
Abstract
Objectives:
Several smoking cessation treatments (nicotine replacement therapy and non-nicotine prescription medication) and electronic cigarettes are widely used. We evaluated the adverse events related to smoking cessation treatments and electronic cigarettes in the US Food and Drug Administration Adverse Event Reporting System database.
Methods:
We analyzed reports of adverse events associated with smoking cessation treatment and electronic cigarettes terms dated between January 2004 and December 2016. We used the reporting odds ratio with 95% confidence intervals to detect a signal for each adverse event.
Results:
In total, 8,867,135 reports in the Food and Drug Administration Adverse Event Reporting System database were analyzed. The numbers of adverse events for nicotine replacement therapy (transdermal, buccal, oral, and respiratory administration) were 1673, 1016, 425, and 56, respectively. Nicotine replacement therapy (transdermal, buccal, and oral) demonstrated adverse events of nausea, nicotine dependence, and dizziness. For nicotine (transdermal) exposure, the top 5 adverse events reported were nausea (149 cases, reporting odds ratio: 2.28 (95% confidence interval: 1.92–2.69)), dizziness (132 cases, reporting odds ratio: 3.04 (95% confidence interval: 2.54–3.63)), application site erythema (108 cases, reporting odds ratio: 32.52 (95% confidence interval: 26.74–39.55)), headache (98 cases, reporting odds ratio: 1.84 (95% confidence interval: 1.50–2.25)), and dyspnea (94 cases, reporting odds ratio: 1.93 (95% confidence interval: 1.57–2.38)). Many cases of improper use of nicotine replacement therapies were reported. Nausea, depression, abnormal dreams, insomnia, and other adverse events were reported for varenicline. Insomnia, rash, anxiety, and dizziness were reported for bupropion. We observed electronic cigarettes–related adverse events such as dizziness, dyspnea, nausea, heart rate increased, and tremor.
Conclusion:
Our findings suggest that an association exists between nicotine-related adverse events and nicotine replacement therapy. Healthcare professionals should closely monitor smokers trying to quit nicotine use for the misuse of nicotine replacement therapy. These findings may be informative to healthcare professionals in order to improve the management of smoking cessation treatment.
Keywords
Introduction
Tobacco use is a risk factor for cardiovascular disease, stroke, cancer, and chronic respiratory diseases and is a major global public health threat.1,2 Guidelines by the US Public Health Service recommend pharmacotherapy to help smokers quit, unless contraindicated. 3 The management of withdrawal symptoms is one of the largest problems for smokers trying to quit smoking.4–6 Several smoking cessation treatments (SCTs) have been approved by the US Food and Drug Administration (FDA). These include nicotine replacement therapy (NRT) (in the form of transdermal, buccal, oral, respiratory, and nasal administration) and non-nicotine medications such as varenicline and bupropion. The cessation rates with proper usage of SCTs were double compared to those with placebo treatments.7,8 The American Cancer Society (ACS) 9 recommends that clinicians advise their patients to use FDA-approved cessation aids that have been proven to be effective.
NRT reduces the motivation to use cigarettes and physical dependence through delivery of nicotine without exposure to harmful combustion products. In general, plasma nicotine concentrations with NRT are lower than those with cigarettes. 10 In the case of nicotine patches, the nicotine plasma concentration can become high when the patch is worn for a long time. Oral NRTs such as gum and inhalers deliver nicotine in relatively low levels to the blood. Nasal irritation often produces mild burning, sneezing, stinging, and cough during the initial usage of nicotine nasal spray. Adverse events (AEs) related to nicotine might occur with NRT; however, the differences in AE onset profiles among NRT forms are not clear.
