
Abstract
Objective:
The aim of this study was to determine the pattern and outcomes of higher-order multiple pregnancies in a tertiary hospital in Nigeria
Methods:
This is a retrospective review of all cases of higher-order multiple pregnancies that were managed between 1 January 2012 and 31 December 2016 in Alex Ekwueme Federal University Teaching Hospital Abakaliki, Nigeria. Data obtained were represented with frequency tables, percentages, bar charts, and odds ratio.
Results:
There were 22 higher-order multiple pregnancies over the study period and 12,002 deliveries, giving a higher-order multiple prevalence rate of 0.2%. Five of the mothers (four triplets and one quadruplet) had in vitro fertilization (0.4 per 1000 deliveries), while other mothers conceived naturally. Many of the women (12, 54.6%) were in the 30–34 years age group, and more than half (16, 72.7%) were multiparas. More than half of the neonates were delivered preterm (13, 59.1%). Being booked is associated with better neonatal outcomes although not significant (odds ratio = 3.06. 95% confidence interval: 0.55–16.83, p = 0.197). Anemia was common in the antepartum and postpartum periods. Half of the women (11, 50%) were delivered by elective cesarean section and 7 (31.8%) by emergency cesarean section (C/S), while 4 (18.2%) had a spontaneous vaginal delivery. The neonates had a mean birth weight of 2.14 ± 0.35 kg. Overall, 61 neonates (91.0%) were born alive and 6 (9.0%) suffered perinatal deaths, giving a perinatal mortality rate of 89.8 neonates per 1000 live births.
Conclusion:
Our study shows that higher-order multiple pregnancies are high-risk pregnancies that are associated with fetal and maternal complications. Anemia is the commonest complication seen in our study. The majority had preterm delivery. Proper antenatal care and close feto-maternal monitoring are important in reducing adverse outcomes associated with these pregnancies.
Keywords
Introduction
Higher-order multiple (HOM) pregnancy occurs when more than two fetuses are present in the uterus at the same time.1,2 Globally, the prevalence of HOM pregnancy has been on the increase, and this has been attributed to the increased rate of ovulation induction, assisted reproductive technologies (ARTs), and increasing maternal age at conception. 3 The incidence of HOM pregnancy ranges from 0.01% to 0.07% of all pregnancies.1,2 Racial differences have a relative influence on the incidence of HOM pregnancies. 4 It has been reported that the comparable incidence of triplets among the White and Black population in the United States was 0.109/1000 pregnancies (1:9183) and 0.197/1000 pregnancies (1:5076), respectively. 4 In Southwest Nigeria, the rate of triplet births (1.6/1000 pregnancies) is markedly higher than in Caucasian populations (0.09–0.1/1000 pregnancies). 4 Umeora et al. 5 and Esike et al. 6 in Nigeria reported an incidence of one triplet pregnancy in 1014 and 771 deliveries, respectively. According to the work of Fajolu et al. 3 in Nigeria, the prevalence of triplets, quadruplets, and quintuplets was reported to be 0.23%, 0.09%, and 0.02%, respectively. Spontaneous quadruplet pregnancy is very uncommon and it is estimated to occur in 1 in 512,000 to 1 in 677,000 births.2,7
HOM pregnancies are associated with myriads of complications, such as miscarriage, preterm birth, low-birth-weight infants, increase in cesarean delivery and neonatal deaths, hyperemesis gravidarum, gestational diabetes mellitus, hypertension, anemia, and psychological disorders in pregnancy.8,9 The occurrence of hypertensive complications is proportional to the total fetal number of fetuses thus: singletons (6.5%), twins (12.7%), and triplets (20.0%). 8 Women with HOM gestations are more likely to develop preeclampsia with atypical features 8 with increased risk of pulmonary edema. 4 In the United States, preeclampsia was reported as a common complication of HOM. 9
In HOM gestation, there is an approximate fivefold increased risk of stillbirth and a sevenfold increased risk of neonatal death, which primarily is due to complications of prematurity. 8 The combination of preterm delivery, low birth weight, and very low birth weight has been reported as the major perinatal complication of a triplet pregnancy. 4 In Lagos Nigeria, all the deliveries of HOM were preterm and perinatal mortality rate was high (243/1000). 3 Esike et al. 6 in Abakaliki, Nigeria, reported a perinatal mortality rate of 91 babies per 1000 in triplets. Wadhawan et al. also observed that triplet or HOM neonates were more likely to have 1 min and 5 min Apgar scores 10 of less than 3 and receive at least one dose of surfactant; the incidence of necrotizing enterocolitis was higher in HOM. 11 Increased perinatal mortality occurs more often in dichorionic triplets than in trichorionic triplets. 12 HOM is also associated with increased risk of maternal death compared to twin or singleton gestation. It (maternal mortality) was reported to be 1% for singleton pregnancies, 2% for twin pregnancies, and 6.3% for triplet pregnancies. 4 Good feto-maternal outcomes can be achieved with adequate feto-maternal monitoring following early diagnosis of HOM and astute antepartum, intrapartum, and postpartum care.
