
Abstract
It is known that for all adults, prevalence of potentially inappropriate prescribing (PIP) and polypharmacy increases with advancing age and morbidity. This has been associated with adverse drug reactions and poor outcomes. As a result, screening tools have been developed to identify PIP and to improve prescribing and health outcomes.
A growing body of evidence supports the fact that there are even greater concerns among older adults with intellectual disability (ID) who are living longer than before but still have premature mortality and poorer health outcomes compared with the general population. They have different patterns of multimorbidity, with higher rates of epilepsy and mental health conditions. Polypharmacy is prevalent and some prescribing practices may be inappropriate. High exposure to anticholinergic and sedative medicines has additional adverse effects on quality of life. There may also be underutilization of clinically needed therapies. There has been substantial controversy internationally relating to extensive use of psychotropic medicines, particularly off-label use for challenging behaviours.
Despite the mounting evidence and concerns about the impact of PIP on quality of life, health and safety for people with ID, appropriate methods to measure PIP are lacking, which represents an important gap in the research literature. Differences in morbidity and medicines use patterns in this population mean instruments used to identify inappropriate medicines in the older population are not suitable. In this perspective article we outline the specific health and medicinal needs for people with ID, the prevalence of polypharmacy and presentation of chronic health conditions in older adults with ID. We provide an overview of the psychotropic medicine classes most frequently used in people with ID which carry substantial risk. We highlight studies to date that have attempted to assess PIP and present research priorities to improve prescribing, health outcomes and quality of life for people with ID.
Keywords
Outline
It is known that for all adults, prevalence of potentially inappropriate prescribing (PIP) and polypharmacy increases with advancing age and morbidity. This has been associated with increased risk of adverse drug reactions (ADRs) and poor outcomes. As a result, screening tools have been developed to identify PIP and to improve prescribing and health outcomes.1,2
A growing body of evidence supports the fact that there are even greater concerns among older adults with intellectual disability (ID) who are living longer than previously but still have premature mortality and poorer health outcomes compared with the general population. 3 They have different patterns of multimorbidity, in particular much higher rates of epilepsy and mental health conditions.4,5 Polypharmacy is prevalent and some prescribing practices may be inappropriate.6,7 High exposure to anticholinergic and sedative medicines has additional adverse effects on quality of life. 8 There may also be underutilization of clinically needed therapies. 9 There has been substantial controversy internationally relating to extensive use of psychotropic medicines, particularly off-label use for challenging behaviours.6,10
Despite the mounting evidence and concerns about the impact of PIP on quality of life, health and safety for people with ID, appropriate methods to screen for and measure PIP are lacking, 11 which represents an important gap in the research literature. Differences in morbidity and medicine use patterns in this population mean instruments used to identify inappropriate medicines in the older population are not suitable. In this perspective article we outline the specific health and medicinal needs for people with ID, the prevalence of polypharmacy and presentation of chronic health conditions in older adults with ID. We provide an overview of the psychotropic medicine classes most frequently used in people with ID, which carry substantial risk [e.g. antipsychotics, anticholinergics, antiepileptics (AEDs), polypharmacy]. We highlight studies to date that have attempted to assess PIP and present research priorities to improve prescribing, health outcomes and quality of life for this vulnerable patient group.
Introduction
With the growing number of older adults and increases in age-related chronic disease, multiple medicines use has increased and polypharmacy is commonplace.12,13 Medications play a critical role in maintaining health and so management of chronic conditions with polypharmacy is increasingly recommended, and in some circumstances may be therapeutically beneficial. Polypharmacy is generally understood to refer to the concurrent use of multiple medicines in one individual. 14 Polypharmacy is an important risk factor for PIP. 15 PIP in older adults occurs when medicines prescribed have no clear evidence-based indication, carry a substantially higher risk of adverse side effects compared with use in younger people, and are not cost effective. 16 PIP encompasses a set of prescribing practices which include overprescribing, misprescribing and underprescribing. 17 There is evidence of more prescribing errors and a higher prevalence of adverse drug reactions (ADRs) with the increasing number of drugs prescribed.18,19 In the general population, falls, increased risk of mortality, and associated impaired physical and cognitive function have been associated with PIP.13,14 The relationship between polypharmacy, multimorbidity and PIP has received increasing attention in the general older population.14,15 A number of prescribing criteria have been developed to assess PIP in older adults 1 and there is an increasing focus on deprescribing as a means of reducing PIP. 20
People with ID comprise 1–3% of the population. ID is ‘a disability characterized by significant limitations in both intellectual functioning and adaptive behaviour, which covers many everyday social and practical skills’. 21 ID is the preferred term for a condition also referred to as developmental disabilities in the USA and Canada, and learning disability in the UK. 22 There are variations in both intellectual and adaptive functioning among people with ID, and hence their capacity to live and function independently varies. 23 There are various aetiologies of ID, including genetic (X-linked, other chromosomal), metabolic, teratogenic (congenital infections, chemical agents), central nervous system (CNS) defects, other birth defects, neonatal, perinatal, causes that are multifactorial, and causes which are unknown. 24
Despite increases in life expectancy in people with ID, there are striking disparities compared with the general population. The Confidential Enquiry of Premature Deaths of People with Intellectual Disabilities (2013) in the UK, suggests that, on average, men with ID die 13 years earlier compared with the population in England and Wales, and on average, women die 20 years earlier. 25 This enquiry concluded that many of these deaths may be avoidable.