Varenicline is a non-nicotine prescription α4β2-nicotinic receptor partial agonist that relieves nicotine withdrawal symptoms. Major AEs of varenicline are nausea, abdominal pain, vomiting, headache, and insomnia.8,11 Neuropsychiatric AEs such as depression, anxiety, hallucination, and suicide have been reported. Bupropion is a relatively weak inhibitor of the neuronal uptake of norepinephrine and dopamine and a nicotinic acetylcholine receptor antagonist.12,13 Bupropion reverses the negative effect associated with nicotine withdrawal. 14 Insomnia, nausea, vomiting, and dizziness are often reported for bupropion. 15
Recently, electronic cigarettes (ECs) and electronic nicotine delivery systems (ENDS) have become a popular nicotine replacement. ECs are battery-powered nicotine delivery systems. Most ECs deliver a nicotine-containing aerosol of ultra-fine particles by heating a solution containing propylene glycol or glycerin, nicotine, flavorings, and other chemicals.16–18 However, ECs are not regulated and have not been confirmed as a safe and effective cessation aid. Organizations such as the American Lung Association have expressed concern regarding the potential health risks of ECs and ENDS. 19 Major AEs associated with EC use include pneumonia, congestive heart failure, seizures, and tachycardia; minor AEs include respiratory symptoms, headache, eye irritation, nausea, cough, and sore throat/irritation.20,21 A policy statement from the American Heart Association indicated that common minor AEs of ECs include throat and mouth irritation, dry cough, nausea, and vomiting. 17 FDA regulatory action supports the need to investigate the AE profiles of ECs. The FDA Center for Tobacco Products (CTP) receives and reviews reports from the Safety Reporting Portal, MedWatch, consumers, and healthcare professionals. The CTP has evaluated AEs associated with e-liquids, EC devices, and exhaled aerosol from ECs and the effects upon non-users exposed to ECs.20,22 The unknown AEs associated with ECs have sparked public health concerns.23,24 However, the relationship between ECs and AEs is still unclear; therefore, we studied the reports of ECs.
Spontaneous reports of AE are used to compile reports of suspected AEs and are available for post-marketing surveillance of products regulated by the regulatory authorities. The Food and Drug Administration Adverse Event Reporting System (FAERS) is the largest and best-known spontaneous reporting system (SRS) database for marketed products, reflecting the realities of clinical practice. 25 Cases are reported by clinicians, pharmacists, other healthcare professionals, patients, and the general public to pharmaceutical manufacturers or to the FAERS database. The FAERS database files are openly available on the FDA website. 26 Regulatory authorities such as the FDA may take regulatory actions to improve product safety and protect public health based on these data.27–29
The purpose of this study was to evaluate the possible relationship among AEs and SCTs and ECs using the FAERS database.
Methods
The FAERS data set from April 2004 to December 2016 that was fully anonymized by the FDA was obtained from the FDA website. 26 The informatic structure of the FAERS database is based on the international safety reporting guidelines issued by the International Council on Harmonization (ICH) E2B. We integrated our database from the FAERS data set using FileMaker Pro 13 software (FileMaker, Inc., Santa Clara, CA), according to ASCII Entity Relationship Diagram that is publicly available from the FDA website. AE reports of NRT were extracted using the following keywords: “nicotine,” “nicotine (transdermal),” “nicotine (buccal),” or “nicotine (oral).” For varenicline, we used “varenicline,” as a generic name together with its trade names “Chantix” and “Champix.” For bupropion, we only used its trade name “Zyban” that is used for smoking cessation. AE reports of ECs were extracted using the following keywords: “eliquid,” “electric cigarette,” “electronic cigarette,” “e-cig,” “e cig,” “electronic nicotine delivery system,” “e-pipe,” “e-cigar,” or “e-hookah.” Product reports were further classified into four categories: primary suspect (PS), secondary suspect (SS), concomitant (C), and interacting (I) drugs, according to their anticipated degree of involvement in AEs. For the analysis, we used reports on NRTs, non-nicotine prescription medication, and EC that were recorded as PS. According to the FDA recommendation, we removed duplicate reports from the same patient in the FAERS database from analysis.
Case report counts of AEs were generated according to the preferred terms (PTs) of MedDRA version 19.0, the Medical Dictionary for Regulatory Activities (MedDRA). 30 This is a database of standardized medical terminology for medical products and devices.
