
Abstract
Background:
Little is known about the initiation, style and content of patient and healthcare provider communication around deprescribing. We report the findings from a content analysis of audio-recorded discussions of proton pump inhibitor (PPI) and benzodiazepine deprescribing in primary care.
Methods:
Participants were healthcare providers (n = 13) from primary care practices (n = 3) and patients aged ⩾65 (n = 24) who were chronic users of PPIs or benzodiazepines. The EMPOWER educational brochures were distributed prior to (n = 15) or after (n = 9) the patient’s usual healthcare provider appointment. Conversations were audio-recorded and coded using MEDICODE to analyze who initiated different themes, whether they followed a monologue or dialogue style, and to what extent the thematic content addressed issues pertaining to: ‘dosage/instructions,’ ‘medication action and efficacy,’ ‘risk/adverse effects,’ ‘attitudes/emotions,’ ‘adherence’ and ‘follow up.’ Descriptive analysis of the conversations was performed with comparison between patients who received the EMPOWER brochure before or after their appointments.
Results:
Patients were mostly women (67%) with a mean age of 74 ± 6 years. For PPI users, prior education resulted in a greater proportion of themes initiated by patients (44% versus 17%) and maintaining dialogue-style conversations (48% versus 28%). Among benzodiazepine users, conversation initiation (52% versus 47%) and conversation style was similar between both groups. The content of deprescribing conversations for PPIs revealed that patients and their healthcare providers focused less on ‘dosage/instructions,’ and more on the ‘medication action and efficacy’ and the necessity for ‘follow up.’ Conversations about stopping benzodiazepines were more likely to stagnate on the ‘if’ rather than the ‘how.’
Conclusion:
The initiation, style and content of the conversations varied between PPI and benzodiazepine users, suggesting that healthcare providers will need to tailor deprescribing conversations accordingly.
Keywords
Introduction
Both the chronic use of proton pump inhibitors (PPIs) beyond 12 weeks and the use of benzodiazepines for insomnia in older adults have been classified as inappropriate by explicit criteria for medications to avoid in older adults.1,2 At least 1 in 4 older adults in Canada are prescribed PPIs and more than 1 in 10 are prescribed benzodiazepines each year.3,4 Although frequently prescribed, approximately 70% of older adults who consume benzodiazepines report that they have never been informed that benzodiazepines can be harmful. 5 The EMPOWER trial provided direct to patient education regarding the benefits and harms of benzodiazepines. 6 This approach improved patient knowledge, beliefs and perceptions of benzodiazepine safety, 7 resulting in 27% of community-dwelling older adults ceasing their benzodiazepines within 6 months. 6 One of the main barriers to deprescribing observed in the EMPOWER trial was discouragement from a physician or a pharmacist. 8
Deprescribing is the planned and supervised process of withdrawing a medication which may be causing harm or may no longer be providing benefit, with the goal of improving outcomes. 9 Although deprescribing may be considered an inherent component of good prescribing practice, 10 clinicians often find it difficult to propose deprescribing in clinical practice. Many barriers to deprescribing have been observed from both the clinician and patient perspective, including prescriber self-efficacy, difficulty communicating the reasons for deprescribing to patients, and patient awareness regarding the need to deprescribe.11–13
Patient–prescriber conversations about medication can be complex, with attention variably drawn to the decision to stop or start a given drug, concern about potential risks and harms, symptom alleviation and recurrence, instructions about dosing and tapering, follow up, and emotional investment.14,15 Research indicates that patients are more prone to recall medication information when a greater number of these themes are discussed during a patient–provider interaction. 16 Conversations initiated by patients and characterized as dialogue, rather than healthcare provider monologue, also improve medication information recall. 16
Shared decision-making is an important enabler for deprescribing, 17 necessitating improved deprescribing communication between prescribers and older adults. 17 Reassuringly, patient deprescribing education has been shown to promote deprescribing without damaging patient–healthcare provider trust. 18 However, the extent to which patient education qualitatively alters the dynamics between the patient and the prescriber remains unknown, especially in regard to the initiation of deprescribing conversations, whether or not the conversation style is interactive or one-sided (e.g. a dialogue or monologue) and the thematic content of the discussion. Understanding how patients and their healthcare providers communicate about medications targeted for deprescribing is an important step for defining best practices for deprescribing interventions in primary care.
Aim
To describe patterns of deprescribing conversations in terms of initiation, style, and content between patients and healthcare providers when a patient-targeted educational intervention on PPIs or benzodiazepines is delivered before or after a primary care encounter.
Methods
Study design, setting and patients
A two-arm exploratory pilot project was conducted in Québec, Canada. All healthcare providers (physicians and nurse practitioners) from three academic family medicine clinics in the greater Montréal area were invited to participate. Eligibility criteria included: (1) ability to identify patients (⩾65 years) taking ⩾1 of the targeted potentially inappropriate medications; and (2) consent to audio-record the healthcare encounter. Healthcare providers were excluded if they were away for an extended period during the data collection period.
Patients aged ⩾65 years were identified from the rosters of consenting healthcare providers according to the following criteria: (1) attending the family medicine clinic for an upcoming scheduled appointment with a participating healthcare provider, (2) having at least one active benzodiazepine or PPI prescription recorded in the electronic medical record within the previous 12 months, (3) self-reported current use of the prescribed benzodiazepine or PPI, (4) ability to speak and read in either French or English and (5) consent to audio-record the healthcare encounter. Exclusion criteria included treatment for cancer, dementia, epilepsy, active depression or other uncontrolled mental health problems (e.g. schizophrenia, bipolar disorder) based on the discretion of the healthcare provider.
Potentially eligible patients were initially contacted by the medical secretary 1 week prior to their scheduled appointment. Patients who expressed interest in participating in the study were directed to the study team who confirmed eligibility and invited patients to arrive at least 1 hour before the scheduled appointment to confirm their participation in the study and to sign the study consent form, including permission to audio-record their healthcare encounter. Patients who were unreachable after several attempts were excluded.
