
Abstract
Background:
PIM-Taiwan criteria were first established in 2010 for potentially inappropriate medications (PIMs). Currently, updating of PIM criteria is mandatory because of newly established evidence and newly developed medications. This study aims to evaluate the prevalence of PIM based on country-specific PIM criteria and factors associated with PIM use by applying 2010 version and newly updating PIM-Taiwan criteria in a cohort with polypharmacy.
Methods:
The baseline data of Medication Safety Review Clinic Taiwan (MSRC–Taiwan) study were used to investigate the prevalence of PIMs. Older patients (aged ⩾65 years) who were either having polypharmacy or visited ⩾3 different physicians were enrolled between August and October 2007. Bivariate analysis and multivariate logistic regressions were used to evaluate the factors associated with PIM use.
Results:
The prevalence of having at least one PIM was 46.1% for 2010 version and increased to 74.6% for 2018 version. The average number of PIMs generally to be avoided per patient also increased for 2018 version (0.2 versus 1.2, p < 0.0001). In contrast, the average number of PIMs considering chronic conditions per patient decreased (0.6 versus 0.3, p < 0.001). The associated chronic conditions of PIM users were distinct between 2010 and 2018 version. The major leading PIMs were benzodiazepines (BZDs) in both versions of criteria.
Conclusions:
As there were significant differences in medication lists between PIM-Taiwan version 2010 and 2018, the prevalence of PIM and factors associated with PIM users varied accordingly. Physicians should pay special attention before prescribing BZDs which keep being the major leading PIM.
Introduction
The prevalence of chronic conditions that are related to an unhealthy lifestyle or the aging process is increasing. 1 Under current clinical guidelines, a higher number of medications is recommended to achieve the goal of treatment.2,3 In Taiwan, the reimbursement of National Health Insurance is mainly pay-for-service; 4 therefore, more effort is made to deal with the disease control, not to prevent diseases. To achieve the treatment goal, older patients are easy to have partake in polypharmacy when they have multiple chronic conditions. Two definitions of polypharmacy were stated most in the literature; one is cases in which more than four types of drugs are prescribed; the other is when certain drugs in all the prescriptions are considered to be potentially inappropriate to older adults. 5 Potentially inappropriate medications (PIMs) is used to define certain drugs that have higher probabilities for inducing drug-related adverse events – alternatives having less adverse events – or those without corresponding indications for long-term use.6,7 In general, PIMs are categorized as being in two classes: those which should be avoided generally, and those which should be avoided for patients diagnosed with certain chronic conditions. A recently published systemic review showed that polypharmacy is the major risk factor associated with PIMs use in different studies conducted across Europe. 8 Other risk factors with consistent positive association in multiple studies were patients having depression, low health quality and low functional status. Although many studies in different populations, such as home care recipients,9,10 patients with cancer11,12 or dementia13,14 showed that polypharmacy was associated with PIM use, limited studies directly focused on the prevalence of PIM among community-dwelling older adults using polypharmacy. Nonetheless, PIMs and polypharmacy were both associated with higher healthcare utilization and adverse drug reactions (ADRs) in previous studies.10,13,15 Reduction of polypharmacy and PIMs is an important strategy to improve the quality of patient care and health outcome among older adults. 16
To reduce polypharmacy and PIMs, explicit criteria are important tools and have been applied to clinical studies. 8 Country-specific PIM criteria would be preferred for clinical practice in local regions. Therefore, PIM-Taiwan criteria were established in a time-efficient methodology. 17 We found it was able to identify a similar number of PIMs in older Taiwanese regardless of their clinical setting by comparing with the Beers and PRISCUS criteria.10,18 As evidence increases showing the negative impact of PIMs and that certain medication classes have a higher incidence of drug-related adverse events, the explicit criteria are recommended to be updated in time.19,20 Hence, we updated our PIM-Taiwan criteria in 2018 by using the modified strategy from our previous version. Some differences were observed between two versions of the criteria, for instance the number of both categories of PIM was increased. In our previous studies, only statements for PIMs to be avoided generally were used in our nationwide studies owing to database limitations. In addition, PIM-Taiwan criteria had not been applied to the specific population using polypharmacy. It would be interesting to investigate the performance of the entire PIM-Taiwan criteria in identifying PIMs and whether the updated version yields a higher prevalence rate than the older version. The aim of this study is to determine the prevalence of PIMs, including those to be avoided generally, and considering chronic conditions in a cohort of community-dwelling older adults (aged ⩾65 years) with polypharmacy. Additional objectives include (1) finding the association of potentially inappropriate medications detected by 2010 and 2018 version of PIM-Taiwan criteria with the demographics and health-related characteristics; and (2) comparing the leading PIMs identified by two versions of criteria.
Methods
A Medication Safety Review Clinic Taiwan (MSRC-Taiwan) study 21 was used for our secondary data analysis to investigate the prevalence of PIMs and PIMs-associated factors using two versions of PIM-Taiwan criteria. The MSRC-Taiwan study was approved by the institutional review board at the National Taiwan University Hospital and conducted at two hospitals in Taipei, Taiwan. Briefly, 668 patients were referred from core physicians and 285 patients could not be reached after three attempts. After a telephone interview, 175 patients declined further assessment in this study. Finally, we enrolled 193 older patients who were aged 65 years or more and they had either been prescribed polypharmacy (eight or more medications for ⩾28 days) or visited three or more different physicians when we conducted 3-month surveillance from August to October 2007. Each patient had been evaluated for the appropriateness of their prescriptions during each clinic visit. Oral prescription medications and dietary supplements that were taken regularly for at least 28 days were reviewed for their appropriateness. Topical, local or inhaled medications were excluded because of their limited systemic effects.
