
Abstract
Background:
This research aims to explore and compare the signals of rhabdomyolysis from the use of Proton pump inhibitors (PPIs) using the United States Food and Drug Administration Adverse Event Reporting System (FAERS) database.
Methods:
Rhabdomyolysis and related terms submitted between 2013 and 2021 were retrieved from the FAERS database. The data were analyzed using the reporting odds ratio (ROR), proportional reporting ratio (PRR), Empirical Bayes Geometric Mean (EBGM) and the information component (IC). The signals of rhabdomyolysis associated with PPIs use were detected in both 3-Hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitors (statins) utilizers and non-utilizers.
Results:
A total of 7,963,090 reports were retrieved and analyzed. Fifty-seven reports linked PPIs to rhabdomyolysis out of 3670 reports from other drugs (non-statin included). The association of rhabdomyolysis and PPIs was significant in both statins included, and non-statin-included reports, although with varying degrees of association. The ROR was 2.5 (95% confidence interval [CI] 1.9–3.2) for PPIs in non-statin-included reports and 2 (95% CI: 1.5–2.6) for PPIs in statin-included reports.
Conclusion:
Significant signals of rhabdomyolysis were associated with PPIs. However, its signals were higher in non-statin-included reports compared to statin-included reports.
Plain Language Summary
Keywords
Introduction
Proton pump inhibitors (PPIs) are regarded as the first line therapy for the management of acid-related illnesses for the last three decades. PPIs are known as a class of pharmacological agents that irreversibly block the H+/K+ ATPase located in the gastric parietal cells. The current approved PPIs available in the United State (U.S) include omeprazole, esomeprazole, lansoprazole, pantoprazole, rabeprazole, and dexlansoprazole.1,2 Moreover, PPIs are widely indicated for the treatment of peptic ulcer disease, functional dyspepsia, Zollinger-Ellison syndrome, gastroesophageal reflux disease, prophylaxis against non-steroidal anti-inflammatory drugs induced ulcers, and erosive esophagitis3–5 PPIs are co-prescribed with antibiotics or dual antiplatelet therapy for the eradication therapy for Helicobacter pylori and management of ischemic heart diseases, respectively.6,7
Due to the surge of long-term use of PPIs in numerous clinical scenarios, there is considerable interest in continuous safety surveillance. Chronic use of PPIs can lead to potential adverse events (AEs) that include bone demineralization and fractures, dementia, interstitial nephritis, hypomagnesemia, and anemia.8–17
Rhabdomyolysis has also been reported with PPI use. 18 This is a serious syndrome causing leakage of muscle contents into the systemic circulation following breakdown of skeletal muscles. As a result, myoglobin, creatinine kinase, and electrolytes are released into the systemic circulation.19,20 The causes of rhabdomyolysis include a variety of diseases, injuries, drugs, and toxins. 21
However, there are no randomized controlled trials showing a relationship between PPIs utilization and rhabdomyolysis risks. Although, a retrospective study conducted in 2011 using the Food and Drug Administration Adverse Event Reporting System (FAERS) database points to potential medications potentially associated with rhabdomyolysis. 22 In the study, Oshima, 22 has reported an estimated 8610 cases of drug induced rhabdomyolysis. In extension, the study further shows that a total of 4325 cases were reported for statins as the first suspect, whereas 100 and 99 cases were, respectively, reported for diclofenac and omeprazole. 22 Moreover, a review of case reports conducted by Duncan and Howden 23 has linked seven cases of rhabdomyolysis to PPIs. Of the seven case reports, two were concurrently on PPIs and HMG-Co-A reductase inhibitors (statins) which have been earlier linked to myopathy. 23 Similarly, Clark and Strandell 24 have reported 35 cases of rhabdomyolysis associated with PPIs use of which 12 cases entailed simultaneous HMG-CoA reductase inhibitors utilization. Also, one Korean study found a case of rhabdomyolysis associated with intravenous (IV) bolus of esomeprazole. 25 In addition, Bebarta et al. 26 reported one case of omeprazole-induced hyponatremic delirium and rhabdomyolysis in emergency department. However, after the discontinuation of omeprazole and initiation of IV saline hydration, the patient recovered completely. In a German study involving a patient with cardiac failure, rhabdomyolysis secondary to esomeprazole administration has been reported. 27 Moreover, Nozaki et al. 28 found one case of rhabdomyolysis following twice daily dosing of 20 mg IV omeprazole. After withdrawal of omeprazole, the laboratory data improved within 5 days. 28 Another case report published in 2014 found one patient who developed rhabdomyolysis after 14 days of twice daily dosing of 20 mg IV omeprazole. 29 The patient recovered completely after deprescribing the PPI and initiation of aggressive fluid repletion and urine alkalization. 29
Given the voluminous nature of spontaneous case reports of drug AEs received from different parts of the globe, the FAERS database serves as a directory for post-marketing surveillance. The purpose of this study was, therefore, to explore the potential link between PPIs utilization and the manifestation of the rhabdomyolysis AEs, using the FAERS database offered by the US Food and Drug Administration (FDA).
