
Abstract
Aims:
To investigate the safety of oral iron therapy in pregnant women with iron-deficiency anemia (IDA) in the real world.
Methods:
A retrospective analysis was performed on 1792 pregnant patients with IDA who received oral iron supplements from 12 hospitals in Shandong Province from 1 April to 31 June 2021; follow-up and adverse reactions were recorded. They were divided into six groups according to the treatment drugs.
Results:
The overall adverse reaction rate was 15.4%, and the main adverse reaction site was the digestive system. The incidence of all kinds of oral iron adverse reactions from high to low in order: compound ferrous sulfate and folic acid tablets (21.88%); iron proteinsuccinylate oral solution (20.90%); ferrous succinate tablets (19.76%); ferrous succinate sustained-release tablets (18.00%); iron polysaccharide complex capsule (12.06%); and iron dextran oral solution (6.94%). It was found that there was a significant difference in the incidence of adverse reactions among the six drugs (p < 0.05). Pairwise comparison showed that the incidence of adverse reactions was higher in the iron proteinsuccinylate oral solution than that in the iron polysaccharide complex capsule (p < 0.05). There was no significant difference in the incidence of adverse reactions in different ages (p > 0.05), but there was a significant difference in the incidence of adverse reactions in different gestational ages (p < 0.05). In Adverse Drug Reaction (ADR) patients, the adverse reaction result of most patients is recovery or improvement, and there was no serious adverse reaction outcome such as sequela and death.
Conclusion:
All the adverse reactions of oral iron were mainly gastrointestinal adverse reactions, and no heavy adverse reactions were found. Iron proteinsuccinylate oral solution has a higher incidence of adverse reactions than iron polysaccharide complex capsule. The results showed that oral iron was safer for anemia patients during pregnancy.
Plain language summary
Introduction
Iron-deficiency anemia (IDA) is a global health problem and a major cause of morbidity in women. The population bearing the highest risk for developing iron depletion is women of fertile age, and they may lose abnormally high amounts of blood during each menstruation period without being aware that the loss is excessive. 1 When the iron deficiency is severe, it may lead to a decrease in hemoglobin (Hb) concentration, a situation known as IDA, which affects a third of women of childbearing age worldwide. 2 IDA is a common complication of pregnancy, being more rampant in the developing countries. Pregnant women are more likely to suffer from anemia owing to increased blood volume during pregnancy 3 and to a greater demand for nutrients during fetal growth. 4 Anemia that occurs before pregnancy and is left untreated can increase the metabolic demand during pregnancy. 5 The World Health Organization (WHO) estimates that 32 million pregnant women were affected by anemia in 2011, of which 50% were attributed to iron deficiency. 6 Pregnancy significantly increases the need for iron; this increased demand for iron subsequently places the mother and infant at risk of developing IDA, which can lead to gestational complications, as well as increased maternal and infant morbidity and mortality.7–10 Iron deficiency and anemia during pregnancy are associated with adverse maternal and fetal outcomes, including neurocognitive deficits in children born to iron-deficient mothers. 11 Some clinical studies have shown that anemia during pregnancy is associated with stillbirth, 12 preterm birth, 13 and low birth weight (LBW). 14 Favorable pregnancy outcomes occur 30–45% less frequently in anemia mothers. Therefore, anemia during pregnancy remains a major public health problem.
Oral iron drugs are the first-line treatment for IDA during pregnancy. However, different drugs have different efficacy and safety. 15 We found that at present, the safety evaluation of iron supplements for anemia during pregnancy mainly focuses on intravenous iron supplements, and there is no comprehensive study on the safety of commonly used oral iron supplements. In this study, we compared the safety of six commonly used oral iron supplements in the treatment of IDA during pregnancy, so as to provide a reference for clinical medication. The study protocol was approved by the hospital’s ethics committee (NO. QFALL-KY-2021-15).