The reporting odds ratio (ROR), an authorized pharmacovigilance index, was calculated using a disproportionality analysis (Figure 1). All reported AEs of interest were defined as “cases” and all reported AEs as “total.” The ROR is the ratio of the odds of reporting specific AEs versus all other AEs for a given product, compared with the reporting odds for all other drugs or products present in the database. To compare one of the index groups with the reference group, we calculated the crude RORs as (a:c)/(b:d). RORs were expressed as point estimates with 95% confidence intervals (CIs). The signal is considered significant when the estimated ROR and the lower limit of the 95% CI are >1. 31 Two or more cases were required to define the signal. 27

Two-by-two contingency table for analysis.
Data analyses were performed using JMP 12.0 (SAS Institute Inc., Cary, NC, USA).
Results
The FAERS database contained 8,867,135 reports for the period from January 2004 to December 2016. After exclusion of duplicate reports, 7,348,357 reports were usable.
NRT
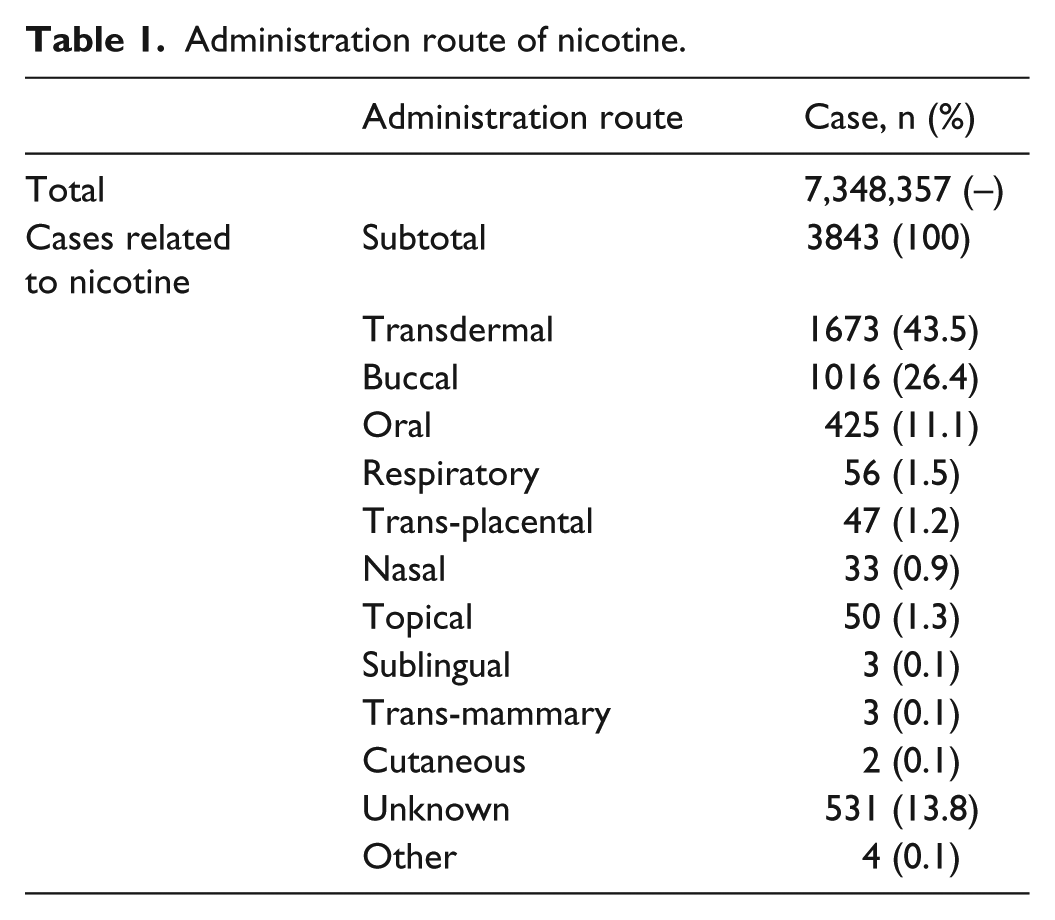
The numbers of AEs for nicotine by transdermal, buccal, oral, and respiratory administration were 1673, 1016, 425, and 56, respectively (Table 1). For transdermal nicotine exposure, top 5 AEs reported were nausea (149 cases, ROR: 2.28 (95% CI: 1.92–2.69)), dizziness (132 cases, ROR: 3.04 (95% CI: 2.54–3.63)), application site erythema (108 cases, ROR: 32.52 (95% CI: 26.74–39.55)), headache (98 cases, ROR: 1.84 (95% CI: 1.50–2.25)), and dyspnea (94 cases, ROR: 1.93 (95% CI: 1.57–2.38)) (Table 2). The numbers of reported cases were drug ineffective (147), treatment noncompliance (128), overdose (87), and product adhesion issue (81), respectively. These reports were not classified as AEs; thus, ROR values were not calculated for these reports.
