
Abstract
Neurocognitive adverse events have been observed with the widespread use of 3-hydroxy-3-methylglutaryl-CoA reductase inhibitors or “statins,” which reduce low-density lipoprotein cholesterol (LDL-C) levels and subsequently cardiovascular risk. The United States Food and Drug Association directed manufacturers of proprotein convertase subtilisin-kexin type 9 (PCSK9) inhibitors to monitor for neurocognitive adverse events due to their potent effects on LDL-C reduction, which is a proposed mechanism for neuronal cell dysfunction. Other proposed mechanisms for PCSK9 inhibitor-associated neurocognitive adverse events include N-methyl-
Introduction
Lipid-lowering agents are among the most commonly prescribed medications in the world. In 2011, one in four United States (US) adults reported use of a prescription lipid-lowering medication in the past 30 days, and most were prescribed a 3-hydroxy-3-methylglutaryl-CoA (HMG-CoA) reductase inhibitor (known as “statins”) alone. 1 Significant reductions in low-density lipoprotein cholesterol (LDL-C) levels, leading to reduced risk of clinical atherosclerotic disease, drives the common use of statins.2–5 However, widespread use of statins has also resulted in several reported adverse events including muscle symptoms, incident diabetes, and cognitive impairment. 6 Following review of the Adverse Event Reporting System database and other published literature in 2012, the US Food and Drug Administration (FDA) issued statin label warnings for reversible cognitive adverse events such as cognitive dysfunction, confusion, and memory impairment. 7 The correlation between intense LDL-C reduction and neurocognitive adverse events remains unclear, but a proposed mechanism is that the inhibition of cholesterol synthesis may affect the essential functions of neurons whose cell membranes and myelin consists of cholesterol and other lipids. 8 The evidence supporting this proposed mechanism is variable due to the inclusion of patient populations at low risk for clinical decline, self-reported memory impairment versus cognitive testing, and largely case reports or observational studies. 9
Like statins, PCSK9 inhibitors including alirocumab and evolocumab provide a robust LDL-C reduction, approximately 60% as monotherapy.4,5 These monoclonal antibodies inhibit the metabolism of PCSK9, which regulates the degradation of LDL receptors in response to intracellular cholesterol concentrations. 10 LDL receptors are rendered more susceptible to enzymatic degradation rather than recycled back to the surface of the hepatocyte when they bind to PCSK9. PCSK9 inhibition results in increased circulation of LDL receptors to clear LDL-C from the bloodstream. These agents are prescribed mainly for patients with very elevated LDL-C levels (e.g., familial hypercholesterolemia), patients with history of clinical atherosclerotic disease who require additional LDL-C reduction, and patients who cannot tolerate statins or other lipid-lowering therapies. 11
PCSK9 inhibitors are generally well-tolerated and lack adverse events commonly seen with previous lipid-lowering therapies such as myopathy. However, there is significant interest in the association between PCSK9 inhibitors and cognitive impairment given the reports of such adverse events with statins and intense LDL-C reduction. In 2014, the FDA directed manufacturers to monitor for neurocognitive adverse events and consider neurocognitive testing, but without recommendations for specific assessment methods or instruments. 12 The objective of this narrative review is to describe the following with regards to PCSK9 inhibitor use and neurocognitive adverse events: proposed mechanisms, incidence and description of adverse events, neurocognitive assessments utilized in clinical trials, and clinical implications of the FDA’s manufacturer directive. 7
Methods
A search of the MEDLINE and PubMed databases was performed to identify articles for a narrative review of neurocognitive adverse events associated with PCSK9 inhibitor use. Combinations of the Medical Subject Headings and terms were searched: PCSK9 inhibitor, alirocumab, SAR236553, REGN727, evolocumab, AMG 145, adverse events, neurocognition, cognitive impairment, and cognitive adverse events. The search was restricted to phase II or phase III human studies in English for articles from January 2010 to March 2019. References cited in the articles identified by the search were also evaluated and included if relevant. A total of 12 articles for alirocumab and evolocumab were reviewed to describe the incidence of neurocognitive adverse events. A third agent, bococizumab, was withdrawn from development in 2016 and therefore excluded from this review.
Proposed mechanisms
The precise mechanism of neurocognitive adverse events associated with PCSK9 inhibitor use is unknown. The molecular size of the PCSK9 monoclonal antibodies are substantially greater than small molecules that easily penetrate the blood brain barrier.13,14 However, sustained low LDL concentrations in the body may pose problems related to neurocognition through a variety of pathways. Figure 1 depicts a conceptual and theoretical framework of four mechanistic routes.

