
Abstract
Introduction:
Older adults with Alzheimer’s disease and related dementias (ADRD) are at increased risk of harm due to prescribing of potentially inappropriate medications. Encouraging patients and caregivers to talk with their providers about potentially inappropriate medications could stimulate deprescribing. Our objective was to explore whether mailing educational materials to patients with ADRD might activate patients or caregivers to initiate a conversation with their provider about potentially inappropriate medications.
Methods:
We conducted semi-structured interviews with patients with ADRD, caregivers of patients with ADRD, and healthcare providers. All participants were shown educational materials referencing potentially inappropriate medications and suggestions to promote deprescribing. Interviews explored reactions to the materials, the idea of patients and caregivers initiating a conversation about deprescribing, and the deprescribing process. Interview transcripts were analyzed using inductive thematic analysis.
Results:
We conducted a total of 27 interviews: 9 with caregivers only, 2 with patients only, 3 with patient–caregiver dyads, and 13 with providers. Patients and caregivers reported that if a medication might cause harm, it would motivate them to talk to their provider about the medication. Trust in the provider could facilitate or inhibit such conversations; conversations would be more likely if there were prior positive experiences asking questions of the provider. Providers were receptive to patients and caregivers initiating conversations about their medications, as they valued deprescribing as part of their clinical practice and welcome informed patients and caregivers as participants in decision-making about medication.
Conclusion:
Mailing educational materials about potentially inappropriate medications to community-dwelling patients with ADRD may promote deprescribing conversations. Ongoing pragmatic trials will determine whether such interventions stimulate deprescribing conversations and achieve reductions in prescribing of inappropriate medications.
Plain Language Summary
Keywords
Introduction
Adverse drug events cause approximately 1.3 million emergency department visits each year. 1 Older adults are at increased risk of medication-related harm due to high rates of multiple chronic conditions and the involvement of multiple prescribers.2–7 Approximately 34.5% of US adults between 60 and 79 years of age used five or more prescription drugs (known as polypharmacy) in the last 30 days between 2015 and 2016 according to a Centers for Disease Control and Prevention (CDC) study. 8 As a result, the prevalence of adverse reaction among older adults is also high. According to a recent systematic review, the prevalence of adverse drug reactions among older adults with dementia ranged from 12.7% to 27%. 9 Polypharmacy increases the risk of prescriptions for potentially inappropriate medications (PIMs), 10 medications for which the risk of harm outweighs the potential benefit; such medications are best avoided by older adults in most circumstances. 11 Patients with Alzheimer’s disease and related dementias (ADRD) are at particular risk from PIMs, as these medications may have cognition-impairing effects, and prolonged polypharmacy may worsen dementia.
Many patients with ADRD rely on a caregiver for medication management, and decision-making around medication changes as their disease progresses and they become less able to manage their medications independently.12,13 For these patients, caregivers can play an essential role, ensuring medication safety, organizing medications, and evaluating medications’ effects.7,12 In other studies, caregivers report limited engagement in medication management decisions, inadequate information, and difficulties in ensuring a medication supply. These studies also suggested that caregivers desire to know more about the medication regimen and medications that impact cognition.12,14
Deprescribing is a planned, supervised process for reducing or stopping medications that are no longer needed, 15 thereby limiting the complexity of the medication management process for patients with ADRD and their caregiver. While recommended as an approach to reducing polypharmacy and PIMs,15–18 the actual deprescribing process is challenging 19 due to the complex prescribing environment and the values and beliefs of the patient, the family, and the provider.15,20–22 The American Geriatrics Society Beers Criteria 11 and other tools such as Screening Tool of Older Persons’ Prescriptions (STOPP) and Screening Tool to Alert to Right Treatment (START) are intended to improve medication safety and to address PIM prescribing, 23 but these tools are inconsistently implemented in practice. Recent research suggests that engaging patients, caregivers, and providers may be the most effective way to encourage deprescribing.12,24 Martin et al. 24 achieved impressive reductions in inappropriate medication prescriptions through an intervention in which pharmacists distributed educational materials on potentially inappropriate medications to patients and providers. However, this study excluded patients with dementia who are also likely to be less able to understand and act on educational materials. Approaches that engage caregivers along with patients may the key because many patients with dementia rely on family caregivers to make medication-related decisions as noted above. 25
Our objective in the present study was to explore whether mailing educational materials to patients with ADRD might stimulate patients and their caregivers to initiate a discussion with the provider about deprescribing of PIMs. We also aimed to identify the factors that might facilitate or impede deprescribing of PIMs in this population.