Material and methods
Data source
FAERS database was exclusively accessed to establish the potential link between PPIs utilization and rhabdomyolysis AE manifestation. Spontaneous AE reports received from 2013 to 2021 were retrieved from the FDA website using the free access link https://open.fda.gov/data/faers/. 30 FAERS database is a useful post-marketing safety surveillance tool for all U.S approved therapeutic biologics and pharmaceuticals. AEs can be reported by physicians, pharmacists, other healthcare provider (HCP), and patients, but it is completely voluntary. Only the manufacturer is legally obligated to send the report to the FDA. 30
Despite the fact that FAERS is a U.S. database, it receives many reports from foreign countries. The large size and global coverage of this database are deemed meritorious for performing robust spontaneous AEs reporting data mining for post-marketing surveillance. A valid FAERS reporting system captures verifiable patient information, the implicated medication, and the associated AEs.
Data collection
The FDA releases FAERS files quarterly. Each quarterly file consists of seven data tables, which include patient demographic and administrative information, origin of information, drug indication, previous and concurrent medications, dates of commencement and discontinuation of therapy, AEs, and drug use outcome. The FAERS reporting system transforms the AEs terms submitted by the reporter into standard AEs terms called Preferred Terms (PTs) via the Medical Dictionary for Regulatory Activities (MedDRA) coding system.
In this study, the main pharmacologic class of the target drugs was PPIs. All reports that included both generic and trade PPIs names were extracted. The desired outcome, “rhabdomyolysis”, was searched in the PTs field of the FAERS database. Also, we have included only the first suspected drug that causes rhabdomyolysis. To exclude duplicate and conflicting data, the assigned identification codes (unique ID or case number) were reviewed on case-by-case basis.
Statistical analysis
In the context of this research “case” was defined as reports of rhabdomyolysis sequel to PPIs, whereas “no-case” was regarded as all other AEs reports linked to PPIs other than rhabdomyolysis. Accordingly, the case/non-case method was adopted to measure the association between PPI utilization and manifestation of rhabdomyolysis.
In this study, the reporting odds ratio (ROR) means the odds of a certain event occurring with medicinal product, compared to the odds of the same event occurring with all other medicinal products in the database; proportional reporting ratio (PRR), which measure of how common an AE for a particular drug is compared to how common the event is in the overall database; information component (IC) which means a measure of the strength of the quantitative dependency between specific drug and specific adverse drug reaction (ADR); and Empirical Bayes Geometric Mean (EBGM), which provide a more stable estimate of the relative reporting rate of an event for a particular product relative to all other events and products in the database, were calculated as measures of pharmacovigilance signal to estimate the association between PPIs and rhabdomyolysis. These indices were calculated using a 2×2 contingency table (Table 1). 31 In this study, a drug–AE combination that met the criteria of all the four indices was defined as a signal (Table 2).32–35
A 2×2 contingency table for disproportionality analysis.

Disproportionality indices calculations and signal detection criteria.