With the above background, this study aims to determine the pattern and outcomes of HOM pregnancies in Alex Ekwueme Federal University Teaching Hospital Abakaliki (AEFUTHA), Ebonyi State. Our study is the first in the center and the findings will assist in the counseling of client with HOM pregnancy in the center and in auditing of care in the hospital. It will also help to stimulate the health care managers in the states and Nigeria in general on the need to provide the requisite infrastructure needed for optimal care of women with HOM pregnancy.
Methods
Study design
This is a retrospective cross-sectional study of HOM pregnancies managed in the Obstetrics and Gynaecology Department of AEFUTHA between 2012 and 2016.
Study setting and background
This retrospective cross-sectional study was carried out in the Department of Obstetrics and Gynaecology of AEFUTHA Ebonyi state. Ebonyi state is one of the states in southeast Nigeria and is populated mainly by Igbos’. It is estimated that the population of Abakaliki as of 2021 is about 1,179,280. Ebonyi is primarily an agricultural region and about 75% of the population dwell in rural areas with farming as their major occupation. AEFUTHA is the only teaching hospital in the state, receiving a referral from primary, secondary, private, and mission hospitals in the state and neighboring states. The Department of Obstetrics and Gynaecology is one of the departments in the hospital. It is managed by consultant obstetricians and resident doctors with the help of trained midwives and nurses.
Antenatal and labor care
Both antenatal and booking clinics hold daily from Mondays through Fridays which are run by consultant obstetricians with their team of resident doctors. The average antenatal attendee in AEFUTHA is 100 women per week and the delivery rate is 155 deliveries per month, with a C/S rate of 34.3%. A woman is said to have booked in the center if she has attended two or more antenatal visits and has done the baseline investigations which must have been reviewed by an obstetrician. Unbooked women are those who have no prenatal care in our facility or those who registered at our hospital but has less than two antenatal visits. During antenatal class, interactive health talk is provided to the women by the midwives before the women are allowed to see their obstetrician. It lasts for about 60 min. The topic discussed includes nutrition, diet, personal hygiene and danger signs in pregnancy, the labor experience, care of the newborn, exclusive breastfeeding, and immunization. Other health issues, such as hypertension, diabetes mellitus, malaria, anemia, HIV/AIDS, and family planning, are also discussed. Routine services following the health talk include weight and height measurement, blood pressure estimation, urinalysis, and hemoglobin estimation. Following this, the women are called in by their doctors. History taking, examination, and appropriate investigations are requested. Some of the investigations requested include blood group, genotype, pack cell volume, fasting blood sugar, HIV screening—after due counseling and offered routinely with an option to opt-out, hepatitis B virus screening, venereal disease research laboratory test, and urinalysis. Ultrasound examination is not done routinely but on an indication. However, it is expected that a third-trimester ultrasound should be carried out to access the fetal well-being, fetal weight, placental localization, and biophysical profile before delivery. For HIV-positive women, other investigations requested include viral load, CD4 count, hepatitis C virus screening, liver function test, kidney function test, full blood count, and platelet. The women are counseled on birth preparedness and complication readiness. Drugs given at routine visits include folic acid, ferrous sulfate, and multivitamins. Other drugs are also prescribed depending on clinical findings. HIV-positive pregnant women are given highly active anti-retroviral therapy and Septrin as a routine in addition to other drugs; at delivery, anti-retroviral prophylaxis is commenced for the neonates using nevirapine or nevirapine and zidovudine depending on the risk of vertical transmission.
