
Abstract
Background
Little is known about changes in prescribing practices in Australia since the introduction of the direct oral anticoagulants (DOACs). Our objective was to examine if the availability of DOACs has coincided with a change in prescribing of oral anticoagulants in older hospital inpatients with regard to risk factors for stroke and bleeding.
Methods
A prospective observational study was conducted between October 2012 and August 2015 of inpatients aged over 60 years initiated on an oral anticoagulant in a large metropolitan, tertiary referral, public teaching hospital in Australia. Treatment groups were patients who commenced an oral anticoagulant prior to inclusion of DOACs on the formulary and those who commenced after the introduction of DOACs. Subgroup analyses were conducted in patients with atrial fibrillation (AF). Differences in clinical characteristics and risk for stroke and bleeding were calculated using the CHADS2 and HAS-BLED scores, respectively, were examined.
Results
A total of 289 patients were included. Inpatients prescribed an oral anticoagulant after the introduction of DOACs were significantly older, a greater proportion were female and more likely to have had a prior stroke. This was associated with a statistically higher CHADS2 score in the post-DOAC group. Similar findings were observed when limiting the sample to patients with AF. Patients with AF who were at greatest likelihood of having a bleeding event were less likely to be treated with a DOAC.
Conclusion
Since the introduction of the DOACs, patients who may have previously received no therapy or suboptimal treatment were now more likely to be receiving anticoagulation, suggesting an appropriate change in prescribing practice.
Introduction
Ensuring the appropriate and safe use of oral anticoagulants in the older population presents a challenge to clinicians. When prescribing anticoagulants, clinicians must balance the risk of thromboembolism against the risk of haemorrhage. Indications for anticoagulant therapy include stroke and systemic embolic prophylaxis in atrial fibrillation (AF) and venous thromboembolic (VTE) diseases such as deep vein thrombosis (DVT).1,2 Warfarin has been the mainstay of oral anticoagulation to reduce the risk of stroke, however it also increases the risk haemorrhage and its use is complicated due to drug and dietary interactions, narrow therapeutic window and need for regular monitoring. 3 In August 2013, the direct oral anticoagulants (DOACs) were listed on the Australian Pharmaceutical Benefits Scheme for prevention of stroke and systemic embolism in nonvalvular AF and were expected to overcome many of the barriers to prescribing warfarin.4–6 These agents, including the thrombin inhibitor dabigatran and the selective factor Xa inhibitors, rivaroxaban and apixaban, have a rapid onset of action, more convenient dosing regimens, fewer drug interactions and more predictable pharmacokinetics.4–6
Clinical trials have demonstrated that DOACs have equivalent efficacy and safety to warfarin for stroke prevention in AF4–6 and treatment of VTE.7–13 However, despite clinical trial evidence suggesting a reduced risk of bleeding with these agents, concerns remain regarding an increased risk of gastrointestinal (GI) bleeding in clinical practice, particularly in patients aged 75 years and older who are under-represented in clinical trials.4–6,12 Older patients are more likely to have impaired renal function or altered pharmacokinetics that may either result in increased risk of haemorrhage or decreased efficacy, that may also complicate use of the DOACs. 14
Little is known about changes in prescribing practices in Australia since the introduction of DOACs. A recent study in the Australian veteran population (median age 86 years) reported an increase in the overall rate of dispensing in oral anticoagulant therapy since the introduction of the DOACs. Patients initiated on DOACs during the study period were more likely to be men, had fewer comorbid conditions and had less hospitalisations for GI bleed, stroke and myocardial infarction in the 12 months prior to initiation compared with patients who initiated warfarin. 15 Therefore, the objective of this study was to examine if the availability of the DOACs has coincided with a change in prescribing of oral anticoagulants in older inpatients, with a focus on stroke and bleeding risk factors in patients with AF.
Methods
This study was approved by the Royal Adelaide Hospital and University of South Australia Human Research Ethics Committees (Protocol number 120911).