It has been estimated that people with ID have up to 2.5 times more health problems compared with the general population, and different patterns of morbidity.26–28 Furthermore, health needs for people with ID are often unmet and unrecognized, meaning poorer health status may often be avoidable.22,29
A concern has emerged in Ireland and in other developed countries, as deinstitutionalization and community integration for people with ID are taking or place. Greater use of primary rather than specialized care in the community raises challenges as there may not be specialist knowledge of the unique health, prescribing and medicine use issues for people with ID among general practitioners, pharmacists and nurses. 30
Although not a formal systematic review, a rigorous approach was undertaken, including an electronic search of PubMed, Medline, Embase, Science Direct and Cochrane database of systematic reviews to identify relevant studies examining polypharmacy, psychotropic medicine use and PIP in adults with ID between 1998 and February 2018. Search terms used for each database included ‘intellectual disabilities’, ‘multimorbidity’, ‘older adults’, ‘psychotropic medicines’, ‘antiepileptic drugs’, ‘antipsychotics’, ‘anticholinergics’, ‘antiepileptics’, ‘potentially inappropriate prescribing’, ‘polypharmacy’. We then screened the references of initial identified articles to find further relevant material (snowball approach). Websites relating to policy matters on ID were also screened to identify further relevant articles. In addition, we examined relevant prescribing guidelines and commentary papers available for adults with ID and personal archives as referenced throughout. Only articles written in English language were reviewed.
In this article we outline the specific health and medicine related issues for people with ID, provide perspectives on studies to date that have assessed the prevalence of polypharmacy in older adults with ID, medicines most frequently used in people with ID which carry risk, studies that have attempted to assess PIP (giving consideration to how appropriateness is assessed), and present research and practice priorities to improve prescribing, health outcomes and quality of life for this vulnerable patient group.
Chronic health conditions in people with ID
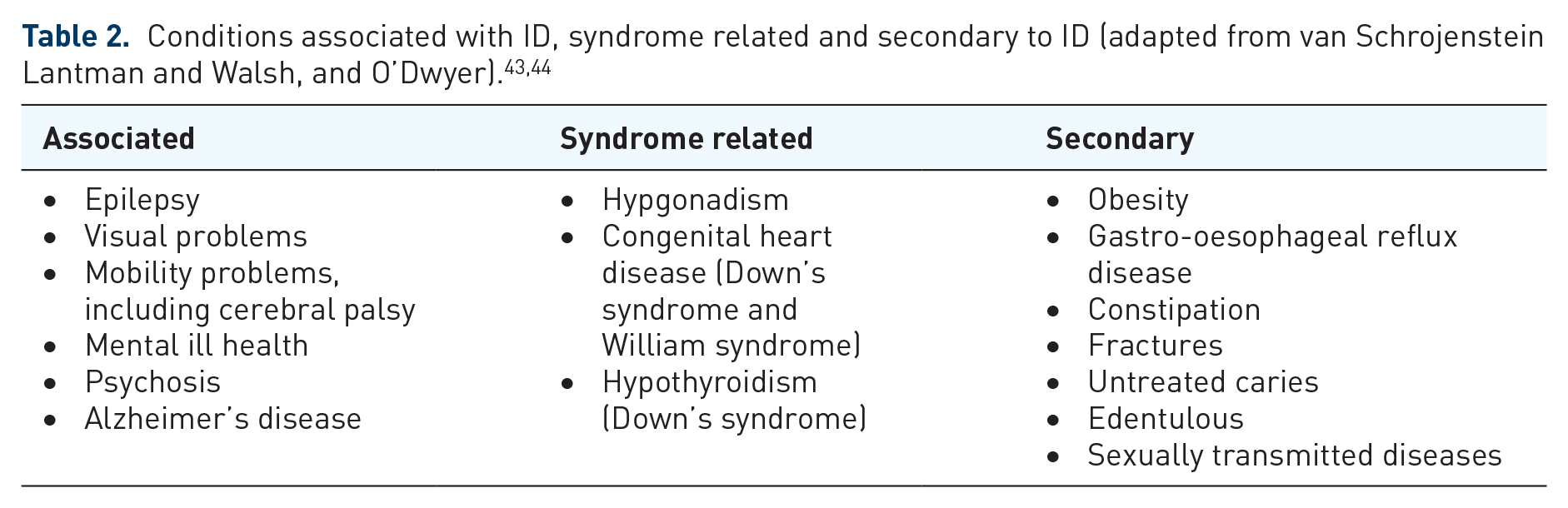
Poor health status in the ID population is multifactorial, and risks include genetic predisposition to certain diseases, social determinants such as less favourable circumstances and discrimination experienced by people with ID, residential circumstances that may promote unhealthy lifestyle choices, and inactivity. 31 People with ID experience a different pattern of chronic diseases, with higher prevalence of mental health and neurological conditions,4,32 and higher rates of multimorbidity (two or more chronic conditions) compared with the general population. In a representative cross-sectional study of 753 adults with ID aged over 40 years in Ireland, 71.2% had multimorbidity. 4 In a cohort study in the Netherlands of 1047 older adults with ID who received paid support, 80% had multimorbidity. 32 A recent population-based cross-sectional study in Scotland of 1023 adults over 16 years of age found that after a comprehensive health assessment, 98.7% had multimorbidity. 33 This is compared with an estimate of 23.2% multimorbidity in the general population in Scotland. 34 In adults with ID, health conditions may be classified as related to the ID (such as epilepsy or mobility problems), as syndrome related (such as hypothyroidism in people with Down’s syndrome), or as secondary health conditions (such as obesity) 35 (Table 2).
People with ID may be poor reporters of their own health and in most cases the history of the present illness must be determined from caregivers or family members rather than the patient. In general, accuracy of diagnosis becomes increasingly challenging and complex as severity of the disability and communication impairments increase. 36 Diagnostic overshadowing occurs when an emotional or behavioural problem is misattributed to the ID itself, rather than a comorbid condition. 37
Medication use challenges in people with ID
The principal medical and pharmaceutical care needs of people with ID are no different from those of the general population. However, there are some unique pharmaceutical care challenges in providing appropriate pharmacotherapy to people with ID (Table 1).