Study intervention
Healthcare providers were given access to a 30-minute online video that provided an overview of deprescribing tools and suggestions for how to communicate with patients on the topic of deprescribing. Additionally, they were provided with electronic and hard copies of EMPOWER patient education brochures along with evidence-based deprescribing algorithms for the targeted medication classes.19,20 A pragmatic approach was taken such that healthcare providers were emailed links, provided with hard copies of the materials and encouraged but not required to review the package before each patient’s planned appointment.
Family medicine clinics were sequentially allocated to one of two groups. In group one, patients received an EMPOWER educational brochure at least an hour prior to their encounter, ensuring they had sufficient time to read it. In the other group, patients received the educational brochure immediately after their appointment. The EMPOWER brochure was specific to either PPIs or benzodiazepines, and included information on the benefits, harms and alternatives for each medication, along with clear instructions relating to how to deprescribe. The development and testing of the EMPOWER brochures has been previously described.7,21 The patient education brochures and the evidence-based deprescribing guidelines can both be freely downloaded from www.deprescribingnetwork.ca or www.deprescribing.org.
Procedures and data collection
Baseline demographic data were collected from participating healthcare providers, including their sex, year of birth, and the number of years of experience. Patient baseline data collection included demographics (year of birth, sex), education level, and patient self-reported number of different medications taken per day including prescribed, over the counter, regular and as-required medications.
Communication analysis with MEDICODE
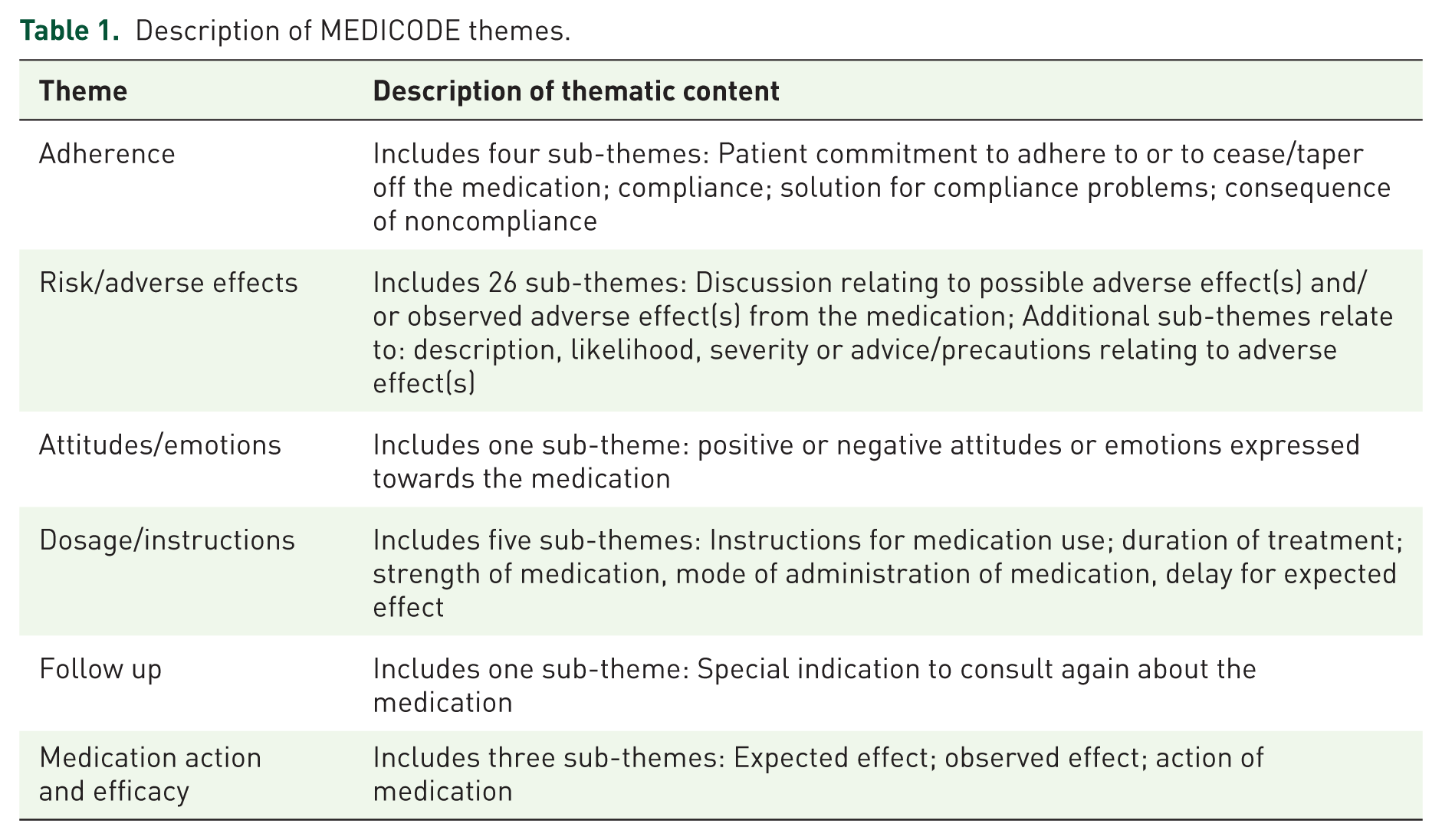
All encounters were audio-recorded, coded and analyzed using MEDICODE.14,15 MEDICODE is designed to qualitatively analyze the conversation between a patient (or caregiver) and a healthcare provider, in relation to health problems and medications. A full explanation of MEDICODE has been published previously.14,15 An experienced MEDICODE coder listened to the entire healthcare encounter, identifying sections in which any medication was discussed. The study medications were isolated and coded. A theme was ascribed to each discussion identified. Through discussion between experienced MEDICODE coders and clinician researchers with deprescribing experience, 40 of the 52 sub-themes relating to medication use were aggregated to create six overarching themes that were deemed important for deprescribing conversations: ‘dosage/instructions,’ ‘medication action and efficacy,’ ‘risk/adverse effects,’ ‘attitudes/emotions,’ ‘adherence,’ and ‘follow up’ (Table 1).
Description of MEDICODE themes.