Methods
Study design and setting
This descriptive study involved semi-structured interviews with patients with ADRD and caregivers of patients with ADRD and their providers. Patients and caregivers were drawn from two settings: primary care practice sites of a large academic health system in the Northeastern United States and ResearchMatch, an online national registry of research volunteers (ResearchMatch.org). Participants recruited via ResearchMatch were from nine different states across the country. Providers were drawn from practices of the academic health system. A convenience sample was selected with all participants completing a single interview.
Patients were eligible if they were over the age of 50, living at home, diagnosed with Alzheimer’s disease or related dementias, and prescribed medication to treat memory loss (e.g. donepezil, rivastigmine, galantamine, and memantine). While the materials which we presented and sought feedback on referred to specific PIMs (e.g. oxybutynin), a prescription for a PIM was not part of the eligibility criteria. The study materials made clear that the purpose of the study was to obtain feedback on materials that were being developed, and that these materials were not intended for the participant. The interviewer reiterated this at the start of the interview, answering questions and clarifying as needed. For patients recruited locally, eligibility was initially determined via the healthcare record and confirmed by self-report or caregiver report; for patients recruited through ResearchMatch, eligibility was determined via self-report. Adult caregivers of patients who met eligibility criteria or with experience helping to care for a person with ADRD during the last 12 months were eligible. Invitation letters introducing the study and its purpose were sent via mail to the health center’s patients. The research assistant then followed up with a telephone call using a script to assess interest and to confirm eligibility. The same process occurred for the ResearchMatch registrants except for using email. Exclusion criteria for patients included residing in a nursing home or skilled nursing facility or receiving palliative care at the time of randomization.
Providers were recruited via email from three practices within the academic medical center: Family Practice, General Internal Medicine, and Geriatrics. Eligibility criteria included experience providing care to patients with ADRD. Invitations to participate were sent via email.
Data collection
The interviews were conducted by the research assistant (J.S.C.) who was a novice qualitative interviewer. Prior to the interviews, the research assistant underwent training with an experienced qualitative researcher (K.M.M.) and conducted practice interviews; once interviews were underway, the interviewer met with the experienced qualitative researcher for feedback.
All interviews were conducted via telephone or Zoom meeting, based on the preference of the interviewee during the Covid-19 pandemic. At the start of each interview, the interviewer introduced himself and his role in the study. Interviews were recorded and transcribed lasting 30–60 min in length. After completing each interview, the interviewer created a short summary capturing any insights or observations that might not be obvious from the transcript and noting suggestions for modifications to the interview process or materials.
Patient and caregiver interviews
Prior to the interview, we mailed a packet containing an informed consent form and the study materials (cover letter and information sheet) to allow participants to review the materials in advance. The educational materials focused on one of three potentially inappropriate prescription drug classes: sedative-hypnotics, antipsychotics, or strong anticholinergics. The selected drug classes can cause harmful side effects, particularly in older patients, 11 and were selected based on their potential to cause harm in this population as recommended by an expert panel. The cover letter referred to the specific drug [e.g. oxybutynin (Ditropan®)] and referenced associated harmful effects (e.g. hallucinations). The cover letter contained three additional key messages: (1) a request to share the materials with the person who helps the patient with their medication at home; (2) a request to bring the materials to the next appointment with their provider and to ask the provider whether the medication should be reduced or discontinued; and (3) the instruction not to change the medication without talking to the provider. The medication information sheet listed multiple medications within the target class, including the medication referenced in the cover letter, indicating these drugs were sometime used for longer than needed and could cause serious side effects, especially in older adults (see Supplemental File for sample materials for the strong anticholinergic medication class).
Interviews were conducted with the caregiver, the patient, or both, according to interviewee preference. Questions explored the interviewee’s reactions to the materials, their understanding of the information presented, the likelihood they would discuss the materials with their provider, and suggestions for improvements. The interview guide provided structure while allowing for flexibility to accommodate the course of the discussion. Patient and caregiver interviewees received a US$50.00 gift card to thank them for their participation.