The labor ward is managed by a team of resident doctors led by a senior registrar under the supervision of a labor ward consultant. They are assisted by trained midwives. Parturients in labor are admitted in the labor ward when the cervical dilatation is 4 cm and above, while those for induction of labor are admitted when the Bishop score 13 is 6 and above. They were managed with individualized partograph according to the departmental protocol. However, pregnant women who were booked for C/S are admitted into the antenatal ward 24 h before the day of surgery. Blood and urine samples were collected for pack cell volume, grouping and typing of blood, and urinalysis as a routine. Other investigations would be requested based on the clinical finding from the patient. The anesthetist and neonatologist were informed to review her and to be present during the delivery process.
Study population
The case files of all women who had HOM pregnancies at the hospital (AEFUTHA, Ebonyi State, Nigeria) from 1 January 2012 to 31 December 2016 were retrieved and reviewed. HOM pregnancies occur when more than two fetuses are present in the uterus at the same time. The diagnosis was made through an ultrasound investigation.
Inclusion and exclusion criteria
Women included in the study were all parturient who was delivered of three or more neonates in the facility during the study period irrespective of the outcome. Those excluded were parturients who were delivered of singleton or twin fetuses.
Data collection
The emergency room, postnatal, theater, and labor ward records were used to identify the cases of HOM pregnancies and deliveries in the facility over the study period. The hospital numbers were compiled making sure that double-entry was avoided. It was used to retrieve the case notes from the record department. Using a data collection form, the following information was obtained from each case note: sociodemographic parameters (maternal age, parity, occupation, level of education, marital status, and religion), gestational age, booking status, mode of delivery (Figure 1), antepartum complication—anemia, hypertension, preterm labor, premature rupture of membrane, neonatal sex, Apgar score, 10 neonatal weight, and postpartum complication (Table 1).