At the first occurrence of a theme, the person who initiated the discussion (patient or healthcare provider) was coded. One-sided conversations between the patient and healthcare provider were coded as either ‘patient monologue’ or ‘healthcare provider monologue.’ Conversations in which both parties participated (e.g. discussions, or argumentative conversations) were coded as ‘dialogue.’ A 10% sample of conversations was analyzed by two experienced MEDICODE coders, with the convergence rate analyzed to ensure accuracy and consistency of coding. There was a 98% agreement for coding of conversation content, with 90% agreement for conversation initiation and style, which is comparable with previous literature. 14
Three different measures are possible with MEDICODE. The first is the proportion of themes raised by healthcare providers or patients. The second is the style of themes discussed, presented as a proportion of patient monologue, healthcare provider monologue, or dialogue. The third is the proportion of encounters in which a theme is discussed. Results were disaggregated by whether the patient received education prior to or after their appointment.
Ethics
The Research Ethics Board of the Dépendances, Inégalités sociales et Santé publique of the Centre Intégré Universitaire de Santé et des Services Sociaux du Centre-Sud-de-l’île-de-Montréal, Canada, approved the study protocol on 6 October 2015. Informed consent was obtained from healthcare providers and patients.
Results
A total of 13 healthcare providers with a mean age of 44 years (range 31–61) participated in the study. Approximately two-thirds were women (n = 7), and the majority had been practicing for more than 10 years (n = 6). An average of two patients per physician were enrolled in the study (range 0–5).
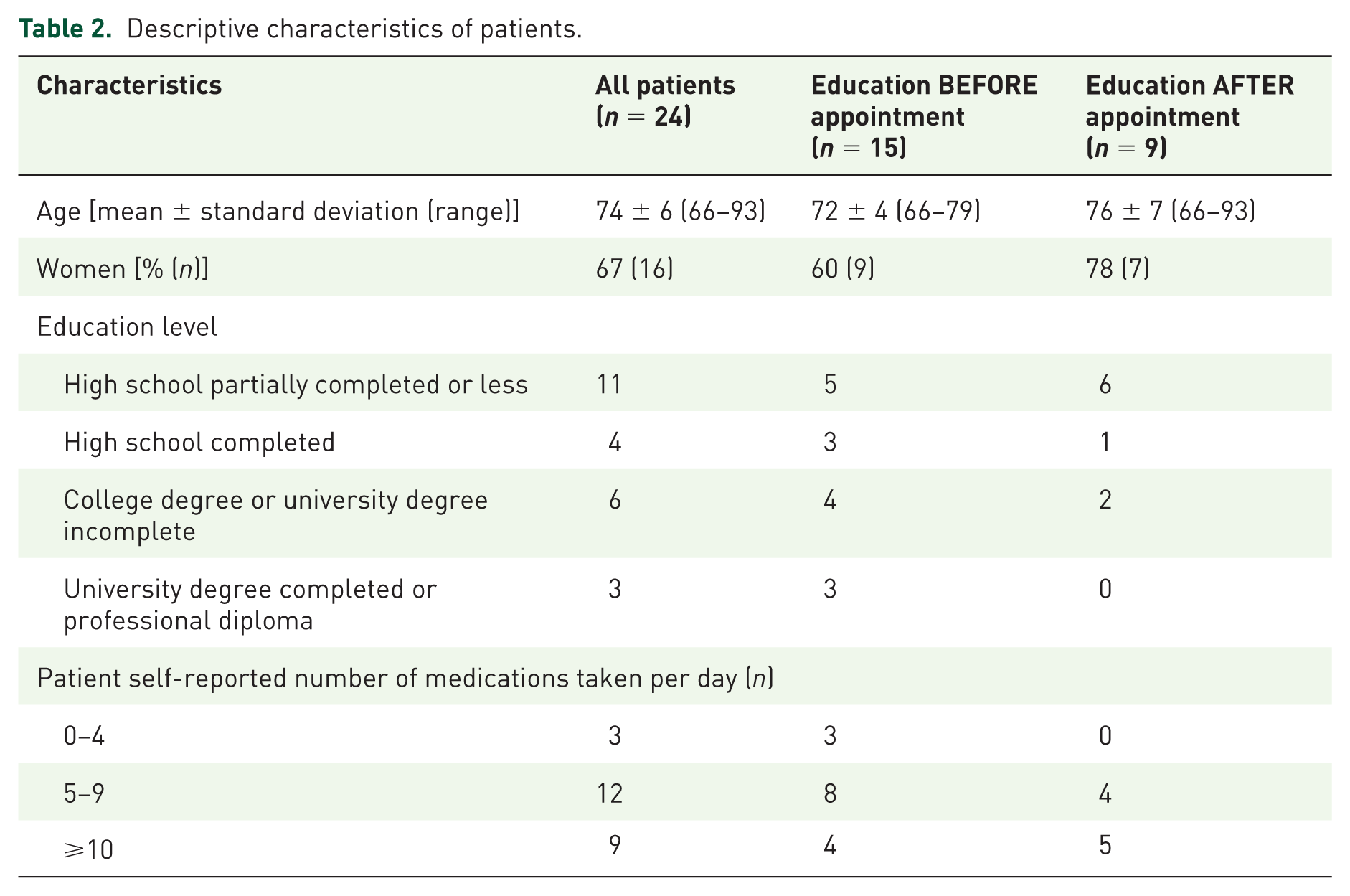
During the study timeframe, 117 patients were assessed for eligibility, with 24 providing consent to participate. Reasons for nonparticipation included: inability to reach the patient prior to the healthcare appointment (n = 48), patient refusal to participate (n = 27), not meeting inclusion criteria (n = 14) rescheduling of the healthcare appointment (n = 2), or tapering had already been initiated (n = 2). Mean patient age was 74 years (range 66–93) and two-thirds of patients were female (Table 2). The majority of patients took more than five medications per day (n = 21).
Descriptive characteristics of patients.