Information about each patient was collected at a baseline for demographics, chronic conditions (including hypertension, type 2 diabetes, peptic ulcer disease, etc.), physical function (the Nagi Index and the Instrumental Actives of Daily Living), cognitive function (the Mini-Mental State Examination), mental health (the Geriatric Depression Scale–15 items), fall and dizziness history and the utilization of healthcare resources in the past 6 months.
PIM-Taiwan 2010 17 and 2018 version were used to identify PIMs. Both sets of criteria have two major classes of PIMs, including those generally to be avoided (the number of individual drugs for 2010 and 2018 version were 83 versus 131, respectively) and those for chronic conditions (the number of individual drugs for 2010 and 2018 version were 99 versus 131, respectively). To detect PIMs for chronic conditions, patients having specific chronic conditions for drug-disease or drug-syndrome PIMs were identified first. PIMs which were considered only for certain chronic conditions were then identified from the patients’ drug lists. At the person-level, the prevalence of PIMs was defined as those having at least one PIM regardless its category. At the drug-level, the prevalence of PIMs was defined as the numbers of PIMs among a total number of medications prescribed for the entire cohort. For the PIMs for chronic conditions, the prevalence was defined as the patients having at least one PIM divided by the total patient numbers having the specific chronic conditions. The difference of PIM prevalence (having at least one PIM) or average number of PIMs between 2010 and 2018 version of PIM-Taiwan criteria was determined by the Student’s t-test and the Chi-square test. To determine the factors associated with PIM use, individuals who had at least one PIM identified from two versions of PIM-Taiwan were compared with those without PIMs, respectively. We used the Shapiro–Wilk test to examine the normality of each continuous variable (age, the number of medications, frequency of clinic visits, number of physician with prescriptions, etc.). We performed the bivariate analysis using Student’s t-test for those with normal distribution, and the Wilcoxon rank-sum (Mann–Whitney) for those without normal distribution. For categorical variables including sex, race, marriage, education, etc., we used the Chi-square test with Fisher’s exact adjustment to their association with PIM users. All tests were two-tailed and significance was set at p < 0.05. If variables were considered as significantly associated in the bivariate analysis, they were selected for stepwise multivariate logistic regression models. We found that all variables with significant association with PIMs in bivariate analysis entering into logistic regression. Therefore, these sentences would be redundant. Data were analyzed using the Stata version 13 statistical package (Stata, College Station, TX, USA).
Results
This study enrolled 193 older patients who aged 76.2 ± 6.2 years and just over half of them were men (53.4%). A total of 72.5% were married and half of them had an education of more than 9 years. They had 9.0 ± 2.6 chronic conditions on average; among these chronic conditions, they had 9.0 ± 2.6 chronic conditions in average; among these chronic conditions the prevalence of hypertension was highest (89.6%), and chronic kidney disease was the lowest (3.1%). They took 8.9 ± 3.1 chronic medications and visited 2.1 ± 1.1 physicians and 4.8 ± 3.1 clinics in average. Only 10.4% of them had been hospitalized once in the most recent 6 months (Table 1). The overall prevalence of PIM in the 2010 version (46.1%) was lower than that in the 2018 version (74.6%) (Table 2). Similarly, higher average number of PIMs for each patient was detected in the 2018 version than in the 2010 version (0.9 ± 1.2 versus 1.6 ± 1.5, p < 0.0001). Nonetheless, the average number of PIMs to be generally avoided in older adults was 0.2 ± 0.4 for each patient in the 2010 version but increased to 1.2 ± 1.1 for each patient in the 2018 version. The number of patients having at least one PIM was also higher, by applying the medications to be avoided generally in 2018 version as against the 2010 version (73.6% versus 22.3%, p < 0.0001). In contrast, the average number of PIMs for each patient detected by listed medication/medication classes to be avoided in older adults with specific conditions in the 2010 version was higher than those in the 2018 version (0.6 ± 1 versus 0.3 ± 0.7, p < 0.001).
Basic characteristics of the older patients in Medication Safety Review Clinic Taiwan (MSRC-Taiwan) study and patient-level bivariate analysis by the presence of least one PIM according to the 2010 and 2018 versions of PIM-Taiwan criteria.