Issues associated with medicine use in people with intellectual disability (ID).
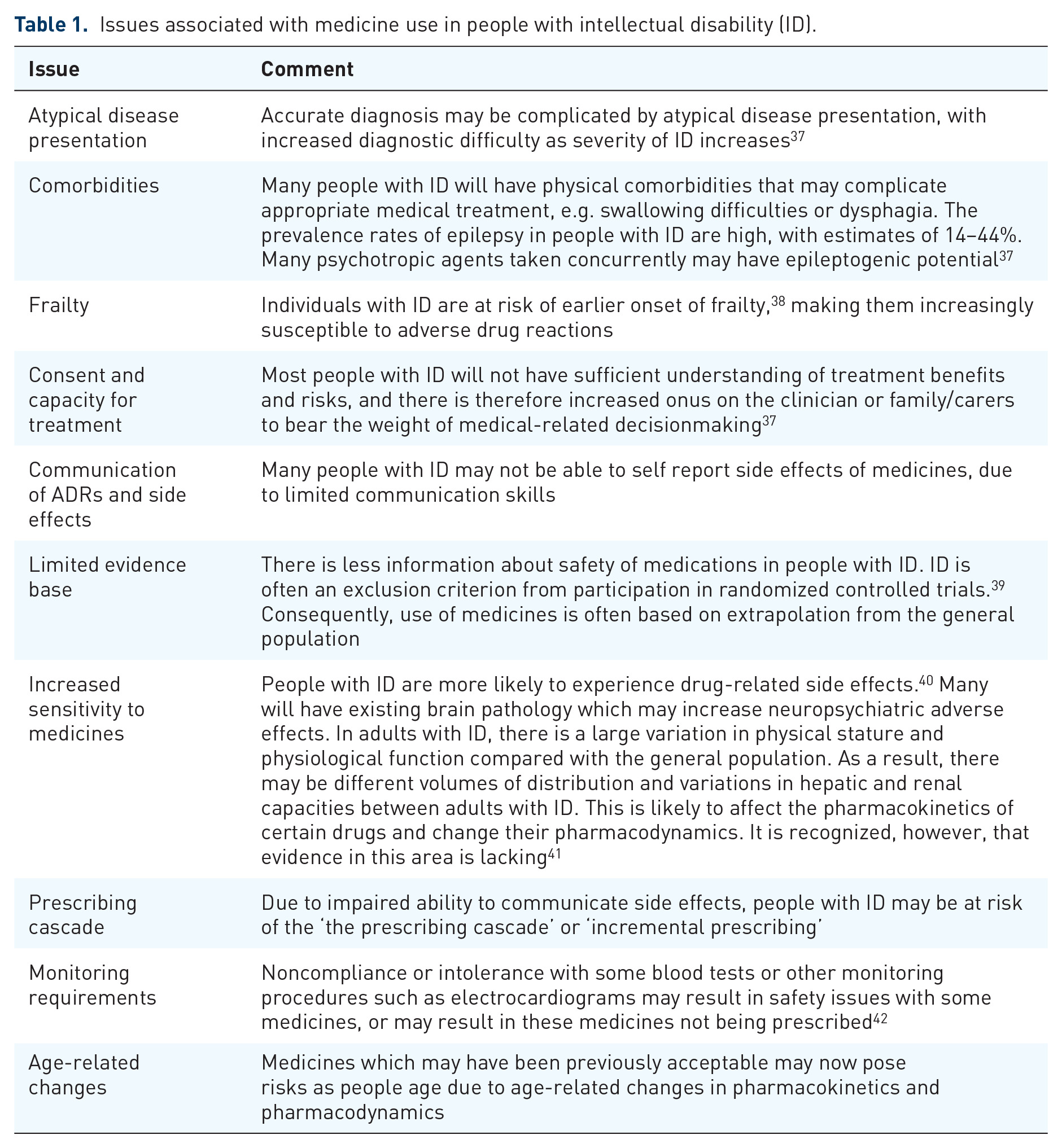
The risk of harm and complexity of polypharmacy are compounded by age-related risk of adverse effects and the presence of organic dysfunction associated with the ID, which may lead to idiosyncratic responses to drugs. Organic brain dysfunction has been recognized to potentially result in unpredictable response to psychotropic medicines in adults with ID. 45 For many adults with ID, the cause of the disability may be due to brain damage. The nature of the brain damage or changes to brain structure may result in altered sensitivity or response to medicines and challenges with determining appropriate doses. 41 The way a drug is processed by the body (its pharmacokinetics, i.e. its absorption, distribution, metabolism and excretion) may be different in adults with ID. This may be due to differences in physical stature and other parameters which may result in changes in volumes of distribution, alterations in electrolytes and differences in renal and hepatic capacity. As a result, there may be variations in drug response compared with the general population.