Of the 24 patients, 4 were taking both PPIs and benzodiazepines, thus accounting for 28 conversations about the target medications. Of the 24 patients, 15 patients received the educational brochure prior to their appointment (n = 9 received a PPI brochure, n = 4 received a benzodiazepine brochure, n = 2 received both) and 9 received the education afterwards (n = 6 received a PPI brochure, n = 1 received a benzodiazepine brochure, n = 2 received both). However, one of the patients who received education relating to PPIs after the healthcare provider appointment did not discuss PPIs during the appointment, therefore, a total of 27 conversations about the target medications were available for analysis.
Initiation of MEDICODE themes
For PPI users, a greater proportion of conversation themes were initiated by patients when they received prior PPI education compared with those who did not (44% versus 17%; Table 3). The most frequent themes initiated by patients who received prior education about PPI discontinuation were: ‘dosage/instructions,’ ‘adherence,’ and ‘medication action and efficacy.’ Healthcare providers were more likely to initiate conversations relating to the themes ‘risk/adverse effects,’ ‘attitudes/emotions,’ and ‘follow up’ particularly when patients had not received prior education.
Initiation of conversations regarding PPIs and benzodiazepines by MEDICODE theme.
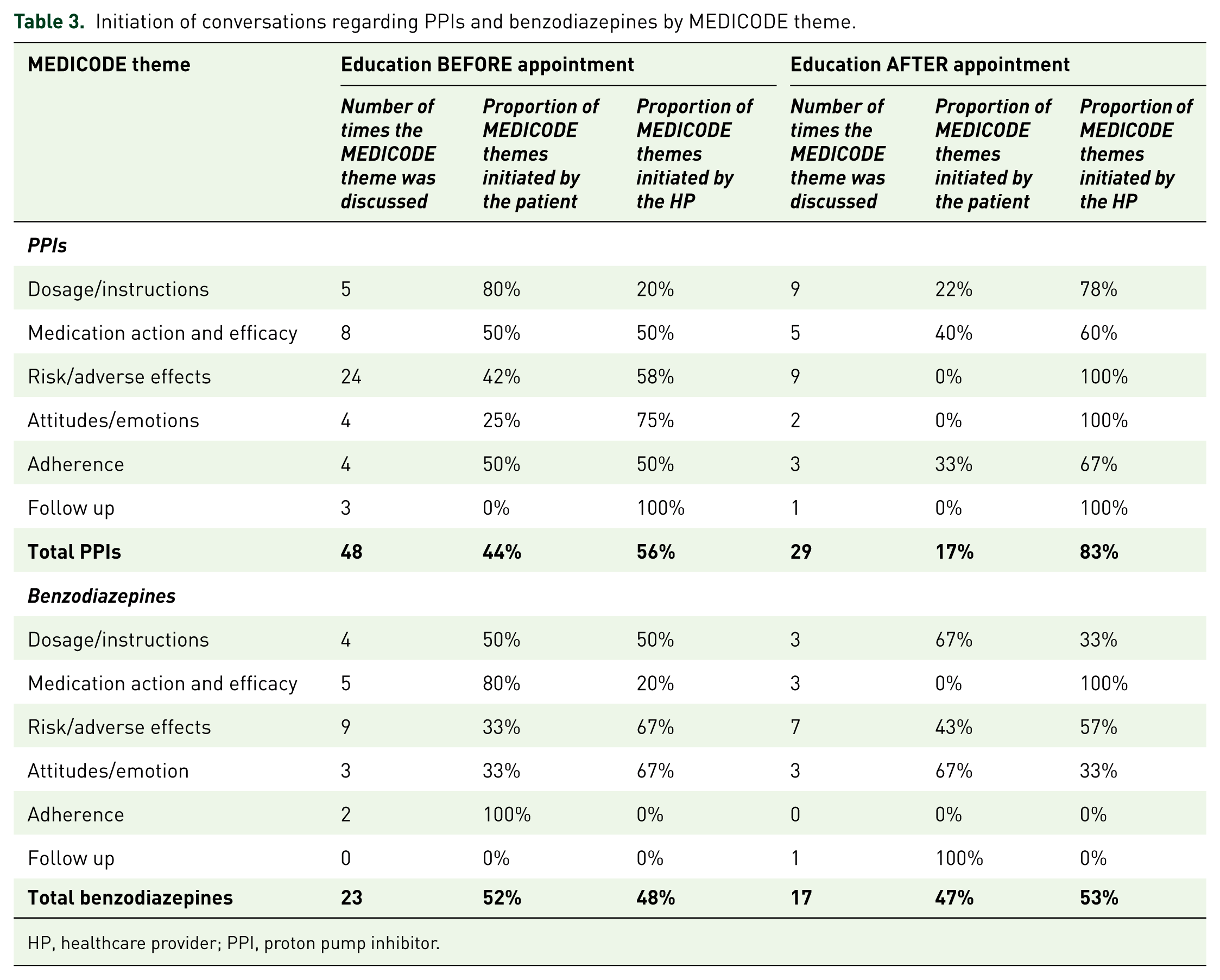
HP, healthcare provider; PPI, proton pump inhibitor.
This pattern was not replicated among benzodiazepine users, with Table 3 highlighting that the frequency of themes initiated by patients was similar between those who received prior benzodiazepine education compared with those who did not (52% versus 47%). However, unlike those who did not receive prior education, the themes initiated by patients with prior education pertained mainly to the themes ‘adherence’ and ‘medication action and efficacy’
Style of conversations
The pattern of monologue and dialogue styles of conversation differed according to medication class, and whether patients received prior education or not.
For the PPI prior education group, 48% of the conversations were dialogue style (Table 4). This contrasted with patients who did not receive prior PPI education where 62% of conversations were healthcare provider monologues. For the benzodiazepine group, there was little difference in the style of conversations between people who did and did not receive prior education (Table 4).
Conversation style for PPIs and benzodiazepines by MEDICODE theme.