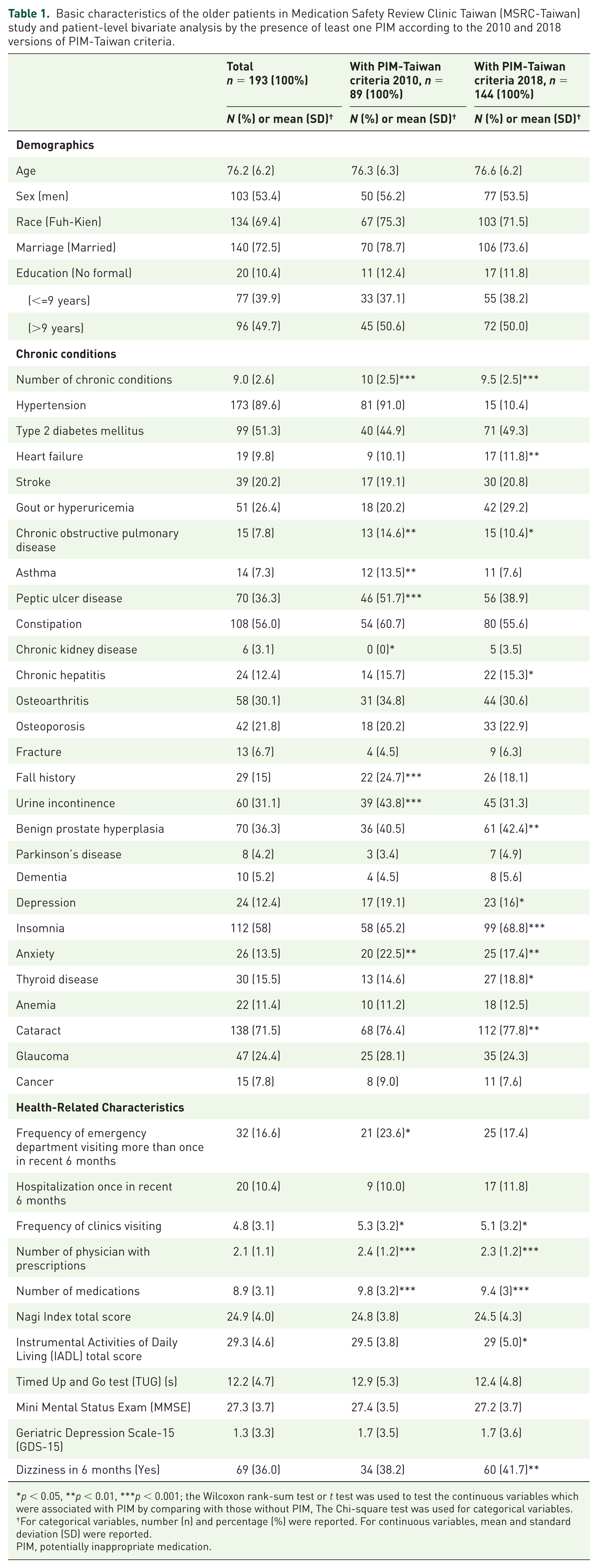
p < 0.05, **p < 0.01, ***p < 0.001; the Wilcoxon rank-sum test or t test was used to test the continuous variables which were associated with PIM by comparing with those without PIM, The Chi-square test was used for categorical variables.
For categorical variables, number (n) and percentage (%) were reported. For continuous variables, mean and standard deviation (SD) were reported.
PIM, potentially inappropriate medication.
The prevalence of having at least one PIM and average number of PIMs prescribed for each patient in Medication Safety Review Clinic Taiwan (MSRC-Taiwan) study.
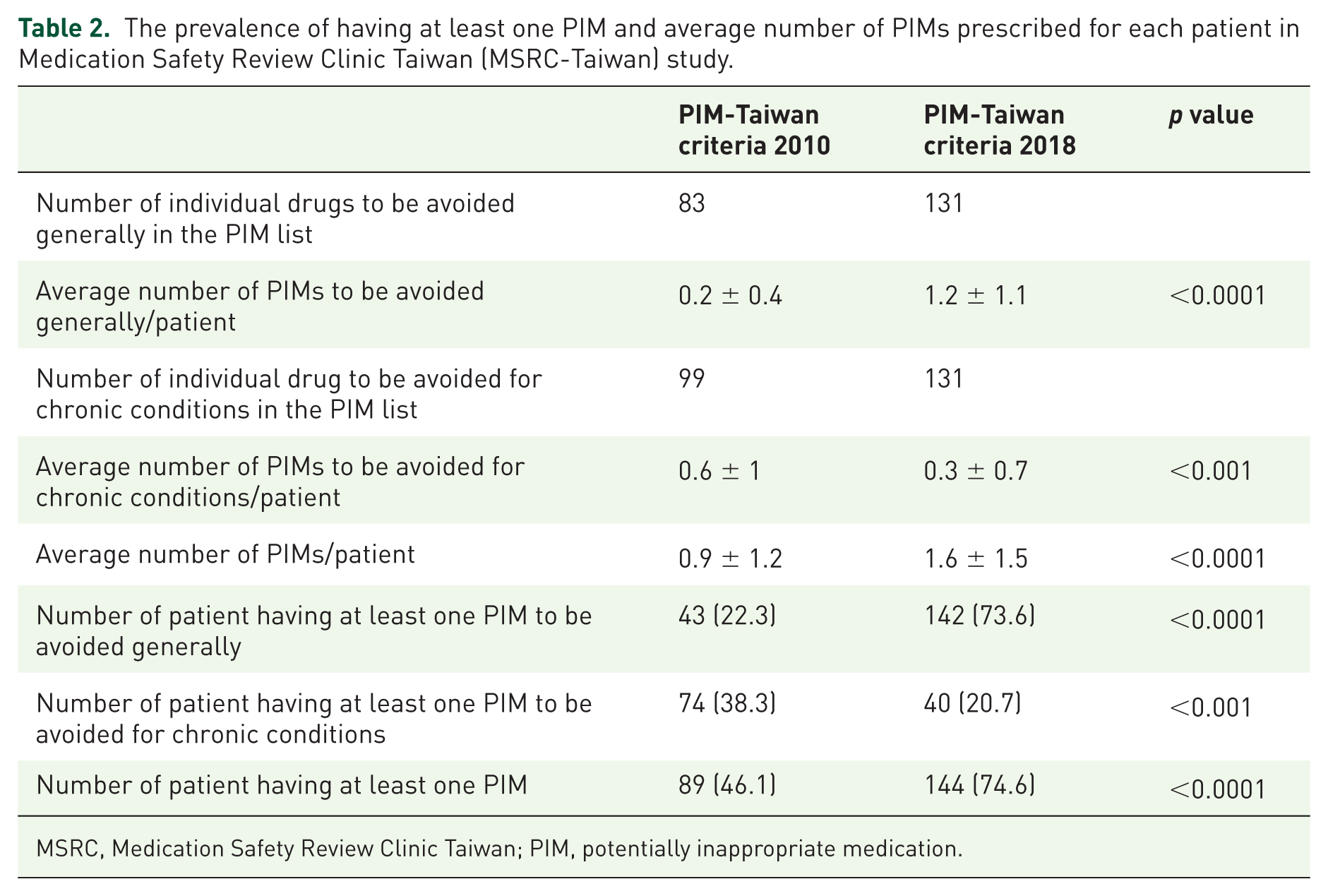
MSRC, Medication Safety Review Clinic Taiwan; PIM, potentially inappropriate medication.
The leading five PIMs to be avoided generally in the 2010 version were oxazolam (n = 13), imipramine (n = 8), clonazepam (n = 6), chlorzoxazone (n = 4), and digoxin (n = 3). For the 2018 version, they were alprazolam (n = 34), doxazosin (n = 24), zolpidem (n = 23), lorazepam (n = 21) and glyburide (n = 14) (Figure 1, Table 3). The number of patients that had PIMs to be avoided generally