
Abstract
Background:
Drug-induced interstitial lung disease (DILD) is an increasingly common cause of morbidity and mortality. However, due to the lack of specificity, DILD detection remains an unsolved public health challenge.
Objectives:
For the first time, we aimed to examine DILD reports submitted to the Food and Drug Administration (FDA) Adverse Event Reporting System (FAERS) to identify demographic characteristics and top drugs associated with DILD at a group level (including age, sex, drug class, and country stratification) and individual drug level.
Design:
A retrospective analysis of the FAERS database was examined by disproportionality analysis.
Methods:
We reviewed the FAERS database from 2004 to 2021, using search terms ‘interstitial lung disease’ and sorting cases by generic drug name. The reporting odds ratio, proportional reporting ratio, and Bayesian confidence propagation neural network were calculated as the measure of strength of association.
Results:
There were 32,821 DILD reports in the FAERS. After excluding reports without age, sex, or country data according to the specific measurement, the median age of patients was 68 (interquartile range: 59), 54.77% were male, and 46.00% of reports came from Japan. The top drug classes related to DILD in the FAERS were antineoplastic, followed by cardiovascular and antirheumatic agents, in varying order in different sexes. Fam-trastuzumab deruxtecan-nxki, ramucirumab, and eribulin were the top three drugs with the highest strength of association. We also found some drugs without DILD in the labels, such as amiodarone, temsirolimus, and ursodiol. There are significant differences in DILD reports in various countries. For example, the United States and France reported more cardiovascular agents, whereas Canada reported more antirheumatic agents.
Conclusion:
We found the top drugs and drug classes that were associated with DILD in the FAERS, which provides a real-world window for different ages, sexes, and countries to formulate precise pharmacovigilance policies.
Plain language summary
Keywords
Introduction
Drug-induced lung injury is a specific adverse event in the pulmonary system caused by drug use, which may involve the airway, parenchyma, pleura, pulmonary vascular system, and neuromuscular system.1,2 It has different clinical phenotypes and histopathologic patterns, including pneumonia (autoimmune, eosinophilic, and hypersensitive), pulmonary fibrosis, sarcoidosis, and pleural effusion. 3 Among these, drug-induced inflammation and fibrosis, also known as drug-induced interstitial lung disease (DILD), are the most common and severe forms of drug-induced lung injury. It can damage gas exchange, resulting in dyspnea, in severe cases, respiratory failure, and death. 4 Compared with other involved pulmonary clinical phenotypes, it has the strongest drug-induced association and is an increasingly common cause of morbidity and mortality. The incidence of DILD varies between 4.1 and 12.4 cases per million per year, accounting for 3–5% of prevalent interstitial lung disease (ILD).5,6 Moreover, the clinical, pathological, and radiological features of DILD are less specific, making the diagnosis of DILD an enormous challenge. 7 Consequently, our knowledge of the demographics and characteristics of DILD is limited, which hinders our ability to develop precise policies to reduce the risk of this severe drug-induced disease.
Big data analysis has promising applications in drug-induced disease prevention and treatment. The Food and Drug Administration (FDA) Adverse Event Reporting System (FAERS) is the largest public pharmacovigilance database for spontaneous reporting of adverse events. And it is also the primary source for post-market safety monitoring and evaluation of drugs and therapeutic biologics.8,9 Recently, some studies have evaluated drug-specific lung injury through the FAERS database.10,11 However, as far as we know, no one has used this database to identify the most frequently reported drugs related to DILD. Therefore, we sought to analyze reporting trends of DILD and determine the most frequently reported drugs, drug classes, and drugs with the highest strength of association with DILD by sex and age, respectively. Additionally, we aimed to assess the differences in DILD reports across countries.
Design and methods
Data source
FAERS is a database that contains adverse event reports, medication error reports, and product quality complaints resulting in adverse events. 12 The data are updated quarterly and has accumulated more than 229,394,683 reports to date. Each report includes a case identification number, suspect drug, adverse events, sex, age, patient outcome, report date, reporter, etc. The database plays a crucial role in the post-marketing safety monitoring of drugs.
Definition of DILD cases
In this study, we solely focus on DILD to assess drug-induced pulmonary toxicity, as it has the most robust drug-induced component. While other pulmonary phenotypes may represent potential disease complications (e.g. rheumatoid arthritis-associated ILD), relevant therapeutic approached (e.g. radiation pneumonitis, radiation alveolitis), or infection-related complications (e.g. bronchiolitis, pneumonitis). This approach reduces the risk of false-positive outcomes. Some research groups have reported detecting DILD signals of post-market drugs through the FAERS database.6,11,13–15 Adverse events in the FAERS database are encoded by the Regulatory Activity Medical Dictionary (MedDRA), with DILD being coded as ‘interstitial lung disease’ (PT = 10022611)’. Therefore, we only retrieved the FAERS database for the term ‘interstitial lung disease’.