Mode of delivery of women.
Sociodemographic characteristics of the women.
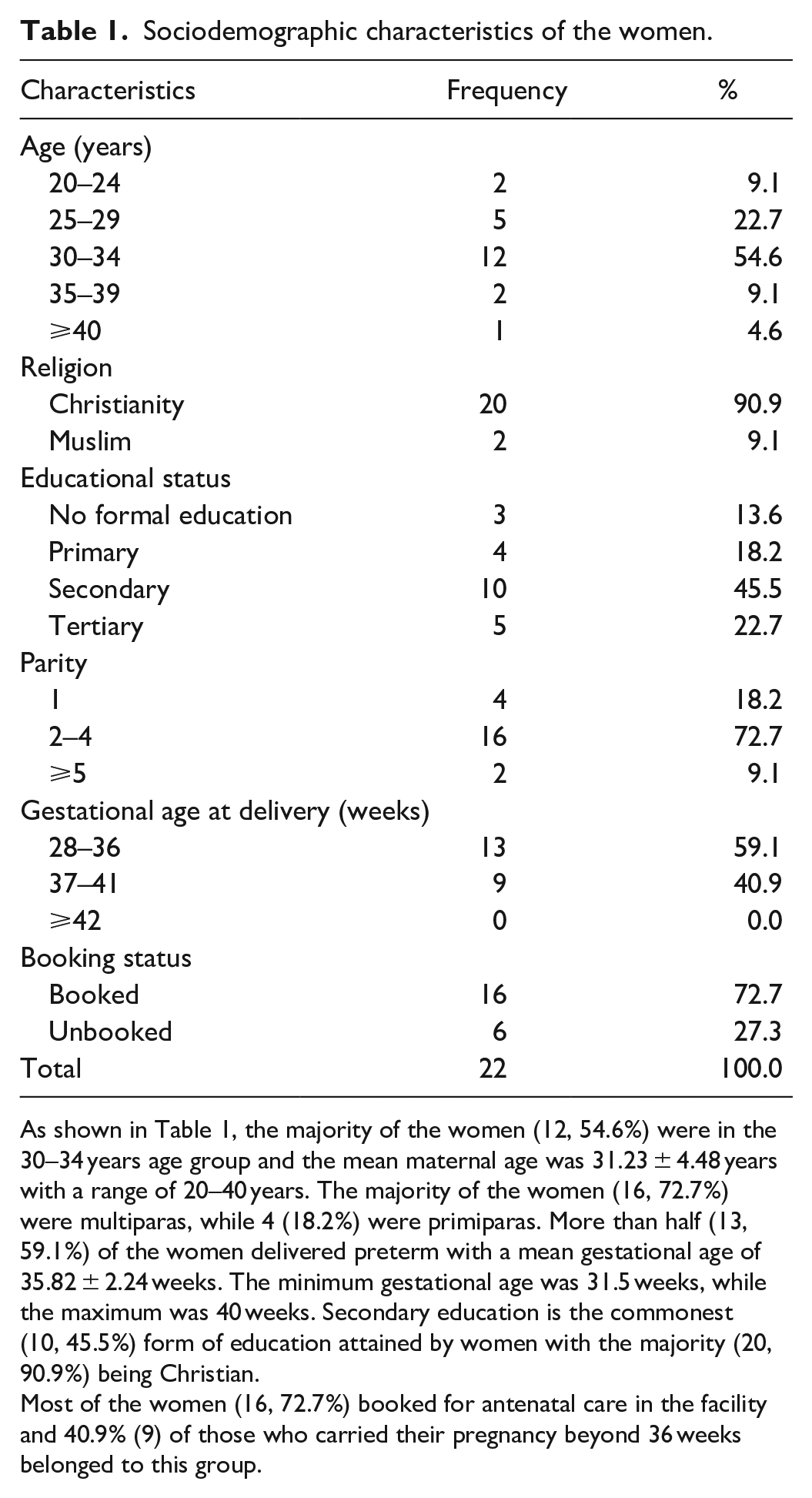
As shown in Table 1, the majority of the women (12, 54.6%) were in the 30–34 years age group and the mean maternal age was 31.23 ± 4.48 years with a range of 20–40 years. The majority of the women (16, 72.7%) were multiparas, while 4 (18.2%) were primiparas. More than half (13, 59.1%) of the women delivered preterm with a mean gestational age of 35.82 ± 2.24 weeks. The minimum gestational age was 31.5 weeks, while the maximum was 40 weeks. Secondary education is the commonest (10, 45.5%) form of education attained by women with the majority (20, 90.9%) being Christian.
Most of the women (16, 72.7%) booked for antenatal care in the facility and 40.9% (9) of those who carried their pregnancy beyond 36 weeks belonged to this group.
Statistical analysis
The data obtained were analyzed using IBM SPSS Statistics version 20 (IBM Corp., Armonk, NY, USA). The results were expressed using odds ratio (OR), bar charts, frequency tables, percentages, mean, and standard deviation. The OR was classified into OR <1 and OR >1. OR <1 represents decreased chances of bad neonatal outcomes occurring, while OR >1 represents increased chances of the neonates having bad outcomes.
Ethical consideration
Ethical approval was obtained from the Health Research and Ethics Committee of AEFUTHA, Ebonyi state. The ethical approval number is FETHA/REC/VOL1/2017/539. Informed consent was waived by the Institutional Review Board due to the retrospective nature of the study.
Results
There were 22 (21 sets of triplets, 1 set of quadruplet) HOM pregnancies of the total of 12,002 pregnancies delivered during the 5 years of the study. This gave HOM pregnancy prevalence rate of 0.18% or one HOM pregnancy per 545.5 deliveries. Seventeen of the triplets were trizygotic and triamniotic, a triplet was monozygotic and diamniotic, while the remaining triplets (3) were monochorionic and monoamniotic. The quadruplet was diamniotic and dichorionic. The prevalence for triplets and quadruplet was 0.17% (1 in 571.5 deliveries) and 0.008% (1 in 12,002 deliveries), respectively. No HOM births beyond quadruplet were recorded.