Swallowing difficulties, poor dental health and tooth loss may lead to people with ID being unable to swallow tablets. 46 Older adults with ID are more likely to be frail at a younger age, which may increase sensitivity to some medicines. In a cross-sectional study in the Netherlands of 982 adults over 50 years of age with ID, participants had frailty scores similar to adults in the general population over 75 years of age. 47 It is likely that age-related and attenuated physiological changes which manifest in frail adults will affect the pharmacokinetics and pharmacodynamics of medicines. Frail older adults may be more susceptible to adverse effects associated with medicines due to the loss of physiological reserve, increase in multimorbidity and polypharmacy. 48 People with ID are also at risk of experiencing the ‘prescribing cascade’. This is a phenomenon in which the side effects of drugs are misdiagnosed as symptoms of another problem, resulting in further medications being prescribed, and further risk of side effects and interactions. 49
Polypharmacy and the burden and risk of medicines
The population with ID have been identified as being among ‘the most medicated groups in society’, with rates of prescriptions and polypharmacy exceeding those of the general population.28,50,51 Polypharmacy and PIP in older adults with ID raise a number of challenges: difficulties with consent to treatments, a poor evidence base [having an ID is an exclusion criterion for many pharmacological randomized controlled trials (RCTs)], difficulties in communication of symptoms and ADRs, and increased sensitivity and adverse medicine effects resulting from the presence of organic dysfunction associated with the ID 52 (Table 1). There are a number of methodological issues relating to studies of polypharmacy carried out to date in the ID population. Many studies that have reported the prevalence of polypharmacy in people with ID have focused on specific drug classes or therapeutic areas such as AED polytherapy53,54 and psychotropic polypharmacy55–57 in isolation, as opposed to broader definitions of polypharmacy employed in the older population. In addition, comparisons are further limited by the fact that many ID studies may have had small sample sizes, convenience or clinic samples,58,59 and often only included those living in institutional settings. Older people (particularly over 65 years) are rarely studied. Given that older adults with ID commonly experience multimorbidity and polypharmacy, studies examining the total medication burden are important.
A cross-sectional study of 897 community-dwelling people with ID in the state of Victoria, Australia who had used health services, were aged from 18 to 82 years (over 90% were under 60), and had all levels of ID, reported that over 20% used five to nine medicines 60 (Table 3). Polypharmacy was examined among 52,404 adults aged 18–64 years with developmental disabilities in Ontario, Canada receiving primary care services and support from the Ontario Disability Support Group, who were dispensed medications covered by the Ontario Drug Benefit Program. 61 In this study, 42.1% of those aged 55–64 years had polypharmacy (at least five medicines), and 3% were taking 11 or more medicines. Both of these studies selected their cohorts from patients who used health services, which may mean that those not taking medicines or without chronic conditions would be under represented or absent.60,61 Polypharmacy was identified as a significant factor associated with prescription errors in a study of 600 older adults with ID (over 50 years) who reported medicines randomly selected from the Healthy Ageing Intellectual Disabilities Study (HA-ID) in the Netherlands. 7 This study included participants from independent and residential settings, with most prescription errors detected relating to drugs acting on the CNS (43.2%). In a national survey of general practice differences among 712 individuals with ID and controls (patients with no ID who were matched on age and sex) in the Netherlands, those with ID received four times more repeat prescriptions compared with adults with no ID. 28 A cross-sectional study of 736 older adults with ID in Ireland found that 21% took ten or more medicines (excessive polypharmacy) on a regular basis and 35% took five to nine medicines. 9
Key studies examining multiple medicines used in populations with intellectual disability (ID).
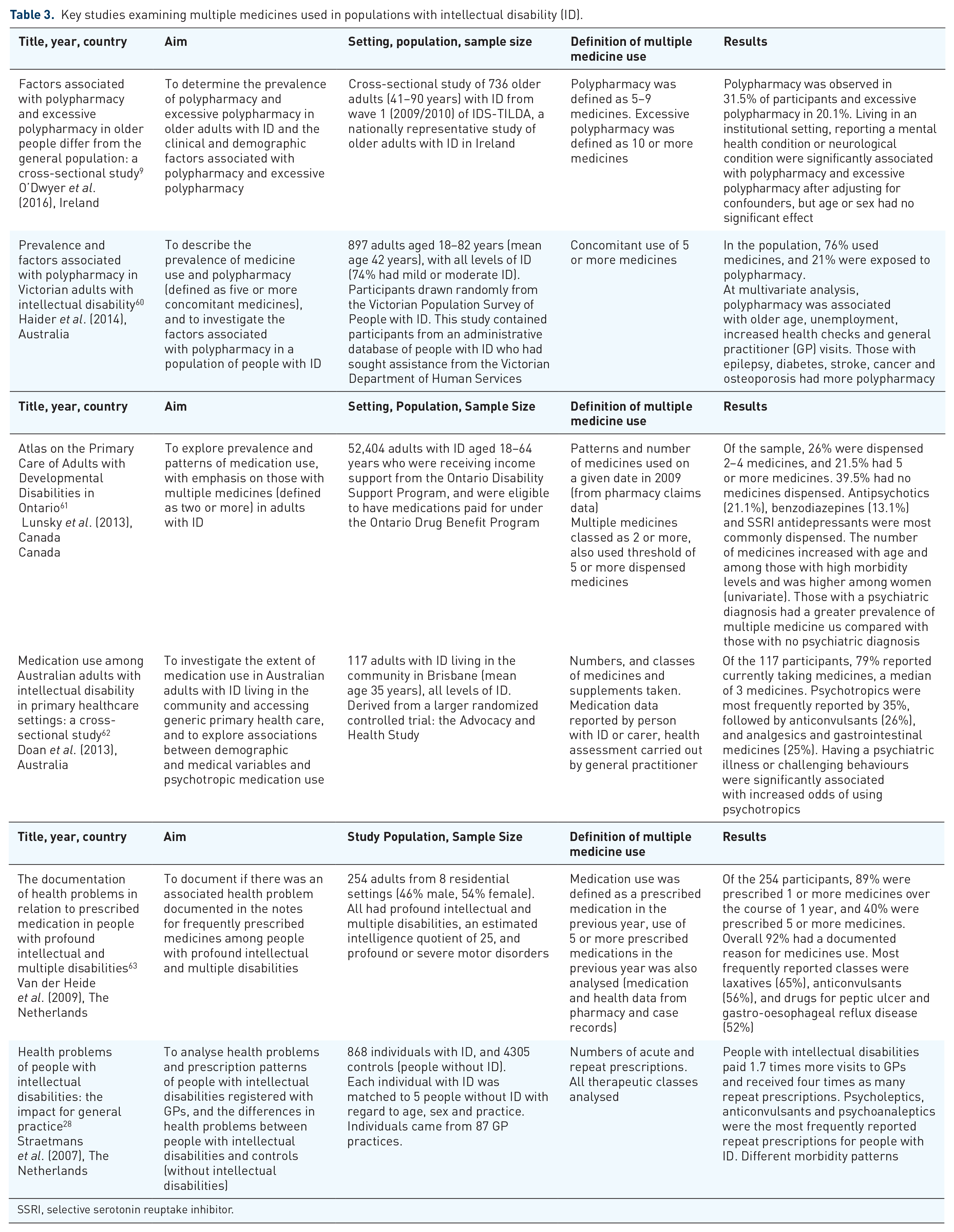
SSRI, selective serotonin reuptake inhibitor.