Proposed mechanisms of PCSK9 inhibitor-associated neurocognitive adverse events.
Dysregulation of lipid and glucose metabolism
The biochemical process behind cholesterol synthesis – regulation of the mevalonate or HMG-CoA reductase pathway – is well-known, and serves as the site of action for statins. 15 Both lipid and glucose metabolism are regulated by homeostatic processes. The dysregulation of these processes may have a role in the evolution of beta-amyloid (Aβ) and tau proteins. 16 The presence and overproduction of Aβ and tau proteins form the basis of Alzheimer’s disease and other dementias. Apolipoprotein E (ApoE) is an essential regulator of brain cholesterol metabolism, and various ApoE mutations could serve as risk factors for Alzheimer’s disease.15,16
Statins increase α-secretase activity and decrease Aβ production based on animal and clinical studies. 17 In contrast, the β-site amyloid precursor protein (APP) promotes Aβ production. The rate-limiting step for Aβ production is severance of APP by the β-site APP-cleaving enzyme 1 (BACE 1). PCSK9 is suggested to contribute to the disposal of nonacetylated BACE 1 where overexpression and downregulation significantly decreased and increased BACE 1 levels, respectively. 18 These findings propose that PCSK9 may be involved with BACE1 metabolism and Aβ production. 18 However, this evidence is not accepted by others where PCSK9 downregulation failed to affected BACE 1 levels in animal models. 19
It is possible that PSCK9 promotes neuroinflammation in patients with Alzheimer’s disease and alcohol use disorder (AUD) since impairment of the blood brain barrier may alter PCSK9 concentrations. 20 Brain autopsies in patients with Alzheimer’s disease reported elevated PCSK9 messenger RNA and protein levels in the frontal cortex. Cerebral spinal fluid PCSK9 concentrations were significantly higher in patients with Alzheimer’s disease and AUD compared with controls.
N-methyl-d -aspartate receptor modulation
Cholesterol is reportedly a potent endogenous modulator of N-methyl-
Altered neuronal cell membrane integrity
Altered cholesterol synthesis leading to low or very low levels of LDL-C is a controversial and commonly suggested cause of neurocognitive adverse events associated with the use of lipid-lowering medications. These actions may influence the development and function of neuronal cell membranes since lipids have a vital role in cell membrane integrity. 23
Patient risk factors for neurocognitive impairment
PCSK9 inhibitors and genetic variants leading to sustained low LDL-C concentrations may also promote the cardiovascular risk factors for Alzheimer’s disease and neurocognitive impairment.8,23 The overall risk factors for Alzheimer’s disease, such as age, obesity, and comorbidities (e.g., hypertension, diabetes) must be considered in the patient assessment.8,16,24
Two large-scale studies examined the possible causal effect of genetic variants on the risk of cognitive impairment using the Mendelian randomization method.25,26 Low LDL cholesterol levels due to PCSK9 genetic variants had no causal effect on cognitive impairment in one study (N = 111,194) but suggested that the low LDL levels may have a causal effect in reducing the risk of Alzheimer’s disease. 25 A second large study (N = 337,348) found no strong associations between PCSK9 alleles and cognitive impairment, contrary to the link between ApoE mutations and cognitive impairment. 26 Together, these studies highlight the difficulty in attributing cognitive impairment to specific genetic PCSK9 variants.