Administration route of nicotine.
Number of reports and reporting odds ratio of AEs and number of reports of other events by nicotine (transdermal).

CI: confidence interval.
Total number of events reported regardless of nicotine (transdermal).
Case number of events associated with nicotine (transdermal).
Not adverse event.
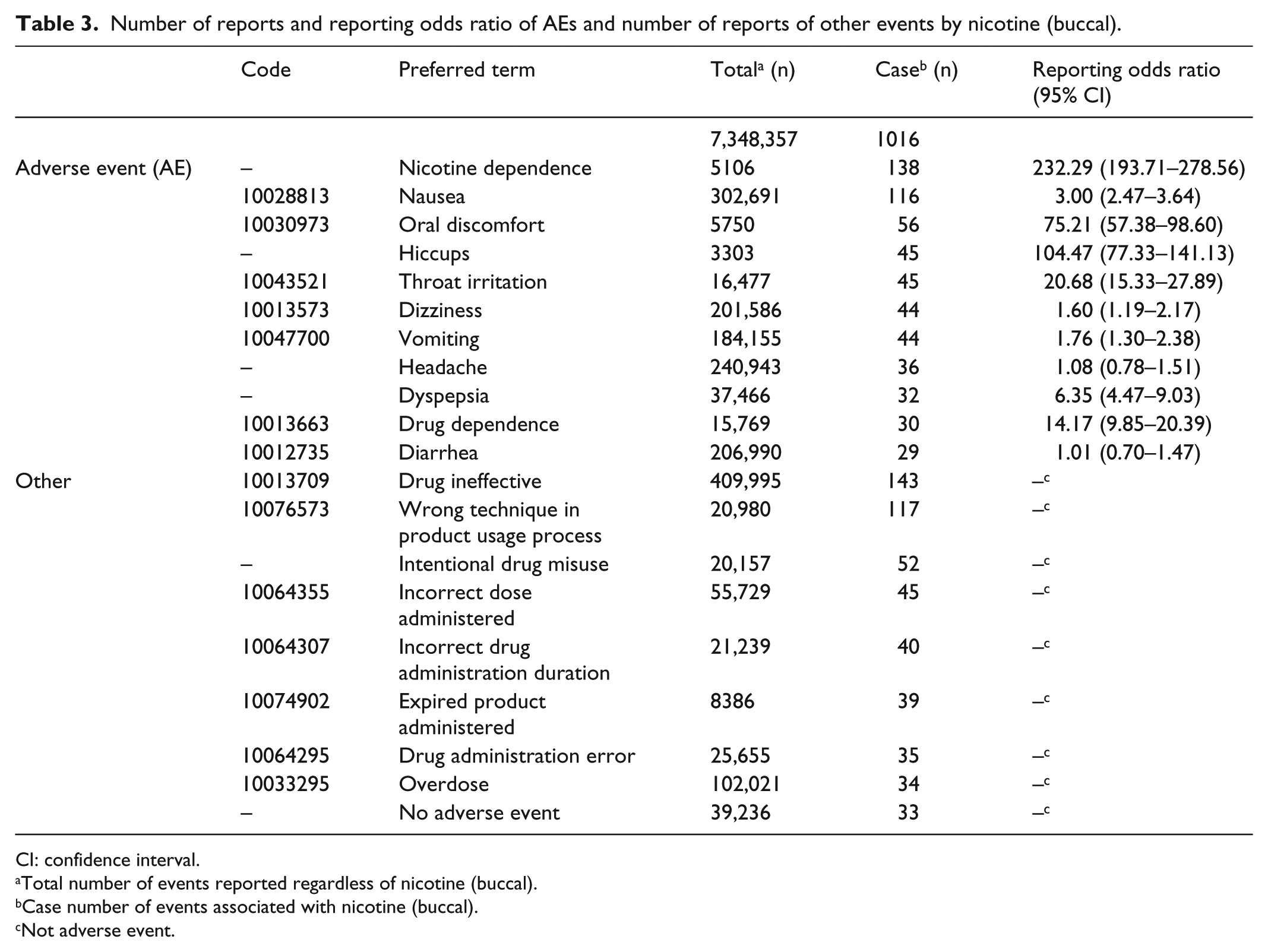
For nicotine (buccal), the top 5 AEs reported were nicotine dependence (138 cases, ROR: 232.29 (95% CI: 193.71–278.56)), nausea (116 cases, ROR: 3.00 (95% CI: 2.47–3.64)), oral discomfort (56 cases, ROR: 75.21 (95% CI: 57.38–98.60)), hiccups (45 cases, ROR: 104.47 (95% CI: 77.33–141.13)), and throat irritation (45 cases, ROR: 20.68 (95% CI: 15.33–27.89)), respectively (Table 3). The numbers of cases were as follows: drug ineffective (143), wrong technique in product usage process (117), intentional drug misuse (52), incorrect dose administered (45), incorrect drug administration duration (40), expired product administered (39), drug administration error (35), and overdose (34).
Number of reports and reporting odds ratio of AEs and number of reports of other events by nicotine (buccal).
CI: confidence interval.
Total number of events reported regardless of nicotine (buccal).
Case number of events associated with nicotine (buccal).
Not adverse event.