was higher in 2018 version than those in 2010 version (73.6% versus 22.3%, p < 0.0001) (Table 2). In contrast, the number of patients that had PIMs to be avoided for chronic conditions was higher in the 2010 version than in the 2018 version (38.3 versus 20.7, p < 0.001). In the 2010 version, patients having chronic obstructive pulmonary disease (COPD) had the highest probability (80.0%) of having PIMs (Table 4). In contrast, there was no patient with bronchial asthma, COPD to be identified with drug-disease interaction according to 2018 version. In the 2018 version, patients having a history of falls or fractures had the highest probability (70.0%) of having PIMs. No one having chronic kidney disease was identified with drug-disease interaction according to both versions of PIM-Taiwan criteria.
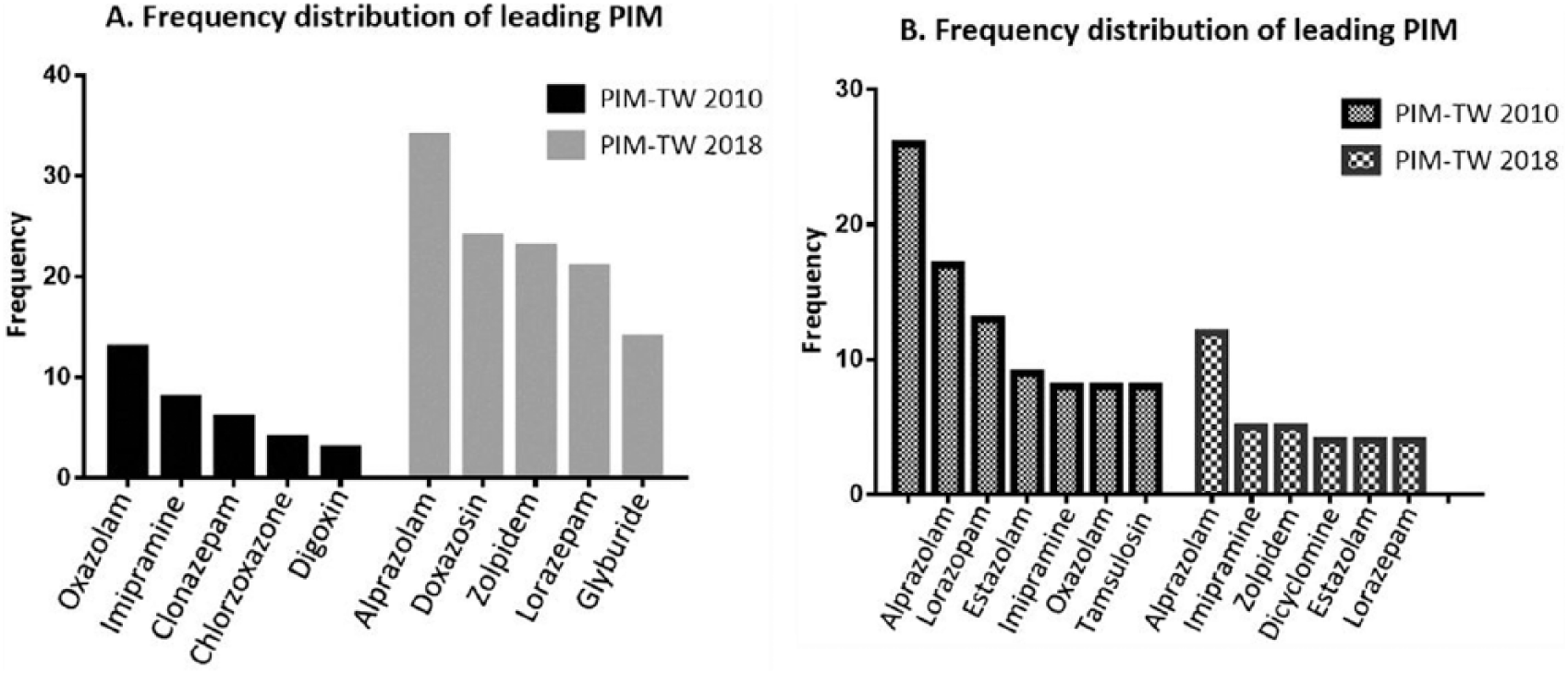
(A) Frequency of leading potentially inappropriate medication (PIM) generally to be avoided in the 2010 and 2018 versions of PIM-Taiwan criteria and (B) frequency of leading potentially inappropriate medication (PIM) considering chronic conditions in the 2010 and 2018 versions of PIM-Taiwan criteria.
