
Abstract
Despite significant population level declines, smoking during pregnancy remains a major public health issue in the United States (US). Approximately 360,000–500,000 smoke-exposed infants are born yearly, and prenatal smoking remains a leading modifiable cause of poor birth outcomes (e.g. birth < 37 gestational weeks, low birth weight, perinatal mortality). Women who smoke during pregnancy are more likely to be younger and from disadvantaged socioeconomic and racial and ethnic groups, with some US geographic regions reporting increased prenatal smoking rates since 2000. Such disparities in maternal prenatal smoking suggests some pregnant women face unique barriers to cessation. This paper reviews the current state and future direction of smoking cessation in pregnancy in the US. We briefly discuss the etiology of smoking addiction among women, the pathophysiology and effects of tobacco smoke exposure on pregnant women and their offspring, and the emerging issue of electronic nicotine delivery systems. Current population-based and individual smoking cessation interventions are reviewed in the context of pregnancy and barriers to cessation among US women. Finally, we consider interventions that are on the horizon and areas in need of further investigation.
Keywords
Introduction
Overview of cigarette smoking as a problem
Despite declines in high-income countries, cigarette smoking remains a major public health crisis with increasing global consumption rates. According to the World Health Organization (WHO), more than a billion people smoke cigarettes worldwide and cigarettes contribute to 5 million deaths annually. 1 In 2015, 15.1% of adults in the United States (US) reported smoking cigarettes or nearly 36.5 million people, and smoking accounts for more than 480,000 deaths annually.2,3 Thirteen out of every 100 women in the US are currently smoking (versus 17 of 100 men) and smoking is more common among both sexes during reproductive ages. 2 Despite well known adverse effects to themselves and the developing fetus, approximately 9% of women report smoking during pregnancy, resulting in roughly 360,000 smoke-exposed infants born in 2015. 2 Tobacco addiction is a unique chronic condition in that cigarettes are extremely addictive, heavily advertised, and significant gradients in smoking rates exist between sexes (male versus female), and across socioeconomic and racial and ethnic groups. 4
Pharmacokinetics of nicotine addiction
When tobacco is smoked (e.g. cigarettes) the primary addictive substance, nicotine, diffuses rapidly into the bloodstream, reaching the brain in less than 20 s and achieving peak blood concentration in roughly 5 min. Upon reaching the brain, nicotine binds to nicotinic acetylcholine receptors triggering a release of dopamine and serotonin along with other neurotransmitters. Dopamine is associated with pleasure and is a major actor in the neuronal reward system. Thus, rapid release of dopamine in response to nicotine is thought to be an addictive feature of tobacco as a positive reinforcement. Continued nicotine intake negatively reinforces smoking by reducing nicotine withdrawal symptoms (e.g. discomfort, agitation, depressive symptoms). 5
Withdrawal symptoms occur in at least half of all smokers upon quitting. Symptoms generally start a few hours after smoking a cigarette, peaking within the first week of cessation, and resolving over a month. 6 The etiology of individual variations in withdrawal symptom severity is multifaceted and may play a role in choice of cessation aid. Women may have increased depressive symptoms and discomfort with quit attempts during the luteal menstrual phase. 7 Those who started smoking at a younger age, have fewer quit attempts, and report heavier smoking may have a stronger nicotine addiction and experience greater withdrawal symptoms.8,9 Nicotine is metabolized by the liver, particularly by the cytochrome enzyme CYP2A6. Genetic variations affecting activity of the CYP2A6 enzyme result in slower metabolism of nicotine, which may lengthen periods without withdrawal symptoms, resulting in less nicotine consumption and more successful tobacco cessation. However, metabolizing nicotine more rapidly may induce withdrawal symptoms sooner, resulting in increased nicotine intake and difficulty with cessation.10,11 Pregnancy and increasing levels of estrogen are thought to also increase activity of cytochrome enzymes and nicotine metabolism. 12
Etiology of cigarette smoking among women
Tobacco use among women has followed a distinct path, taking approximately 25 years longer for cigarette smoking to become commonplace among women than it did for men. 13 In 1920, with women achieving suffrage and recently entering into wage work, the tobacco industry capitalized on a new demographic of potential smokers, successfully marketing cigarettes to women as a symbol of glamour and of independence (Figure 1 14 ). Additionally, cigarettes were heavily advertised to women as a weight-loss tool. 15 Between 1924 and 1935 it is suggested that cigarette smoking prevalence among women more than tripled from 6% to 20%. 13 Today the tobacco industry continues to cast smoking as a sexy or edgy behavior, one that creative and adventurous women partake in.16,17,18 Although never reaching the proportion of male smokers, by 1965 over 33% of women reported smoking cigarettes (versus 62% of non-Hispanic white men). The Surgeon General’s 1964 warning and concerted efforts to limit access and exposure to tobacco as well as to increase public awareness of tobacco-related health hazards led to significant declines in cigarette smoking among women and men. 19 Concerning is the fact that from 1965 to 1979 male smoking rates declined by nearly 15% compared with a 4% decline among women. A flatter decline among women has led to narrowing in the smoking gender gap from 18% in 1965 to 3.1% today.19,20

Young woman smoking a cigarette circa 1922 (Image take from the US Library of Congress - www.loc.gov/item/95504332/).
Women seem to differ in physical and psychological experience of smoking. Estrogen is linked to increased activity of CYP2A6 and increased metabolism of nicotine, which is associated with tobacco dependence. 21 Women are more likely than men to report using smoking as a coping tool for negative affective states such as depression and anxiety. Women also report more withdrawal symptoms.12,22,23 Data regarding smoking initiation among adolescents suggest young men and women are influenced by peer and parental smoking. Studies have found that compared with young men, young women may start smoking out of rebellion and may be more sensitive to smoking attitudes of family and peers, while young men have shown greater sensitivity to direct peer pressure.24–26 In light of variations in uptake of cigarette smoking by sex, 19 sex-targeted tobacco marketing schemes, 17 and flatter declines in smoking rates among women 13 sex-based approaches to primary prevention of smoking and smoking cessation techniques are appropriate.