Five of the cases (four triplets and one quadruplet) had an earlier treatment for primary infertility and eventually had an in vitro fertilization (IVF) (0.4 per 1000 deliveries); all the other mothers with HOM births in this study conceived naturally. IVF procedures were not done in AEFUTHA as there are no facilities for ART in the hospital. Women who had IVF procedures were only managed and delivered in our facility; hence, information on the number of embryos transferred could not be assessed.
Discussion
The overall prevalence of HOM pregnancy in this study was 0.2% or one in 545.5 of all deliveries. This is higher than the prevalence of 0.01%–0.07% reported by other studies,1,2,7 but lower than 1.48% earlier reported in the United States. 3 The lower prevalence may be because all the HOM pregnancies in the earlier studies by Nnadi et al., 1 Rathod et al., 2 and Shrestha et al. 7 were conceived naturally. The higher prevalence reported in the United States was due to the increased use of ART for conception, compared to Abakaliki (Nigeria), where the ART procedure is still in its rudimentary stage due to the problems of affordability and acceptance among the majority of women who need it. The prevalence of 0.2% for HOM pregnancies in this study is relatively higher than the 0.13% and 0.1% reported by Umeora et al. 5 and Esike et al., 6 respectively, in Abakaliki, Southeast Nigeria. It is, however, lower than the 0.32% reported by Fajolu et al. 3 in Lagos, Southwest Nigeria. Besides, all the HOM pregnancies in the earlier studies in Abakaliki 6 were conceived naturally without the use of ART.
The higher prevalence of HOM pregnancies reported by Fajolu et al. 3 in Lagos, Southwest Nigeria may be due to a higher number of women who used ART procedures for conception in Lagos compared to Abakaliki, owing to a higher public awareness, acceptance, and affordability of this procedure in Lagos. The prevalence of triplets and quadruplets in this study was 0.17% and 0.01%, respectively. These explained triplet and quadruplet pregnancies to be a rare type of pregnancy in this part of the world. This degree of rarity may be due to the slow acceptance and utilization of ART for conception.
Total deliveries and incidence of HOM pregnancies during the period of review.

HOM: higher-order multiple.
As seen in Table 2, the year 2012 had the lowest point prevalence of HOM pregnancies, while the years 2014 and 2016 recorded the highest incidence number of HOM pregnancy deliveries.
Booking status and perinatal outcome.

HOM: higher-order multiple; OR: odds ratio; CI: confidence interval.
As shown in Table 3, the total number of live births was 67 with a perinatal survival rate of 85.1%. Being booked is associated with better neonatal outcomes although not significant (OR = 3.06, 95% CI: 0.55–16.83, p = 0.197). The perinatal mortality rate was 89.6 per 1000 total births with an equal frequency of neonatal death on both booked and unbooked women. Table 3 also shows the number of fetuses among the HOM pregnant women, and 63 (94.0%) were triplets from 21 women (95.5%), while 4 (6.0%) quadruplet fetuses were from one woman representing 4.6%.