Leading five PIMs in the 2010 and 2018 version of PIM-Taiwan criteria.
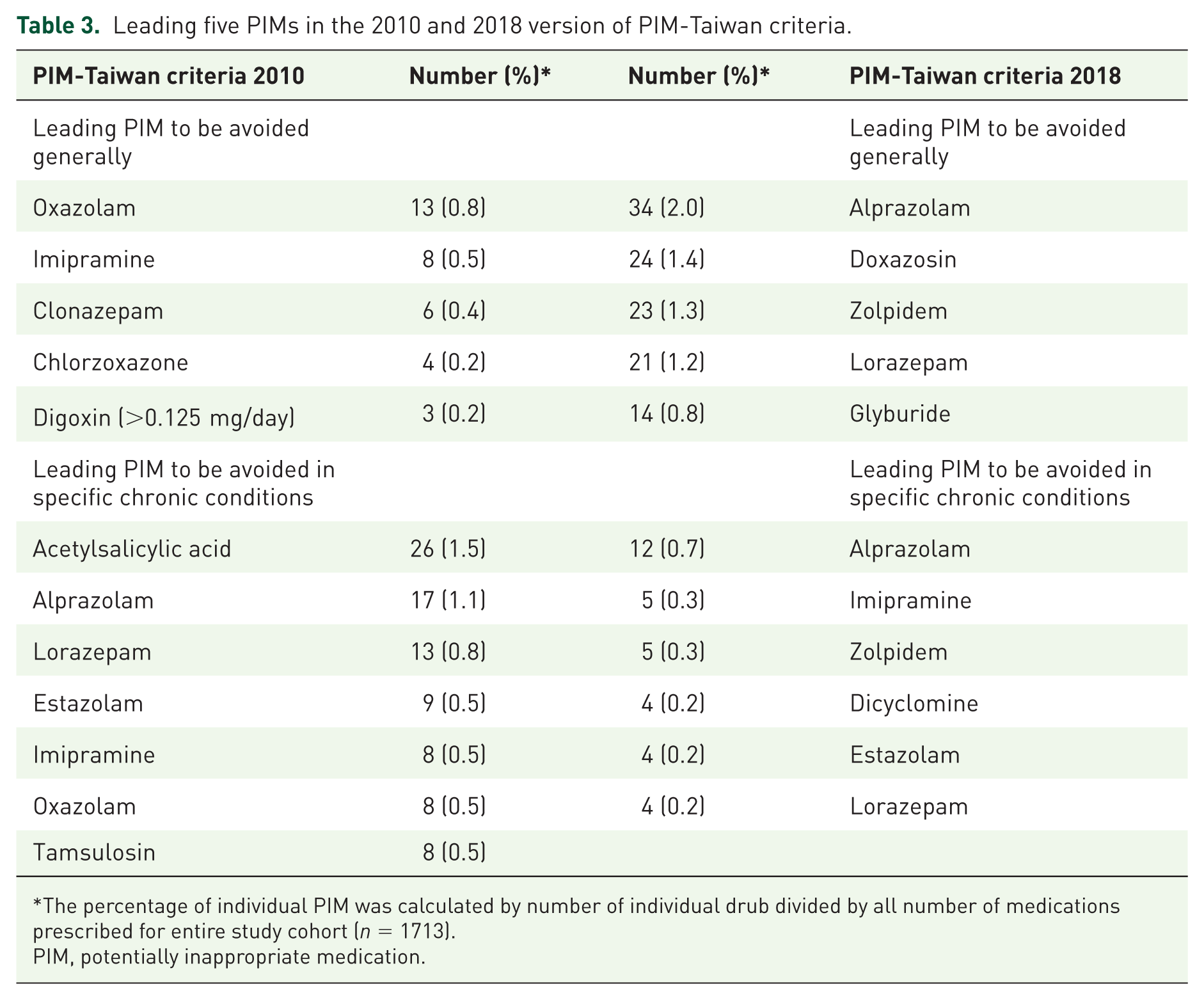
The percentage of individual PIM was calculated by number of individual drub divided by all number of medications prescribed for entire study cohort (n = 1713).