Data processing and analysis
Data standardization and filtering
This study involved reports from the FAERS database between 2004 and 2021, with retrieval in March 2022. In the event of repeated submissions from the same patient, as recommended by the FDA, only collected the most recent version of the report. Meanwhile, to focus our results on the drug most likely responsible for the reported DILD, we only selected drugs with the role code ‘primary suspect drug’ (Figure 1). Drugs with ‘secondary suspect drug’, ‘concomitant drug’, and ‘interacting drug’ were excluded due to the greater uncertainty of association between the drug and the reported DILD. To ensure the accuracy and convenience of subsequent analyses, we manually standardized the drug names and classes, and unified age units. Moreover, based on various analysis objectives, incomplete reports regarding age or sex, or country from the DILD database had been excluded to facilitate further investigation into the demographic characteristics of DILD. 16 For example, when examining the gender proportion of DILD in a specific drug/drug category, only reports with available sex data were included in the denominator rather than the total data.

Data acquisition and processing flow chart.
Stratified analysis
Excluding incomplete reports such as age and gender absence, the remaining reports were obtained for stratified analysis. We analyzed the development trend of DILD reports over years and the demographic distribution of DILD reports according to sex and age. 17
The rankings, proportions, and disproportionality strength of DILD reports involved drugs and the drug classes were analyzed. We classified drug classes according to the primary therapeutic purposes, including antineoplastic, antirheumatic, antimicrobial agents, etc. It also examined outcomes in patients with DILD stratified by age and sex. Furthermore, the top 10 drugs related to DILD in four countries that reported the most DILD were compared.
Statistical analysis
We determined the strength of association of DILD at an individual drug level through the reporting odds ratio (ROR), proportional reporting ratio (PRR), and Bayesian confidence propagation neural network (BCPNN).18–20 We compared the proportion of DILD of the target drug in the FAERS database with that of all other drugs to detect the potential DILD reporting risk. To avoid false-positive signals, only when three statistics achieve the criterion, it can be regarded as disproportionality, suggesting that the proportion of DILD reports of the target drug is higher than that reported for all other drugs in the database. 21 The methods and criteria were shown in Table 1.
The statistics used for detecting drugs with high-risk DILD.

a, number of reports with DILD caused by the target drug; b, number of reports with other AEs caused by the target drug; c, number of reports with DILD caused by other drugs; d, number of reports with other AEs caused by other drugs.
BCPNN, Bayesian confidence propagation neural network; CI, confidence interval; DILD, drug-induced interstitial lung disease; PRR, proportional reporting ratio; ROR, reporting odds ratio.
We used descriptive statistics to analyze the demographic characteristics of the DILD database, including age, sex, reporter, and reporter country. A curve regression model was used to evaluate the development trend of DILD reports. The data was processed using EXCEL2019 presented as mean ± SD or a median with the 25th percentile [M (25p)].
Results
Temporal trends and demographic characteristics
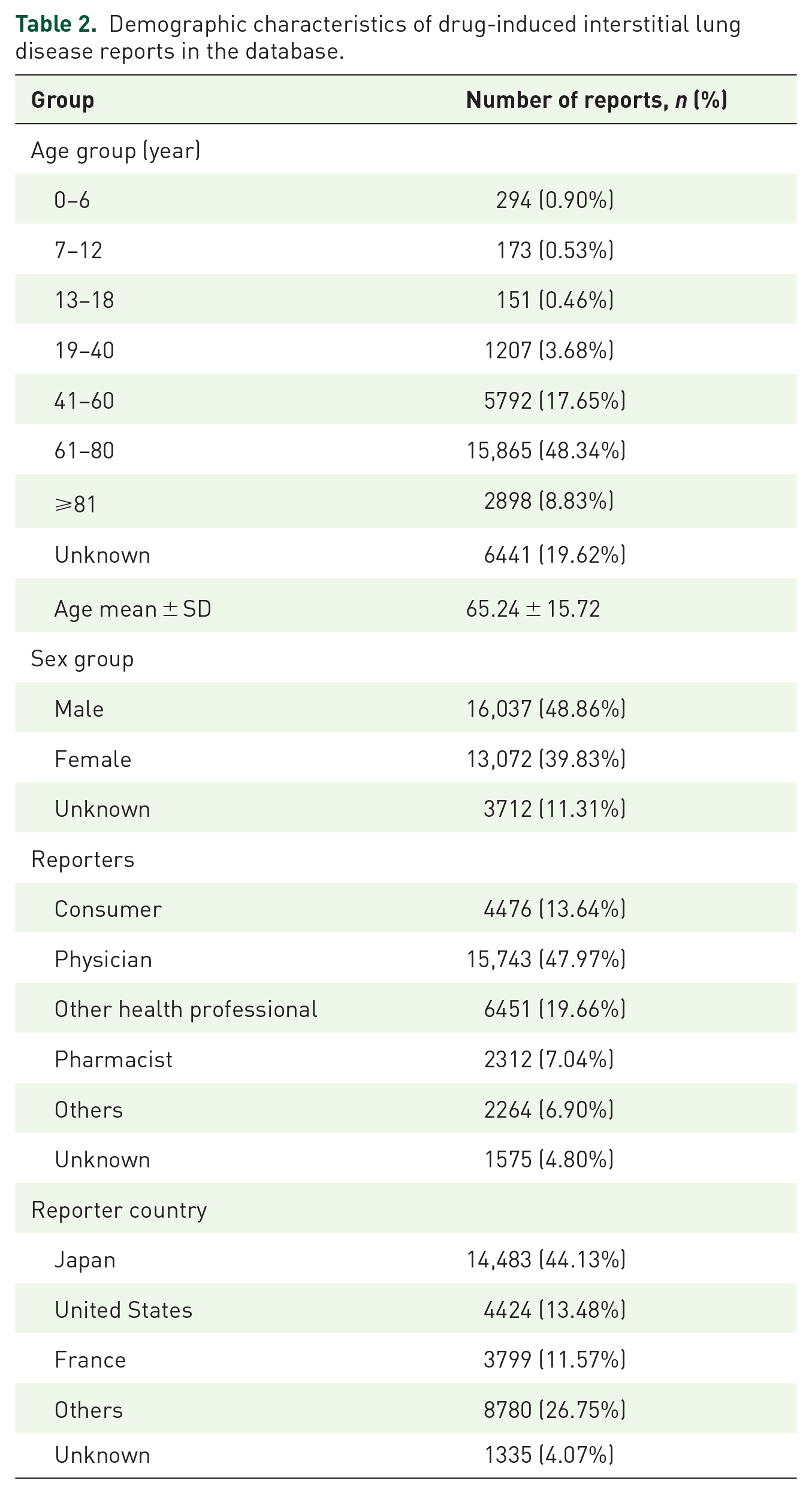