A number of factors have been identified as being associated with higher rates of polypharmacy in adults with ID, including living in institutional settings, having mental health conditions, neurological conditions and female sex.9,60 Studies in the ID population have also identified a different pattern of frequently reported medicine classes compared with the general population, reflecting the different patterns of multimorbidity. Among adults with ID, antipsychotics, AEDs, antidepressants and laxatives are the most frequently reported therapeutic classes.9,28,61 These findings are in contrast to the general older population, in which cardiac therapies, analgesics, gastrointestinal agents and antithrombotics are the therapeutic classes more frequently implicated in polypharmacy.64,65
Few studies have examined the impact of medication reviews on polypharmacy and outcomes in people with ID. 66 A narrative review examining pharmaceutical care interventions for people with ID, and pharmacists’ contribution to multidisciplinary teams caring for people with ID from 1994 to 2014, identified only eight articles. 66 While the evidence base was limited, studies were found to demonstrate that pharmacists did have an impact on identifying therapy-related problems through medication review and improving outcomes in people with ID.67,68
Specific drug classes
Psychotropic use
Psychotropic agents, in particular the antipsychotics, are frequently prescribed in adults with ID. Antipsychotics have been prescribed to manage mental health conditions, and controversially, challenging behaviours in the absence of a diagnosed mental illness. 69 In a large national study in the UK of 33,016 adults with ID in primary care, 21% of the cohort had mental illness, 25% had a record of challenging behaviours and 49% had a record of psychotropic prescribing. 6 New antipsychotic prescribing was significantly higher in those with challenging behaviour in this study. It has also been reported that 20–45% of adults with ID have been prescribed psychotropic medicines for control of aggression and self injury. 70 Their widespread use has been subject to criticism and concerns relating to the quality of prescribing. With less information available about the safety and efficacy of these agents in people with ID, particularly the effects of long-term use and prescribing in older adults, use of these drugs is often based on extrapolation of knowledge from the general population. 71
People with ID are frequently treated with more than one psychotropic medicine. There are clinical situations in psychiatry when the use of more than one psychotropic medication from the same or a different class may be indicated, justified and considered ‘rational polypharmacy’. The addition of an antipsychotic agent to a mood stabilizer for acute mania, for example, is an example of rational or empirically supported polypharmacy. 72 However, use of multiple agents may be irrational and increase the risk of adverse effects, drug interactions and medication errors in older adults with ID.2,72 One small study by Mahan and colleagues found a greater prevalence of side effects, including general effects on the CNS, in people with ID taking two or more psychotropics than in those who reported taking one. 73 A recent cohort study by Sheehan and colleagues as part of the Health Improvement Network database from UK primary care found that people with ID had a significantly higher incidence of movement side effects associated with antipsychotics compared with a control group cohort of adults without ID. 74 Table 4 summarizes key studies examining medicines acting on the CNS in adults with ID.
Key studies examining psychotropics and other centrally acting medicines in people with ID.
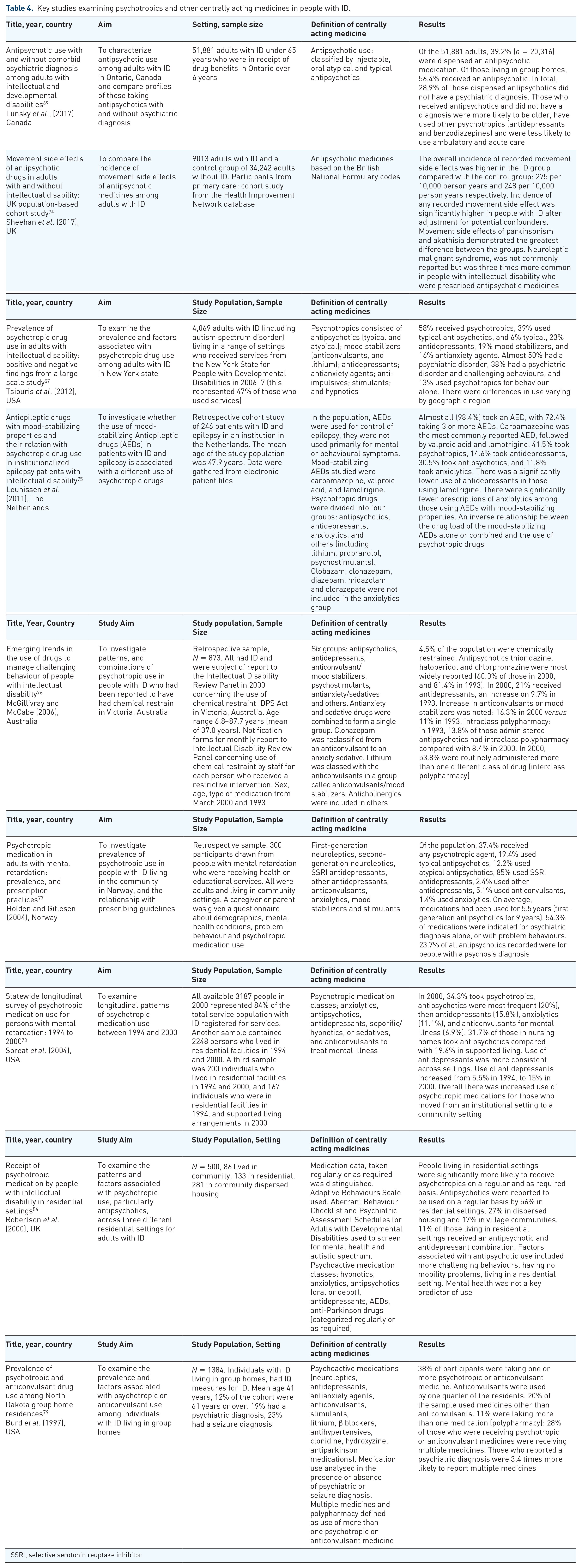
SSRI, selective serotonin reuptake inhibitor.