For nicotine (oral), the top 5 AEs reported were dependence (200 cases, ROR: 263.66 (95% CI: 217.84–319.12)), nicotine dependence (133 cases, ROR: 672.55 (95% CI: 546.84–827.15)), drug dependence (41 cases, ROR: 49.78 (95% CI: 36.06–68.71)), dizziness (23 cases, ROR: 2.03 (95% CI: 1.33–3.09)), and nausea (19 cases, ROR: 1.09 (95% CI: 0.69–1.73)), respectively (Table 4). We extracted the PTs for the identification of nicotine (oral)-related AEs such as “dependence,” “nicotine dependence,” and “drug dependence,” which are coded according to the terminology prescribed by the MedDRA. From the Introductory Guide MedDRA Version 19.0, each PT is a distinct descriptor (a single medical concept) for a symptom, sign, disease, diagnosis, therapeutic indication, or medical procedure. 32 PTs should be unambiguous and as specific and self-descriptive as possible in the context of international requirements. Therefore, eponymous terms are only used when they are recognized internationally. The granularity/specificity of the PT level is such that clinical pathologic or etiologic qualifiers of the descriptors are represented at the PT level. 32 According to ICH E2B, the international safety reporting guidelines, the spontaneous volunteers only report AEs relying on the definitions provided by MedDRA to the FAERS database. Because detailed patient information about “dependence,” “nicotine dependence,” and “drug dependence” is not intrinsically included in the FAERS database, it was difficult to confirm the exact differences among “dependence,” “nicotine dependence,” and “drug dependence” reported as PTs by volunteers, even though they are healthcare professionals. Therefore, we separately described each result, but further validation of these associations is needed.