Between 2004 and 2021, the FAERS received 43,046,990 adverse events. In this study, there were 32,821 DILD reports, which accounted for 0.08% of all reports. After excluding incomplete reports such as age and gender absence, a total of 25,501 reports were obtained. The number of DILD reports continued to increase from 2004 to 2021 [Figure 2(a)]. The year with the most DILD reports was 2020, with 3645 cases. Interestingly, the number of DILD reports exhibited an approximately normal distribution with age, first increasing and then decreasing [Figure 2(b)]. Of those, the 61–80 age group had the highest number of DILD reports, followed by the 41–60 age group and the over 81 age group. These age groups made up 74.82% of the total reports (Table 2). Notably, until 60 years, the number of DILD reports was higher in females, and after that, the opposite was true [Figure 2(b)].

(a) Temporal trends in the number of DILD reports (only for reports with reporting date). (b) Distribution curves of DILD reports in different sex and age groups (only for reports containing age and sex).
Demographic characteristics of drug-induced interstitial lung disease reports in the database.
The proportion of drug classes in different sex and age groups was further analyzed (Figure 3). We found that males over 60 years had higher proportions of antineoplastic agents than females in the corresponding age groups. Cardiovascular, antimicrobial, hematological, and urinary agents also contributed to the rise in DILD reports in males. In addition, we also found that females over 19 years had an advantage in reporting antirheumatic agents compared to males.

Number of drug classes in different age and sex groups (only for reports containing age and sex).
Overall, the number of DILD reports was 1.23-fold for males compared to females (Table 2). As shown in Table 2, the majority of reports submitted to the FDA were from physicians (47.97%), followed by other health professionals (19.66%); the top three countries reporting DILD cases were Japan (44.13%), the United States (13.48%), and France (11.57%).
Nearly 60% of the reports described serious consequences (Table 3), with a high proportion of hospitalizations (initial or prolonged) and deaths. Regarding DILD-related death reports, males were disproportionately affected more than females. The proportion of such cases was observed to be lowest in young adults aged 19–40 years (20.05%) and highest in child patients aged 0–6 years (37.41%). Moreover, the proportion of DILD leading to life-threatening in patients aged 0–6 years was relatively higher than other age groups.
Stratification for the clinical outcomes of drug-induced interstitial lung disease reports.

Exclude reports without age or sex data (depending on the specific measurement).
DE, death; DS, disability; HO, hospitalization (initial or prolonged); LT, life-threatening; OT, others.
Classification of drugs associated with DILD
There were 1047 kinds of drugs related to DILD. The major drug classes related to DILD were antineoplastic, cardiovascular, antirheumatic, antimicrobial, hormone agents, and others (Figure 4). Of those, antineoplastic agents were the most frequently reported drug classes related to DILD, accounting for 47.69% of all DILD reports in the FAERS. During our study period, the years with the highest number of DILD reports for most drug classes were in the latest 3 years (2019–2021), and the median age was mostly 60–70 years. There were some differences in the proportion of drug classes in different sex groups. Except for the antirheumatic, psychotropic, central nervous system, and antiparasitic agents, the proportion of males in most drug classes was higher than females (Figure 4, Table 4). We performed linear regression for the main drug classes related to DILD. Regression of each drug class showed an increasing slope with time. Of these, urinary (0.84, 95% CI: 0.23–1.46, p = 0.009), dermatology (0.99, 95% CI: 0.29–1.69, p = 0.009), and antiparasitic (0.89, 95% CI: 0.41–1.36, p = 0.001) increased faster than any other drug class (Table 4).