Provider interviews
Interview materials were sent to providers in advance via email, including: (1) an informed consent form, (2) a copy of one of the information sheet sent to patients, (3) a sample cover letter developed for providers, (4) a sample deprescribing algorithm intended to help providers make decisions about deprescribing for the relevant drug class adapted from the Canadian Deprescribing Guidelines, 26 and (5) a sample tapering guide providers might give to patients to help track dose reductions. The cover letter presented identified a specific drug class, introduced the subject of deprescribing, and indicated drugs in this class were identified as potentially harmful and inappropriate for older patients. The cover letter included a table with (fictitious) patient names, drug names, and dates as an example. The materials used in the provider interviews were prototypes and did not refer to actual patients. Providers received a US$100.00 gift card to thank them for their participation.
Data analysis
We used inductive thematic analysis to identify interview themes.27,28 Coding and analysis occurred in three phases. In the first phase, two investigators (J.S.C. and M.T.A.) independently reviewed two transcripts from the patient–caregiver interviews and two from the health care provider interviews to create a codebook for each set of interviews. The codes and definitions were expanded and refined through iterative discussion until consensus was reached, and then applied to the full set of transcripts. Once the initial coding was completed for each set of interviews, the second phase began with further analysis and organization of the codifying the data resulting in 10 categories for the patient–caregiver interviews and 11 categories for the provider interviews. The third phase of analysis continued until major themes were identified from the categories for each set of interviews with supporting sub-themes. A third investigator (K.M.M.) reviewed the coding at each phase to ensure accuracy of interpretation and substantiation for each code/theme from the data. Any disagreements related to the coding were discussed by the three investigators involved in the qualitative analysis and resolved. Participant checking did not occur due to constraints of the study. Exemplary quotes were identified to elucidate the themes. The sample size was determined pragmatically according to the constraints of the study timeline; however, we believe saturation was achieved, as the themes identified were consistent across interview transcripts. Analysis was conducted using Microsoft Word and Excel.
Results
A total of 27 interviews were conducted, 9 interviews with caregivers only, 2 with patients who did not have caregivers, 3 with patient–caregiver dyads, and 13 with providers. Patient and caregiver characteristics are presented in Table 1; provider characteristics are presented in Table 2.
Patient–caregiver demographics.

GED, General Education Development.
Healthcare provider demographics.