Study design, setting and participants
A prospective observational study was conducted between October 2012 and August 2015 of inpatients aged 60 years or older initiated on an oral anticoagulant (warfarin or DOAC) in a large, metropolitan tertiary referral public teaching hospital in Australia. Treatment groups included those who commenced an oral anticoagulant prior to the introduction of DOACs on the formulary in March 2014 (precohort) and those patients who commenced after the introduction of DOACs (postcohort). The postcohort was further stratified by (a) those who were prescribed warfarin (termed Post-warfarin) and (b) those who were prescribed a DOAC (either dabigatran, rivaroxaban or apixaban, termed post-DOAC). Exclusion criteria were use of an oral anticoagulant in the previous 12 months or significant hearing impairment. During the patient recruitment period, all inpatients prescribed an anticoagulant were systematically identified. For the precohort (new warfarin users only), all international normalised ratio (INR) results conducted in the hospital were sent in a report to the study coordinator (NF) daily and these reports were screened twice a week for patients who appeared to be newly prescribed warfarin. For each patient, this was then confirmed with the ward pharmacist or ward team physician. For the postcohort, those patients initiating warfarin were continued to be identified as described above, in the precohort period. A similar approach was used to identify patients who were initiated on a DOAC. Reports of all DOAC dispensings were generated from the pharmacy department every 2–3 days and reports were screened by the study coordinator (NF) to find patients who appeared to be newly started on a DOAC and confirmed with ward pharmacist or ward team physician. Prospective patients were provided with an information sheet, and informed consent was obtained prior to enrolment in the study. Patients with cognitive impairment had consent provided by appropriate next of kin. Of all identified prospective patients, there was a 40% response rate for inclusion in the study. Patient recruitment and data collection was limited to within 4 weeks from commencing an oral anticoagulant to limit potential for recall bias.
All data were collected from either interview with patients or medical records. Baseline data collection included socio-demographics, medical history (including comorbid conditions and medications), pathology results and frailty using the Reported Modified Edmonton Frail Scale, with a score of ⩾8 considered frail. 16 For patients with cognitive impairment, data were either obtained from the next of kin who provided consent or medical records.
Stroke and bleeding risk assessment
To facilitate prescribing and the assessment of stroke and bleeding risk in patients with AF, clinical guidelines recommend the use of the CHADS2 (or CHA2DS2-VASc) score and HAS-BLED tool.17,18 These are designed to facilitate informed prescribing of oral anticoagulants, to ensure the benefits of anticoagulation outweigh potential bleeding risks. Characteristics for inclusion in stroke and bleeding risk assessment were measured at the time of commencement of oral anticoagulation and included any prior history of a stroke or bleed prior to initiation.
We used the CHADS2 score to assess stroke risk. 19 The individual components of the CHADS2 score include: congestive heart failure (one point), hypertension (one point), age ⩾75 years (one point), diabetes mellitus (one point), stroke/transient ischaemic attack (TIA) (two points). The maximum score is 6 and a total score of ⩾2 indicates a high risk of stroke, and oral anticoagulants are recommended for these patients.
The HAS-BLED bleeding risk score provides a practical tool to assess individual bleeding risk of patients with AF to support clinical decision making regarding antithrombotic use. 20 One point is assigned for each individual component, including hypertension, abnormal renal function (dialysis, kidney transplant, creatinine clearance >200 μmol/l), abnormal liver function [cirrhosis or bilirubin more than two times normal or aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase (ALP) more than three times normal], history of stroke, history of bleeding or predisposition to bleeding (anaemia), labile INR (time in therapeutic range <60%) if on warfarin, age >65 years, concomitant antiplatelet or nonsteroidal anti-inflammatory drug (NSAID) use, or alcohol abuse. The maximum score is 9 and a total score of ⩾3 indicates a high risk of bleeding. 20 In the current study, because those patients who were new to warfarin or a DOAC could not have their labile INR measured, everyone included in the study (both pre and postcohorts) scored 0 for labile INR in the calculation of the HAS-BLED score.