PCSK9 inhibitors: incidence of neurocognitive adverse events
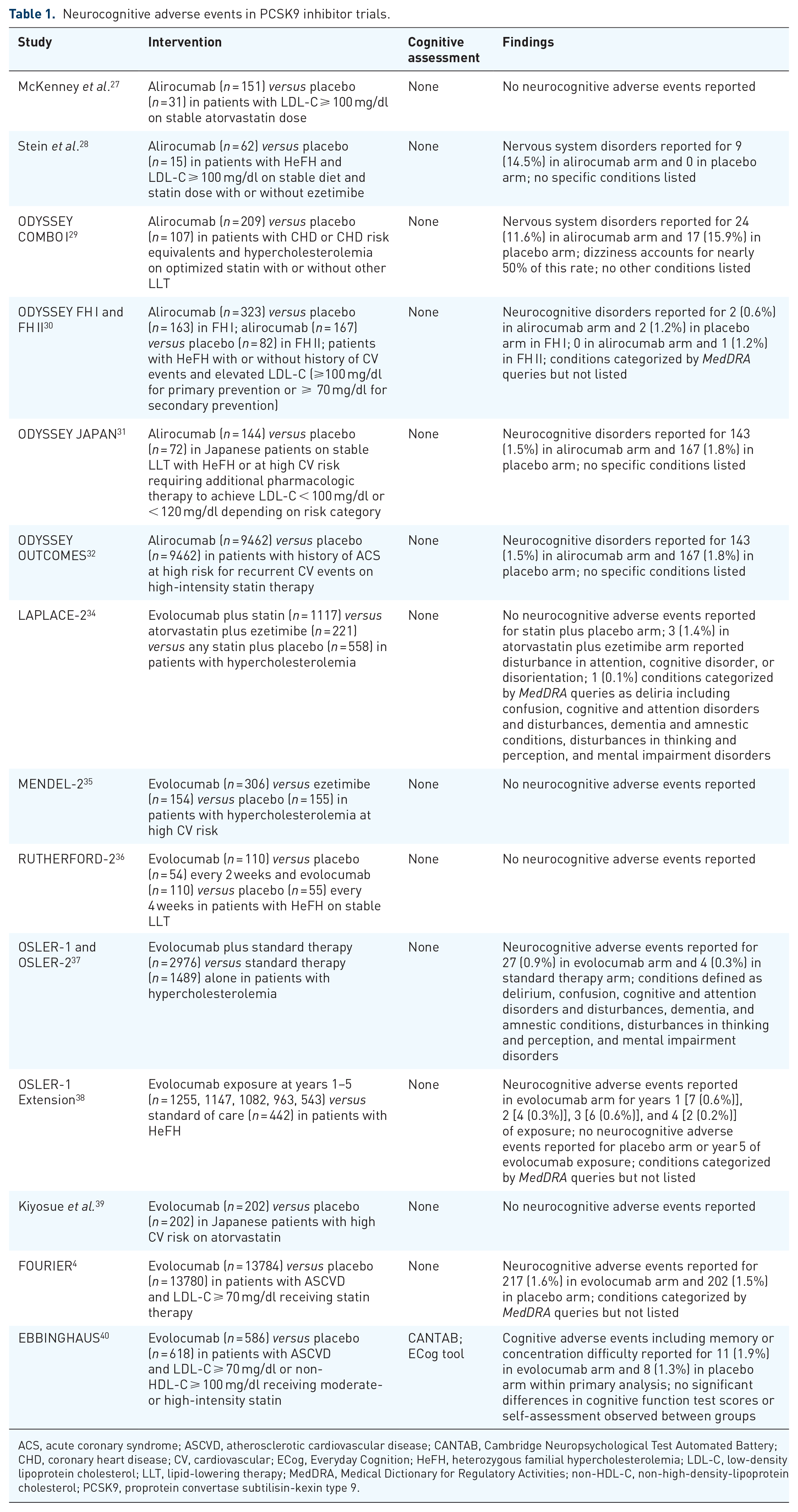
Following the FDA directive to manufacturers, many study investigators observed for neurocognitive adverse events based on the proposed mechanisms described above. The table lists the findings from the phase II and III trials that evaluated neurocognitive adverse events.4,27–40 Specific conditions, broadly described as neurocognitive adverse events or disorders, are also included in the table if provided by the study authors.
Alirocumab
Two early studies compared alirocumab (SAR236553/REGN727) with placebo in patients on statin therapy.24,27,28 Neurocognitive adverse events were not reported in a study by McKenney et al. on safety and LDL-C-lowering efficacy of SAR236553 versus placebo in patients with primary hypercholesterolemia taking atorvastatin (N = 183). 27 Stein et al. compared the LDL-C-lowering efficacy of SAR236553 with placebo in patients with heterozygous familial hypercholesterolemia on statin therapy with or without ezetimibe in a phase II trial (N = 77). 28 Nine (20%) patients in the treatment arm reported nervous system disorders compared with zero patients receiving placebo, but the type or severity of the nervous system disorders was not discussed.