Figure 1 organizes the key qualitative findings to describe how the themes emerged from the interviews could facilitate or impede a deprescribing conversation and the deprescribing process. Table 3 presents details and exemplary quotes from the patient and caregiver interviews, and Table 4 presents the same from the provider interviews. In the following sections, we summarize the main findings.

Facilitators and challenges to deprescribing conversations between patient–caregiver and provider.
Patients–caregivers’ themes and sub-themes.

Healthcare providers’ themes and sub-themes.
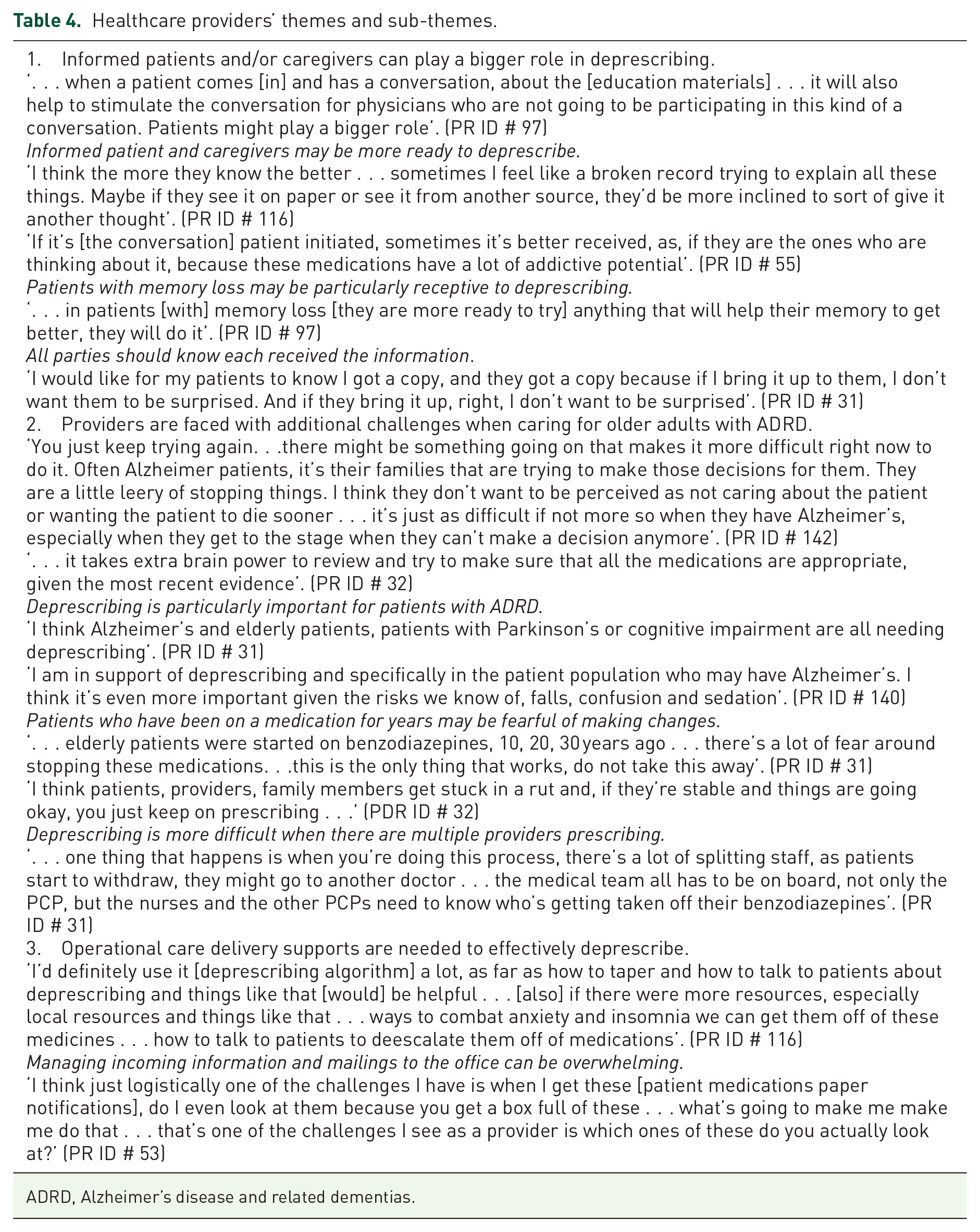
ADRD, Alzheimer’s disease and related dementias.
Patients’ and caregivers’ themes and sub-themes
Information that a medication may cause harm is important and would motivate action
Patients and caregivers consider information that a medication may cause harm to be important and would be motivated to act as a result. While some interviewees noted that learning of the potential for harm would be ‘scary’, no one preferred not to be informed if this were the case. As one patient (PT ID # 50) said, ‘the fact that it’s [informational materials] saying it may be harmful, that’s very valuable to me when I read it, and I’d call a doctor’. A caregiver (CG ID # 70) expressed, ‘. . . it’s pretty scary, that medication that you’re taking could be causing some really bad side effects and you don’t realize it. I’d want to talk to my doctor about it’. Patients and caregivers were unanimous in asserting they would not make any medication changes without first contacting the provider. The materials also generated questions about the medications and concerns regarding the potential side effects. Often caregivers and patients seek this type of information to help manage their care, understand the medications, and make decisions. One patient (PT ID #86) shared, ‘when we get these materials it tends to make us have questions . . . I show it to my wife. She will say, “yeah I will look it up.”’ The credibility of the source of the information increased the materials importance and increased the likelihood of the materials being read. ‘If it is signed by my medical officer . . . I’m going to read it and think it is valid and legitimate piece of mail’ (CG ID# 120).
Caregivers play a critical role and would initiate the conversation
Caregivers indicated they (not the patient) would be the one to act and bring questions to the provider. Caregivers viewed themselves as the organizers, coordinators, action-takers, and decision-makers with respect to their loved ones’ care, especially as the patient experienced cognitive decline. Because of this, caregivers stressed the importance of ensuring that the information was addressed to them, as well as, or instead of, the patient. It was also important for the information to be personalized to the patient and written in an empathic tone to capture the attention of the caregiver or patient for the materials to be read. One caregiver (CG ID # 126) shared that the most important role of the caregiver is ‘to give input because we are [their] security’.