Number of reports and reporting odds ratio of AEs and number of reports of other events by nicotine (oral).

CI: confidence interval.
Total number of events reported regardless of nicotine (oral).
Case number of events associated with nicotine (oral).
Not adverse event.
The numbers of reported cases were as follows: intentional drug misuse (142), incorrect drug administration duration (40), drug administration error (39), overdose (22), drug ineffective (21), product quality issue (19), incorrect dose administered (13), and accidental exposure to product (10).
Non-nicotine prescription medication
For varenicline, including Chantix and Champix, the numbers of reports for nausea, depression, abnormal dreams, insomnia, and anxiety were 13,038, 8209, 6944, 5256, and 4994, respectively (Table 5). The RORs (95% CI) were as follows: nausea (5.71 (5.60−5.82)), depression (9.42 (9.20−9.65)), abnormal dreams (81.78 (79.24−84.40)), insomnia (5.07 (4.93−5.22)), and anxiety (5.29 (5.14−5.45)).
Number of reports and reporting odds ratio of AEs and number of reports of other events by varenicline.

CI: confidence interval.
Total number of events reported regardless of varenicline.
Case number of events associated with varenicline.
Not adverse event.
For bupropion, the numbers of reports were as follows: insomnia (162), rash (110), anxiety (109), dizziness (102), and convulsion (101), respectively (Table 6). The RORs (95% CI) were as follows: insomnia (6.95 (5.91−8.18)), rash (2.37 (1.95−2.88)), anxiety (4.95 (4.08−6.02)), dizziness (2.53 (2.07−3.10)), and convulsion (7.67 (6.27−9.38)).
Number of reports and reporting odds ratio of AE and number of reports of other issues by bupropion.

CI: confidence interval.
Total number of events reported regardless of bupropion.
Case number of events associated with bupropion.
Not adverse event.
ECs
For ECs, 27 cases of PS were reported. The numbers of AEs for dizziness and dyspnea were 4 each. The reported numbers of cases of nausea, chest pain, heart rate increased, tremor, disorientation, cough, and wheezing were two for each category. The reported numbers of cases of thermal burn, pulmonary edema, and throat irritation were one for each category. Because ECs are not medication products, we also reviewed other reported terms related to AEs that were not listed in the MedDRA database. The detected terms that were not included in MedDRA were as follows: altered visual depth perception (1), chills (1), device component issue (1), device deposit issue (1), device malfunction (2), device physical property issue (1), fear (1), headache (1), insomnia (1), lung disorder (1), malaise (1), migraine (1), pain (2), product label issue (1), productive cough (1), panic reaction (1), sensation of heaviness (1), and VIIth nerve paralysis (1).
Discussion
NRT
SCTs generally reduce nicotine withdrawal symptoms that interfere with successful cessation. Nicotine from cigarettes is rapidly absorbed into the pulmonary venous circulation, and the nicotine reaches the brain within seconds. 33 Nicotine dependence and abuse liability are influenced by the bioavailability, absorption, distribution, and disposition characteristics of nicotine. 34 All forms of NRT are considered to have almost the same efficacy. 10 Thus, we compared the AE profile based on the type of NRTs using the FAERS database.
Nicotine (transdermal, buccal, and oral) caused AEs such as nausea, nicotine dependence, and dizziness, which might have been caused by nicotine in our study. The RORs of nicotine (buccal) and nicotine (oral) were higher than those of nicotine (transdermal). Based on real-world FAERS data, we considered that the risk of nicotine dependency related to oral or buccal formulas should not be underestimated. When the patient uses transdermal nicotine in the morning, the nicotine level slowly increases over many hours. If a 24-h nicotine patch applied at night causes insomnia or unpleasant dreams, the patch can be removed at bedtime. Although several transdermal nicotine formulations with tapering dosages are available, clinical trials have not demonstrated the effect of smoking cessation by tapering. 35 It is reported that because buccal nicotine formulations have a slow absorption rate and are subject to a first-pass effect, they may be associated with lower dependence. Because oral NRT formulations deliver relatively lower nicotine levels, oral NRT formulations require multiple administrations per day to reduce withdrawal symptoms.