CI, confidence interval; EBGM, Empirical Bayes Geometric Mean; IC, information component; PRR, proportional reporting ratio; ROR, reporting odds ratio.
N*expected = (Ndrug × Nreaction)/Ntotal.
All statistical analyses were conducted using Statistical Analysis Software (SAS 9.4; SAS Institute Inc., Cary, NC, USA).
Confidentiality
There was no trackable personal patient or reporter information from the FAERS database. The ethics approval for the conduct of this study was granted by the chair of medication safety research domiciled at King Saud University.
Results
A total of 7,963,090 reports were retrieved and analyzed between 2013 and 2021. Most of the PPI reports were from Japan (56.6%) followed by France (13.2%), USA (11.3%), South Korea (94%), and Australia (9%). Moreover, Luxembourg and Germany occurred at similar rates (1.8%). In addition, those reports involved more male patients (80.95%). Also, the highest population was elderly ⩾ 65 years old (42.86%) (Table 3). Esomeprazole 28 and omeprazole 17 were the most implicated PPIs, while dexlansoprazole 1 appeared the least (Figure 1). Physicians and pharmacists appeared to be the most frequent spontaneous reporters compared to other HCPs (Figure 2).
Demographic distribution of reports.

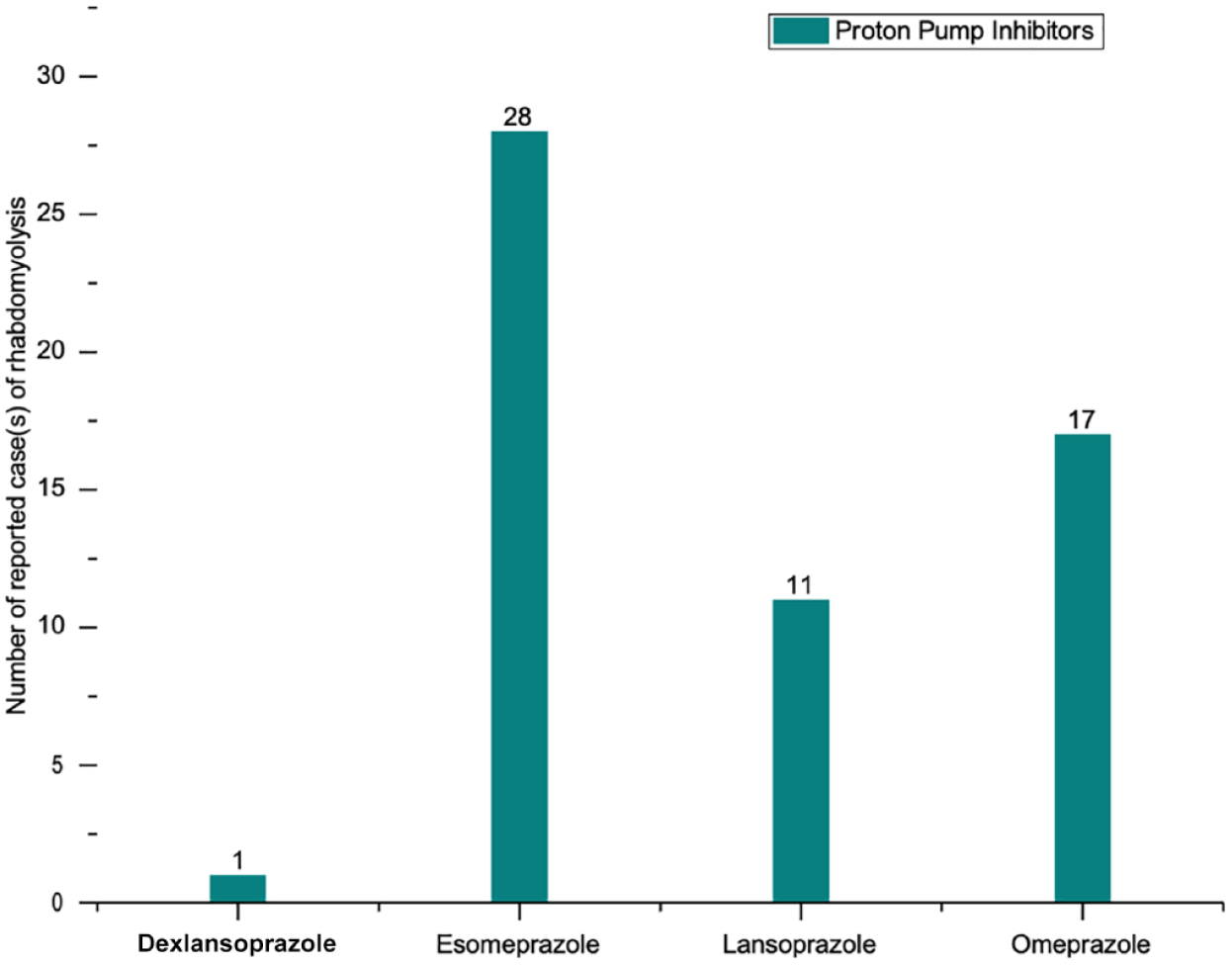
Distribution of cases of rhabdomyolysis induced by proton pump inhibitors as reported in the FDA adverse event reporting system database from 2013 to 2021.

Distribution of reported cases of rhabdomyolysis by reporter designation from the FDA FAERS database from 2013 to 2021.
A total of 4471 reports were associated with rhabdomyolysis. Of these reports, there were 57 (1.27%) cases in which the PPIs were considered as the implicated drugs leading to rhabdomyolysis. On the contrary, 4414 reports were linked to rhabdomyolysis associated with drugs other than PPIs (Table 4).
Pharmacovigilance metrics for reported cases of rhabdomyolysis in PPIs and statin reports.
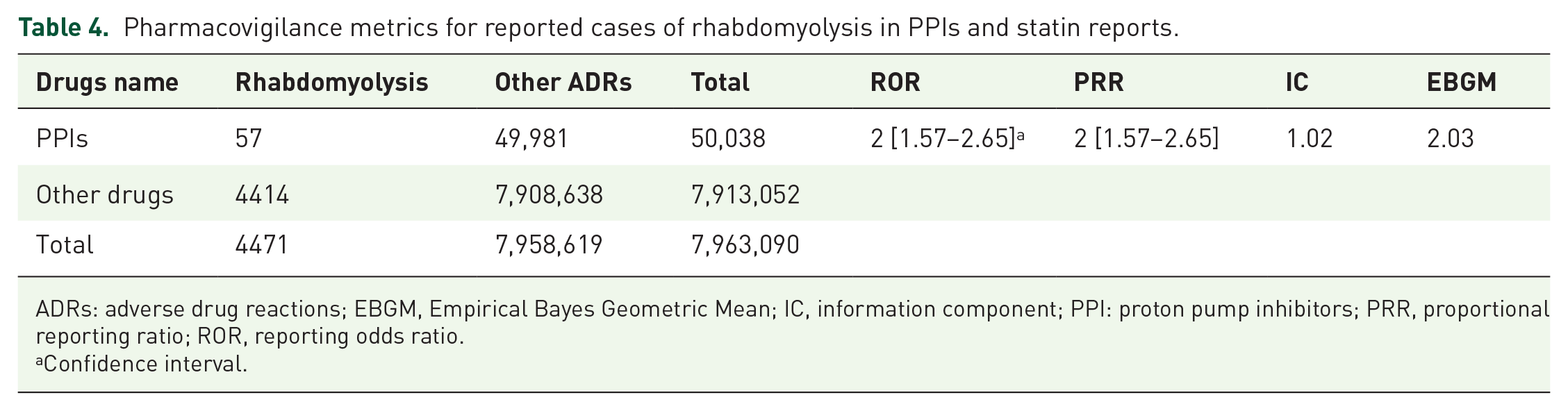
ADRs: adverse drug reactions; EBGM, Empirical Bayes Geometric Mean; IC, information component; PPI: proton pump inhibitors; PRR, proportional reporting ratio; ROR, reporting odds ratio.