The mean gestational age of triplets in this study was 35.56 ± 2.11. The mean gestational age at delivery observed in our review is higher than the 32.35 weeks reported in Sokoto 12 and 32.6 weeks reported in Abakaliki, Nigeria. 5 This marked improvement in gestational age at delivery in our review could be attributed to increased antenatal booking among women with HOM pregnancies and prompt treatment of antenatal complications which resulted in reduced preterm births. The majority of the mothers (72.7%) in this study booked for antenatal care and this was lower than the 78.5% reported in Sokoto, 12 and 100% and 85.7% reported by Umeora et al. 5 and Esike et al., 6 respectively, both in Abakaliki Southeast Nigeria. The lower number of booked women compared to that in the previous study by Esike et al. 6 may be influenced by the difference in the study population. In our review, equal frequency of neonatal death was seen on both booked and unbooked women, which is in contrast with the findings from other studies done in Sokoto 12 and Lagos, 3 where the overall perinatal mortality was more in the unbooked women. This may be attributed to the attendant challenges of vaginal delivery in HOM pregnancies. Most of the women booked early had regular antenatal care, and complications that developed in the course of pregnancy were promptly managed which probably contributed to the good maternal and neonatal outcome in the group.1,2
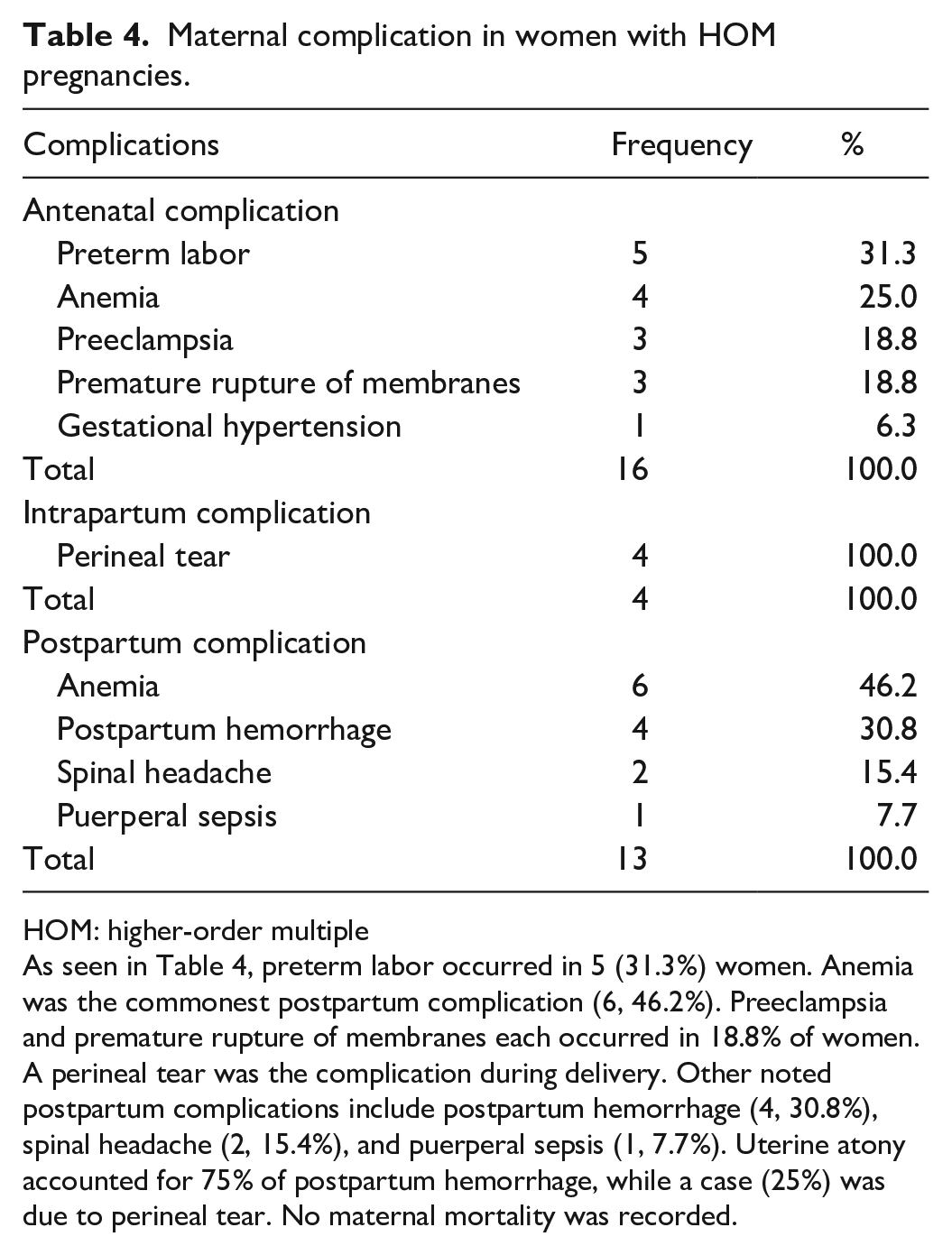
Maternal complication in women with HOM pregnancies.