Materials and methods
The general information
A total of 1792 pregnant women with anemia who were admitted to the obstetrics clinic of 11 tertiary A hospitals and 1 tertiary B hospital in Shandong Province of China from 1 April to 31 June 2021 were selected as the research objects. The 12 hospitals were Qingdao Women and Children’s Hospital, Shandong Provincial Hospital, Shandong Qianfoshan Hospital, Shandong Second People’s Hospital, Qingdao Haici Hospital, Qingdao municipal hospital, Linyi Maternal and Child Health Care Hospital, Jinan Maternal and Child Health Hospital, Weifang Maternal and Child Health Hospital, Tengzhou City Maternal and Child Health Hospital, Zaozhuang Maternal and Child Health Hospital, and Taian Maternal and Child Health Hospital. They were divided into six groups according to the treatment drugs: compound ferrous sulfate and folic acid tablets group (64 cases), iron proteinsuccinylate oral solution group (268 cases), ferrous succinate tablets group (167 cases), ferrous succinate sustained-release tablets group (350 cases), iron polysaccharide complex capsules group (871 cases), and iron dextran oral solution group (72 cases). All patients had mild or moderate anemia, and no severe anemia.
Inclusion and exclusion criteria
Inclusion criteria: All patients met the diagnosis of “pregnancy complications” in the “Guidelines for the diagnosis and treatment of iron deficiency and iron deficiency anemia in pregnancy” issued by the WHO and the Chinese Society of Perinatal Medicine. That is, pregnancy with IDA, Hb concentration <110 g/L patients. Hb concentration can be divided into mild anemia (100–109 g/L), moderate anemia (70–99 g/L), severe anemia (40–69 g/L), and extremely severe anemia (<40 g/L).
Exclusion criteria: Patients with thalassemia or other hereditary anemias, sideroblastic anemias, megaloblastic anemias, hyperemesis gravidarum, or overuse of combination medications were not included in the study.
Treatment
Compound ferrous sulfate and folic acid tablets group: compound ferrous sulfate and folic acid tablets, oral, 0.2 g/time, 3 times/day; iron proteinsuccinylate oral solution group: iron proteinsuccinylate oral solution, oral, 0.04 g/time, twice a day; ferrous succinate tablets group: ferrous succinate tablets, 0.2 g/time, twice a day; ferrous succinate sustained-release tablets group: ferrous succinate sustained-release tablets, oral, 0.2 g/time, once a day; iron polysaccharide complex capsule group: iron polysaccharide complex capsule, oral, 0.15 g/time, once a day; iron dextran oral solution group: iron dextran oral solution, oral, 0.05 g/time, twice a day.
Observation indicators
The adverse reactions of the six groups were compared, including nausea, vomiting, abdominal pain, abdominal distension, diarrhea, dyspepsia, constipation, dizzy, rash, vomiting, burning, decreased appetite and so on; Hb levels before and after treatment; the outcome, severity, causality and frequency of adverse events in the six groups.
Statistical methods
IBM SPSS Statistics 23 software was used for statistical analysis to compare the incidence of adverse reactions of different types of oral iron, different ages, and different gestational ages. Measurement data were expressed as mean ± standard deviation (x ± s), and One-way ANOVA method was used. Chi-square test, Fisher exact test, and Yates continuity correction were used to compare the quantitative data between groups (p < 0.05 was statistically significant.). If the overall incidence of adverse reactions was statistically significant, further pairwise comparisons were made, that is, multiple comparisons.
Results
Comparison of general data
Among the 1792 samples, 8 samples were of no age and 50 samples were of no gestational age, so general data were not included. All patients included in the study ranged in age from 16 to 44 years and gestational age from 4 to 40 weeks. According to gestational age, the samples were divided into four groups: low age group (<20), appropriate age group (20–34), advanced age group (35–39), and super age group (⩾40). According to the stage of pregnancy, it was divided into three stages: first trimester (<14 weeks), second trimester (⩾14 weeks, <28 weeks), and third trimester (⩾28 weeks). Baseline mean Hb levels in six groups were in the range of mild anemia (Hb: 100–109 g/L). General information is compared as follows (Table 1).