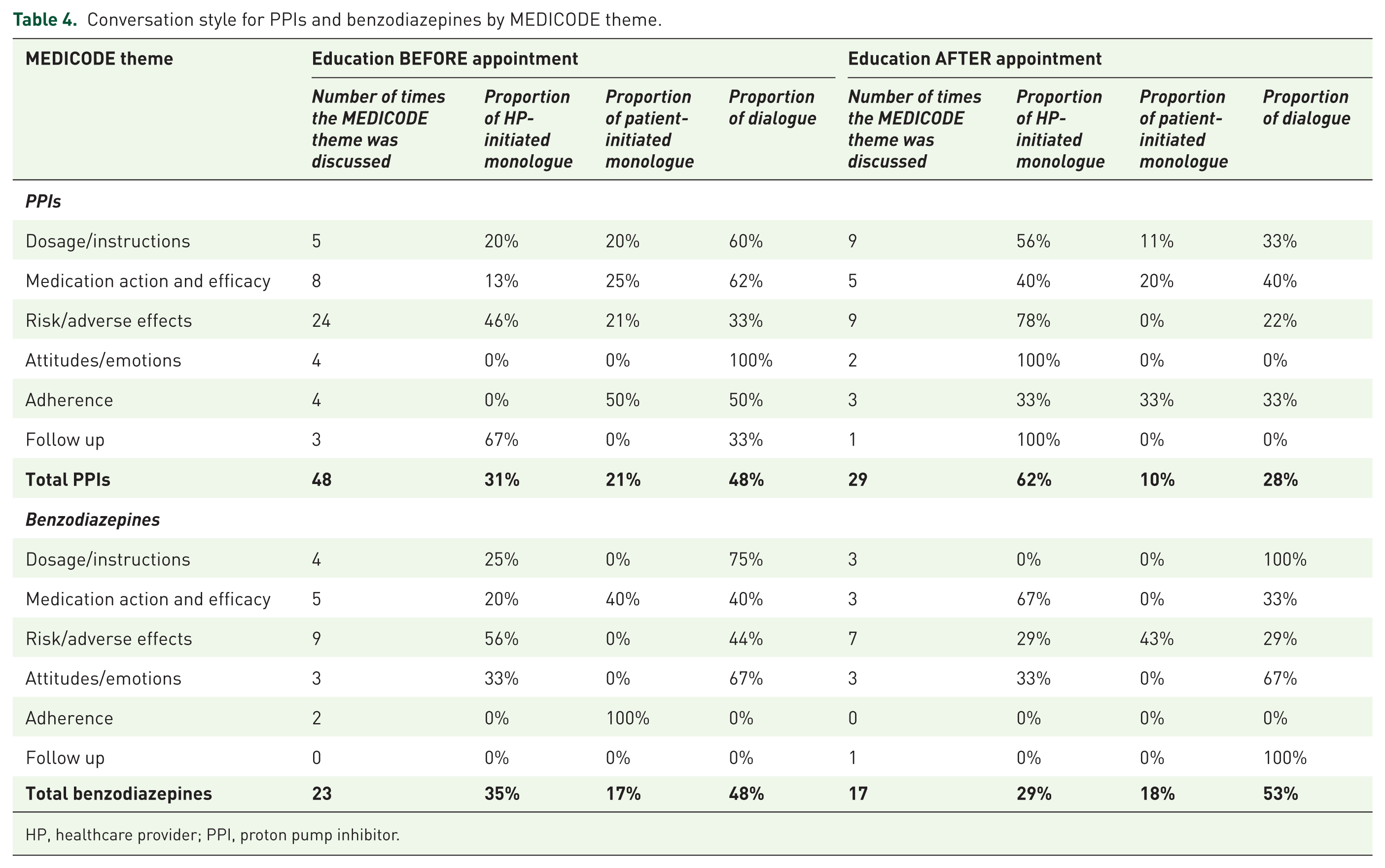
HP, healthcare provider; PPI, proton pump inhibitor.
Content of conversations
Deprescribing conversations included an average of three main themes per medication in all groups. Conversations with patients who received education after the appointment were characterized by a wide variation in frequency in which different themes were discussed for both medication classes (Figures 1 and 2). Conversely, for both medication classes there was a narrower variation in frequency for which the same themes were discussed by patients when they received prior education.
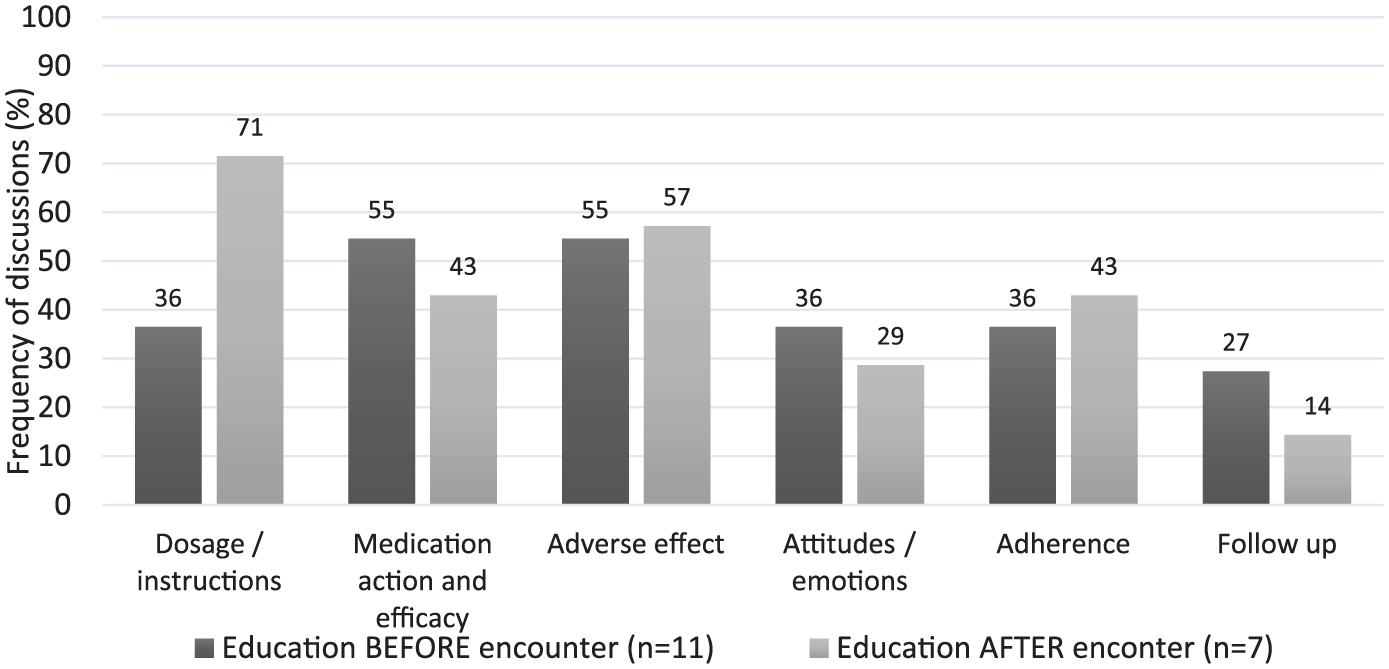
Frequency of MEDICODE themes for proton pump inhibitors per encounter.