For patients with AF, the distribution of bleeding and stroke risk scores and associated predicted risks of bleed and stroke from the HAS-BLED score and CHADS2 score, respectively were calculated.19,21 This is presented as a matrix of the proportion of patients and their individual bleed and stroke risk scores for each of the study cohorts.
Statistical analyses
Descriptive statistics, including frequency calculations, means, medians and interquartile ranges (IQRs) were used to examine demographic and clinical characteristics for each group. Significant differences between the groups were analysed by t tests for continuous variables and chi-squared statistics for categorical variables, between those in the pre-DOAC period with those in the post-DOAC and post subgroups (warfarin users and DOAC users). The post-DOAC subgroups were also compared with each other.
All analyses were conducted using Statistical Package for the Social Sciences (SPSS) version 21 (Chicago, IL, US).
Results
A total of 289 patients were included in the overall study cohort, 153 patients in the precohort and 136 patients in the postcohort. In the postperiod, 65.4% (n = 89) received warfarin, followed by apixaban (n = 34, 22%), rivaroxaban (n = 10, 4.7%) and dabigatran (n = 3, 2.2%). Overall, 54% of the study cohort received an oral anticoagulant for AF, with the majority (87.2%) of DOAC use for AF. The demographics and clinical characteristics at study entry are presented in Table 1. Inpatients prescribed an oral anticoagulant in the postperiod were significantly older, with a median age of 77 years and a higher proportion were female (54.4%) by comparison with the period before the introduction of DOACs. A significantly higher proportion of patients in the postperiod had a prior stroke (27.9%), especially those commenced on a DOAC (n = 20, 42.6%), compared with 16.3% in the precohort. Other comorbid conditions with a significantly higher prevalence in the postperiod included prior falls and connective tissue disorders but fewer patients had anaemia in the postperiod. Consistent with the higher proportion of patients with a prior stroke, the postcohort had statistically significantly higher CHADS2 scores but no significant differences were observed in HAS-BLED scores or frailty scores between the two groups. The postcohort required greater assistance with activities of daily living (ADLs) (Table 1).