Compliance with recommended NRT use was highest for patches, lower for gum, and very low for sprays and inhalers. 10 The RORs of application site edema and application site pruritus were high. These AE-related application sites might cause a problem of treatment noncompliance. Clinicians should pay attention to cutaneous symptoms. Furthermore, the RORs of oral discomfort and throat irritation were high. These AEs also might decrease patient compliance.
In particular, we should not ignore the risk of misuse of NRTs, regardless of the route of administration (transdermal, buccal, and oral). Many cases of improper use have been reported, such as nicotine overdose for transdermal nicotine; wrong technique in product usage process, intentional drug misuse, incorrect dose administered, incorrect drug administration duration, expired product administered, and drug administration error for buccal nicotine; and intentional drug misuse, incorrect drug administration duration, drug administration error, and overdose for oral nicotine. Healthcare professionals should closely monitor the methods of use of NRT by smokers attempting cessation to prevent misuse.
Non-nicotine prescription medication
Nausea, depression, abnormal dreams, and insomnia have been reported for varenicline (Table 5). We observed that the reported numbers of abnormal dreams and nightmares were ranked in the top 12 and the RORs of both AEs were high (81.78 for abnormal dreams, 20.92 for nightmare) for varenicline (Table 5). However, these AEs were not listed in the top 19 AEs for bupropion (Table 6). The causal relationship between varenicline and these neuropsychiatric AEs is not settled.
Safety concerns regarding the potential for an increased risk of serious cardiovascular AEs for varenicline were demonstrated by a meta-analysis. 36 Another meta-analysis showed no significant increase in serious cardiovascular AEs. 37 We did not observe cardiovascular AEs in the top 20 AEs associated with varenicline (Table 5).
For bupropion, the commonly reported AEs were insomnia, nausea/vomiting, and dizziness in a post-marketing observational cohort study. 15 There was no evidence of an increase in all-cause mortality up to 12 weeks after starting bupropion. 15 The occurrence rate of seizures was approximately 0.1%. 13
Moore et al. 38 reported suicidal behavior and depression in SCTs using the FAERS database. Varenicline showed a statistically significant increased risk of depression and suicidality. Bupropion had relatively smaller increased risks. 38 We also listed suicidal ideation and suicide attempts with varenicline and bupropion (Table 5 and 6). In contrast, suicidality risks did not appear to show a significant increase associated with use of any specific smoking cessation pharmacotherapy. 39 Cigarette smoking itself is considered a predictor of suicidal acts.35,40 Given these conflicting data, we considered that the evaluation of the suicidality risk for SCT is difficult.
Recently, based on the phase 4 randomized, double-blind EAGLES trial, 41 the FDA revised the description of mental health side effects related to mood, behavior, and thinking with varenicline and bupropion to be lower than previously suspected and removed the warning on the box and updated the warning section for both drugs. 42 The results of the trial confirm that the benefits of smoking cessation outweigh the risks of these non-nicotine prescription medications.
It is important to note that our results do not justify not using non-nicotine prescription medication because the benefits and safety of these drugs have been accepted worldwide.
ECs
We observe EC-related AEs such as dizziness, dyspnea, nausea, heart rate increased, and tremor. Some studies have found no increase in heart rate with EC use.43–45 Some studies reported that short-term vaping of ECs resulted in increased heart rate in EC-naive smokers.46,47 ECs containing nicotine may increase heart rate and blood pressure because of systemic absorption of nicotine. However, nicotine content, constituents, and toxicant levels in ECs vary based on solution formulation and the design of the device.48–50 Furthermore, in several studies, plasma concentrations of nicotine from ECs were lower than concentrations in conventional cigarettes.44,51 As the exact brands of ECs were not included in the FAERS reports, we have no information on the concentrations of nicotine involved. Prescribers and users of ECs should carefully monitor cardiovascular events.