Epidemiology of smoking in pregnancy
Pregnancy presents a unique opportunity for smoking cessation. Up to 45% of women who smoke quit before their first antenatal visit or during pregnancy.27,28 In 2014, 8.4% of US women reported smoking at any time during pregnancy. Approximately one quarter of the 10.9% who reported smoking prior to pregnancy had quit. 20 Unfortunately, these smoking estimates are likely conservative. Based on nicotine biomarker data, up to 25% of women inaccurately report their smoking status at prenatal visits, 29 in particular, African American and Hispanic women have higher nondisclosure rates. 30 Furthermore, there are populations and geographic regions in the US that are disproportionally affected by prenatal smoking. In 2016, 1.2% of Californian pregnant women reported smoking compared with 27.1% of women in West Virginia. 2 Trend data from 2000 to 2010 show smoking prevalence before, during, and after pregnancy actually increased among three US states: Louisiana, Mississippi, and West Virginia; and for the majority of states the prevalence remained unchanged for all three measures. 31 Overall, smoking disproportionally affects those residing in rural areas versus urban areas. 32 Female adolescents who report abuse have 5.90 times the odds of smoking compared with girls who do not report abuse. 33 By race, the highest prevalence of smoking occurs among those who identify as native American, white, multiracial, and African American, with the lowest prevalence among women of Hispanic ethnicity and Asian and Pacific Islander races. Pregnant smokers are more likely to have a low level of education (⩽12 years) and earn less income than pregnant nonsmokers.20,34
Although in general women are more likely to stop smoking in pregnancy than at any other time in their lives, women with unplanned pregnancies are approximately 15% less likely to quit or reduce cigarette consumption than women with planned pregnancies [odds ratio (OR) 0.86; 95% confidence interval (CI) 0.78–0.95]. 35 Pregnancy may be an additional stressor for women already living in stressful environments. Healthy People 2020 links socioeconomic and environmental disadvantages to different health disparities. 36 Some groups systematically experience barriers to health and wellness based on primarily immutable factors such as race and ethnicity, sex, economic status, or geographic location. WHO acknowledges that poor health behaviors such as smoking are a consequence of life circumstances. 37 Targeted and accessible cessation interventions for women who are most likely to smoke during pregnancy are crucial. 38
The use of electronic nicotine delivery systems (ENDS) among pregnant and nonpregnant women is an emerging issue. In 2015, 7.4% of US women reported using e-cigarettes and a survey of pregnant women demonstrated that 40% did not realize that ENDS contained nicotine or could be addictive. 39 The most recent National Youth Tobacco Surveys found that 16% of high-school students were using e-cigarettes; this is up from 1.5% in 2011. 40 With rising popularity among adolescents who will soon enter their childbearing years, the rate of ENDS use in pregnancy is a concern.
Effects of smoking in pregnancy
Smoking is the leading preventable cause of preterm birth (birth <37 gestational weeks) and is linked to 5–8% of premature births yearly.41,42 Women who smoke are more likely to have a fetal loss, premature rupture of membranes, and placental abruption and placenta previa. 42 Smoking is causatively linked to some congenital anomalies of the mouth and face (cleft lip/palate), and is associated with increased cardiac, limb, and gastrointestinal defects. 3 Maternal smoking increases the relative risk of low birth weight (LBW) by 1.3–10 and has been attributed to up to 19% of LBW term infants. Increased health risks for smoke-exposed offspring are multisystem and include respiratory infections, reactive airway disease, otitis media, bronchiolitis, short stature, hyperactivity, obesity, and decreased academic performance. Furthermore, up to 34% of sudden unexpected deaths in infants are attributed to maternal smoking.42–44 Second-hand tobacco smoke exposure during pregnancy also increases the risk of delivering premature and LBW infants. 45
There are more than 7000 chemicals in tobacco smoke, hundreds of which are toxic including ammonia, polycyclic aromatic hydrocarbons, and hydrogen cyanide.46,47 Nicotine and carbon monoxide (CO) are major compounds of tobacco smoke with documented fetal neurotoxic effects.46,47 Nicotine and CO readily cross the placenta into fetal circulation where they can exceed maternal circulating levels by more than 15%, while nicotine levels in amniotic fluid can exceed maternal plasma levels by 88%.48,49 Animal and human studies demonstrate that nicotine and CO initiate pathologic mechanisms disrupting uterine artery blood flow and fetal oxygenation. Restricted oxygen and nutrition transfer to the fetus likely underlay the significant associations between maternal smoking and preterm birth and low birthweight.50,51
Nicotine also binds to widely available fetal acetylcholine receptors, influencing epigenetic changes affecting lung and brain development. Interaction with α7 nicotinic acetylcholine receptors (nAChR) in the lung of animal models causes upregulation of collagen gene expression resulting in increased collagen deposition and thickened airway walls, a potential pathway to the pulmonary function deficits seen in offspring of smokers.52–54 Nicotine-induced abnormal activation of neuronal acetylcholine receptors may impact brain development, explaining the increased incidence of neurobehavioral problems and poor academic performance in children of smokers.55,56 Quitting smoking at any point during pregnancy may improve the outcomes listed above. Notably, quitting by the third trimester is associated with neonatal birth weights similar to those of nonsmokers.57–59
Population-level primary prevention and cessation interventions
Smoking bans
Smoking bans are considered an effective tool to reduce second-hand smoke exposure and encourage smoking cessation and primary prevention of smoking by limiting smoking opportunities.60,61 After the implementation of national smoking bans, continuing smokers have reported smoking the equivalent or significantly fewer cigarettes per day. 62 Smokers with stronger nicotine dependence, 8 lower level of education, and past illicit drug use are less likely to comply with smoking bans. 63 Concerning, is a potential for displacement of smoking to indoor locations after implementation of US smoking bans, potentiating maternal and fetal nicotine exposure through indoor tobacco smoke. 64 Further limiting access, retail stores such as CVS Pharmacy have committed to not selling cigarettes 65 and it is illegal for children under the age of 18 to purchase tobacco products.