Demographic and clinical characteristics of study cohort at study entry (n = 289).
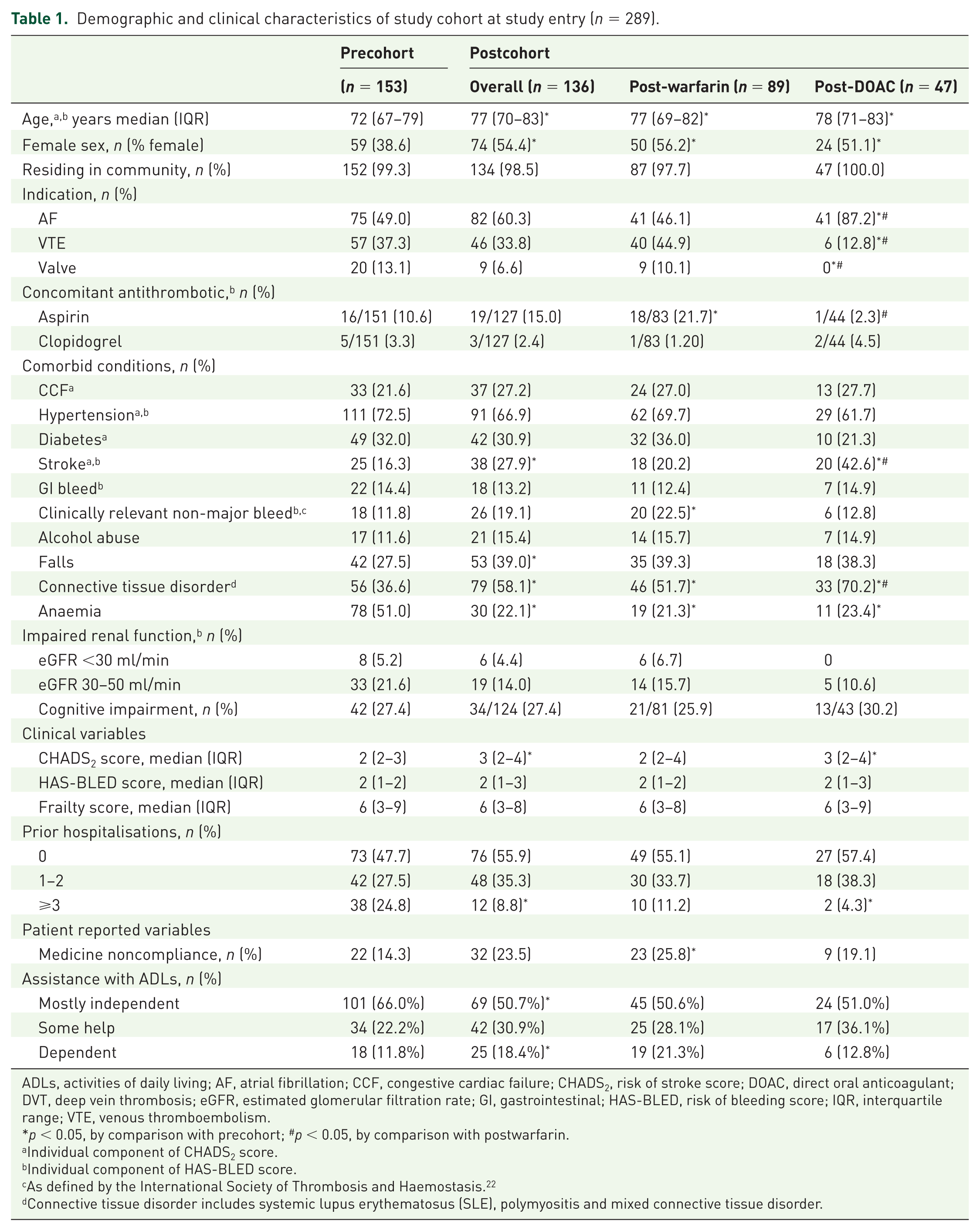
ADLs, activities of daily living; AF, atrial fibrillation; CCF, congestive cardiac failure; CHADS2, risk of stroke score; DOAC, direct oral anticoagulant; DVT, deep vein thrombosis; eGFR, estimated glomerular filtration rate; GI, gastrointestinal; HAS-BLED, risk of bleeding score; IQR, interquartile range; VTE, venous thromboembolism.
p < 0.05, by comparison with precohort; #p < 0.05, by comparison with postwarfarin.
Individual component of CHADS2 score.
Individual component of HAS-BLED score.
As defined by the International Society of Thrombosis and Haemostasis. 22
Connective tissue disorder includes systemic lupus erythematosus (SLE), polymyositis and mixed connective tissue disorder.
Stroke and bleeding risk factors in patients with atrial fibrillation
A total of 157 patients were prescribed an oral anticoagulant for AF; 71 in the preperiod and 86 in the post. Half of the patients in the postperiod were prescribed a DOAC (Table 2). Examination of stroke risk factors showed that in AF patients, the median CHADS2 score was significantly higher [median score 3 (IQR 2–4)] in the postperiod by comparison with the preperiod [median score 2 (IQR 2–3)] (Table 2). Examination of individual components of the CHADS2 score showed that those in the postcohort were significantly older and had an almost three times increase in the proportion of people with a prior stroke (45.1%) by comparison with the precohort (16.3%). In the postperiod, patients who were treated with a DOAC had a significantly higher CHADS2 score and had a greater proportion with a prior stroke, than those patients who received warfarin (Table 2).
Subgroup analysis of stroke and bleeding risk factors in patients with atrial fibrillation (n = 157).