Comparison of general data among the six groups.

Hb, hemoglobin.
Incidence of adverse reactions in the six groups
Among the six groups, 276 ADR patients reported 302 adverse reactions. The incidence of adverse reactions from high to low was as follows: compound ferrous sulfate and folic acid tablets (21.88%); iron proteinsuccinylate oral solution (20.90%); ferrous succinate tablets (19.76%); ferrous succinate sustained-release tablets (18.00%); iron polysaccharide complex capsule (12.06%); and iron dextran oral solution (6.94%). Statistical results showed that there were statistically significant differences in the incidence of adverse reactions among the six drugs (p < 0.01). The results of pairwise comparison showed that the incidence of adverse reactions of iron protein succinate oral solution was higher than that of iron polysaccharide complex capsule (p < 0.01), and there was no statistically significant difference in the incidence of adverse reactions of the other four oral iron agents (Table 2).
The number of adverse reaction reports in the six groups.

Compared with iron polysaccharide complex capsule group.
p < 0.05.
Adverse reactions accumulated organ systems and clinical manifestations
The treatment was similarly well tolerated during the follow-up. The main site of adverse reactions in ADR patients is the digestive system, mainly gastrointestinal (GI) adverse reactions. The main clinical manifestations include nausea, vomiting, constipation, burning sensation, abdominal pain, diarrhea, etc. Statistical analysis showed that the higher incidence of adverse reactions was constipation (6.96%), nausea (2.54%), diarrhea (1.89%), and vomiting (1.29%). Among