HOM: higher-order multiple
As seen in Table 4, preterm labor occurred in 5 (31.3%) women. Anemia was the commonest postpartum complication (6, 46.2%). Preeclampsia and premature rupture of membranes each occurred in 18.8% of women. A perineal tear was the complication during delivery. Other noted postpartum complications include postpartum hemorrhage (4, 30.8%), spinal headache (2, 15.4%), and puerperal sepsis (1, 7.7%). Uterine atony accounted for 75% of postpartum hemorrhage, while a case (25%) was due to perineal tear. No maternal mortality was recorded.
In this study, the predominant antenatal complication (5, 31.3%) was preterm labor/delivery. This was similar to the reports from other studies.1,4–6,9,14 Other antenatal complications include anemia in 4 (25.0%), while 3 (18.8%) each for preeclampsia and premature rupture of membranes, and 1 (6.3%) had gestational hypertension. This is similar to the findings from a study done in Abakaliki, 6 and by other studies.4,9 This is in contrast to the findings by Wadhawan et al. 11 who noted that mothers of HOMs were less likely to have preeclampsia or hypertension compared with singleton mothers. A study from the United States reported that women with HOM fetal gestations are more likely to develop preeclampsia but also to present in an atypical manner, 8 but this was not in keeping with the findings from this study. Prompt diagnosis and treatment of these complications contributed significantly to the overall improved perinatal outcome recorded in this study.
Neonatal outcome.

As shown in Table 5, the total number of neonates delivered was 67; 94% (63) of these were from triplet gestation, while 6% (4) were from quadruplet conception. Most of the fetuses (35, 52.2%) delivered weighed between 2.0 and 2.49 kg. The mean birth weight of the babies was 2.14 ± 0.35 kg with a minimum weight of 1.3 kg and a maximum weight of 3.0 kg. In total, 48 babies (71.6%) had an Apgar score of ⩾7 in 1 min, with only 9 (13.4%) having an Apgar score of ⩽ 3 in 1 min. The Apgar score of the fetuses at 5 min showed that the majority of the fetuses (55, 82.1%) had an Apgar score of ⩾7. Only 6 (9.0%) had Apgar scores of ⩽3 at 5 min. Out of the 67 births recorded, 61 (91.0%) were live births, while 6 (9.0%) were perinatal deaths. The perinatal mortality of HOM pregnancies was 89.8 per 1000 live births (not in table). Three (50%) of the perinatal mortality in this study occurred in triplets weighing between 1.3 and1.5 kg who suffered early neonatal death. The remaining three perinatal deaths resulted from stillbirths recorded in unbooked patients who presented in advanced labor who had a spontaneous vaginal delivery.
The most common mode of delivery in our study is C/S (15, 68.2%). This is similar to the finding in Lagos 3 and similar reports by Nnadi et al. 1 and Shrestha et al. 7 Our results fail to agree with earlier studies in Abakaliki where the commonest mode of delivery was vaginal route.5,6 The reason for this difference may be due to the current hospital protocol that allows HOM pregnancies as an indication for C/S, while vaginal delivery is allowed if a patient presents in advanced labor or does not give consent for C/S. The majority were booked which is a favorable factor for counseling on the mode of delivery. The majority of the neonates in our study (35, 52.24%) were male, with 32 (47.76%) being female, which is in tandem with previous studies.6,14
The perinatal mortality of 89.8/1000 births in this study is lower than earlier reports in Abakaliki and Lagos,3,5 but similar to the finding of Esike et al. 6 in the study area. Three (50%) of the perinatal mortality in this study are from premature triplets weighing between 1.3 and 1.5 kg who suffered early neonatal death. This finding is similar to what was reported in other works.1,2,5,6,8 The other cases of perinatal deaths resulted from stillbirths recorded in unbooked patients who presented in advanced labor and had spontaneous vaginal delivery; two of the pregnancies were complicated in the antenatal period by preeclampsia and maternal anemia, respectively. Most of the fetuses (35, 52.24%) in our review weighed between 2.0 and 2.49 kg. This is similar to the findings in studies done in Abakaliki,5,6 but in contrast to the study done in Sokoto where 74% of babies weighed less than 2.5 kg. 14 The increased rate of low-birth-weight babies recorded in this study is due to prematurity. However, this can be improved through early booking in the antenatal clinic and prompt diagnosis and treatment of pregnancy-related complications in women with HOM pregnancies. In this study, the majority of babies had a reassuring Apgar score. 10 This is similar to the finding of Esike et al. 6 in Abakaliki. The significant number of birth asphyxia following vaginal delivery of triplets supports the prevailing view that elective C/S should be the ideal mode of delivery in centers where resources for safe C/S are available. In quadruplet pregnancies, C/S is the preferred route of delivery because of the increased risk of fetal malpresentation and difficult intrapartum fetal monitoring.1,7