Antipsychotic agents have been the most broadly reported medicines for people with ID and comorbid psychopathology. 80 While antipsychotic pharmacotherapy has an important role in managing psychopathology, the role of antipsychotics in dealing with challenging behaviours has less evidence and more risk of harm. 80 The National Institute for Health and Care Excellent issued guidelines about appropriate responses to challenging behaviours in adults with ID in 2015. These guidelines highlighted that antipsychotic medication should only be considered to manage behaviours which challenge if psychological or other interventions alone do not produce change within an agreed timeframe; treatment for a coexisting mental or physical health condition has not led to a reduction in behaviour; and the risk to the person or others is very severe (because of violence, aggression or self injury). 81 In the UK, the 2012 Department of Health Review ‘Transforming care: a national response to Winterbourne View Hospital’ highlighted ‘deep concerns’ about overuse of psychotropic medicines in people with ID.82,83
There are few studies of high quality in relation to medication efficacy in the long-term treatment of challenging behaviour in the absence of mental illness, or of the associated risks with treatment. However, key findings that have emerged include the following:
The proportion of people with ID who are prescribed psychotropic medicines, in particular antipsychotics, exceeds that in those with a recorded diagnosis of mental illness.6,69
A RCT of typical (haloperidol) and atypical (risperidone) antipsychotics versus placebo for aggressive behaviour in people with ID found no significant advantage for either antipsychotic. 45
Antipsychotics are often more frequently used to treat challenging behaviour rather than schizophrenia in this population, despite little or no evidence for their effectiveness and some evidence of detrimental side effects.84,85
Despite these findings, antipsychotics may be prescribed continuously for many years, often resulting in chronic adverse effects. Findings include the following:
Substantial potential for deleterious side effects such as tardive dyskinesia, akathisia, pseudo-Parkinsonism in the case of first-generation antipsychotics such as chlorpromazine and haloperidol.74,40
Increased risk of metabolic side effects and weight gain in the case of atypical antipsychotics. 86
Antiepileptic drugs
The prevalence of epilepsy in people with ID is high, with estimates of 14–44%, 87 compared with estimates of 1.1% in the general population. Many people with ID have epilepsy that is ‘refractory’ to treatment, due to underlying abnormalities of the nervous system, and may have idiosyncratic responses to treatment.88,89 It has been reported that only 25–35% of patients with ID may become seizure free. 90
While the principles of AED therapy for an older person with ID are essentially the same as the general older population, there are unique issues that also need to be addressed. These include higher frequencies of epilepsy that may be refractory to treatment, atypical presentation of symptoms, seizures of multiple types and the presence of comorbidities. There is a limited evidence base associated with the safety and effectiveness of AED use in the ID population.91,92 While the incidence of side effects may be as high as 58% in the general population receiving AED treatment, 93 people with ID who have epilepsy are less likely to report side effects, particularly cognitive adverse effects. 94 A systematic review of tools to measure side effects of AEDs highlighted that, of 108 measures identified, only 8 were appropriate for use in adults with ID, and only 2 measures had been designed for use in people with ID. 95 As a result, side-effect detection is likely to be overly reliant on carer reports and side effects remains under detected. This represents a challenge for doctors, pharmacists and other health professionals in assessing the efficacy and safety of treatment in adults with epilepsy.