PIM, potentially inappropriate medication.
The prevalence of PIM considering chronic conditions.
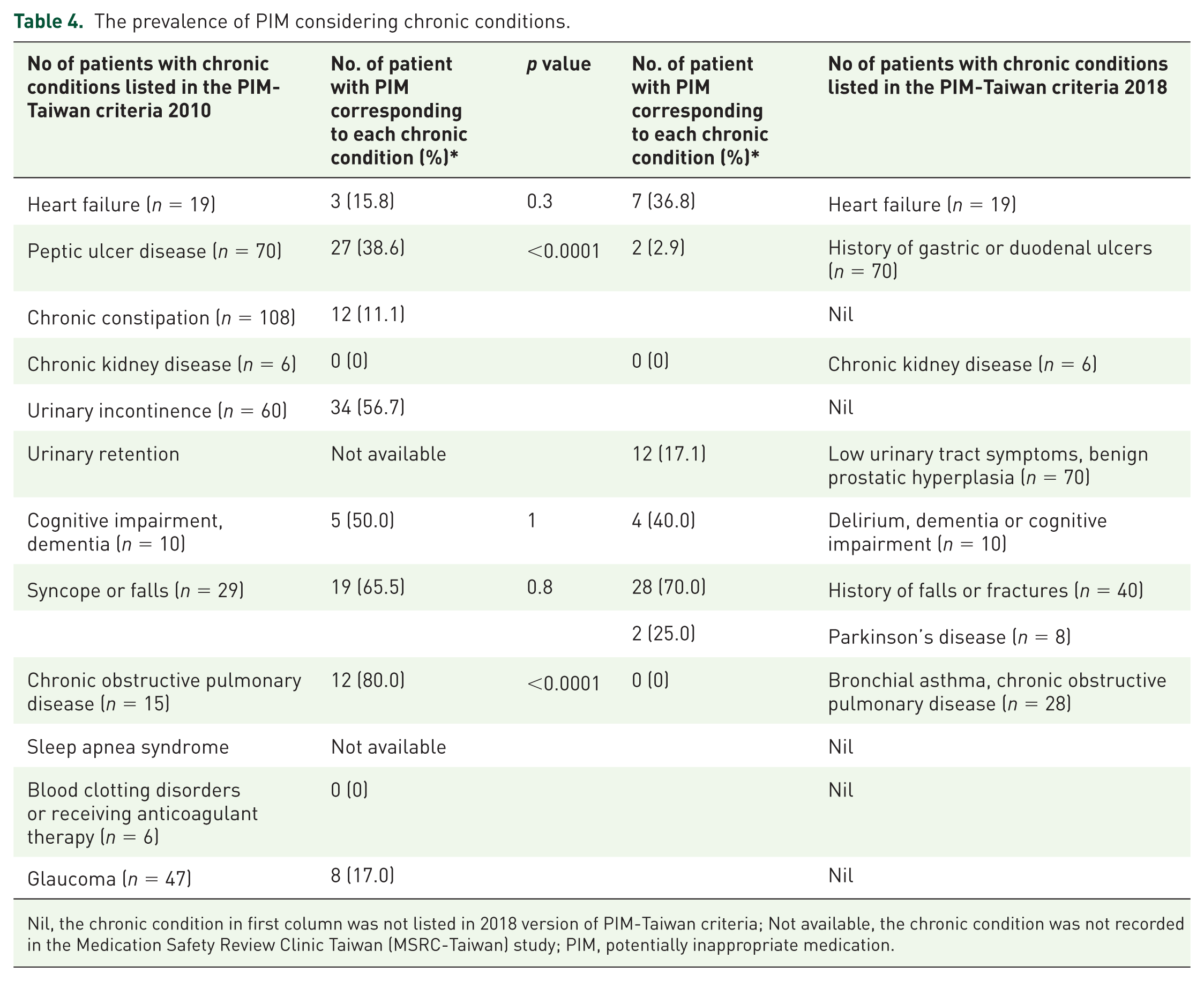
Nil, the chronic condition in first column was not listed in 2018 version of PIM-Taiwan criteria; Not available, the chronic condition was not recorded in the Medication Safety Review Clinic Taiwan (MSRC-Taiwan) study; PIM, potentially inappropriate medication.
The bivariate analysis for associated factors showed there was no demographic factor associated with PIM use in PIM-Taiwan 2010 and 2018 (Table 1). The users of both versions of PIM-Taiwan had a higher number of chronic conditions than those who did not have PIMs. For PIM-Taiwan 2010, PIM users had a higher percentage of chronic obstructive pulmonary disease (COPD), asthma, peptic ulcer disease, fall history, urine incontinence and anxiety. In contrast, PIMs user defined by 2018 version had a higher percentage of heart failure, chronic obstructive pulmonary disease, chronic hepatitis, benign prostate hyperplasia, depression, insomnia, anxiety, thyroid disease and cataracts. For healthcare resource utilization, PIM-Taiwan 2010 users had higher healthcare resource utilization, except hospitalization. However, PIM-Taiwan 2018 users did not have a higher level of emergency department visits or hospitalization. There was no association between the results of the functional assessment and PIM-Taiwan 2010 users. In contrast, PIM-Taiwan 2018 users had lower IADL scores and a higher probability of dizziness.