The ODYSSEY series of double-blind, placebo-controlled trials analyzed the efficacy and safety of alirocumab. A custom Medical Dictionary for Regulatory Activities (MedDRA) query was utilized to identify neurocognitive adverse events in these studies based on five High-Level Group Terms, described in the table. The ODYSSEY LONG TERM investigators compared alirocumab with placebo in patients with heterozygous familial hypercholesterolemia and/or clinical ASCVD on an optimized statin dose (N = 2341). 5 The mean study-drug exposure was 70 weeks, and the mean age of study participants was 60 years. Neurocognitive adverse events were reported for 18 (1.2%) patients receiving alirocumab and four (0.5%) patients receiving placebo. Of the 18 patients, 3 reported at least two consecutive LDL-C levels below 25 mg/dl. The most common neurocognitive events in the alirocumab arm included amnesia (n = 5), memory impairment (n = 4), and confusional state (n = 4). No statistically significant differences between the alirocumab and placebo arms with regards to incidence of neurocognitive adverse events were found.
The 52-week ODYSSEY COMBO I study compared alirocumab with placebo in patients with hyperlipidemia and established coronary heart disease or coronary heart disease risk equivalents on an optimized statin dose with or without other lipid-lowering therapy (N = 316). 29 No patients in the alirocumab arm and only one patient in the placebo arm (0.9%) reported neurocognitive events. Overall, the incidence of adverse events was comparable between the two treatment arms except for injection-site reactions. ODYSSEY FH I (n = 486) and FH II (n = 249) compared alirocumab with placebo in patients with heterozygous familial hypercholesterolemia and inadequate LDL-C control on optimized lipid-lowering therapy at 78 weeks. 30 Within FH I and FH II combined, a total of two patients taking alirocumab and three patients taking placebo reported neurocognitive disorders. The cardiovascular outcomes trial ODYSSEY OUTCOMES noted a similar incidence of neurocognitive disorders between the alirocumab (1.5%) and placebo (1.8%) arms. 32 Among the ODYSSEY trials, the overall incidence of adverse events was similar between groups except for injection-site reactions.29,30,32
The efficacy and safety of alirocumab was also studied in native Asian populations. ODYSSEY KT compared alirocumab with placebo in South Korean and Taiwanese patients with high cardiovascular risk on an optimized statin dose (N = 199). 33 One patient (1%) receiving placebo reported neurocognitive disorders within the entire study population. On the contrary, ODYSSEY JAPAN reported nervous system disorders in 15.4% of patients on alirocumab (n = 143) and 11.1% of patients on placebo (n = 72). 31 The mean age of the study group was 60.8 years. All patients in the study received a stable dose of statin, and 14.4% of these patients received additional lipid-lowering therapy. Two patients experiencing nervous system disorders on alirocumab had two consecutive LDL-C levels less than 25 mg/dl. It is unclear whether these adverse events resulted in treatment discontinuation. Potential relationships between PCSK9 inhibitor use and cognitive impairment in Japanese subjects have not been described. However, this adverse event is particularly concerning due to the increased prevalence of all-cause dementia among the rapidly aging Japanese population. 41
Evolocumab
The safety and efficacy of evolocumab was first evaluated in the randomized, open-label studies OSLER-1 and OSLER-2 for patients with cardiovascular risk factors on standard therapy. 37 The combined incidence of adverse events (69.2% versus 64.8%) and severe adverse events (7.5% versus 7.5%) was comparable between the evolocumab and standard therapy groups. Of patients in the combined evolocumab arm, 27 (0.9%) experienced neurocognitive adverse events (conditions defined in Table 1), which was not associated with differences in minimum post-baseline LDL-C levels. In the OSLER-1 Extension Study, only 0.4% of patients receiving evolocumab (n = 1255) experienced neurocognitive adverse events compared with zero patients receiving standard therapy. 38 Additionally, no neurocognitive adverse events were reported in a phase III trial of evolocumab in Japanese patients at high cardiovascular risk on statin therapy (N = 404). 39
Neurocognitive adverse events in PCSK9 inhibitor trials.
ACS, acute coronary syndrome; ASCVD, atherosclerotic cardiovascular disease; CANTAB, Cambridge Neuropsychological Test Automated Battery; CHD, coronary heart disease; CV, cardiovascular; ECog, Everyday Cognition; HeFH, heterozygous familial hypercholesterolemia; LDL-C, low-density lipoprotein cholesterol; LLT, lipid-lowering therapy; MedDRA, Medical Dictionary for Regulatory Activities; non-HDL-C, non-high-density-lipoprotein cholesterol; PCSK9, proprotein convertase subtilisin-kexin type 9.