Increasing social stigma
Imagery of smoking in print, on television or in movies, and in other forms of mass media has dramatically evolved in the US since the 1930s. Aside from traditional avenues of public health education around dangers of smoking to self and others, antismoking media campaigns including the Truth Initiative and others successfully increased social stigma around smoking, in part by targeting self image.66,67,68 Pregnant and nonpregnant women report concern for weight gain as rationale for continued smoking, 69 thus targeting the negative consequences to appearance may be particularly effective at preventing and decreasing smoking among some women.
As discussed previously, declines in smoking rates heavily favor higher socioeconomic classes in the US. Such disparities in light of increased stigmatization have shifted the public image of smoking from one of independence and glamour to one of shame and deprivation.38,70 Shame related to smoking may have unintended consequences on maternal reporting of smoking status during screening. As described earlier, up to a quarter of pregnant women will not report smoking. 29 Nondisclosure leads to missed opportunities for intervention and to inaccurate reporting of national prevalence rates and subsequently to poor understanding of tobacco use by public health entities. In a 2006 report published in the American Journal of Public Health, authors Ronald Bayer and Jennifer Stuber 71 recalled, ‘Stigmatization represented a profound psychological and social burden on those with AIDS or HIV infection and it also [fueled] the spread of the epidemic.’ Further adding, ‘Yet, in this instance [referring to smoking], the concerns about the impacts of stigmatization have been given little consideration.’
Taxation
Tobacco taxation is described as the leading population-based method for reducing smoking and its health-related consequences. 72 Increased tobacco taxation is passed on to consumers, raising the purchase price of cigarettes. A 10% increase in the price of cigarettes can lead to a 4% reduction in demand. 73 Research overwhelmingly supports that those of lower socioeconomic status (SES) are equally or more responsive to taxation than those of higher SES. However, nicotine is still a highly addictive substance and people of lower SES who remain smoking may suffer great financial burden.74,75 As evidence, heavier smokers and those of lower SES groups are more likely to seek contraband cigarettes.76,77 Contraband cigarettes have been viewed as a necessary strategy for those living in deprived environments to combat higher tobacco costs in the face of limited smoking cessation support. 76 Additionally, tobacco sales on Native American lands are exempt from state taxation and up to 30% of smokers in some US states report purchasing cigarettes on tribal land. 78 Currently, ENDS are not subject to federal taxation and as of 2015 just five states taxed ENDS. Experimental data from a sample of 1200 adults who smoked suggested responsiveness to taxation of ENDS and to the restriction of ENDS flavors. 79 Overall, considering the potential consequences of smoking bans and stigmatization, taxation should occur in conjunction with individual smoking cessation interventions to mitigate unintended adverse consequences on high-risk populations with fewer resources. 77
Individual-level cessation interventions
Behavioral support therapy
Screening
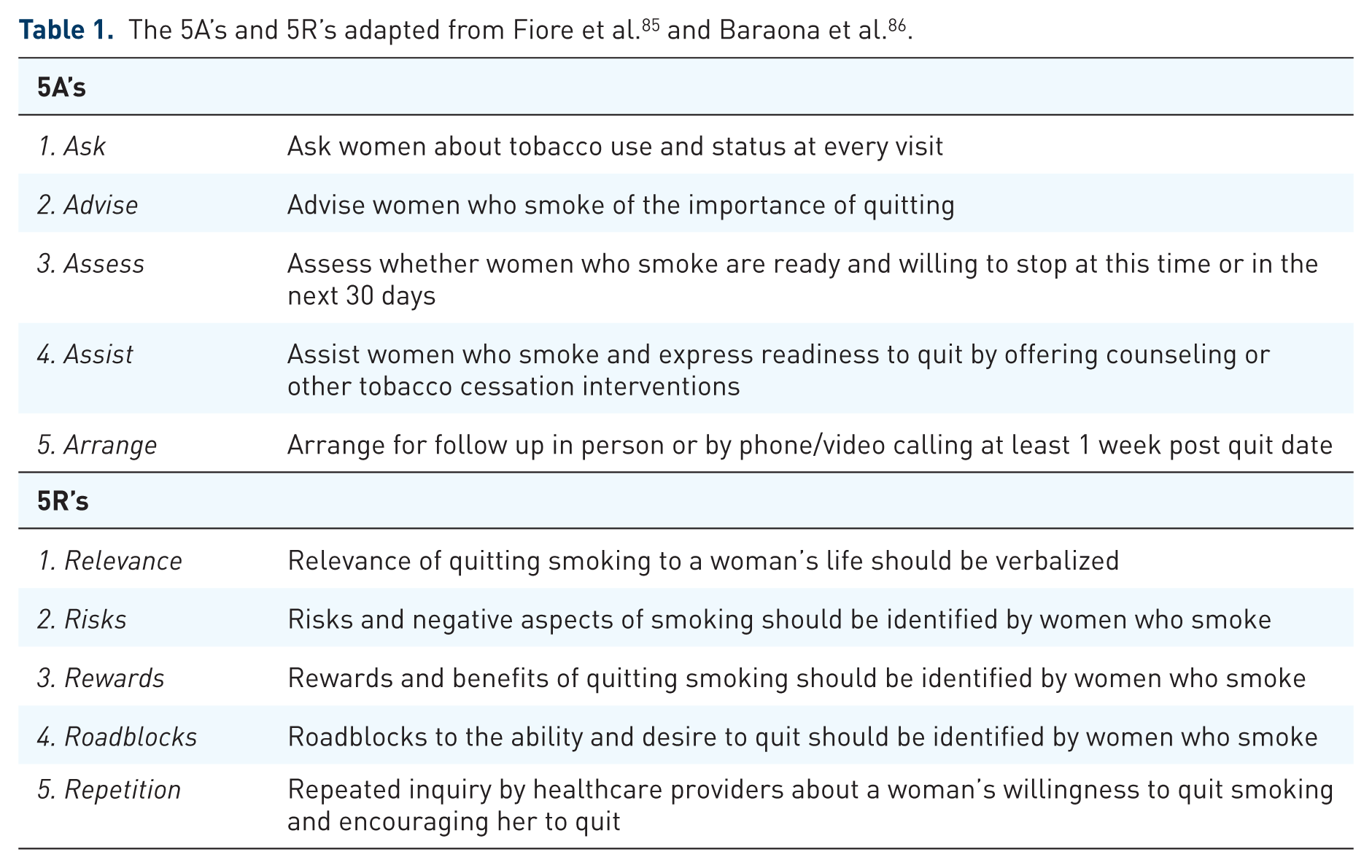
Asking a woman if she is smoking is the first step toward tobacco cessation. Providers should document smoking status at the initial prenatal visit, and at each subsequent visit for active smokers. Multiple choice formats improve smoking disclosure rates by 40%. 80 Comprehensive screening for pregnant women includes asking whether she smokes currently; if no, asking whether she smoked in the last year; if no, asking whether she uses ENDS (adapted from Tolosa and Stamilio 81 ). If a woman responds positively to any of the screening questions she should be provided with counseling and interventions. The 5A’s 82 is a five-step screening and brief intervention designed for providers to identify women who smoke and to help women if they verbalize a desire to quit in the next month (Table 1). The 5A’s is recommended by the American College of Obstetricians and Gynecologists. 83 Routine CO monitoring at prenatal appointments may help identify women who incorrectly disclose smoking status, but regardless of identification, a woman’s desire to quit is key. 84 Among patients reporting not willing to quit, providers should use the 5R’s in conjunction with motivational interviewing techniques (Table 1). 82 The 5R’s do not need to be completed in one visit, instead identify the most relevant R’s based on conversation with the woman. For example, if a woman reports that smoking is a stress reliever then focus on the stress-reducing rewards of eliminating nicotine exposure and discuss replacement activities (e.g. taking a walk or calling a friend).