them, the drug with a high incidence of constipation was iron proteinsuccinylate oral solution (11.19%), the drug with a high incidence of nausea was compound ferrous sulfate and folic acid tablets (9.38%), and the drug with a high incidence of diarrhea was ferrous succinate tablets (3.59%). No patients opted out because of adverse events, the specific results are shown in the Figure 1.
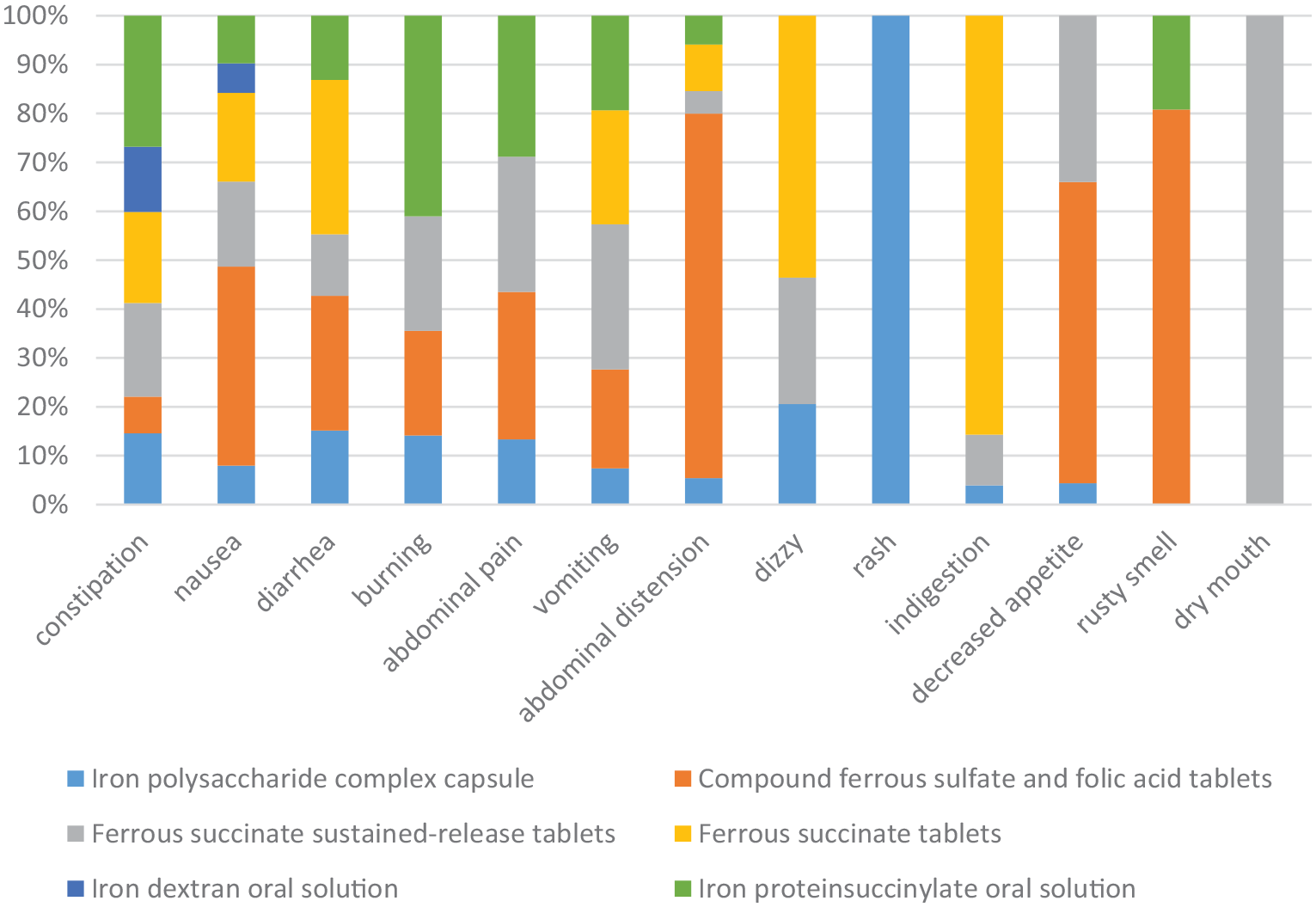
Main clinical manifestations and numbers of adverse reactions (%).
The distribution of age and gestational age of ADR patients
Patients were divided into low age group, appropriate age group, advanced age group, and super age group according to their age. There was no statistically significant difference between the four groups (p > 0.05). Among them, the incidence of adverse reactions was highest in the low age group, which was 30%. Among 276 patients with adverse reactions, 18 patients had no pregnancy week information, so no statistics were made. There were significant differences in the incidence of adverse reactions among the three different gestational age groups (p < 0.05). The incidence of adverse reactions in the first trimester was significantly higher than that in the second trimester, which was 25.67% (Tables 3 and 4).
Incidence of adverse reactions in each age.

Incidence of adverse reactions in each gestational age.
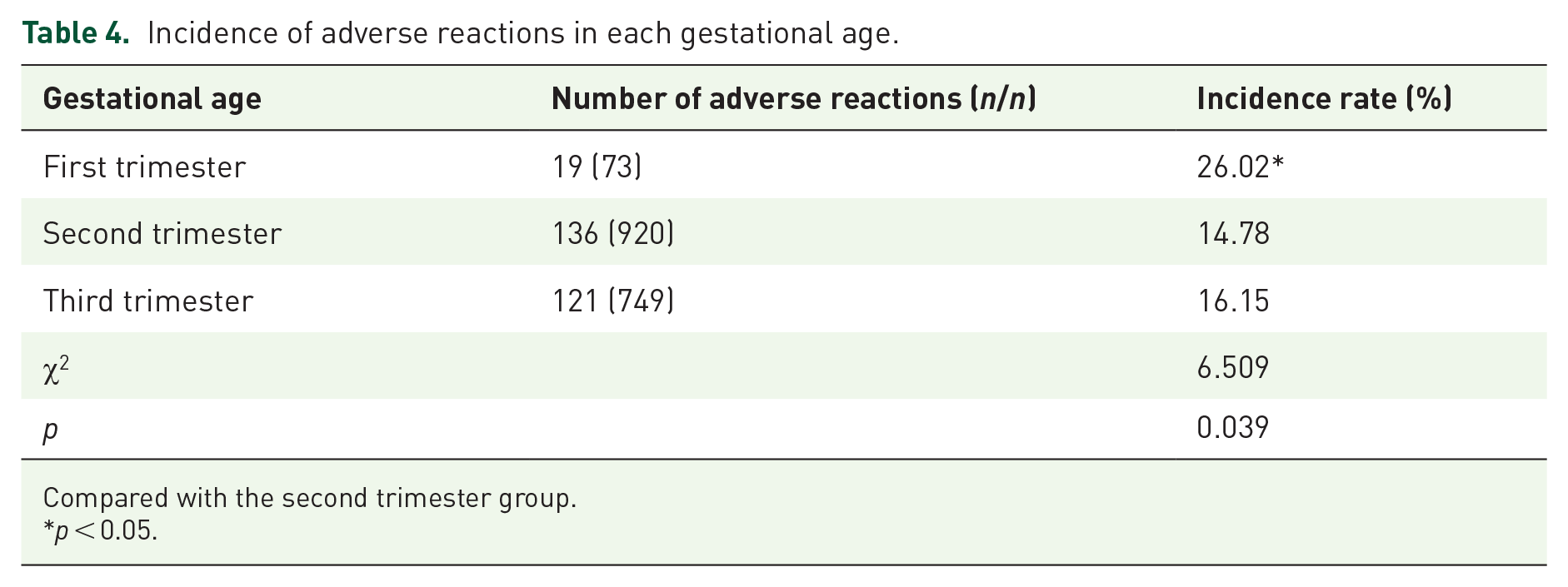
Compared with the second trimester group.
p < 0.05.
Comparison of therapeutic effect among six groups