Confidence interval.
The ROR significance points to the high risk of rhabdomyolysis with PPIs utilization in both statins and non-statin-included reports, although with different degrees. The ROR index was lowest for statin-included reports (2 [95% CI: 1.5–2.6]; Table 4), but highest for non-statin reports (2.5 [95% CI: 1.9–3.2]; Table 5).
Pharmacovigilance metrics for reported cases of rhabdomyolysis following PPIs use only (non-statin-included group).

ADRs: adverse drug reactions; EBGM, Empirical Bayes Geometric Mean; IC, information component; PPI: proton pump inhibitors; PRR, proportional reporting ratio; ROR, reporting odds ratio.
Confidence interval.
The PRR was significant for the risk of rhabdomyolysis in similar trend to ROR. The PRR index was lowest for statin-included reports (2 [95% CI: 1.5–2.6]; Table 4), but highest for non-statin reports (2.5 [95% CI: 1.9– 3.2]; Table 5).
In addition to ROR and PRR, which are based on statistical shrinkage transformation, IC and EBGM were utilized to perform disproportionality analysis. It was found that both IC and EBGM algorithms exceeded specified threshold value (0 and 2, respectively at 95% CI) and were regarded as signals. IC and EBGM were low for statin-included reports (1.02, 2.03 [95% CI] respectively) (Table 4), but high for non-statin reports (1.31, 2.47 [95% CI] respectively) (Table 5).
Both IC and EBGM indices indicated that there were unprecedented reports of rhabdomyolysis and a significant statistical association between the AEs and PPIs in both statin and non-statin-included reports.
Discussion
Upon approval of a new biologic or pharmaceutical product by the FDA, post-marketing surveillance is needed to evaluate medications safety and determine the public health risks that are associated with these drugs. The reason is that after the drug is issued to the market, the probable consumers differ from clinical trials’ sample people. Consequently, safety surveillance is mandatory throughout the product life cycle. The FAERS database is a very essential tool for post-marketing surveillance. Moreover, researchers can freely access the database for signal detection in pharmacovigilance and pharmacoepidemiologic studies. 36
In this study, we identified 57 rhabdomyolysis cases associated with PPI use in FAERS system based on spontaneous reports submitted between 2013 and 2021. We categorized these cases into two main categories: (1) rhabdomyolysis following PPIs in statin-included reports and (2) rhabdomyolysis following PPIs in non-statin-included reports.
The novelty of our findings was that we were able to show the association between rhabdomyolysis and PPIs use in reports including HMG-Co-A inhibitors (statins), with the following pharmacovigilance signal measures: (ROR and PRR (2 [95% CI: 1.5–2.6]), IC and EBGM (1.02, 2.03 [95% CI] respectively), are lower than non-statin-included reports with the following pharmacovigilance signal measures: ROR and PRR (2.5 [95% CI: 1.9– 3.2]), IC and EBGM (1.31, 2.47 [95% CI] respectively). However, one recent study found that PPI use has been associated with rhabdomyolysis in patients after total thyroidectomy with electrolytes imbalance. 37
Our findings are in concordance with numerous published reports that associate rhabdomyolysis with PPI utilization. A retrospective study conducted by Oshima et al. 22 assessed the medications that may be linked with rhabdomyolysis by using the reports that submitted to FAERS database between January 2004 and December 2009. They found that out of 8610 cases of rhabdomyolysis, 99 were related to omeprazole. Furthermore, Duncan and Howden 23 found that seven cases of rhabdomyolysis were linked to PPIs use, out of which two were statins users. Similarly, 292 cases of PPI-induced myopathies were retrieved in a data mining study involving VigiBase- a spontaneous ADRs reporting database hosted by the World Health Organization (WHO). In the report PPIs appeared as the sole implicated drug in one-third of the cases and turned out to be the only suspected medication reported by 57% in cases of PPIs concomitant pharmacotherapy. Moreover, 35 were rhabdomyolysis. In 17 of the cases, the onset of rhabdomyolysis ranged from 1 to 2 weeks and in few cases may extend up to 3 months. In addition, concurrent statin utilization was recorded in 12 cases. However, there was no clear causal link between PPIs use and exposition of rhabdomyolysis. 24