The overall spectrum of drug classes reported to drug-induced interstitial lung disease.
The drug classes associated with reports of DILD in the FAERS between 2004 and 2021.
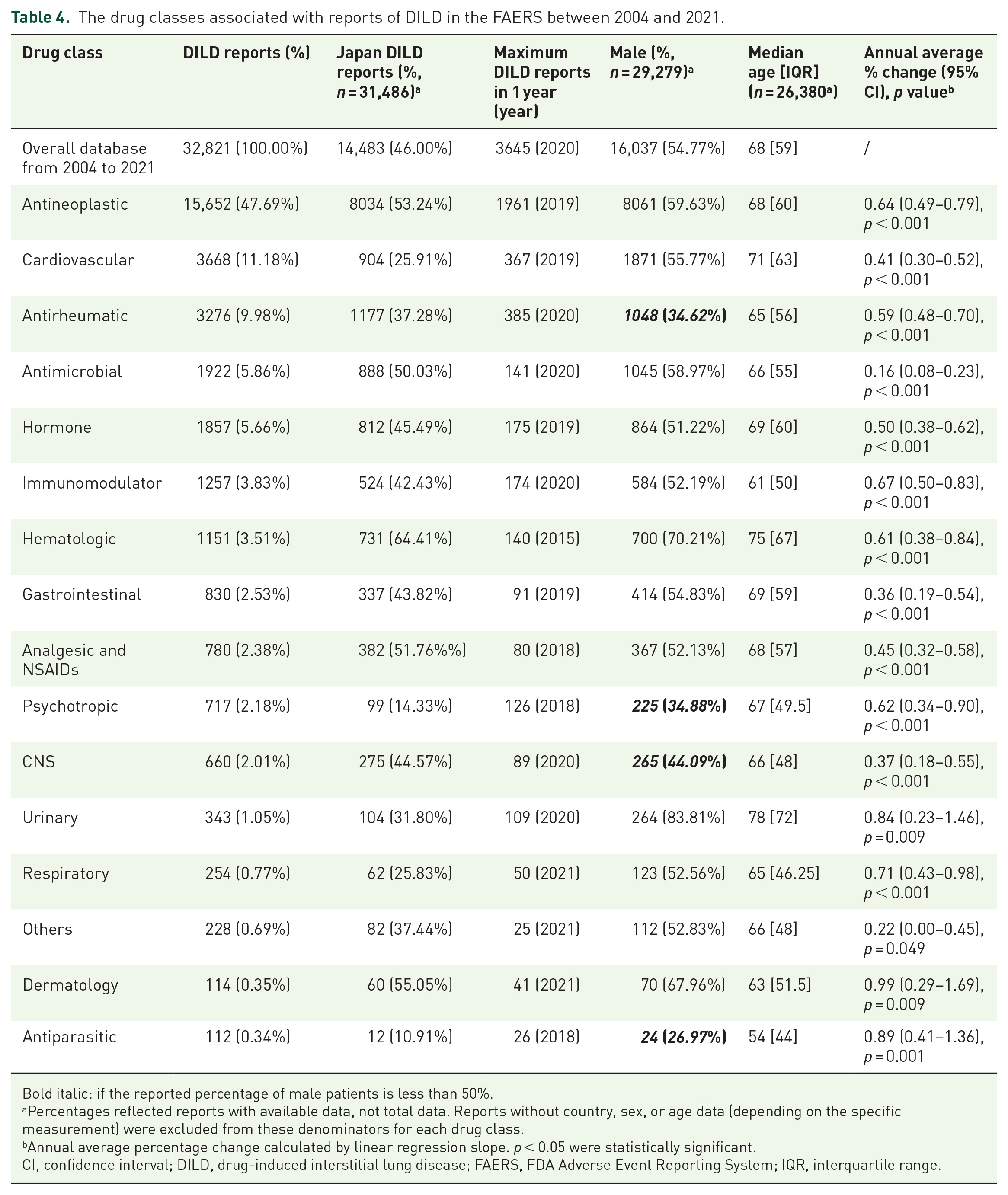
Bold italic: if the reported percentage of male patients is less than 50%.
Percentages reflected reports with available data, not total data. Reports without country, sex, or age data (depending on the specific measurement) were excluded from these denominators for each drug class.
Annual average percentage change calculated by linear regression slope. p < 0.05 were statistically significant.
CI, confidence interval; DILD, drug-induced interstitial lung disease; FAERS, FDA Adverse Event Reporting System; IQR, interquartile range.
Figure 5 listed the top 10 DILD-related drug classes by age. The reported proportion of DILD associated with antineoplastic drugs ranked first in every age group and exceeded 40% in 7–12, 41–60, and 61–80 years. The reported proportion of DILD associated with hematologic agents initially decreased with age (0–6 years: 10.88%, 7–12 years: 5.20%, 13–18 years: 4.64%), and then increased with age (41–60 years: <2.12%, 61–80 years: 3.40%, ⩾81 years: 8.49%). The number of DILD reports associated with cardiovascular agents increased with age (except for the 0–6 years), ranking above 10 in the 7–12 age group and the top 3 after 60 years. The reported proportion of DILD related to antipsychotic agents was higher in the 13–18 and 19–40 years. The reported proportion of DILD associated with antimicrobial agents could be roughly divided into three ranges: (1) 61–80 years with a proportion less than 5%; (2) 7–12, 41–60, and over 81 years with a proportion of 5–10%; and (3) 0–6, 13–18, and 19–40 years with a proportion more than 10%.