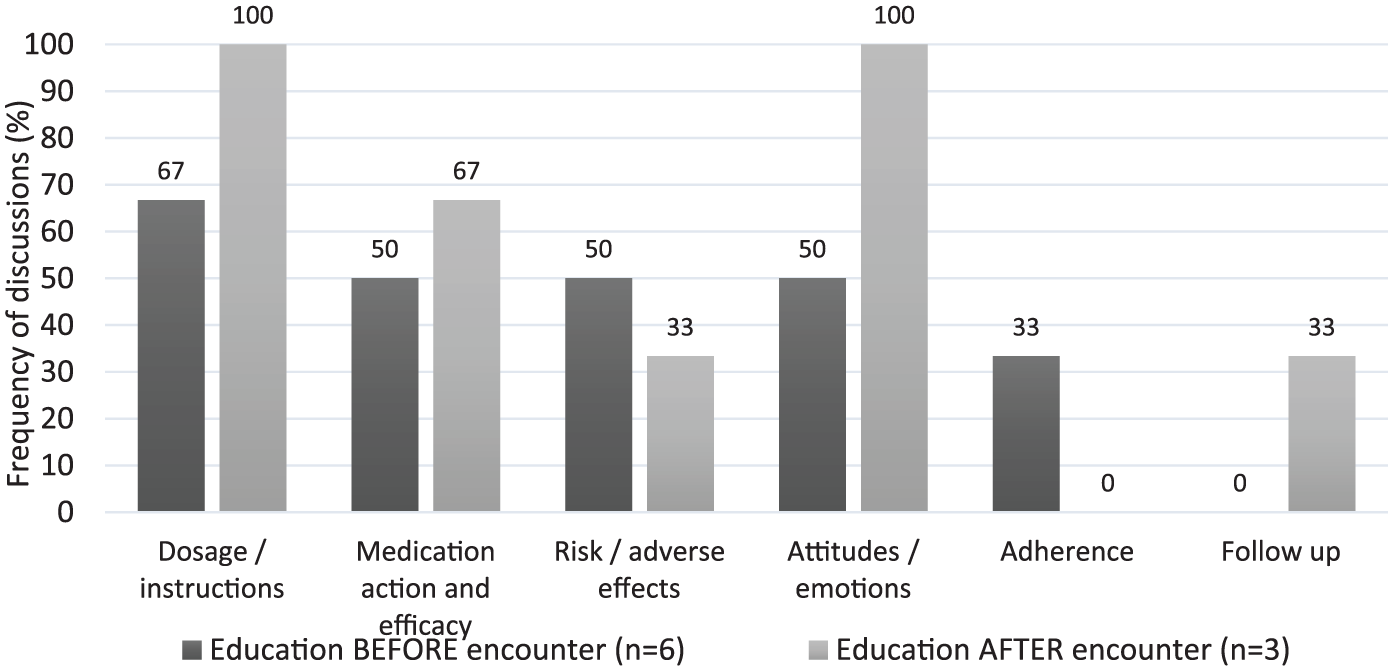
Frequency of MEDICODE themes for benzodiazepines per encounter.
Themes related to ‘dosage/instructions’ arose less frequently when patients received prior education in contrast with those who did not for both medication classes. Examination of the verbatim revealed that conversations focused on the logistics of ‘how to deprescribe’ for PPIs (e.g. conversation #24, Table 5), while conversations for benzodiazepines focused more on ‘if I should deprescribe’ (e.g. conversation #4, & #5, Table 6).
Examples of patient and healthcare provider conversations according to MEDICODE themes for PPIs.