In multivariate analysis, most associated factors were different between the 2010 and 2018 versions (Table 5). Based on both versions of PIM-Taiwan, patients prescribed with higher number of medications had a higher probability of having PIMs. For chronic conditions associated with PIMs use, the probability was highest for asthma (OR = 4.9) and lowest for anxiety (OR = 3). In the 2018 version of PIMs, patients having anxiety, insomnia, and benign prostate hyperplasia had a higher probability of PIMs (OR were 16.3, 11.9, and 5.4, respectively). PIMs use was also associated with dizziness in the 2018 version.
Multivariate logistic regression for factors associated with potentially inappropriate medications.
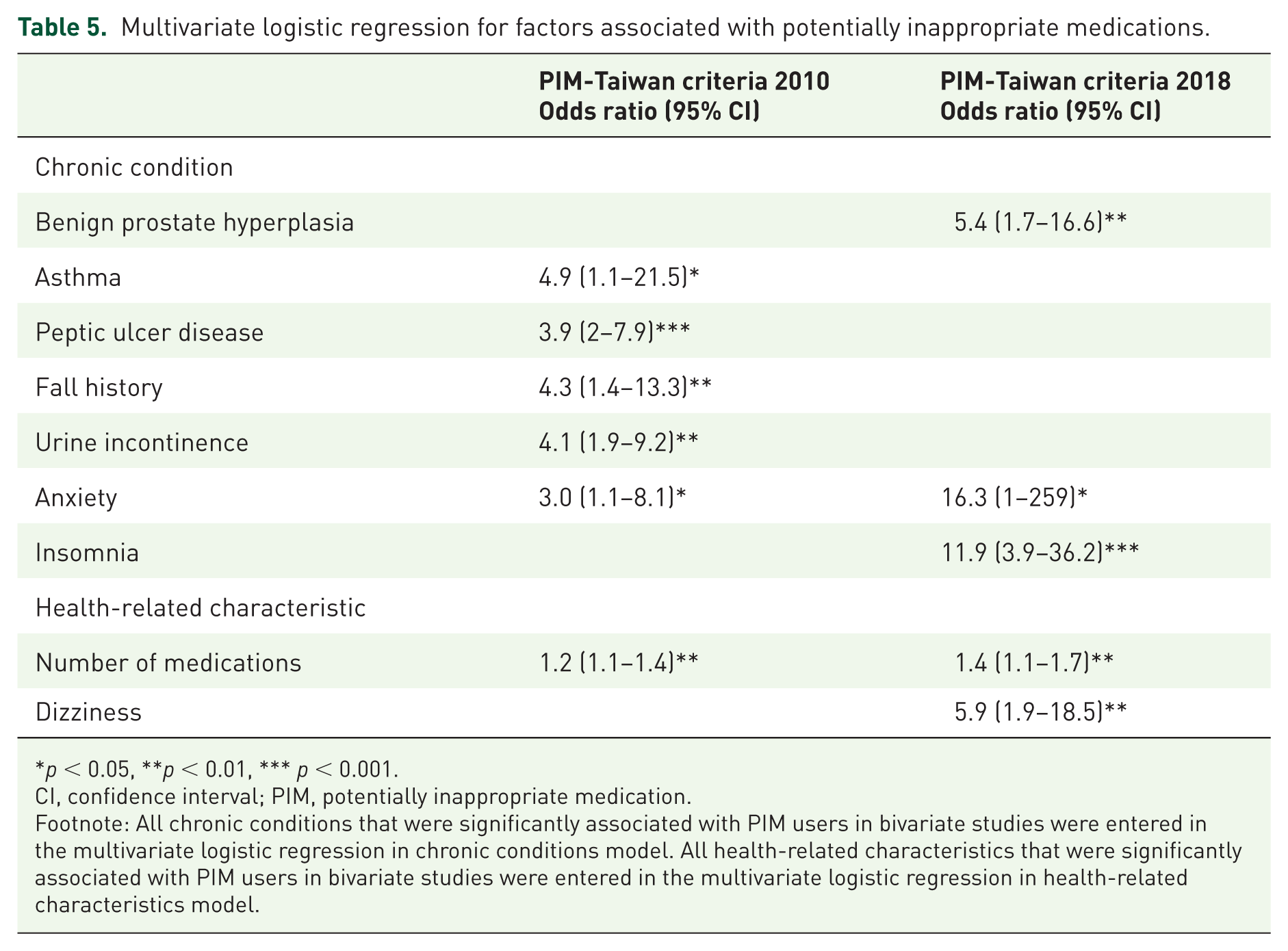
p < 0.05, **p < 0.01, *** p < 0.001.
CI, confidence interval; PIM, potentially inappropriate medication.
Footnote: All chronic conditions that were significantly associated with PIM users in bivariate studies were entered in the multivariate logistic regression in chronic conditions model. All health-related characteristics that were significantly associated with PIM users in bivariate studies were entered in the multivariate logistic regression in health-related characteristics model.