Top 10 drug classes related to drug-induced interstitial lung disease reports by age group (only for reports containing age).
Drugs associated with DILD
The top 20 drugs associated with DILD by frequency of reporting were shown in Table 5. These top 20 drugs comprised 10,186 (31.04%) of all reports associated with DILD in the database. Compared with all adverse events of the drug, DILD reports of doxorubicin, pembrolizumab, amiodarone, and osimertinib accounted for more than 1%, respectively. Methotrexate, doxorubicin, etanercept, tocilizumab, infliximab, and osimertinib had a higher proportion of DILD reports in females (Table 5).
Top 20 most reported drugs with interstitial lung disease, by frequency of reporting (FAERS, 2004–2021).

Bold italic: if the reported percentage of male patients is less than 50%; if the reported percentage of DILD reports accounts for more than 1% in all adverse events reports of the target drug.
Percentages reflected reports with available data, not total data. Reports without country, sex, or age data (depending on the specific measurement) were excluded from these denominators for each drug.
DILD, drug-induced interstitial lung disease; FAERS, FDA Adverse Event Reporting System; IQR, interquartile range.
Figure 6 showed the top 10 DILD-related drugs by age group. There were some differences between drugs in different age groups. Defibrotide sodium was the leading drug associated with DILD in the 0–6 years, making up 9.25% of all DILD reported in this group. The proportion of methotrexate related to DILD ranked top in all age groups except the 0–6 years. Cyclosporine has a high frequency of DILD under 60 years old. The frequency of DILD in tacrolimus was significantly higher in minors than in other age groups.

Top 10 drugs associated with drug-induced interstitial lung disease reports by age group (only for reports containing age).
During the study period, we also used a disproportional analysis to mine the potential drugs responsible for DILD. Table 6 showed the top 20 drugs with the highest signal strength in reports of DILD. Fam-trastuzumab deruxtecan-nxki, ramucirumab, and eribulin had the highest ROR, PRR, and IC values, and the proportion of DILD reports accounted for more than 2% (compared with all adverse events of the drug). In the DILD reports of fam-trastuzumab deruxtecan-nxki, eribulin, and pertuzumab, male patients accounted for 10.45%, 9.09%, and 0.85%, respectively, which