More than half of pregnant women who quit smoking will relapse in the first 4 months after delivery. 31 A barrier to cessation and a risk factor for relapse is having an intimate partner or family member who smokes. 87 Other risk factors include depression symptoms, severity of nicotine addiction, and low prenatal weight gain. Effective relapse prevention strategies are poorly elucidated, but smoking abstinence should be closely monitored, with cessation support provided through postpartum. Including a woman’s partner during smoking cessation may increase abstinence.87,88
Counseling
Behavioral counseling remains the number one recommended smoking cessation intervention for pregnant women from the US Preventative Services Task Force (USPSTF). 89 A health care provider discussing smoking with women at a prenatal visit for 5–15 min can provoke a 5–10% cessation rate. 82 Telephone-based cessation support via hotlines such as the national and local QUITLINE or 1-800-QUIT-NOW also aids in cessation. 82 Effectiveness is improved if providers guide women to use hotlines, such as making the initial call together at a prenatal appointment.
There is a strong dose response between frequency and duration of counseling and its effect on smoking cessation. A 2017 Cochrane Database meta-analysis 90 affirms that person-to-person psychosocial interventions are more effective than usual care, which varied from self-help booklets to health education [n = 30 studies; mean relative risk (RR) 1.44; 95% CI 1.19–1.73], and more effective than minimal advice to quit (n = 18 studies; mean RR 1.25; 95% CI 1.07–1.47). Pregnant smokers receiving counseling have demonstrated an 80% greater cessation than those receiving usual care (e.g. advice to quit and self-help material) (OR 1.8; 95% CI 1.4–2.3). 82 Lee and colleagues 91 tested the impact of 120 min of cognitive-behavioral therapy (CBT) over four sessions on long-term smoking cessation rates among 227 disadvantaged pregnant women living in an urban setting. At 5 months postpartum, 37.3% of women who were randomly allocated to receive the CBT were abstinent compared with 19% of women allocated to usual care. Women who reported higher self efficacy and lower negative consequences of quitting were more likely to be abstinent at 5 months. Quitting smoking at any point during pregnancy is associated with real improvement in clinical outcomes, including a 20% reduction in the number of LBW babies and a 17% decrease in preterm births.57,92
The 5A’s has an estimated cost of $24–34, which equates to a saving of $881 per US pregnant smoker. This is a total saving of $8 million (in 2006 US$), resulting from decreased neonatal care expenditures given increased quit rates of 70%. 93 Despite cost savings and efficacy of counseling, and USPSTF recommendations, 94 women most vulnerable to smoking during pregnancy may not have access to counseling services. A 2015 Centers for Disease Control and Prevention (CDC) report 95 indicated that 20 states do not cover individual counseling services for Medicaid enrollees and most states have barriers to access counseling services, including prior authorization requirements; limits on duration and annual limits on quit attempts; copayments. Additionally, although 88.1% of US providers surveyed reported screening for tobacco use at initial prenatal visits, only 59.9% followed up at subsequent visits when a woman reported tobacco use. The most common reported barriers were insufficient time and expecting women to resist treatment. Very few providers report addressing the use of any other forms of tobacco at prenatal visits. 96
Financial incentives
Financial incentives, including voucher-based contingency interventions (e.g. withholding incentives when relapse is detected), increase the rate of smoking cessation and have improved clinical outcomes such as infant birth weight. 97 A recent meta-analysis found that compared with noncontingent incentives, incentive-based interventions were more effective at increasing smoking cessation among pregnant women (n = 4 studies; RR 2.36; 95% CI 1.36–4.09). 90 A previous meta-analysis found cessation at 6 months among incentive-based intervention participants was 42% greater than controls (n = 17 trials; OR 1.42; 95% CI 1.19–1.69). 97 Trials focusing on deposit-based (e.g. money lost) versus reward-based (e.g. money received) programs have found that participants are more receptive to the latter, but when smokers did enroll in a deposit-based intervention they were more likely to quit. Generally, smokers of lower SES are less likely to remain smoke free at long-term follow up 98 and may be receptive to the reward-based interventions. Financial incentives for smoking cessation among pregnant women are a promising avenue for research.