Patients’ and caregivers’ trust in the provider’s judgment may facilitate or inhibit their initiating a deprescribing conversation and sharing of information
Patients and caregivers expressed trust in their provider as expert on the patient’s medications, health condition, and what is best for the patient. Comments such as ‘you trust your doctor knows everything’ and ‘I’ve never thought much about this [talking with the provider about medications] because we trust that doctor’ (CG ID # 70) exemplify patients’ and caregivers’ reliance on the provider’s judgment around medications. Some interviewees who expressed trust in their provider referenced prior positive experiences with raising questions and voiced confidence that the provider would be receptive to a conversation about the medication. Others who trusted their provider expressed reservations about raising questions about the medication, suggesting a deference to the provider that could be a barrier to their initiating a conversation. One caregiver suggested that patients and perhaps caregivers may overestimate their provider’s ability to discern what is happening with the patient, and therefore may not mention concerns or symptoms, implying that a patient’s or caregiver’s silence might not be evidence that there are no concerns.
Healthcare providers’ themes and sub-themes
All the providers interviewed endorsed deprescribing as good practice and also reported incorporating it into their own clinical practice. Some noted deprescribing is particularly important to consider in older patients with ADRD, as these patients are especially vulnerable and at risk of adverse events.
Informed patients and/or caregivers can play a bigger role in deprescribing
Providers expressed support for having patients and caregivers receive information about potentially inappropriate medications and possible side effects, believing informed patients and caregivers would be better able to participate in conversations about medications. The providers were receptive to having the patient or caregiver initiate a conversation about medications and to take an active role in decision-making. Some providers recommended that materials about potentially inappropriate medication be sent to the provider as well as the patient, and that each be informed that the other had also received materials, as this would allow the providers to be better prepared to discuss the medication while also making it more likely the patient or caregiver would initiate the conversation (knowing the provider received the information as well). A provider stated, ‘I think the more they know the better . . . Maybe if they see it on paper or see it from another source, they’d be more inclined to sort of give it another thought’ (PR ID # 116). Providers also noted that decisions about deprescribing are often not made within a single visit, and that having both parties aware of the concern could help to ensure that the topic would be discussed again at a future visit.
Providers are faced with additional challenges when caring for older adults with ADRD
Although providers value deprescribing and are open to deprescribing conversations with patients and caregivers, they face significant challenges in deprescribing for this population due to many competing health priorities and care complexity. One provider (PR ID # 85) stated, We might see these patients once every six months or once every four months . . . When we see those patients . . . there is a laundry list of five other things with their diabetes and their cholesterol and their heart disease and their heart failure to talk about.
Many providers spoke of time constraints as a barrier to deprescribing conversations, noting it takes time to discuss a medication reduction and alternatives, and then to agree upon a tapering plan. Deprescribing conversations were described as ‘tough’, ‘lengthy conversations’, especially if the patient has been on the medication for many years and is feeling well without symptoms.
Operational care delivery supports are needed to help providers effectively deprescribe
Providers identified that specific challenges to effectively deprescribe related to how the health care system is structured. Greater availability and ease of access to clinical resources during visits and information management within the provider’s office are needed for efficiency in the process. Providers shared that access to clinical tools to inform, to remind, and to guide decision-making would be helpful during the health care visit as they are assessing and evaluating competing health concerns. Many providers also reported struggles with managing the volume of information they receive and expressed a desire for help to ensure important information is not being missed. At the same time, some providers expressed that communication about medication is valuable, as one provider (PR ID # 32) shared: ‘. . . sending these mailings out to remind us, as to what people are on and side effects and contraindications can be helpful’. Providers reported deprescribing conversations can be very difficult, especially when there is strong resistance from the patient and caregiver; therefore, it would be helpful to have guidance on how best to approach deprescribing conversations.