was significantly lower than that of female patients. Defibrotide sodium is widely used in the treatment of hepatic vein occlusive disease in adults and children. In the DILD reports related to defibrotide sodium, the median age of patients was 6 years old. In addition, we also found that half of the top 20 drugs didn’t mention DILD in the labels, such as amiodarone, temsirolimus, doxorubicin, and ursodiol.
Top 20 drugs most associated with interstitial lung disease, by strength of association (FAERS, 2004–2021).
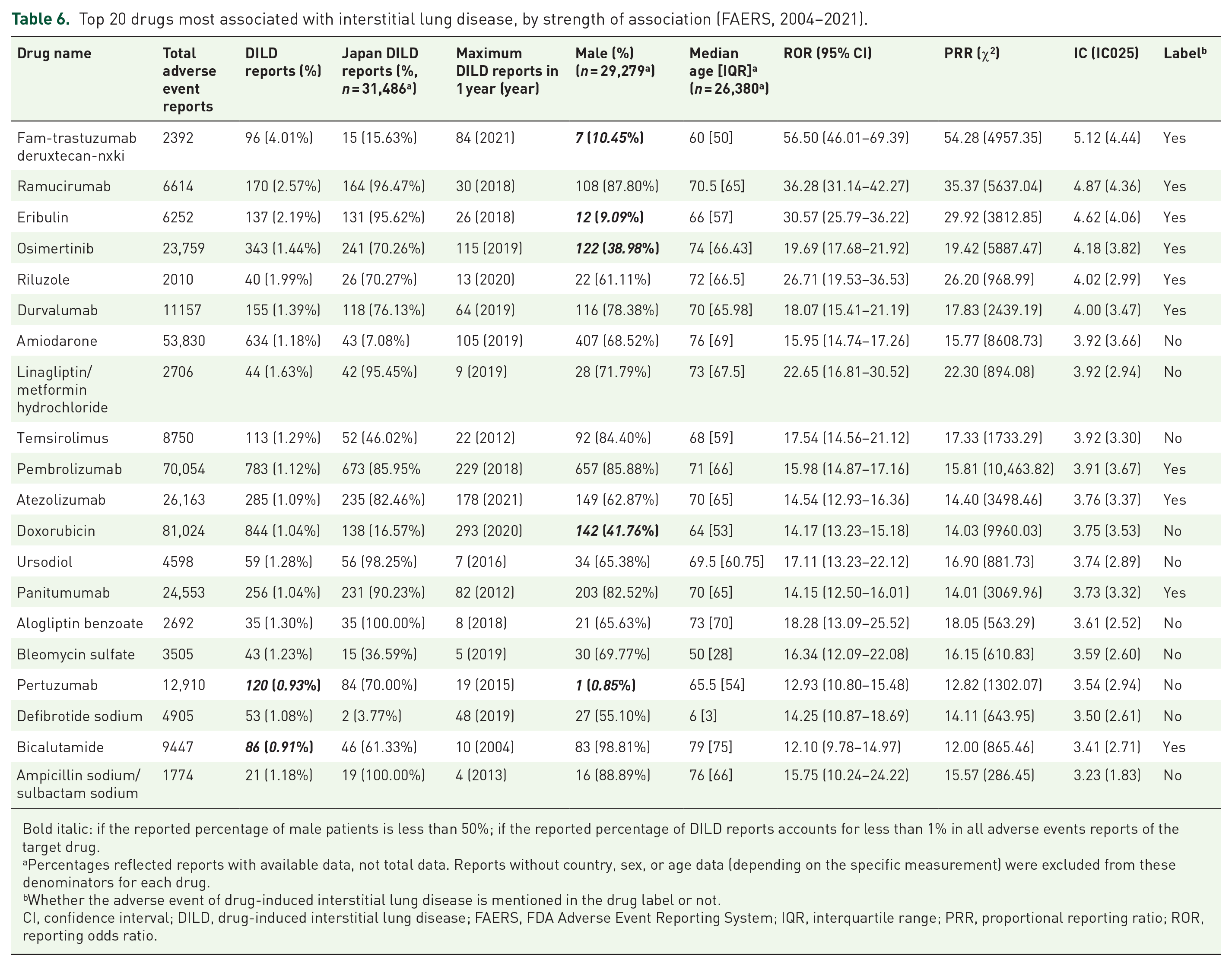
Bold italic: if the reported percentage of male patients is less than 50%; if the reported percentage of DILD reports accounts for less than 1% in all adverse events reports of the target drug.
Percentages reflected reports with available data, not total data. Reports without country, sex, or age data (depending on the specific measurement) were excluded from these denominators for each drug.
Whether the adverse event of drug-induced interstitial lung disease is mentioned in the drug label or not.
CI, confidence interval; DILD, drug-induced interstitial lung disease; FAERS, FDA Adverse Event Reporting System; IQR, interquartile range; PRR, proportional reporting ratio; ROR, reporting odds ratio.
Data comparison of reporting countries
DILD reports submitted by Japan accounted for 46.00% (14,483/31,486) of that by related countries. As shown in Table 4, in DILD cases reported in Japan, psychotropic drugs (14.33%) and antiparasitic drugs (10.91%) accounted for less than 15%. All other drug classes were in the range of 25–65%.
Of the top 20 frequently reported drugs (Table 5), pembrolizumab, nivolumab, bevacizumab, osimertinib, and cyclosporine reported more than 70% of their DILD cases in Japan, whereas methotrexate, amiodarone, and rituximab had less than 10% of their DILD cases in Japan. Methotrexate, amiodarone, and rituximab were all in the top 10 DILD-related drugs in the FAERS, so the reported cases of these three drugs were contributed by other countries outside Japan.
To better discern the source of DILD cases reported outside Japan, we identified the three non-Japanese countries (the United States, France, and Canada) that reported the most DILD cases in the FAERS and examined the top 10 drugs that the most frequent occurrence of DILD in each country (Table 7).
The top four countries associated with DILD in the FAERS between 2004 and 2021 – top 10 drugs.