There are few high-quality observational and intervention studies of the treatment of epilepsy in ID cohorts. 96 A Cochrane review assessing pharmacological interventions for epilepsy in people with ID identified 14 RCTs and highlighted how under investigated this population is with regards to treatments for epilepsy. 97 The authors also noted variable study designs, small sample sizes and high dropout rates among some studies, which limited reliability of results. This review noted that ‘a moderate reduction in seizure frequency and occasional seizure freedom was obtained’ with use of therapeutic interventions. As the review pooled all AEDs together, comments or recommendations about the relative efficacy of each AED could not be made. The UK Royal College of Psychiatrists guidelines on prescribing AEDs for people with epilepsy and ID recommend lamotrigine and sodium valproate as the AEDs that should generally be considered as appropriate first-line treatments in the population with ID. These recommendations are based on evidence of efficacy and side effects and clinical experience. 98
Both seizures and AEDs may play a role in behavioural disturbances in people with ID and epilepsy. 99 As people with ID are at increased risk of mood disorders and epilepsy, using an AED for its mood-stabilizing effects as well as an anticonvulsant is commonplace.50,99 Concurrent use of psychotropics in the population with epilepsy carries risk due to the potential for drug–drug interactions (DDIs): some psychotropics, including the first-generation antipsychotics, reduce the anticonvulsant activity of first-generation AEDs such as carbamazepine. 50 Pharmacists and prescribers therefore need to be vigilant for DDIs between AEDs and psychotropics. Moreover, many enzyme-inducing AEDs may lower the plasma levels of other psychotropics, for example selective serotonin reuptake inhibitor antidepressants, and impair control of psychiatric symptoms. 100
Anticholinergic medicines
Medications with anticholinergic effects have been associated with central and peripheral side effects, such as sedation, confusion, dry mouth and constipation. The risk of adverse outcomes increases with increasing anticholinergic exposure.101–103 Older adults are particularly vulnerable to anticholinergic adverse effects due to a high probability of exposure to medicines with anticholinergic properties to treat age-related morbidities. They may also experience increased age-related sensitivity to anticholinergic-related cognitive adverse effects.102,103 Medical conditions which are commonly presented in older people, such as urinary dysfunction, constipation and dementia, may be worsened by the use of anticholinergics.104,105 Anticholinergic medications have been highlighted as being potentially inappropriate in older and frail adults,1,106 including vulnerable older people and those with dementia. 107
People with ID may experience the ‘prescribing cascade’ in relation to anticholinergic medicines, for example, prescribing of anticholinergic medications for movement disorders to treat extrapyramidal symptoms associated with antipsychotic agents, a practice no longer recommended in older adults. 1 Medications which people with ID may have been taking for many years may start to produce anticholinergic side effects that may go unrecognized because they had not previously presented a problem.
It is likely that many older adults with ID would have a high burden of anticholinergic medicines due to the high prevalence of use of psychotropic agents. An observational cross-sectional study of 736 older adults with ID identified that there was a high burden of anticholinergic use: 70% of adults with ID had anticholinergic exposure. Older age and having a mental health condition were significantly associated with having a high Anticholinergic Cognitive Burden (ACB) score (ACB score 5+). 8 Those with high burden were more likely to report chronic constipation and daytime drowsiness. Antipsychotics, anticholinergics and AEDs were the highest contributors to the burden in the population, accounting for 35%, 16% and 11% of the burden respectively. These findings were in contrast to a previous cross-sectional study of 6666 Irish community-dwelling adults in the general population over 50 years of age in whom cardiac agents were most commonly reported. 108 There have been no longitudinal studies to date on the outcomes of anticholinergic exposure and long-term effects on physical and cognitive function in older adults with ID. There has been research carried out in the older population examining the risks associated with cumulative sedative and anticholinergic burden through use of the Drug Burden Index (DBI) tool and associations with adverse outcomes such as cognitive decline. 109 Findings from a cross-sectional study of 677 older adults with ID in Ireland identified that 54% had a high DBI score (score of 1+). 110 This study identified that this high burden was associated with higher levels of dependence, as measured by the Barthel Index.
Measuring PIP
Few studies to date have examined PIP in older adults with ID. In an observational pilot study of 27 adults with ID living in residential facilities, STRIP (Systematic Tool to Reduce Inappropriate Prescribing) was applied to medication records to identify the prevalence of drug-related problems (DRPs). This tool has been developed for older patients with polypharmacy in the Netherlands. 111 For this study, DRPs were identified by applying the STOPP/START (Screening Tool of Older Persons Prescriptions/Screening Tool to Alert Doctors to Right Treatment) criteria. In addition, the pharmacist carrying out the medication review identified additional DRPs based on their professional judgment and guidelines on appropriate prescribing in people with ID or the general population. At least one DRP was identified for each person with ID in the pilot study, and after 6 months, 15.7% of interventions recommended from the review had been implemented. In another study in the Netherlands, a structured medication review in a treatment facility for people with mild and borderline ID and behavioural problems was described. 112 Here DRPs were defined and identified by the pharmacist and were categorized into those relating to drug selection (e.g. duplication, DDI, lack of indication, unclear indication) and those related to dosage/formulation (e.g. dosage too high, inappropriate formulation). Prevalence and types of DRPs among 55 patients with ID who were taking at least one psychotropic medicine were examined. This study identified a prevalence of DRPs of 34%. The most common DRP identified was a prescribed medicine having no indication or an unclear indication. In this study, the pharmacist and psychiatrist implemented a care plan and 60% of recommended actions were executed. A cross-sectional study in the Netherlands examined the prevalence and risk factors for prescription errors in 600 adults aged 50 years and over with ID from the Health Ageing and Intellectual Disability Study. 7 Participants taking at least one medicine were screened for prescription errors, which were defined as prescriptions that were not in accordance with current prescribing standards. Types of error were classified into dosage errors (dose too high or low) and therapeutic errors, including DDIs, time interaction, unnecessary drug therapy. Prevalence of errors was 47.5% and relevant errors (those that required a change of pharmacotherapy) were identified in 26.8% of individuals. Older age, higher frailty, less severe level of ID, polypharmacy and use of CNS medicines were associated with prescription errors. No study to date has used a tool specifically developed and validated for adults with ID.
A recent study in Sweden used a national register of 7936 adults with ID who were matched to people from the general population and examined the prevalence of PIP compared with those in the general population. 113 This was carried out using a list of medicines that may need extra attention in older adults, published by the Swedish National Board of Health and Wellbeing. Adults with ID were more likely to be prescribed PIPs, including anticholinergic medicines, benzodiazepines and antipsychotics, but less likely to be prescribed nonsteroidal anti-inflammatory drugs. A limitation of the study was that there was no information on clinical diagnosis and no ID-specific PIPs.