The FOURIER study compared evolocumab with placebo for secondary prevention of clinical ASCVD in patients on optimized statin therapy with or without ezetimibe (N = 27,564). 4 Neurocognitive adverse events were reported in 1.6% and 1.5% of evolocumab and placebo groups, respectively. Patients enrolled in FOURIER were screened for eligibility for the EBBINGHAUS study (N = 1204) – a randomized placebo-controlled trial evaluating the cognitive function of patients adding evolocumab to statin therapy. 40 The assessment tool and study endpoints are described in the Neurocognitive Assessment section of this review. The mean age of patients was 63 years, and the median study period was 19 months. The mean ± standard deviation (SD) change in the raw score for the Cambridge Neuropsychological Test Automated Battery (CANTAB) spatial working memory strategy index was −0.21 ± 2.62 for evolocumab and −0.29 ± 2.81 for placebo compared with baseline (p < 0.001 for non-inferiority; p = 0.85 for superiority). The authors did not report significant differences between groups for working memory, episodic memory, or psychomotor speed. Most patients within the evolocumab arm were prescribed a high-intensity statin (n = 399; 68.1%), with 5.5% of these patients on concomitant ezetimibe. A post hoc analysis revealed no direct relationship between LDL-C levels and neurocognitive changes. Significant differences in ECog questionnaire results were not observed between groups for either individual domains or the total score. Cognitive adverse events, categorized by MedDRA terms, were reported in 1.9% of patients on evolocumab and 1.6% of patients on placebo.
Neurocognitive assessment
Cognitive decline is assessed among patients with various forms of dementia such as Alzheimer’s disease, and the use of such evaluations is uncommon in disease states beyond the neurology and psychiatry communities. A wide variety of neurocognitive assessments are available to examine medication effects on cognitive and non-cognitive aspects of dementia.42–45 However, these assessments are typically reserved for clinical trials monitored by regulatory agencies since they are time-consuming and not designed for routine patient monitoring. The FDA had issued a directive to the developers of PCSK9 inhibitors to investigate possible neurocognitive adverse events originally noted in the various clinical trials. 46 The neurocognitive assessments described in this review article are summarized in Table 1.
The EBBINGHAUS study was the first prospective evaluation of PCSK9 inhibitor use and cognitive function. 40 EBBINGHAUS utilized the CANTAB among patients randomized to evolocumab or placebo with statin therapy. Used in a variety of clinical trials for over 30 years, the CANTAB is a language- and culture-independent computerized test that employs digital touch screen technology. 47 The primary outcome of EBBINGHAUS was the spatial working memory index of executive function score. Secondary outcomes included the scores for working memory, episodic memory, and psychomotor speed. The CANTAB was completed at baseline, at 24 weeks, annually, and at the end of the study. The effect of evolocumab on cognition was determined by changes in the CANTAB scores from baseline to the end of the study. At the final visit, EBBINGHAUS study participants also completed a cognition self-assessment, the Everyday Cognition (ECog) scale. The 23-item version of the ECog scale assesses memory and executive function such as planning, organization, and divided attention. 48
Mefford et al. evaluated the neurocognitive impact of PCSK9 loss-of-function variants among blacks enrolled in REGARDS study. 49 The rationale is that PCSK9 loss-of-function variants cause lifelong exposure to low LDL-C levels, which could possibly affect neurocognition. Two cognitive assessments were conducted via telephone at baseline and either biannually or annually for the duration of subject enrollment in the study. The biannual Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) battery consisted of three word assessments derived from the Alzheimer’s Disease Assessment Scale-cognitive section: word list learning, world list recall, and semantic animal fluency.50,51 The annual Six-Item Screener (SIS) consisted of a three-item word test and orientation questions derived from the Folstein Mini-Mental Status Exam.52,53 Both the CERAD battery and SIS were validated in Alzheimer’s disease to differentiate subjects with neurocognitive impairment compared with age-matched normal elderly subjects.50,52 Mefford et al. noted that patterns of neurocognitive decline were similar between subjects with or without PCSK9 loss-of-function variants. 49 This finding suggests that lifelong exposure to low LDL-C levels is not associated with neurocognitive impairment among this population.