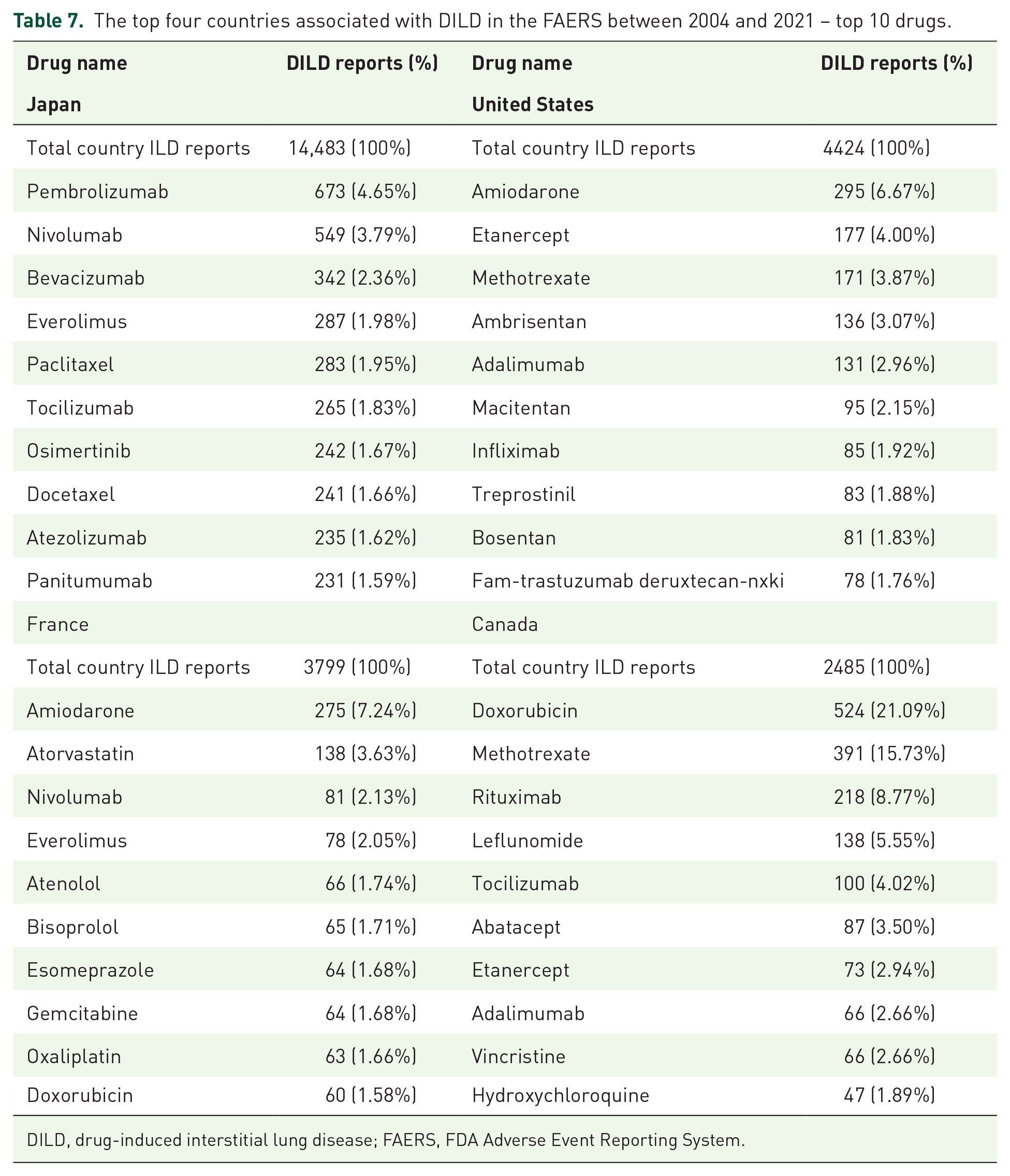
DILD, drug-induced interstitial lung disease; FAERS, FDA Adverse Event Reporting System.
There are significant differences in the top 10 drugs with the most frequent DILD in various countries. According to the classification of the top 10 drugs reported in each country, we found monoclonal antibodies accounted for 6 of the top 10 drugs reported in Japan related to DILD. And it also made contributions to the top drug in the United States and France. Additionally, 9, 5, and 4 of the top 10 drugs in Japan, France, and Canada were antineoplastic agents, respectively. Cardiovascular agents accounted for 50% of the top 10 drugs reported in the United States. Half of the top 10 drugs reported in Canada were related to antirheumatic agents, whereas France was the only country with no antirheumatic agents in its top 10 drugs.
Discussion
DILD has a significant impact on the health and quality of life of patients. More than 350 drugs may cause DILD, but most drugs cannot be discovered until later in development or after post-marketing. 5 Due to the unpredictability of DILD, the lack of specific biomarkers, histological manifestations, and diagnostic clinical features, the unclear pathogenesis, and the possibility of life-threatening or disabling conditions, the prediction and characterization of DILD in preclinical drug development and post-marketing have brought extreme challenges to clinicians, the pharmaceutical industry, and health regulators. 22
From 2004 to 2021, reports of DILD increased year by year. The reasons for this may be likely multifactorial. First, the drug safety awareness of the public and the pharmaceutical industry has gradually enhanced, resulting in greater attention to adverse events. 23 And second, several contributing facilitators might promote the reporting of adverse events, including institutions engaged in risk evaluation and mitigation strategies, more stringent regulatory authorities, and the convenience of the Internet. 24
During the study period, we observed significant differences related to age and sex in all DILD cases submitted to the FDA. In total, 57.17% of all reports of DILD were over 60 years, and males were more frequently reported than females. We have also observed the age- and sex-related risks in clinical outcomes, with higher death rates in older/male patients. It has been reported that smoking is an important risk factor for patients with DILD, and male smoking preference is more than female, which may be the reason for the higher frequency of male reporting. 5 However, in some drug classes, female patients reported more than male patients, such as antirheumatic agents. The possible reason is that the drugs themself for diseases with female susceptibility or unique (such as rheumatoid arthritis and menstrual disorders).25,26 The mechanism of DILD remains unclear, which may be mainly related to the allergic reaction and direct cytotoxicity caused by drugs and their metabolites. 22 Of those, oxidative stress is considered a risk factor for the occurrence and progression of lung tissue damage. 27 With age, the antioxidant capacity of the human body, the activity of drug-metabolizing enzymes, the anti-inflammatory reaction, and the repair ability are all reduced, so more DILD may occur. In addition, the underlying diseases of the elderly are one of the significant reasons for DILD. For example, patients with underlying respiratory disease may die from mild DILD28–30; for patients with underlying renal disease, prolonged excretion of certain drugs may increase the risk of DILD.31,32 It is worth paying attention that the elderly, as a high-risk group, will increase the number of cases and social burden of DILD as the global population ages, and global public health management will face more challenges.