Deprescribing
In the general population, deprescribing as a means of reducing PIP is gaining increasing attention.20,114 To date, deprescribing initiatives in the population with ID have generally focused on antipsychotics. 115 In a study in the Netherlands which took place in six service providers for people with ID, the reasons why physicians did not discontinue off-label use of antipsychotics were examined as part of an antipsychotic discontinuation trial. Prevalence of antipsychotics use was 30% among 3299 participants. Reasons for not discontinuing were previous unsuccessful attempts, objections from legal representatives, and presence of an autism spectrum disorder with a large variance in reasoning between the service providers. 116 A pilot RCT of drug reduction of 22 adults with ID treated with risperidone for challenging behaviour with no known current or previous psychosis was carried out in the UK. 117 Of the 22 participants, 59% achieved progression through the stages of reduction and the study found no clinically important changes in the participant’s level of aggression or challenging behaviour at the end of the study. The findings were limited by the small number of participants, difficulties in recruitment and limited availability of alternative behavioural interventions.
A systematic review identified that antipsychotics may be reduced or discontinued in a large proportion of adults with ID who use them for challenging behaviour, but the authors concluded that this may not be without adverse effects. These risks included unmasking of a mental disorder and withdrawal reaction. 115 However, no predictors of poor response could be reliably identified in the available studies. Due to the scarcity of data and limitations of the available studies, no conclusions or recommendations at a population level could be made by the authors and they recommended an individualized approach to treatment and regular medication review.
In response to reports published in England highlighting inappropriate use of antipsychotics and psychotropics, NHS England initiated the ‘Stopping over medication of people with a learning disability, autism or both (STOMP)’ project. 10 This is a 3-year project (ending in 2019) and the STOMP pledge was signed by partners in the UK, including NHS England, the Royal College of Psychiatrists and the Royal Pharmaceutical Society. Health care professionals in England are being trained to support this initiative. Activities include ensuring that those receiving a psychotropic medicine for challenging behaviour have a positive behaviour support plan, audits of psychotropic use to assess the impact of the project on a quarterly basis, and recommendations for comprehensive monitoring of medicine. As a result, a number of guidelines have been developed, including practice guidelines on psychotropic prescribing from the Royal College of Psychiatrists. 118
Underutilization of therapeutic classes
Paradoxically, a patient already exposed to polypharmacy may not receive other medicines due to challenges associated with communication and diagnostic overshadowing and fears of interactions with drugs already prescribed. In a study of polypharmacy in older adults with ID in Ireland, almost half of the cohort reported pain, but only 2% used paracetamol–codeine combinations, and 1% opioids, while a third reported using paracetamol. 9 Pain and its appropriate treatment need to be examined in more detail in the ID population.
Priorities for research and practice
Research is needed on the long-term effects of medicines in older adults with ID, particularly psychotropic medicines and sedative and anticholinergic medicines which may adversely affect physical and cognitive outcomes. Since people with ID are often excluded from RCTs, there needs to be more representative longitudinal studies allowing for international comparisons assessing the benefits and risks of polypharmacy. This should include studies on antipsychotics, but also encompass other important classes of medicines that may cause long-term harm, including anticholinergics.
Specific prescribing criteria need to be developed for people with ID to guide identification of PIP at a population level and associated adverse outcomes. Attention should be paid to other medicines that may be underutilized, such as for eye conditions and pain management. This criterion should take into account multimorbidity specific to adults with ID, particularly epilepsy and mental health conditions, and should be applicable in different care settings for people with ID. The use of ID-sensitive versions of scales such as the ACB scales, in addition to a review of the patient’s symptoms and screening for side effects, may provide a useful aid in multidisciplinary medication reviews to identify those at risk of medication-related harm. The effectiveness of pharmacists in this context with other patient groups has been acknowledged, 119 and needs to be further developed in interventions for patients with ID.
Education of health care professionals in primary care is required as people with ID move into community settings and access primary care. This should include initiatives to carry out comprehensive multidisciplinary medication reviews. Awareness of the potential of the prescribing cascade among all healthcare professionals is required. There is a need for increased visibility of the complex health issues in adults with ID, addressed through education of pharmacists and general practitioners in primary care and students at undergraduate level. 92 There is an important opportunity for pharmacists to lead these efforts.
Complex interventions have been increasingly used in the general older population to reduce PIP.120,121 Similar types of interventions to improve prescribing and health outcomes in older adults with ID should be explored. A multifaceted intervention may be more effective than one single intervention by targeting behaviours among prescribers, pharmacists and other health care professions. These interventions should include stakeholder views of patients and carers or family members, involving people with ID and their families who experience polypharmacy in the decisionmaking processes.
Conclusion
People with ID experience poorer health compared with the general population and are at risk of medication-related harm relating to appropriateness and safety of medicine use. While many older adults with ID gain benefit from polypharmacy, PIP carries substantial risk. With the growing older population of people with ID, it is necessary to be vigilant for adverse effects of medicines that may not manifest at younger ages. Evaluating the benefits of polypharmacy and its role in the appropriate treatment of complex comorbidities in older people with ID must be balanced with the risks of adverse outcomes associated with the use of polypharmacy, particularly medicines which have anticholinergic or sedative properties. In particular, the use of multiple psychotropic agents should be frequently evaluated to assess benefits and risks. Prescribing and providing pharmaceutical care in this population should be carried out in a manner that explicitly considers the overall effect of the total drug burden. There is a need for the development of ID-specific validated tools to measure PIP, which would provide health professionals with means to evaluate medication regimens in a structured manner. Health professionals in primary care need education on the unique medical and pharmaceutical care needs of people with ID. When considering prescribing, clinicians should consider risks and benefits, and impact on quality of life. Long-term outcomes of polypharmacy in this population and PIP warrant further research.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This review was completed as part of a PhD studentship supported by Trinity College Dublin.
Conflict of interest statement
The authors declare that there is no conflict of interest.