Discussion
The findings from interviews with community-dwelling patients with ADRD, their caregivers, and providers offer further support for the feasibility of activating caregivers to participate in the deprescribing process using educational mailings. Bloomstone et al. 29 found strong support for providing materials to encourage the caregivers to initiate a conversation with the provider about educational materials on prescribing cascades among patients with ADRD and caregivers but also identified a need to understand how the materials might motivate such a conversation. The study advances these findings in two ways. First, patients and caregivers are often not aware of the potential for harm from a medication, and learning about this possibility was a motivator to initiate a conversation about the medication with the provider. Second, the findings underscore the caregiver’s influential position in the successful implementation of deprescribing and highlights the need to prioritize reaching and activating caregivers. Engaging the caregiver may appear to be a simple task, but in fact health care records may not contain the caregiver’s name or contact information, or permission to reach out to the caregiver directly, making it challenging to reach the caregiver outside of an appointment. Although policy efforts highlight the need for caregiver identification, more effective system-level strategies are needed to make this information readily available. 30
Two particularly important factors are likely to influence the success of efforts to increase deprescribing: patient and caregiver trust in the provider, and provider openness to including the patient and caregiver in deprescribing the process. Trust in the provider’s expertise was a strong underlying relational factor that would lead many caregivers to initiate a conversation with the provider. However, for some caregivers, trust is linked to deference, which may result in a hesitancy to raise questions to avoid being perceived as challenging the provider. The reluctance to engage in shared decision-making by the patient–caregiver is a known phenomenon. Blumenthal-Barby 31 noted contributing factors for this reluctance, such as health literacy, the cultural and value system of providers, and limited visit time. Providers will need to be aware of these factors and seek ways of encouraging patient and caregiver engagement during the visit. Providers in this study were not only supportive of mailing educational materials to patient and caregivers but also expressed an openness to having a patient or caregiver initiate a conversation about their medications. From the provider perspective, informed patients and caregivers would be more engaged in the conversation and more ready to accept deprescribing, increasing the chances of success. Research also supports the importance of the patient/caregiver–provider communication to achieve clinical outcomes through engagement and shared decision-making.29,31–33
Providers acknowledged the need to deprescribe potentially inappropriate medications for patients with ADRD, but seek effective clinical resources, alternatives to medications, and operational systems designed to support the deprescribing process within their practices. Providing such resources could help to address the known challenges that impede the deprescribing conversation, including time constraints, communication with multiple prescribers, and information management.19,20,32,34 The findings suggest these challenges may be magnified for patients with ADRD due to the disease trajectory and care complexities. The multiplicity of health conditions, behavioral and cognitive symptoms experienced, and the relational dynamics between the caregiver and the patient may all require the provider’s attention and preclude discussion of deprescribing. Evaluating these findings from a systems perspective confirms the need to consider multi-level interventions intended to promote deprescribing for patients with ADRD (Figure 1). Experts suggest effective health care delivery, including deprescribing, should be from a patient-centered and multi-level framework.15,35–37 These frameworks provide a conceptualization of the influencing factors related to deprescribing, which may guide the evaluation and decision-making to address gaps in the deprescribing process for sustainability.
Our study has limitations. While typical for qualitative studies, our sample was relatively small. The patients and caregivers were predominantly White and educated, the providers were drawn from a single health system, the inclusion criteria for patients with ADRD, and the financial incentives all may limit generalizability. We also focused on a hypothetical situation, rather than a real decision facing the interviewee; responses in real decision-making situations may differ. ADRD represents a disease spectrum with the role of caregiver becoming much more important as the disease advances. We did not explore whether there were any differences in willingness to engage in conversations about deprescribing based on the severity of dementia. Finally, the use of Zoom and telephone calls to conduct the interviews may have reduced the ability to cultivate an environment of trust and comfort for complete disclosure.
Conclusion
Sending educational materials to community-dwelling ADRD patients about the need to discuss deprescribing of potentially inappropriate medications may promote deprescribing conversations with providers. This study identified specific information that may motivate patients and caregivers to initiate a medication conversation. Our findings also underscore the importance of ensuring that medication-related information reach the caregiver as well as the patient, as the caregiver may be the one to initiate a conversation with the provider. Providers in this study acknowledged the importance of deprescribing, especially for patients experiencing ADRD, but face challenges in implementing deprescribing. Ongoing pragmatic trials will determine whether such interventions can stimulate deprescribing conversations and achieve reductions in prescribing of inappropriate medications among patients with ADRD.
Supplemental Material
sj-pdf-1-taw-10.1177_20420986221118143 – Supplemental material for Motivating deprescribing conversations for patients with Alzheimer’s disease and related dementias: a descriptive study
Supplemental material, sj-pdf-1-taw-10.1177_20420986221118143 for Motivating deprescribing conversations for patients with Alzheimer’s disease and related dementias: a descriptive study by Mary T. Antonelli, John S. Cox, Cassandra Saphirak, Jerry H. Gurwitz, Sonal Singh and Kathleen M. Mazor in Therapeutic Advances in Drug Safety
Footnotes
Acknowledgements
We thank the patients, caregivers, and providers who gave generously of their time in the sharing of their opinions, ideas, and experiences with us to conduct this research. Dr Antonelli acknowledges the support of the Junior Investigator Intensive Program of the US Deprescribing Research Network in conducting this study.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.