In our study, antineoplastic agents were the most frequently reported drug class that induced DILD. A study found that the incidence of respiratory failure caused by DILD was 6.6 per 100,000 patients per year, with more than half of the cases related to chemotherapy. 33 It also had been reported that antineoplastic agents were the primary cause of DILD, accounting for 23–51% of all reported cases. 34 As a major complication in cancer treatment, DILD increases the risk of drug withdrawal and death.35,36 Moreover, many new antineoplastic agents have been widely used in medicine over the past few years. In our study, we found that monoclonal antibodies, as an emerging therapy against cancer, had a high volume in the frequency of DILD reported in multiple countries. However, this scenario may correspond to the increased use of monoclonal antibodies in treatment. Some monoclonal antibodies have been reported in association with true DILD, such as fam-trastuzumab deruxtecan-nxki, nivolumab, pembrolizumab, and others.37–43 Of these, fam-trastuzumab deruxtecan-nxki was the top drug related to DILD reported to the FDA, with an incidence of 15.8% and a mortality of 2.4% in clinical trials.44,45 While some reports may be confused by its off-label therapy.39,46 On the other hand, we also noted that half of the top 20 drugs with high strength of association did not mention DILD in the labels. It draws attention that healthcare professionals should enhance monitor related to drugs of potential importance. In short, DILD brings a higher risk of drug withdrawal and death, as well as the emergence of many new antineoplastic agents with the lack of real-world safety data makes patients confused about drug selection. The results of our study can help physicians choose drugs with low DILD risk from similar effects to improve patient compliance and survival rate.
At the same time, we observed significant country-related differences in DILD reports in the FAERS. In Japan, the United States, France, and Canada, 60–70% of the top 10 drugs most related to DILD were antineoplastic agents, consistent with their high tumor incidence rate. 47 The proportion of cardiovascular agents in the United States was significantly higher compared to other countries, which was related to its higher cardiovascular burden. 48 Four and five antirheumatic agents were found in the frequently reported top 10 drugs in the United States and Canada, respectively. It may be related to the higher prevalence in North America compared to other regions. 49 These differences across countries can be attributed to differences in disease maps, demographics, genetic effects, drug use patterns, and reporting rates. Furthermore, our research showed that more than one-third of the reports came from Japan, seeming to indicate a higher prevalence of DILD in Japan. However, due to coding and spontaneous reporting, most of them are considered to be man-made rather than biological. 50 In contrast to Japan, many regions of the world have reported little data on DILD to FAERS, including Africa and much of Asia.
We respectively calculated the ROR, PRR, and BCPNN to detect the correlation strength between an individual drug and DILD. van Puijenbroek et al. 21 found that these methods have different advantages and limitations. Different health regulators use various statistical indicators to measure the correlation between drugs and adverse events, such as ROR currently used by Lareb in the Netherlands, PRR by the UK Medicines and Healthcare Products Regulatory Agency, and BCPNN by the World Health Organization Drug Monitoring Centre in Uppsala. Each of these methods may lead to different sensitivities and specificities in signal risk detection, with no single measure of effect superior to others. 51 Therefore, we utilized ROR, PRR, and BCPNN to detect the risk drug in the DILD database to reduce the generation of false-positive signals. Moreover, many previous studies and papers have used these methods to detect adverse event signals in spontaneous reporting systems.52–54
Limitations
There were limitations in this study. FAERS is an adverse drug reaction spontaneous reporting system with a lack of denominator data and a high false report rate, limited by uncertain causality, repeated reports, missing information, and spelling errors. Therefore, the data are biased against the true incidence of DILD.55,56 We obtained the ROR, PRR, and IC values according to the reported frequency of the combination of drugs and adverse events. This value represents the adjustment between the DILD ratio reported by a drug and the ratio of all other adverse events reported for the target drug. They calculate the reporting risk rather than the risk of DILD occurrence. 52 There are differences in drug use and race in various countries and regions. Nevertheless, the FAERS database lacks ethnicity data, an indispensable part of considering the environmental and genetic factors that lead to adverse events. Moreover, there was a ‘Weber effect’ in the FAERS database, where adverse event reports peaked in the initial post-marketing phase and following declined year after year. 57 Nonetheless, it still provides references to formulate precise and targeted policies to prevent DILD in the real world.
Conclusion
In a review of the FAERS database, we uncovered that the top drug classes associated with DILD in FAERS were antineoplastic, cardiovascular, and antirheumatic agents, in varying order in different sexes/age. Fam-trastuzumab deruxtecan-nxki, ramucirumab, and eribulin had the highest strength of association with DILD. We also found some unexpected drugs without DILD in the labels, such as amiodarone, doxorubicin, and ursodiol. Our findings provided real-world data for the development of novel management strategies of drug-related adverse events.