The Hb level of the six groups before and after treatment was compared. Comparison of Hb level in six groups before treatment (p < 0.05), but paired comparison showed no statistical significance between groups (p > 0.05). After treatment, the Hb level of the six groups was higher than that before treatment, and the difference was statistically significant (p < 0.05). There was statistical significance in the comparison between the ferrous succinate sustained-release tablets group and the iron dextran oral solution and ferrous succinate tablets group (p < 0.05). Before treatment, the baseline average Hb level of the six groups was mild anemia. After treatment, the average Hb level of the three groups of compound ferrous sulfate and folic acid tablets, ferrous succinate sustained-release tablets, and iron polysaccharide complex capsule was >110 g/L; the other three groups were still in the range of mild anemia (Table 5).
Hb level before and after treatment in six groups.

Compared to before treatment.
p < 0.05, compared with ferrous succinate sustained-release tablets group.
p < 0.05, compared with compound ferrous sulfate and folic acid tablets group.
p < 0.05.
Hb, hemoglobin.
New adverse reactions and serious adverse reactions
The new adverse symptom of iron polysaccharide complex capsule was rash. Two patients with rash had no history of drug allergy. All adverse reactions were general, and no heavy adverse reactions were found.
Outcome of adverse reactions
Among 302 ADR events, the adverse reaction outcomes of 273 patients were collected, 29 patients were lost to follow-up, and the outcome of adverse reactions could not be determined. Most of the adverse reactions were cured or improved (Table 6), and no serious adverse outcomes such as sequelae and death occurred in each group.
Outcome of adverse reactions [n (%)].