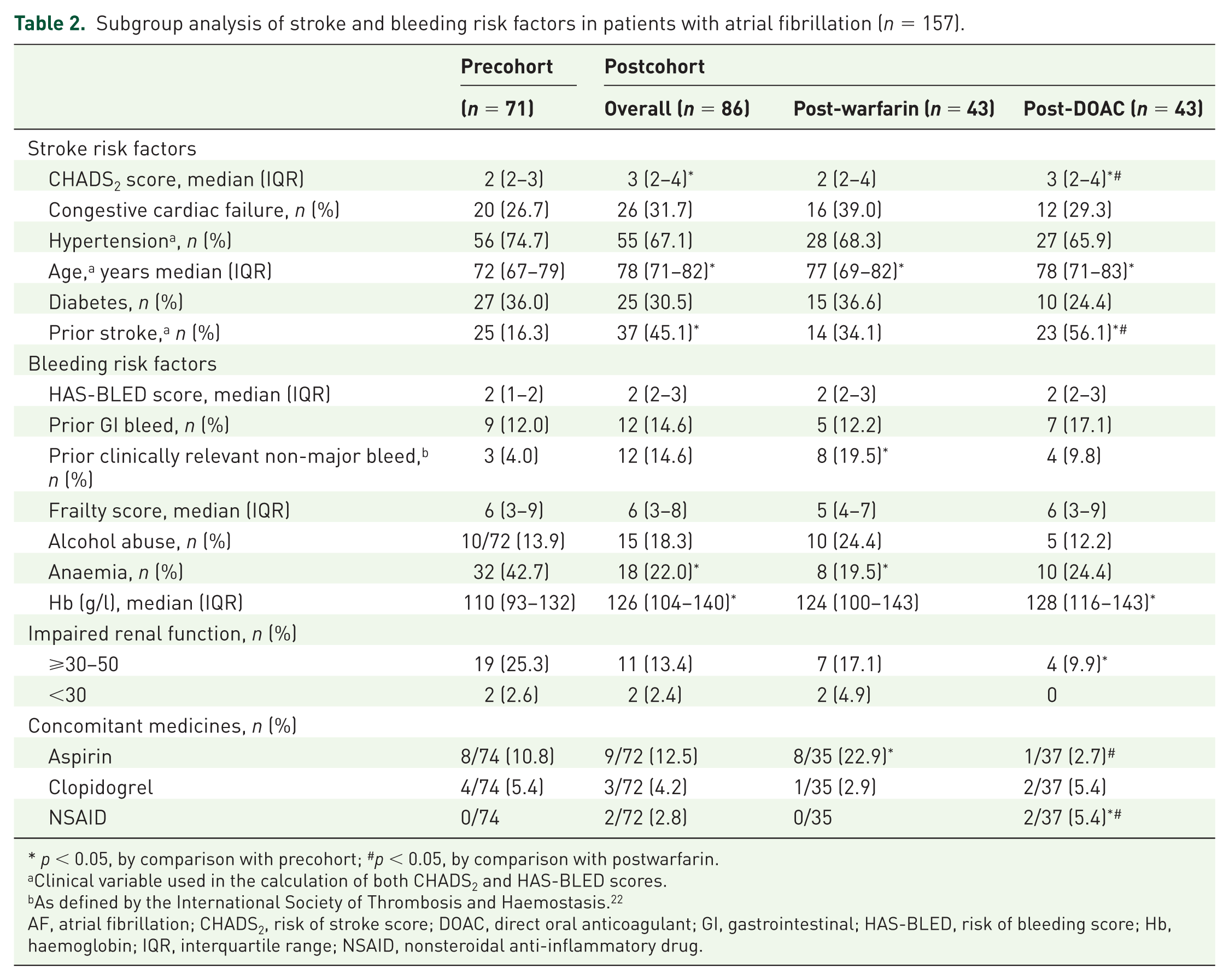
p < 0.05, by comparison with precohort; #p < 0.05, by comparison with postwarfarin.
Clinical variable used in the calculation of both CHADS2 and HAS-BLED scores.
As defined by the International Society of Thrombosis and Haemostasis. 22
AF, atrial fibrillation; CHADS2, risk of stroke score; DOAC, direct oral anticoagulant; GI, gastrointestinal; HAS-BLED, risk of bleeding score; Hb, haemoglobin; IQR, interquartile range; NSAID, nonsteroidal anti-inflammatory drug.