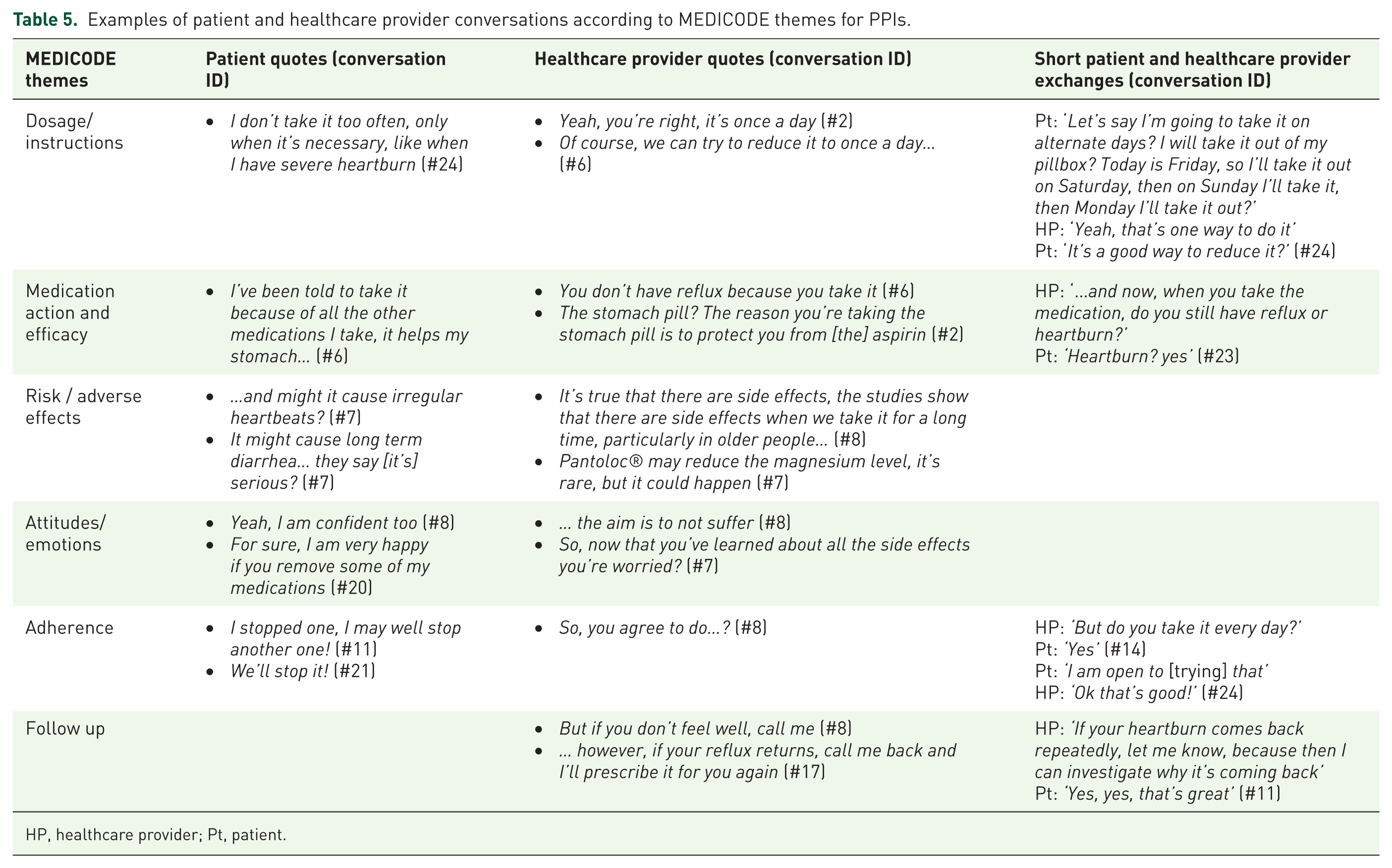
HP, healthcare provider; Pt, patient.
Examples of patient and healthcare provider conversations according to MEDICODE themes for benzodiazepines.
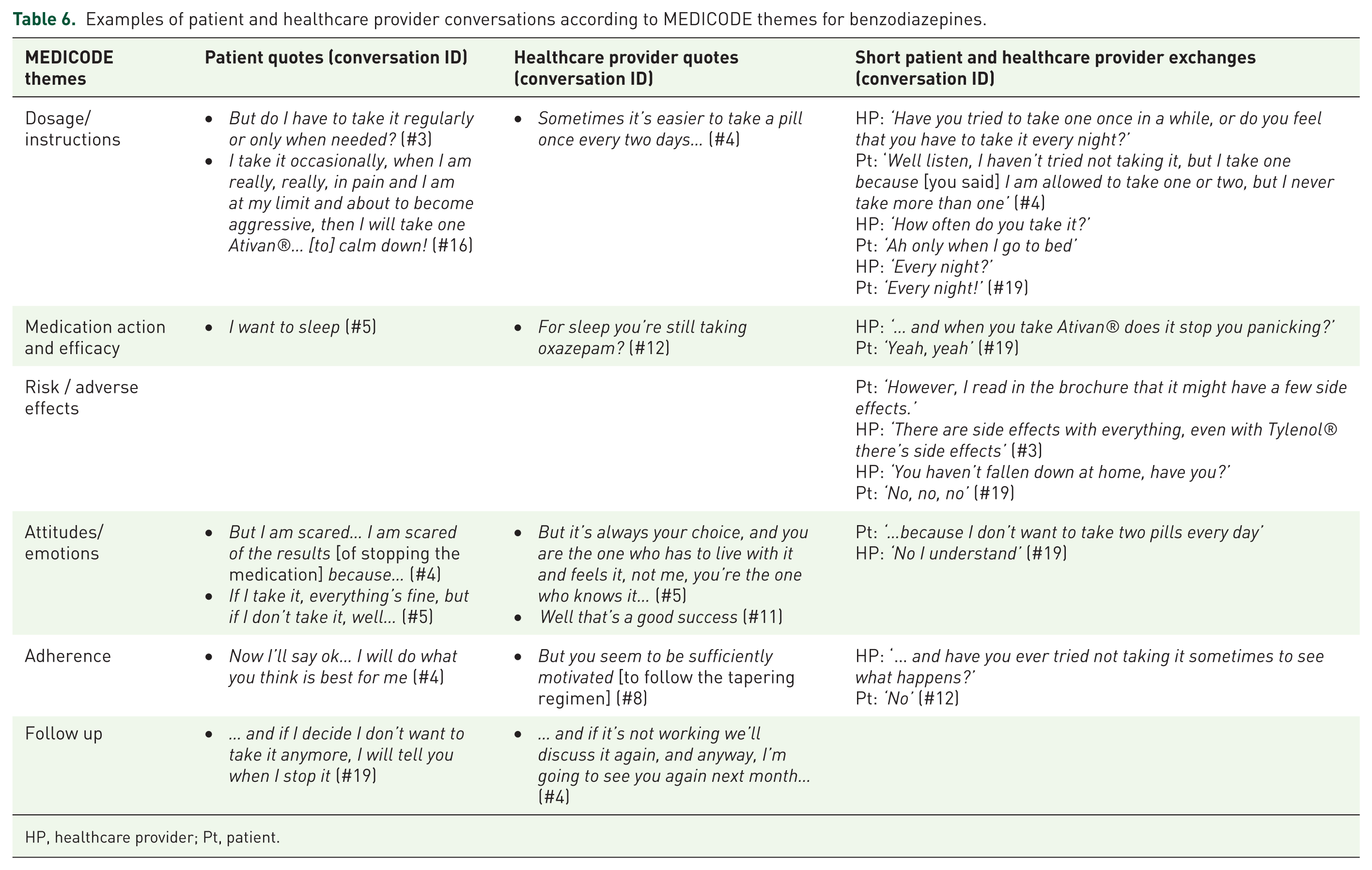
HP, healthcare provider; Pt, patient.