Comparison of causality, severity, and frequency of adverse events in six groups
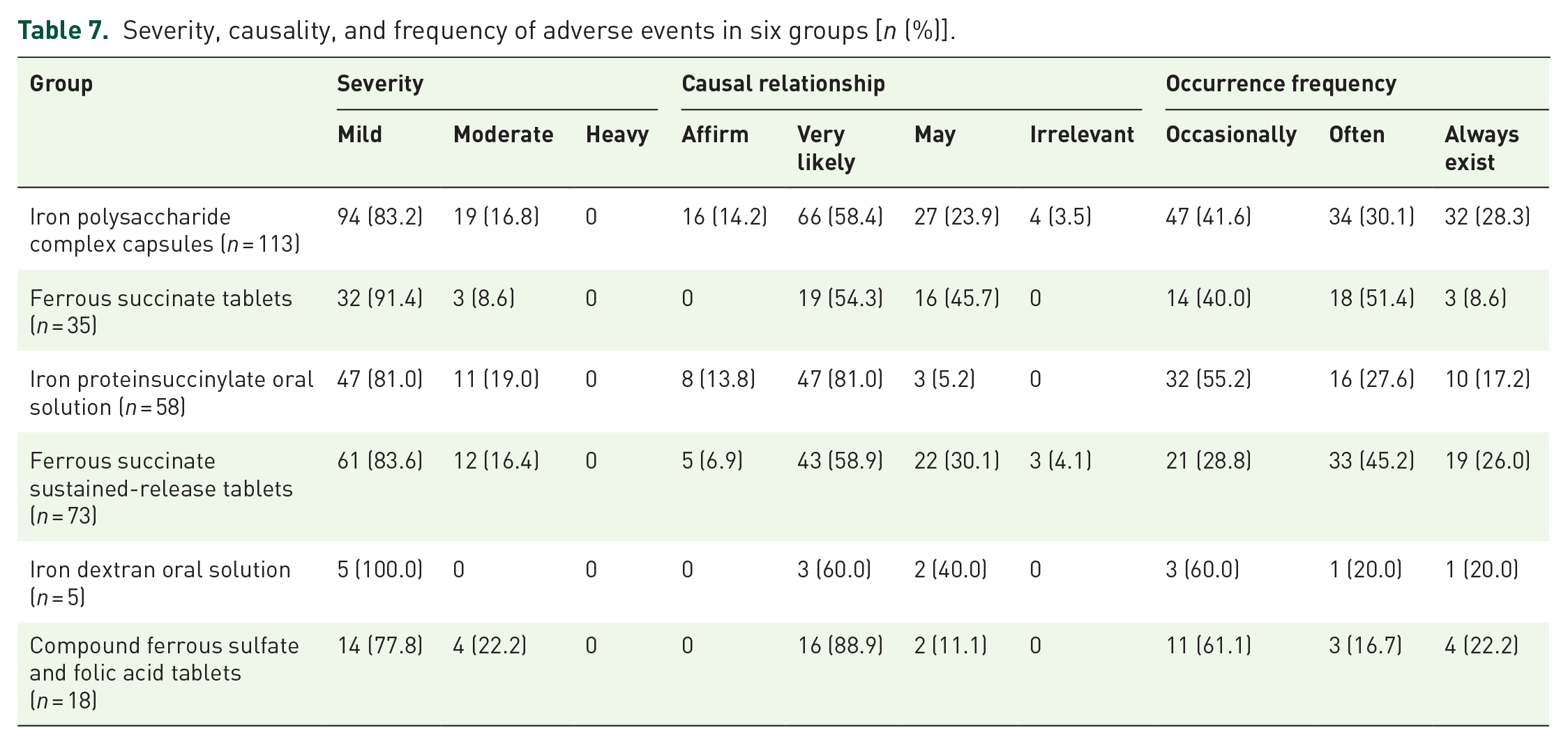
The severity of adverse events was mostly mild and rarely moderate, no heavy adverse reactions. Most adverse events are likely to be related to oral medications; the frequency of adverse reactions was occasional or frequent, and very few patients showed persistent phenomenon (Table 7).
Severity, causality, and frequency of adverse events in six groups [n (%)].