Examination of HAS-BLED scores and bleeding risk factors found that no significant differences were observed in median HAS-BLED scores between the groups (Table 2). Almost 20% of those who received warfarin in the postperiod had a prior clinically relevant non-major bleed by comparison to 10% for those who received a DOAC. The prevalence of patients who received an anticoagulant with anaemia was significantly lower after the introduction of DOACs, with haemoglobin levels being higher in the postcohort. Only 2.7% of patients in the DOAC group had concomitant use of aspirin at discharge compared to 22.9% of patients who received warfarin over the same period. Concomitant use of NSAIDs was significantly higher (5.4%) in the DOAC group than in the warfarin group (Table 2).
Distribution of bleeding and stroke risk scores in patients with atrial fibrillation
Table 3 shows a matrix of the bleeding and stroke risk scores within individuals during the study period for patients with AF. In the precohort, the majority of patients (n = 34, 47.9%) had a higher risk for bleed than for stroke. A similar proportion was observed in the postwarfarin group; n = 21 (48.8%) had a higher bleeding risk than stroke risk, a quarter (n = 11) had equal bleeding and stroke risk and a quarter (n = 11) had a higher calculated stroke than bleeding risk. Introduction of the DOACs resulted in a shift to a greater proportion of patients with a higher risk of stroke (32.6%) and lower risk of bleeding (37.6%) receiving them, by comparison with warfarin users in the pre- and postwarfarin cohorts (Table 3).
Subgroup analysis of bleeding and stroke risk in patient with atrial fibrillation (n = 157). a
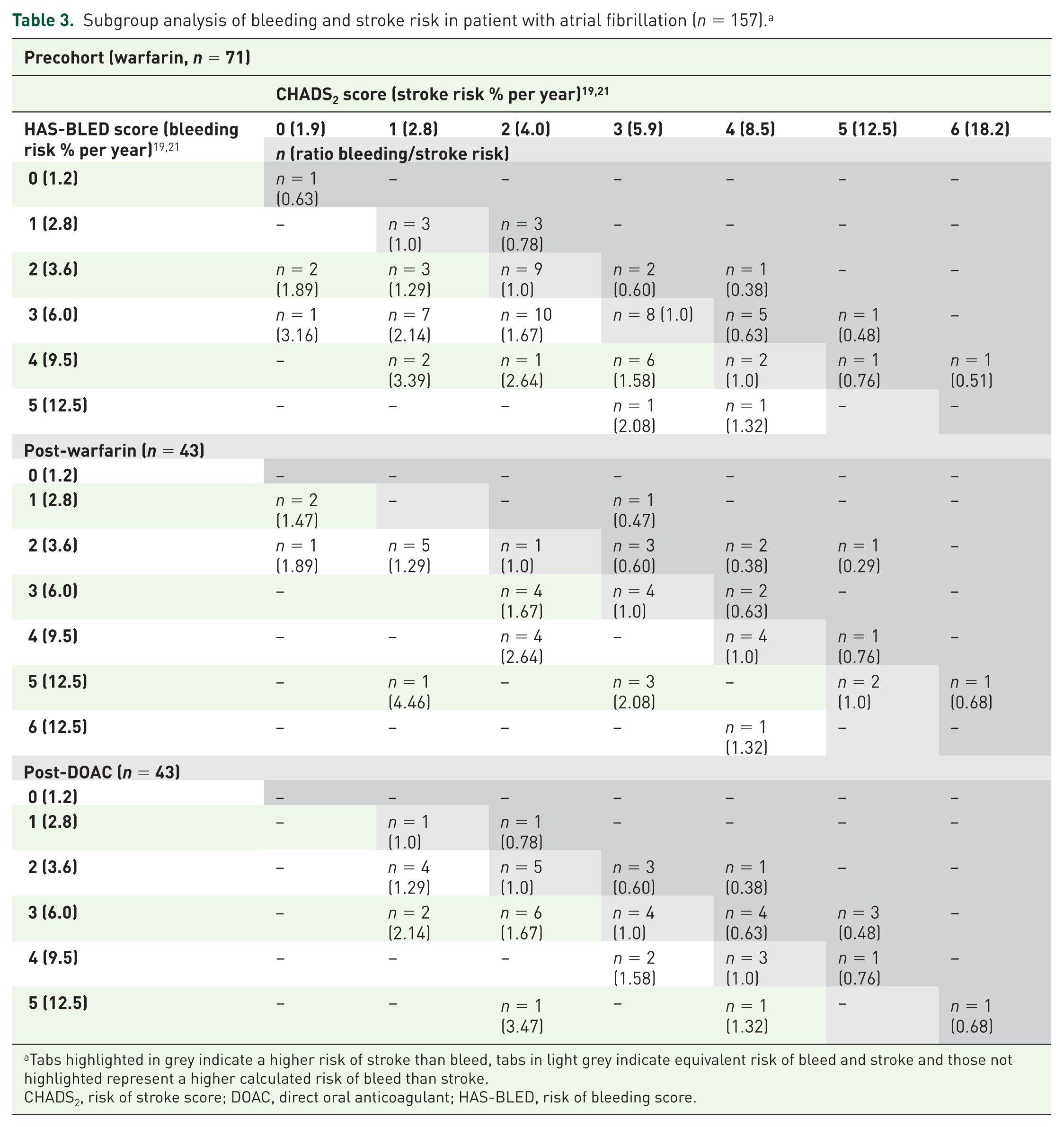
Tabs highlighted in grey indicate a higher risk of stroke than bleed, tabs in light grey indicate equivalent risk of bleed and stroke and those not highlighted represent a higher calculated risk of bleed than stroke.
CHADS2, risk of stroke score; DOAC, direct oral anticoagulant; HAS-BLED, risk of bleeding score.
Discussion
The current study has shown that since the introduction of DOACs, hospital inpatients commenced on an oral anticoagulant are older, and have a higher risk of stroke but similar risk of bleeding and level of frailty. These findings were also observed in the subgroup analysis of patients who received an oral anticoagulant for AF. This suggests that with the introduction of the DOACs, a group of patients that would likely benefit