Discussion
Although PCSK9 inhibitors are generally well-tolerated, there is concern for neurocognitive adverse events based on associations among other lipid-lowering medications and cognitive impairment. The FDA directive to manufacturers to assess the neurocognitive impact of PCSK9 inhibitors possesses unique challenges. The selection of appropriate assessment tools is essential to detect any impairment. One major limitation among the included trials is the lack of formal neurocognitive assessments in each trial. The ODYSSEY trials coded adverse events using Standardized MedDRA Queries (SMQs), which are pre-determined sets of medical terminology grouped by system or condition (e.g., hypersensitivity). SMQs are designed as safety tools, not tools for diagnosis or monitoring of disease progression. The symptoms within the SMQ categories of neurocognitive disorders or central nervous system disorders may not be well-defined or consistent with clinical criteria for diagnosis of cognitive impairment.
EBBINGHAUS utilized validated cognitive assessment tools such as CANTAB and the Ecog scale. However, both instruments have inherent limitations. The CANTAB computerized assessment is a validated tool used primarily for research purposes, but it has limited utility for clinicians. CANTAB does not utilize certain tests that have been essential in determining neurocognitive changes; subjects are not asked to recall words, draw diagrams, or answer questions related to orientation. Findings with the Ecog scale may translate more easily to the bedside; however, this self-assessment data is more prone to internal bias from the subjects. Patients with possible cognitive impairments may present with less than accurate data compared with the findings from a trained observer or caregiver.
There is a paucity of prospective studies specifically evaluating PCSK9 inhibitor-associated neurocognitive adverse events. Study duration, as well as number and type of assessments administered during the designated time-period, can provide an overall portrayal of possible neurocognitive effects. Perhaps, the methodology for these studies can be derived from the clinical trials for Alzheimer’s disease. One suggestion is to combine the CANTAB, CERAD, and SIS assessments to furnish a broad spectrum of cognitive data to identify neurocognitive adverse events with high sensitivity and allow for translation to clinical practice as indicated.
Having working memory of the proposed mechanisms for PCSK9 inhibitor-associated neurocognitive effects is likely unnecessary given the actual incidence of adverse events. Among the articles included in this review, the incidence of neurocognitive adverse events with alirocumab or evolocumab use ranged from 0% to 15.4%.29,33 Most importantly, there were no significant differences in neurocognitive adverse event rates between intervention and placebo groups in these studies. Similar findings were noted in a review article by Robinson et al., who pooled data from 14 trials pertaining to alirocumab and very low LDL-C levels with subsequent use. 54 The authors concluded that LDL-C levels less than 25 mg/dl or less than 15 mg/dl in patients treated with alirocumab were not associated with an increased risk of neurocognitive events. One critique is the evaluation of calculated versus measured plasma levels, which could potentially lead to underestimated LDL-C concentrations. 55 Contrarily, a meta-analysis by Lipinski et al. reported an increased incidence of neurocognitive adverse events associated with PCSK9 inhibitors compared with placebo (OR 2.34; 95% CI 1.11–4.93; I2 = 4%; p = 0.02). 56 The authors noted that this finding was largely influenced by the ODYSSEY LONG TERM and OSLER trial results.5,37
The PCSK9 inhibitors alirocumab and evolocumab have demonstrated great efficacy in reduction of LDL-C levels and improvement of cardiovascular outcomes among patients on optimized statin therapy.4,32,37 Additionally, PCSK9 inhibitor use is associated with a decreased incidence of all-cause mortality.5,37 Though there is concern for neurocognitive adverse events based on associations among other lipid-lowering medications and cognitive impairment, and there is some evidence to support this concern; the preponderance of evidence does not support the need to monitor neurocognitive function clinically in most patients prescribed PCSK9 inhibitors. However, clinicians should be prudent in considering a patient’s overall risks for non-vascular neurocognitive impairment when PCSK9 inhibitor therapy is indicated.
This narrative review summarizes the assessments used in clinical trials to evaluate, proposed mechanisms for, and incidence of neurocognitive adverse events associated with PCSK9 inhibitor use. Limitations of this review include possible selection bias and a small number of data sources since only two databases were searched. Additionally, no measures of heterogeneity were utilized.
Conclusion
Given the reports of neurocognitive adverse events observed with prior lipid-lowering therapies, the more prominent role of PCSK9 inhibitors for prevention of cardiovascular events, and continued development of agents within this novel drug class; the findings described in this article are relevant to clinicians. PCSK9 inhibitors are indicated primarily for reduction of LDL-C levels among patients on optimized statin therapy or those who do not tolerate statins. Overall, neurocognitive adverse events associated with PCSK9 inhibitors appear to be uncommon. Additional prospective studies evaluating cognitive impairment may be beneficial, especially to determine the long-term safety of these agents.