We found reports on respiratory, thoracic, and mediastinal disorders, including wheezing, cough, and pulmonary edema. The effect of ECs on respiratory and thoracic functions cannot be ignored. The health effects of ECs should be evaluated in terms of the constituents of EC aerosols and their known toxicities.16,52,53 Propylene glycol and glycerin are the base ingredients of the EC solution. 50 Propylene glycol exposure causes respiratory and eye irritation.16,54 When heated and vaporized, propylene glycol and glycerol form propylene oxide and acrolein, respectively, which can cause upper respiratory tract irritation. 55 Respiratory irritation and bronchial constriction might be caused by propylene glycol aerosols, raising concerns about harm to individuals with asthma and chronic obstructive pulmonary disease. There have been case reports of lung disease caused by ECs.56–58 Polosa et al.,59–61 however, reported that smokers with asthma and chronic obstructive pulmonary disease saw an improvement in symptoms after switching from conventional cigarettes to ECs.
In a clinical trial of long-term EC use, lower rates of AEs were reported from the use of nicotine patches than from the use of conventional cigarettes. 62 Another study found no significant differences in AEs between ECs and nicotine patches. 63
Smoking conventional cigarettes exposes smokers to harmful and potentially harmful constituents that contain thousands of chemicals and can cause serious diseases.64,65 In line with the current tobacco harm reduction strategy, the toxicity of ECs should be determined relative to the known toxicity of conventional cigarettes. 17
The ACS recently released a statement supporting EC use for certain groups. There are smokers not considering quitting smoking and also smokers who do not use FDA-approved SCTs despite clinician advice. For these individuals, switching to exclusive use of the least harmful form of tobacco products such as ECs is preferable to continuing to smoke combustible tobacco products. 9 Of course, the ACS 9 has emphasized that these individuals should be regularly advised to completely quit using all tobacco products such as combustible tobacco and ECs.
One case of a thermal burn was reported in our study. However, the FDA has indicated that at least four reports on burn injuries from ENDS have been published.66,67 The FAERS data set may not have corresponded with the CTP or other clinical reports. However, information from these data sets might be considered of complementary value.
Limitations
Because the FAERS database is subject to various biases, including under-reporting, event misclassification, the lack of a clear denominator (healthy individuals), and possible confounding factors, the RORs offer only a rough indication of the signal strength. The prevalence of reported AEs is influenced by several factors, including smoking status and health history. Because detailed information on the background of relevant persons is not included in the FAERS database, findings should be interpreted with caution. Causality was not established for any of the AEs and cases discussed, and some may be related to preexisting patient history and medical conditions. Therefore, robust epidemiological studies are recommended.
The FAERS database is the largest primary data tool available to the FDA for post-marketing drug AE surveillance and represents an opportunity to interrogate data that reflect the realities of clinical practice. Our results strengthen the already-available evidence, and we consider that our supportive and equivalent results will further add to the existing knowledge.
Conclusion
We first evaluated the association between AE and SCTs and ECs using the FAERS database. NRTs such as transdermal, buccal, and oral nicotine caused AEs such as nausea, nicotine dependence, and dizziness. As many cases of improper use of NRTs have been reported, healthcare professionals should closely monitor smokers attempting smoking cessation for the misuse of NRTs. Nausea, depression, abnormal dreams, insomnia, and other AEs have been reported for varenicline. Insomnia, rash, anxiety, and dizziness have been reported for bupropion. We observed EC-related AEs such as dizziness, dyspnea, nausea, heart rate increased, and tremor. These findings may be informative to healthcare professionals in order to improve the management of SCT.
Footnotes
Declaration of conflicting interests
The author declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: R.U. is an employee of Micron Inc. No additional external funding was received for this study.
Ethical approval
Ethical approval was not sought for this study because the study was an observational study without any research subjects.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partially supported by Japan Society for the Promotion of Science KAKENHI grant number, 17K08452. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.