Pharmacotherapy
Of note, the US Food and Drug Administration (FDA) has recently published a new rule for labeling drugs regarding safety and efficacy during pregnancy and lactation. This new rule will replace the pregnancy letter categories (e.g. pregnancy category C = ‘Animal reproductive studies have shown an adverse effect on the fetus and there are not adequate and well-controlled studies in pregnant women, but potential benefits may outweigh potential risks’) with narratives detailing safety and efficacy for pregnancy, lactation, and women and men of reproductive ages. Drug companies must comply with this rule by 29 June 2018 by removing pregnancy letter categories from drugs approved before June 2001, and by removing the letters and replacing them with narratives for drugs approved after June 2001. 99
Nicotine replacement therapy
Among the general population the USPSTF 2015 guidelines recommend pharmacological treatment along with behavioral counseling for those who report cigarette smoking. 94 Nicotine replacement therapy (NRT) provides nicotine systemically without intake of cigarette smoke to reduce withdrawal symptoms and cravings with the ultimate goal of complete smoking cessation. NRT is available in multiple formulations, including transdermal patch, nasal spray, gum, inhaler, and lozenge. The dosing regimen is flexible and NRT is typically taken as needed for cravings. Patches, gum, and lozenges are available over the counter, adding to accessibility (Table 2). Overall, NRT compared with control increases the rate of quitting in the general population by 50–70%. 100 Reported quit rates do vary across NRT formulations from a 43% increase in quit rates utilizing nicotine gum to 90–100% increase in quit rates with inhaler, lozenge, and nasal spray.100,101 The FDA classifies NRT in the form of gum as a pregnancy category C and all other forms as a pregnancy category D drug, indicating that it has demonstrated risks to the fetus.
Nicotine replacement therapy (NRT) dosing regimen (not adequately studied in pregnancy).*
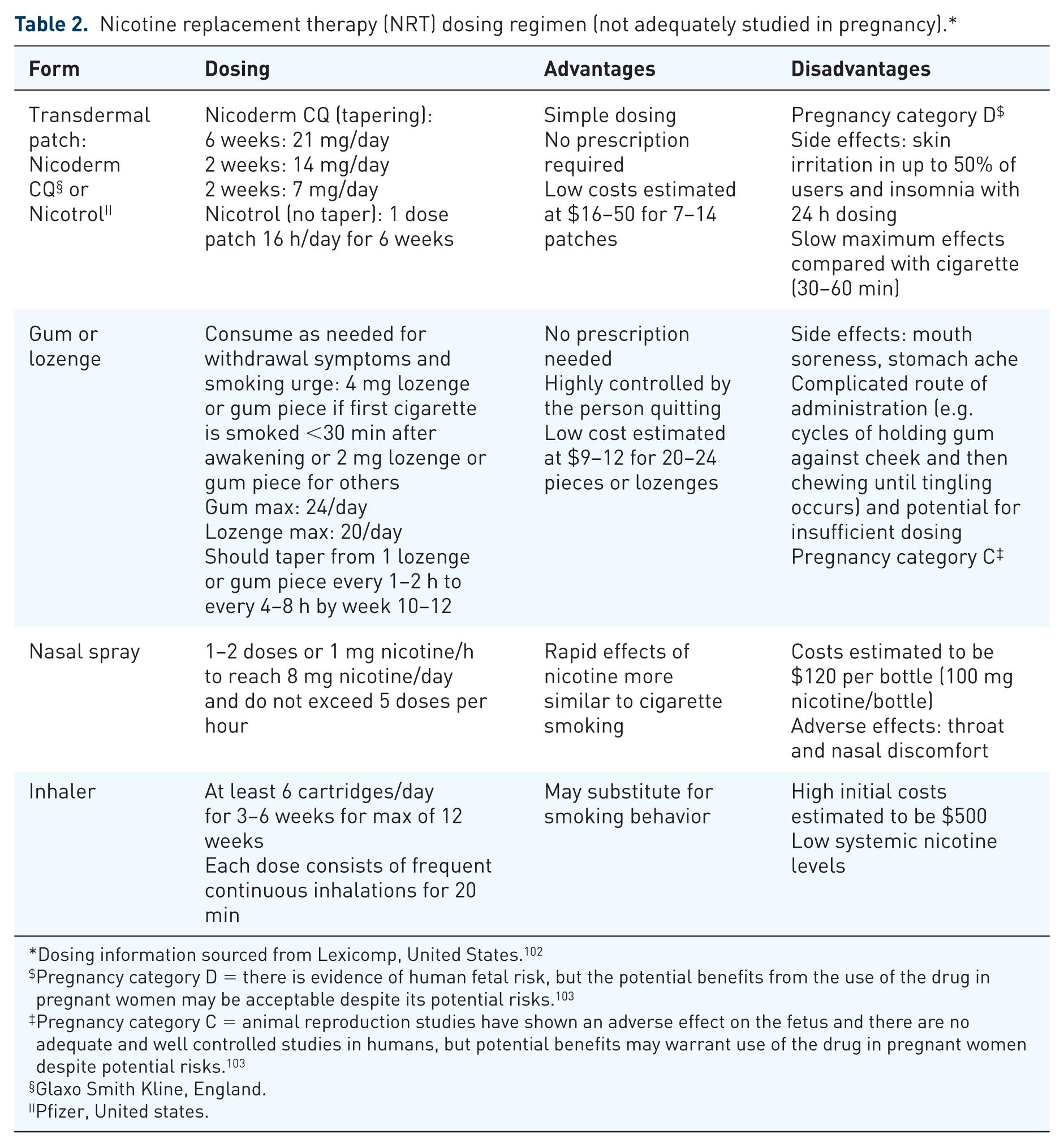
Dosing information sourced from Lexicomp, United States. 102
Pregnancy category D = there is evidence of human fetal risk, but the potential benefits from the use of the drug in pregnant women may be acceptable despite its potential risks. 103
Pregnancy category C = animal reproduction studies have shown an adverse effect on the fetus and there are no adequate and well controlled studies in humans, but potential benefits may warrant use of the drug in pregnant women despite potential risks. 103
Glaxo Smith Kline, England.
Pfizer, United states.
