth and change of medical knowledge, the medical curricula in Europe and the USA – where the vast majority of Cypriot doctors study – have become overloaded, resulting in the dilution of focus and insufficient depth in the treatment of subjects they cover. 27 Notably, health workforce planning experts agree that the current skill mix of the health workforce might not be able to tackle some of the key challenges and key changes in demand for healthcare of the 21st century, 27,28 and calls for inclusion of practical nutritional advice to patients and families during consultations are included in official reports. 29
In view of the above, we propose the introduction of Applied Nutrition – the application of systems biology-based nutritional science in therapeutic interventions – into the new national health system, as an essential complementary partner to mainstream medicine. Twenty-first century nutritional science, supported and reinforced by the revolutionary developments in Nutrigenomics, 11 – which study the way gene expressions are regulated and modified by different nutrients and environmental substances in different humans under different conditions 11 – has the potential to play an integrationist role, crossing disciplinary barriers 30 throughout the whole spectrum of healthcare practice. Firmly grounded on the idea that the underlying mechanisms of disease rest at the intracellular level, 11 and in line with WHO’s view of health as ‘a dynamic continuum rather than a series of isolated health states’, 16 Applied Nutrition is a necessary component of holistic models of care that address the multitude of web-like interactions of people with their environments.
Applied Nutrition is already an essential evidence-based partner of the functional paradigm, which promotes a novel model of chronic care based on the integration of applied nutritional science into mainstream primary healthcare. 11 In the United Kingdom, Applied Nutrition is practised on the basis of National Occupational Standards and a Code of Conduct, Performance and Ethics, under a new regulatory body, The Complementary and Natural Healthcare Council (CNHC) 25 which was commissioned and funded by the Department of Health in 2009. 31
Limitations
This study had a few limitations related to the nature of the study, being a questionnaire survey, and the high probability of biases and inconsistencies in reporting, as compared to clinical outcomes. A further limitation relates to the comparison between studies due to the fact that multimorbidity as a conceptually new area of study is poorly defined, with limited evidence on the care of multimorbid patients.
Implications for policy and research
The findings of this research may have important implications for government policies, particularly in view of the fact that the immediate implementation of an effective National Health System – delayed for decades due to the inability of past governments to face the opposition of related parties – is one of the measures demanded by the Troika (IMF, ECB, European Commission) which currently reviewed the Cyprus Economy. This study threw light into the issue of patient complexity providing a first challenge to the single disease approach exclusively used by the current health system. More research based on clinical data is needed to inform policy makers, as health policies can be effective only if they are adequately informed about the actual needs and expectations of citizens and the multiple factors contributing to their complex conditions that may rest with socioeconomic, environmental and other circumstances. Health workforce planning, for example, should be based on demand not on supply, a fundamental prerequisite to ensure needs and expectations are met.
Conclusions
This study provided adequate evidence to reinforce existing criticisms for the imperative of radical reforms in the health system. The proposed model of healthcare conforms both to European ideals and the World Health Organisation’s global strategies, for providing citizens with the essential prerequisites to live longer and healthier lives in harmony with their environments. Under the devastating effects of the economic crisis, our model offers low-cost, high-impact solutions which address the roots of illness and, at the same time, empowers citizens to become active participants in maintaining their health and preventing illness, reducing the burden of expensive treatments on the system. The Ministry of Health as the predominant defender of health has a major role to play, acting as a ‘catalyst’, 14 to enhance and upgrade the knowledge available to political actors in order to stimulate political action on the social determinants of health. To this end, a robust health equity surveillance system is essential to inform the right interventions in the right sectors. Policy makers need to be also aware that a more anthropocentric paradigm is already materialising in Europe in the form of policies formulated on core values, such as people-centeredness 1 and citizen’s empowerment. 18 It is important when formulating policies to keep in mind the World Health Organisation’s, clearly anthropocentric, definition of health as ‘a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity’.