The theme ‘follow up’ was more prevalent and driven by healthcare providers when patients received prior education on PPIs (e.g. conversation #11, Table 5). Conversations with patients who received prior education about benzodiazepines, were more likely to address adverse effects (e.g. conversation #3, Table 6) and adherence (e.g. conversation #4, #8 & #12, Table 6).
Of note, the ‘attitudes/emotions’ theme was discussed more frequently in the prior PPI education group (e.g. conversation #7, Table 5) than in the after-education group. We observed a lower frequency of discussion of this theme in the benzodiazepine prior education group than in the after-education group.
Discussion
The initiation, style and thematic content of the conversations varied between patients who did and did not receive prior education. PPI users who received prior education had a higher frequency of patient-initiated deprescribing themes than those who did not, a pattern which was not replicated among benzodiazepine users. Dialogue-style conversations occurred more frequently for PPI users who received prior education, but no difference was observed in the benzodiazepine group. An average of three themes was discussed in each group, with patients who did not receive prior education frequently discussing ‘dosage/instructions.’ Conversations focused on the logistics of ‘how to deprescribe’ for PPI users, while conversations for benzodiazepine users focused more on ‘if I should deprescribe.’
The higher proportion of patient participation, as evidenced by patient initiation of themes and dialogue-style conversations suggested that the ‘patient voice’ was heard more frequently when patients received prior PPI education in comparison with those who did not. Additionally, there was a higher frequency of discussions of ‘medication action and efficacy’ and ‘attitudes/emotions.’ The pattern of conversations observed with prior PPI education is in line with literature on shared decision-making which highlights that the first step is the provision of information.17,22 Shared decision-making requires a discussion between the patient and healthcare provider that explores all relevant options, the benefits and harms of each option, and how the options relate to the patients’ goals of treatment. 17 However, we observed that the initiation, style and thematic content of conversations varied between PPI and benzodiazepine users, suggesting that physicians may need to vary their shared decision-making approach to deprescribing for different medication classes.
The theme ‘dosage/instructions’ was discussed less often when patients received prior education compared with those who did not. Although it may appear counterintuitive, this observation is in agreement with Grice’s Maxim of quantity (where one tries to be as informative as one possibly can, and give as much information as is needed, and no more). 23 Thus, in the limited time available in a family medicine encounter, patients do not ask for information that they have just learned from the educational brochure, and prescribers do not repeat the information that they know the patient has just read.
Patients who received prior PPI education appeared less concerned about ‘dosage/instructions’ and more concerned about ‘medication action and efficacy.’ This may reflect a re-evaluation of the benefits and harms of chronic PPI use as a result of the education. The focus on the ‘medication action and efficacy’ reflects the difficulty that healthcare providers can have identifying the indication for PPIs. This observation is well documented, with up to 80% of people prescribed PPIs not having a documented indication. 24 More discussions involving ‘attitudes/emotions’ occurred in the prior PPI education group, which was mainly physician initiated dialogue, possibly reflecting concerns about withdrawal symptoms. As hyperacidity occurs in over 40% of patients when chronic PPI use is abruptly stopped, this observation was expected. 25 Similarly, physicians were more likely to initiate discussion relating to the need to ‘follow up’ and re-evaluate symptoms. Providing patients with clear tapering and follow-up instructions can improve the success of deprescribing interventions. 26
Benzodiazepine deprescribing conversations in both groups appeared to focus on ‘if I should deprescribe’ rather than ‘how to deprescribe,’ as observed by the frequency of discussions on ‘dosage/instructions,’ ‘attitudes/emotions’ and ‘risk/adverse effects.’ Conversations about ‘medication action and efficacy’ were more frequently initiated by patients who received prior benzodiazepine education compared with those who did not. This may reflect patients’ desire to discuss the balance between the perceived benefits and harms of benzodiazepines. With 70% of older benzodiazepine users reporting that they had never been told about the adverse effects of benzodiazepines, 5 providing this information prior to the medical encounter is likely to cause cognitive dissonance. 21 The observed variation in frequency of themes and patient initiation may explain how increased concern and increased perception of risk on the patient’s behalf leads to more productive conversations and eventually to successful deprescribing. 8
This exploratory study provides insight into how educational interventions may change patient and healthcare provider deprescribing conversations. The inclusion criteria for the study were broad, thus increasing the generalizability of the results. However, our study has several limitations. First, the sample size was small, and did not permit statistical comparisons between groups. Second, while all healthcare providers in the family medicine clinic were invited, the possibility of recruitment bias due to the limited number of family medicine clinics involved with the study cannot be ruled out. Third, it was not possible to determine if physicians interacted with the education materials during the study and, therefore, it remains unknown if this had an impact on their conversations. Fourth, information relating to past experiences in deprescribing either benzodiazepines or PPIs was not collected from either patients or healthcare providers. It is possible that previous experiences with deprescribing (either successful or unsuccessful) may influence the approach to initiation, style and content of deprescribing conversations, and thus may have affected the results observed in this study. Finally, as there was no longitudinal follow up, deprescribing outcomes related to education in this study remain unknown.
Conclusion
Initiation, style and thematic content of deprescribing conversations between patients and primary care healthcare providers varied between groups of patients who received a written educational brochure prior to their healthcare provider appointment and those who did not. Patients receiving prior PPI education initiated themes more frequently, and a higher proportion of dialogue (as opposed to monologue) was observed. Different themes were discussed among PPI and benzodiazepine users, suggesting that primary care healthcare providers may need to tailor deprescribing conversations according to different medication classes.
Footnotes
Acknowledgements
The authors would like to thank the healthcare providers and patients who participated in this study, along with the staff at each of the three family medicine clinics, for without their collaboration, this research could not have been conducted.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a Partnership for Health System Improvement Grant from the Canadian Institutes of Health Research (201410PHE-PHE- 337814–96399) and a National Chair Award from the Fonds de Recherche de Santé du Québec (2016/2017–33087).
Conflict of interest statement
The authors declare that there is no conflict of interest.