In contrast, a Korean study found a prominent causal relationship in one case report that developed rhabdomyolysis after single IV esomeprazole bolus. Although the patient was on IV insulin, it was deemed unlikely that the co-prescribed medication was the causal agent for rhabdomyolysis. 25 Moreover, one case was recorded in a patient with chronic cardiac failure having medical history of cardiac surgery and co-prescription of anesthetics, thiazide diuretics, µ-receptor agonist opioids, catecholamines, and β-lactam antibiotics. Upon administration of IV esomeprazole at 40–80 mg/day for 1 month, there was suspected incidence of rhabdomyolysis following elevated levels of serum myoglobin, although CK remained at baseline. The study did not explain the variance between creatinine kinase and myoglobin elevation. Also, Nishikawa et al. 38 reported case with reflux esophagitis who developed rhabdomyolysis occurred at 10 months after starting esomeprazole. This case improved rapidly after holding esomeprazole in term of symptoms and CK level normalization. Conclusively, there was no clear link between esomeprazole withdrawal and restoration of myoglobin levels to baseline. 27
Conversely, a case study conducted by Sipe et al. 39 has established a case of rhabdomyolysis associated with esomeprazole in patient who had a medication of statin (atorvastatin) for over 1 year and 6 weeks of esomeprazole, and few doses of clarithromycin (500 mg) just before hospitalization. Using Naranjo probability scale potential association between PPI use and rhabdomyolysis was established. This was explained by a P-glycoprotein mediated inhibition caused by esomeprazole leading to remodeling of atorvastatin biotransformation. 34
The mechanisms by which PPIs cause rhabdomyolysis are yet to be comprehensively elucidated. However, CYP2C19-mediated metabolism of PPIs and CYP3A4 inhibition is thought to cause clinically significant interactions with statins augmenting the risks of rhabdomyolysis. 40 Moreso, by virtue of their ability to specifically and irreversibly block the H+/K+-ATPase of the gastric parietal cells, PPIs are believed to inactivate the enzyme in vascular smooth muscle cells which may lead to vasoconstriction, ischemia and eventually cellular injury. 41 Similarly, aryl hydrocarbon receptor-mediated over expression of muscle protein synthesis has been proposed as a probable pathophysiological mechanism of PPI-induced rhabdomyolysis. 36
This study has various advantages, including availability of a sufficiently large data, free access AEs database with millions of spontaneous reports from diverse geographical regions of the globe. Interestingly, the accessibility of the database by non-U.S FDA researchers and its user-friendly interface dramatically simplifies the data mining process. Also, we have utilized additional AEs signal metrics (EBGM and IC) which is not common practice by other studies using FAERS.
However, like most spontaneous reporting utilizing the FAERS database, this study has some inherent limitations including (1) lack of complete information in spontaneous reports such as dose, duration, patient-specific risk factors, hepatic and renal function, (2) under-reporting, (3) over-reporting, (4) the difficulty to establish the causal link between the suspected drug and AEs, (5) risk of bias based on HCP preference of one medication over others, (6) a patient’s negative experience with some product. 42 Notwithstanding these limitations, this study further corroborates previous findings on the safety margins of PPIs.
Conclusion
Quantitative drug AE signal detection using ROR, PRR, IC, and EBGM algorithms substantiates the significant link between rhabdomyolysis and PPI utilization from spontaneous reporting data of the FAERS database. These signals were deemed higher in non-statins compared to statin-included reports. Clinicians and patients are particularly recommended to be well informed about increased risks of rhabdomyolysis sequel to PPIs prescription. The findings of this research further point to the need for comprehensive clinical studies to corroborate PPIs utilization in patients with augmented risks of rhabdomyolysis and identity specific metabolomic markers in both statins and non-statin users.