Metabolism of cotinine, the primary metabolite of nicotine, is accelerated in pregnancy, 104 thus systemic levels of nicotine from NRT dosing may be too low to effectively curb withdrawal symptoms and cravings. Conversely, lower systemic nicotine levels limit fetal exposure. Studies indicate that, compared with smoking, NRT formulations including gum, nasal spray, and patches are associated with lower serum nicotine and cotinine levels during pregnancy. 105 Impacts of NRT on maternal and fetal cardiovascular systems appear similar to smoking (e.g. maternal heart rate and blood pressure, and fetal heart rate). 106 A recent meta-analysis of nine randomized controlled trials (RCTs) testing the effectiveness of NRT in pregnancy found mixed results. 28 Among eight trials investigating counseling alone, or with NRT, or with placebo found increased cessation among the NRT group (RR 1.43; 95% CI 1.03–1.93). Subanalyses of placebo-controlled trials demonstrated that NRT was not more effective than placebo (RR 1.28; 95% CI 0.99–1.66). These trials did not explore NRT versus placebo alone.
Insufficient evidence exists to confirm safety and efficacy of NRT in pregnancy. The American College of Obstetricians and Gynecologists (ACOG) guides providers to administer NRT with close supervision and only when total cessation is the goal; 83 assessment with nicotine biomarkers such as urine cotinine may be helpful. 107 Congruent with USPSTF guidelines, available evidence suggests women smoking fewer than five cigarettes per day may benefit more from behavior therapy than NRT, while smokers with heavier nicotine addiction benefit from the addition of NRT. 38
Bupropion HCL (Zyban, Wellbutrin, Glaxo Smith Kline, England (manufactures all of these drugs))
Bupropion is an antidepressant and a FDA category C drug in pregnancy, with demonstrated efficacy in tobacco cessation and no known adverse fetal effects.108–110 Bupropion’s primary pharmacokinetic advantages are to increase the availability of dopamine and act as a partial nicotine acetylcholinergic receptor agonist blocking the effect of nicotine.101,111 The former serves to protect the fetus from nicotine exposure. Bupropion-aided cessation is associated with limited depressive symptoms, cravings, 112 and weight maintenance, which may be particularly attractive to women, although weight gain post discontinuing treatment is similar to other cessation methods. 82 Bupropion requires approximately a week to achieve a steady state and women should begin treatment within 2 weeks of expected quit date at a dose of 150 mg twice daily (Table 3). Treatment should last 7–12 weeks, with cessation less likely to occur among those still smoking after 7 weeks. 112 The most common negative side effects of bupropion include dry mouth, insomnia, and nausea.112,113 Titrating the total daily dose and avoiding taking the second dose near bedtime may limit some side effects. 114 Bupropion and its active metabolites are found in umbilical venous plasma at concentrations lower than maternal plasma concentrations. 115 Two observational studies found increased risk of left-sided outflow cardiac defect (n = 10; adjusted OR 2.6; 95% CI 1.2–5.7) and ventricular septal defect (OR 1.6; 95% CI 1.0–2.8), but these results should be interpreted cautiously as participants were taking bupropion for depression not smoking cessation, samples were small, and confidence intervals were large.110,116 Overall, research demonstrates bupropion is not teratogenic.108,109
Smoking cessation pharmacotherapy: typical dosing regimen.
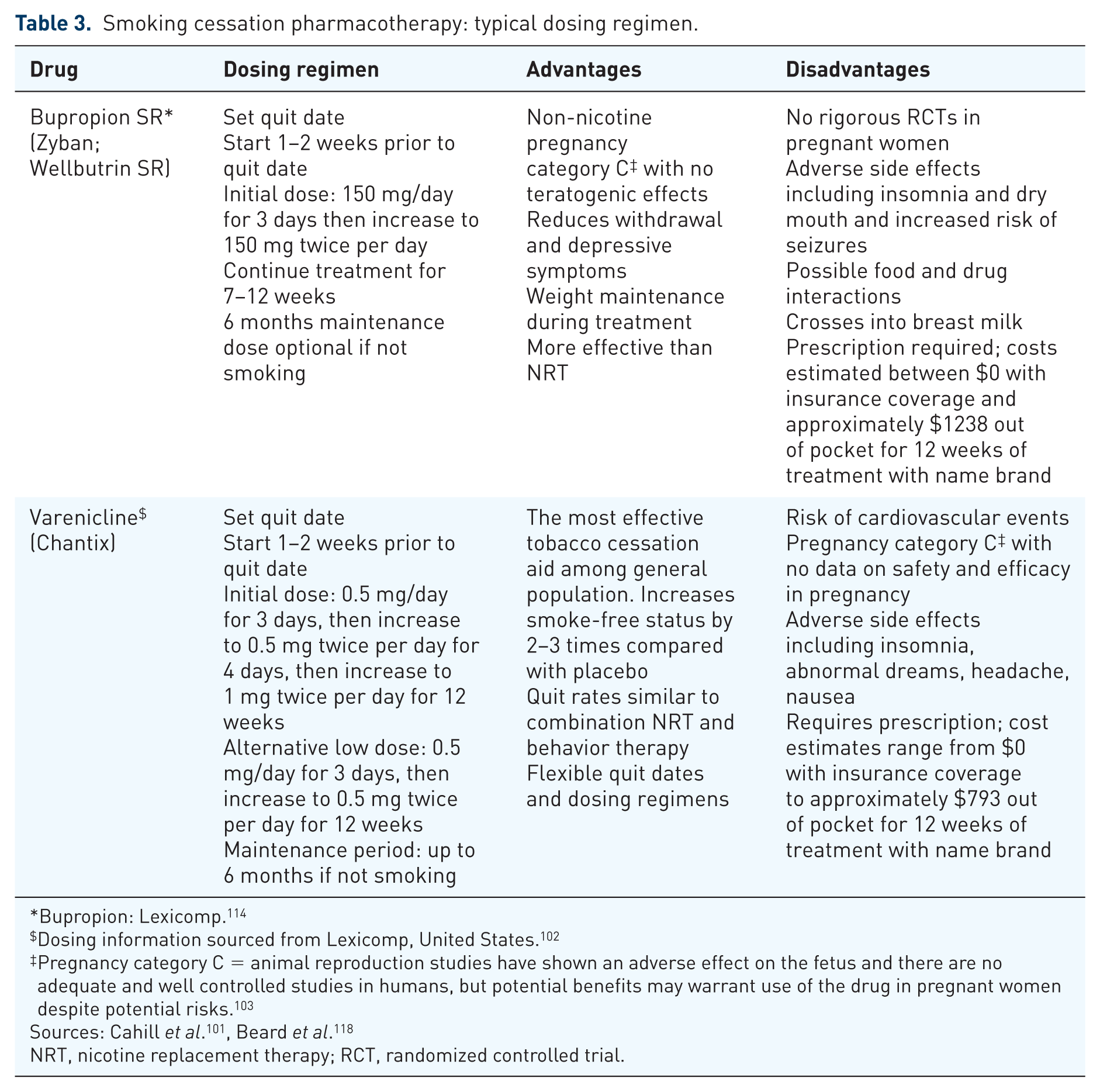
Bupropion: Lexicomp. 114
Dosing information sourced from Lexicomp, United States. 102
Pregnancy category C = animal reproduction studies have shown an adverse effect on the fetus and there are no adequate and well controlled studies in humans, but potential benefits may warrant use of the drug in pregnant women despite potential risks. 103
NRT, nicotine replacement therapy; RCT, randomized controlled trial.