Discussion
In this study, we found that the overall prevalence of PIMs increased from 46.1% to 74.6% after revising our criteria. The average number of PIMs among each patient increased from 0.9 to 1.6. Although the overall number of PIMs listed in our new criteria increased up to 44%, we found that specific classes of medications to be avoided generally or for certain chronic conditions accounted for the increment. Therefore, the chronic conditions having associations with PIMs were different between two the versions of criteria. The risk factor of having PIMs based on two version of the criteria is the number of medications after considering health-related characteristics. The major medication class of leading PIMs is benzodiazepine (BZD).
The PIM-Taiwan criteria have been applied to determine the overall nationwide prevalence of PIMs in Taiwan.10,18 The incidence changed when we focused on different clinical settings. The prevalence is highest (73.3%) among older patients having at least one clinic visit in 1 year and lower (60.0%) among older home healthcare service recipients. Because there were so many sets of criteria developed worldwide,19,20,22–25 only one study conducted in the country other than Taiwan used PIM-Taiwan criteria to determine PIMs incidence. Among community dwelling older Brazilians, the prevalence of PIMs in PIM-Taiwan criteria was 31.3%. 26 In this study, the prevalence in the 2010 version of PIM-Taiwan criteria was relatively higher than that in the Brazil study but lower than the nationwide cohort of Taiwan. This study was conducted in a medical center and its branch, 21 the physicians in this hospital prescribed the majority of medications for this cohort. The prescribing preference of physicians and drugs availabilities in different countries and regions in Taiwan may account for the differences between the studies. The most important finding of this study was that the prevalence of having PIM was improved in the updated version of PIM-Taiwan criteria. Such improvement may be related to the increase in the number of individual drugs listed in the updated version, and all BZDs, Z-drugs, glyburide and doxazocin were considered as potentially inappropriate.
There were differences between associated factors in the two versions of the PIM-Taiwan criteria. Compared with the 2010 version, all antipsychotic, Z-drugs, BZD and alpha-blockers were considered as potentially inappropriate in 2018 version. Patients having psychological conditions (anxiety and insomnia, etc.) and benign prostate hypertrophy had higher probabilities of being prescribed these medications; therefore, these chronic conditions were associated with PIM use. Both long-acting and short-acting BZDs were proved to be associated with fall and fall-related injury. 27 It is reasonable to consider all BZDs as potentially inappropriate. In spite of most PIM criteria listing BZDs because of their adverse effects, the use of long-term BZDs among older adults was still common. 28 Detailed evaluation of fall risk and education for fall prevention were necessary before prescribing BZDs for older patients with insomnia. 27 For PIMs with drug-disease interaction, acetylsalicylic acid was considered as potentially inappropriate among patients having peptic ulcer disease in the 2010 version without considering its daily dose, but only aspirin >325 mg considered as potentially inappropriate in 2018 version. In this study population, 35.7% of patients having peptic ulcer disease were still prescribed with acetylsalicylic acid (100 mg); therefore, peptic ulcer was one of the risk factors in the 2010 version PIM users but not in the 2018 version.
In previous studies, most of the results showed that PIMs were associated with higher healthcare utilization.10,15,18,26 We also demonstrated this association in bivariate analysis. However, it was not significant after considering all health-related characteristics in logistic regression analysis. In the study among community-dwelling older adults in Brazil, Lucchetti showed PIM-Taiwan criteria has higher specificity but lower sensitivity for hospitalization and fall by comparing with the Beers, STOPP, and EU(7)-PIM criteria. 26 There were several reasons for these discrepancies. First, this cohort enrolled population with higher functional status and lower healthcare utilization in the baseline. Second, the sample size was relatively small and it could not represent entire older Taiwanese. Third, the education level was relatively high; therefore, the health literacy may be better than other sectors of the population. Further studies with large sample sizes and participants with different demographic characteristics are needed to confirm that avoidance of PIMs in PIM-Taiwan criteria lowers healthcare utilization.
Limitations of the study include the fact that not all chronic diseases listed in both sets of criteria for prevention of drug-disease interactions were fully addressed in this study conducted in 2007. This study was designed as a cross-sectional study, thus the effect of PIM use on healthcare utilization could not be determined. Both versions of PIM criteria were established based on medications that were available in Taiwan. A modification of PIM-Taiwan criteria should be applied to regions having different drug reimbursements in their national health insurance. The sample size of this study was relatively small, so some PIM risk factors might not be found to have associations with PIM users.
Conclusions
Drug prescribing for older patients is a complex decision made by physicians who need to consider the multiple chronic diseases and ADRs specific to each patient. Potentially inappropriate criteria is an important tool in preventing ADRs but the drugs listed in PIM-Taiwan criteria would be one of the major determinants of the PIM prevalence and their ability to detect PIMs. 29 The updated PIM-Taiwan could identify more PIMs than older version. Physicians should pay special attention before prescribing BZDs which keep being the major leading PIM. These tools, as well as clinical decisions made by physicians after comprehensive evaluation and detailed examination, would complement each other to prevent ADRs. Further studies are needed to evaluate their ability to improve health quality and prevent adverse drug events among older adults.