Discussion
Maternal anemia is strongly associated with maternal and perinatal mortality. When occurring in pregnancy, anemia increases the risk of adverse maternal, fetal, and neonatal outcomes.16,17 These adverse outcomes include maternal mortality, preterm and LBW deliveries, perinatal and neonatal deaths, and long-term developmental sequelae in the surviving offspring. 18 The infants may also suffer iron deficiency, which may lead to developmental impairment. Therefore, such pregnancy complications need to be paid attention to clinically. By reviewing the literature, there are two main ways to treat IDA: intravenous iron and oral iron. There are many clinical comparative studies of oral and intravenous iron in the treatment of anemia.19–22 Oral iron is the most commonly prescribed therapy for pregnant women with mild-to-moderate anemia.23,24 Use of oral iron is primarily limited by its GI side effects that are mediated by non-absorbed iron. Although newer preparations were claimed to have less side effects, ferrous sulfate is still the most commonly used oral iron preparation.25–27 At present, the main oral iron agent is divalent iron agent, which has some shortcomings such as low iron absorption rate, large GI stimulation response, and relatively slow onset effect, which affect the therapeutic effect to some extent. 28 Compound and sustained-release preparations such as compound ferrous sulfate folic acid and compound ferrous sulfate sustained-release tablets have appeared, which has improved the bioavailability and reduced GI adverse reactions. New oral preparations, such as polysaccharide–iron complex and iron dextran, are made from ferric iron instead of divalent iron, and then compounded with other compounds, reducing the production of free iron and improving the iron. As far as we know, there is no comprehensive study on the safety of six commonly used oral iron in the treatment of IDA during pregnancy: iron polysaccharide complex capsules, iron proteinsuccinylate oral solution, ferrous succinate sustained-release tablets, ferrous succinate tablets, compound ferrous sulfate and folic acid tablets, and iron dextran oral solution. Therefore, this study evaluated the safety of oral iron supplements commonly used in women with anemia during pregnancy in the real world, in order to further guarantee the drug safety of women with anemia during pregnancy.
According to the results of multi-center investigation, off-label use is rare, and it is more in line with the technical guidelines such as the “Guidelines for the diagnosis and treatment of iron deficiency and iron deficiency anemia in pregnancy.” All adverse reactions are given priority to with GI side effects; higher rate of adverse reactions for constipation, nausea, diarrhea, vomiting, the results were similar to those of other studies.29–33 In terms of the incidence of adverse reactions, new oral iron agents such as polysaccharide–iron complex and iron dextran have lower incidence of adverse reactions and fewer side effects. This is consistent with the results of some previous studies, controlled-release iron preparations and polysaccharide–iron complexes were found to have fewer GI side effects than ferrous sulfate in a few randomized trials.33,34 The results showed that there was a significant difference in the incidence of adverse reactions between the ferritin succinate oral solution group and the iron polysaccharide complex capsule group, while there was no significant difference in the incidence of adverse reactions in the other four categories, indicating that the safety was consistent. New adverse reactions such as skin rash (0.23%) were found in the follow-up, which should be monitored in clinical use, and the manufacturer is suggested to revise the instructions. According to the results of this study, the adverse drug reactions of oral iron in pregnant women with IDA are mostly mild to moderate, and no heavy adverse reactions were observed, and the safety of oral iron is relatively good in the real world.
This safety evaluation belongs to a real-world study, that is, a large sample of non-intervention registries. Women with anemia during pregnancy who took oral iron from 1 April to 31 June 2021 in 12 hospitals in Shandong Province were enrolled as subjects, and the required data were collected, followed up, and analyzed. Through the analysis of multi-center and large sample data in Shandong Province, the widespread use of drugs in the real world and the occurrence of adverse reactions were evaluated, so as to provide more accurate basis for clinical application. As a multi-center study, this study also has certain limitations, such as errors in data filling and imbalance in the number of cases in each group. After that, oral iron preparations with relatively small number of cases can be expanded and improved to obtain more reliable and safe data. Nevertheless, we can still find the characteristics of adverse reactions when using oral iron supplements in patients with anemia during pregnancy. The use of oral iron in the treatment of anemia during pregnancy should be reasonable and standardized according to the patient’s own conditions, drug indications strictly followed, and the monitoring of adverse reactions should be strengthened to ensure the safety of medication in the anemia population during pregnancy.
In conclusion, the above six oral iron agents have good safety in the treatment of IDA during pregnancy, which provides a reference for the clinical treatment of such diseases.