The effectiveness of bupropion only for smoking cessation in pregnancy is not well studied, with limited existing data from observational studies108,119 and one RCT unable to meet sample size to show differences; recruited 11 women of 50 planned. 120 Berard and colleagues 119 reported on results from a population-based cohort study comparing cessation rates and birth outcomes among pregnant smokers receiving NRT (n = 316), bupropion (n = 72), or no intervention (n = 900). All groups were enrolled at the beginning of pregnancy. Women were dispensed bupropion for smoking cessation only in the first trimester (e.g. pregnant women with depression were excluded). Compared with no intervention, women taking bupropion for an average of 87 days had greater cessation (81% of women quit versus 0%), and lower preterm birth rates (adjusted OR 0.12; 95% CI 0.03–0.50). Outcomes for the NRT group were similar to those who took bupropion, except NRT was additionally associated with significantly less small-for-gestational-age births. Upon discontinuing bupropion, 60% of women remained smoke free through birth. 119
Recently, Nanovskaya, and Oncken and colleagues 121 tested whether combined bupropion and individual therapy could reduce withdrawal symptoms and improve abstinence rates among 65 pregnant daily smokers. Women randomly allocated to receive standard individual therapy and 150 mg of bupropion twice daily had reduced withdrawal symptoms compared with the placebo group (1.5 ± 1.1 versus 2.1 ± 1.2, p = 0.02) and greater overall abstinence rates (19% versus 2%, p = 0.003). Urine cotinine provided weak evidence of lower tobacco exposure among the bupropion group with large standard deviations (348 ± 384 ng/ml of cotinine versus 831 ± 727 ng/ml of cotinine, p = 0.007). Abstinence rates at 1 week post treatment were not significantly different. These results confer little confidence in the use of bupropion as a cessation tool in pregnancy.
Varenicline (Chantix, Pfizer, United States)
Varenicline is an FDA-approved smoking cessation aid, but an FDA pregnancy category C drug with unknown safety and efficacy among pregnant women (Table 3). Varenicline is a partial agonist of the α4–β2 neuronal nicotinic acetylcholine receptor (nAChR) and full agonist of the α7 nAChR, which explains its association with limited cravings and withdrawal symptoms as well as believed ability to block fetal exposure to nicotine. Varenicline has proven efficacy for long-term cessation among nonpregnant populations and better long-term cessation rates than NRT or bupropion alone.101,112 Starting in 2009, the FDA placed a black box warning regarding the association between varenicline and serious neuropsychiatric events including suicide. Since then, multiple large observational studies and RCTs have been unable to confirm an association between varenicline and neuropsychiatric events among those with and without history of psychiatric disorders. 113 As a result, the FDA has removed the black box warning from varenicline (The United States Department of Health and Human Services (DHHS)-FDA). Adequate trials of safety and efficacy are still needed among pregnant populations.
Other pharmacologic therapies
The following non-FDA-approved drugs have been inadequately studied or found to have low efficacy and are not recommended by the authors of this review. Clonidine (Catapres, Kapvay, Boehringer Ingelheim, Germany), an antihypertensive drug has shown limited efficacy in aiding withdrawal symptoms or improving quit rates; not always superior to placebo. Side effects include drowsiness, fatigue, and postural hypotension, and close monitoring by a health care provider is required.122,123 Nortriptyline (Pamelor, Aventyl HCL, Mallinckrodt, Inc., United States) is a tricyclic antidepressant that may limit severity of withdrawal-related symptoms (e.g. depression). A Cochrane review reported results from two RCTs demonstrating the effectiveness of nortriptyline in smoking cessation and limited side effects, but safety in pregnancy is unknown. 122 Selective serotonin reuptake inhibitors (SSRIs) are a class of widely used antidepressants that have not shown effectiveness in smoking cessation. 124 Additionally, some SSRIs have been linked to congenital anomalies of the cardiovascular and central nervous system. 125
Cytisine is a nicotine receptor partial agonist and has been used outside the US for tobacco cessation since the 1960s (e.g. Bulgaria). Cytisine was found to be four times more effective than placebo at tobacco cessation by Cochrane systematic review, 126 and significantly improved abstinence at 6 months by nonrandomized trial and combined with counseling. 127 Side effects of cytisine are similar to previously reported pharmacological agents: headache, insomnia, irritability, nausea, restlessness. 118 Additionally, based on WHO criteria (ratio of per capita gross domestic product to cost per life year gained), cytisine is the most affordable pharmacological intervention for smoking cessation across low- to high-income countries. 128 OncoGenex Pharmaceuticals, Inc., the National Center for Complementary and Integrative Health, and others are currently collaborating to study cytisine as a smoking cessation tool with phase III trials expected to start in 2018. 129
Nicotine vaccines are under development. 118 These vaccines are proposed to block nicotine’s activation of dopamine-releasing receptors in the brain. Currently, no evidence supports the effectiveness of two different potential vaccines.118,122
Harm reduction
Needle exchange programs are a routine example of harm reduction, where transmission of blood-borne pathogens is reduced in intravenous drug users who freely exchange dirty for clean needles. 130 Alternative methods of nicotine delivery (e.g. ENDS) and vitamin supplementation are two harm reduction approaches that may limit fetal exposure to nicotine or block the negative effects of nicotine on the mother and fetus. NRT, as described earlier, is also a harm reduction approach until complete nicotine cessation is achieved. Additionally, the use of NRT in the presence of smoking cessation decreases maternal and fetal exposure to other toxic compounds found in cigarettes, thus may be preferred over continued smoking. Concerning this point, limited recent data showed no significant difference in the birthweights of term infants born to light smokers (one to five cigarettes per day) compared with infants of nonsmokers. 131 However, these study results should be interpreted cautiously as only 41 infants were born to light smokers compared with 982 infants born to nonsmokers and smoking status was measured via self report.