HOM pregnancies are associated with high rates of intrapartum and postpartum complications. The commonest postpartum complication in this study is anemia, but this is in contrast to the findings from other studies.4,5,9 The low socio-economic status among most of the unbooked patients in this study would have also contributed immensely to the anemia. Most of the cases of postpartum hemorrhage recorded in our study are due to uterine atony and this is similar to the finding from a study done in Abakaliki. 5 Puerperal sepsis occurred in the unbooked patient who had a vaginal delivery. No maternal mortality was recorded in this study in contrast to previous Nigerian studies that reported a high risk of maternal mortality associated with HOM pregnancies. 4 The pattern of intrapartum and postpartum complications observed in this study underscores the importance of early booking and antenatal care, and elective C/S in the management of women with HOM pregnancies.
Limitation of the study
The study is limited by its small sample size which might be a confounding factor to the power of the maternal and neonatal outcomes observed in our review. However, because of the rarity of HOM pregnancy, our findings help to reflect the challenges inherent in the management of HOM pregnancy in a low-income setting such as Abakaliki. This, we hope, will help to prime the maternal and child health care delivery system in Nigeria and other sub-Saharan African countries to proactively prepare for the best care for women with HOM pregnancy. The findings from our study might not be generalized for the body of obstetrics population in the state although it is likely to be a representative since our facility is the only tertiary center in the state. No other center in the state has the Special Care Baby Unit (SCBU) needed for the management of the neonate. Even though the facility has a SCBU, the neonatal outcome might be influenced by the quality of care, thereby making it difficult to juxtapose our outcomes with what is obtainable in the advanced world. The unbooked status of some of the women and allowing a woman with HOM pregnancy to undergo vaginal delivery is likely to negate the outcome because of inherent difficulties in maternal/fetal monitoring. The latter becomes more difficult in a low economic setting like us. The data collection form was not validated and could add to the limitation of the study.
Conclusion
The prevalence of HOM pregnancies in Abakaliki is gradually increasing. Perinatal mortality is also quite high. Reduction of early preterm births by proper antenatal care with close feto-maternal monitoring and planned elective cesarean deliveries will significantly reduce the resultant immediate poor outcomes for these pregnancies and also reduce the risk of long-term disabilities.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221127160 – Supplemental material for Fetal and maternal outcome of higher-order multiple pregnancies in a tertiary hospital: A 5-year single-center observational study from Nigeria
Supplemental material, sj-docx-1-smo-10.1177_20503121221127160 for Fetal and maternal outcome of higher-order multiple pregnancies in a tertiary hospital: A 5-year single-center observational study from Nigeria by Emmanuel I Ogumu, Chidebe Christian Anikwe, Bartholomew C Okorochukwu, Osita S Umeononihu, Basil I Nwokoye, Okoroafor F Chigozie, Chukwuemeka J Ofojebe and Lucky O Lawani in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank all the medical students who participated in this study; without them, this study would not have been possible, and they are also grateful to the staff of the records department who assisted in the retrieval of case notes.
Author contributions
E.I.O., C.C.A., and L.O.L contributed to study design, data collection/analysis, and interpretation of finding and drafting of the article O.S.U., B.I.N., B.C.O., and O.F.C. participated in the interpretation of findings and drafting of the article. All participated in the review of the final article. All the authors approved the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Health Research and Ethics Committee of Alex Ekwueme Federal University Teaching Hospital Abakaliki (AEFUTHA), Ebonyi state (FETHA/REC/VOL1/2017/539).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was not sought for this study because of its retrospective nature. It was waived by the Institutional Review Board.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.