ENDS supply nicotine through vaporization of a nicotinic solution. 132 Although pregnant women acknowledge potential harm to fetus from ENDS use, the general perception is that ENDS are a safer alternative to traditional cigarettes. ENDS have been shown to reduce and eliminate exposure to some harmful substances, including CO, and they may assist cessation.39,133,134 Conversely, available data from a systematic review elucidate an array of harmful substances found in ENDS products, including known carcinogens and animal and human studies demonstrating altered gene expression and increased airway resistance. 135 Pisinger and Dossing further caution that substances unique to ENDS such as propylene glycol have unknown risks when inhaled. A Cochrane review 136 found mixed results for effectiveness of ENDS for smoking cessation. ENDS improved abstinence rates at 6 months (n = 662; RR 2.29; 95% CI 1.05–4.96), while no difference in cessation rates were found between ENDS and transdermal nicotine patch users (n = 584; RR 1.26; 95% CI 0.68–2.34) All studies were affected by wide confidence intervals and quality was graded ⩽ low. Pharmacokinetics reveal that ENDS use equates to similar or even greater plasma nicotine levels than traditional tobacco cigarettes. 137 While little to no evidence exists affirming safety and efficacy of ENDS and its vapor content, the literature clearly confirms the maternal and fetal harm of nicotine, including teratogenic effects. In 2019, results should be available from a multicenter trial of long-term efficacy and safety of ENDS among a nonpregnant population. 138
Vitamin C and E administration to pregnant women unable to quit smoking appears to have proximal effects on pregnancy outcomes and distal effects on offspring health burden.139,140 Vitamin C supplementation of 500 mg/day compared with placebo showed a reduction in reported wheezing and improved pulmonary function among infants of mothers who smoked during pregnancy. 139 Among vitamin C and vitamin E treated pregnant smokers there were reduced pregnancy-related complications, including placental abruption and preterm birth, compared with placebo-treated smokers. 140
Other nonpharmacological approaches
Complimentary and integrative health (CIH) practices are rising in popularity and CIH is covered under some state Medicaid plans (e.g. Oregon Health Plan). 141 Pregnant women who smoke may view CIH practices as a safe alternative to pharmacological aids for smoking cessation. CIH research contains many gaps in knowledge regarding safety and efficacy of tobacco cessation therapies. The objective of most CIH methodologies such as acupuncture is to reduce withdrawal symptoms allowing the user to move towards abstinence. Hypnotherapy is proposed to act on impulse control to aid in smoking abstinence. 142 Cochrane reviews of hypnotherapy, acupuncture, and exercise therapy to aid in smoking cessation have been inconclusive.143–145 To date there is minimal evidence from adequate RCTs or large observational trials to support the recommendation of CIH for tobacco cessation among pregnant women. Considering 20% of pregnant women report receiving acupuncture, 146 and acupuncture has an alternative application for labor induction, 147 more studies should be completed to establish safety and efficacy of acupuncture for smoking cessation during pregnancy.
Conclusion and future steps
While prenatal smoking rates have declined from 16.3% in 1987 to 8.6% today,19,20 significant disparities in smoking exist across geographic regions, and socioeconomic and racial and ethnic groups. Additionally, women have a unique history of smoking uptake, distinct rationale for continued smoking, and accelerated nicotine metabolism compared with men. 19 The tobacco industry also targets women differently in the media and advertising. 148 While more women quit smoking when they become pregnant than at any other time in their lives, 27 over half of women who smoke do not quit during pregnancy 149 and addressing the barriers to cessation for persistent smokers is crucial. Antismoking policies (e.g. smoking bans and taxation) are safe and effective tools for cessation and primary prevention of smoking, however there may be unintended consequences from the social stigma associated with bans and denormalization of smoking. 27 Individual behavioral counseling is the only intervention recommended by the USPSTF as a safe and effective tool for smoking cessation among pregnant women. Other high-income countries such as the United Kingdom offer NRT during pregnancy. 150 While NRT and other pharmacological agents carry potential, the USPSTF and a Cochrane meta-analysis found they lack clear evidence of effectiveness in the pregnant population.28,94
Tobacco addiction is a chronic disease involving a complex interplay between the central nervous system, genetics, the environment, and physical and psychological states. Addiction is positively enforced by activation of the neuronal reward system via rapid release of dopamine in response to nicotine. Without nicotine, withdrawal symptoms arise. This cycle likely plays a critical role in continued smoking despite financial and health costs. Women are more likely than men to report smoking to cope with negative psychological states or emotions including anxiety and depression.12,22 Additionally, women who are socioeconomically disadvantaged, who report food insecurity, or report active post-traumatic stress disorder or history of trauma have increased risk of smoking during pregnancy. Prenatal smoking is also more prevalent among younger women aged 20–24 years old.23,151
Unfortunately, women most vulnerable to smoking have limited access to counseling services through Medicaid, depending on the state in which they reside. Mechanisms to support counseling such as hotlines, text messaging, 152 or nurse home visiting programs 153 require further investigation among pregnant populations. Smoking cessation in pregnancy will likely need to address competing influences from socioeconomic circumstances, media and marketing, and individual biological and psychological factors. Comprehensive and combination approaches such as repeated CBT sessions 90 or reward-based cessation incentives97,154 are important avenues for future research among pregnant populations in the US who face high health disparities. In addition to continued individual cessation efforts, harm reduction via nutritional supplementation may mitigate some of the adverse effects of nicotine in women unable to quit.139,140 Finally, economic and social policy that work to alleviate inequalities (e.g. affordable housing and access to education and services) should also be considered by overarching public health and governmental entities. 38