were now receiving anticoagulation, which prior to the introduction of DOACs, may have received no therapy or been sub-optimally treated with anti-thrombotics. A potential patient safety concern is the high proportion of patients with AF who received an oral anticoagulant where the risk of major bleed outweighed the risk of stroke. However, the implications of this with regard to actual bleeding events need to be determined. This highlights the challenge that clinicians face when balancing the risks and benefits of oral anticoagulant therapy in older people. Encouragingly, patients with AF who were at greatest likelihood of having a bleeding event were less likely to be treated with a DOAC, an important consideration due to the limited availability of antidotes to reverse the coagulation effect of the DOACs.
Since the introduction of DOACs in Australia, there has been an overall increase in the proportion of patients receiving oral anticoagulation. 15 Together with our results demonstrating that older patients and those with a higher risk of stroke but not bleeding were more likely to be prescribed an oral anticoagulant after introduction of DOACs, it is highlighted that there is a shift in prescribing for patients who prior, were potentially suboptimally treated. Further, increased awareness and education of the need to treat patients at risk of stroke through updated clinical guidelines at this time, and perceived increased safety and convenience of these newer agents may have also shifted prescribing patterns. Underuse of oral anticoagulants has been identified as an issue among older people, with reports that 30% or more of older patients with AF considered at risk of stroke (defined as a CHADS2 score ⩾2) were not treated with an oral anticoagulant.23,24 In a recent Australian study, 44.3% of hospitalised patients with AF were not prescribed an oral anticoagulant on discharge and the clinical characteristics identified to be predictive of not receiving an oral anticoagulant included increasing age [odds ratio (OR) 0.93, 95% confidence interval (CI) 0.89–0.96], bleeding history (OR 0.57, 95% CI 0.34–0.95) or abnormal renal function (OR 0.33, 95% CI 0.13–0.87). 25 The results of our study suggest that patients with a prior history of stroke are more likely to be receiving anticoagulation therapy since the introduction of DOACs, and that fewer patients may be undertreated in this setting. Similar findings regarding characteristics of patients initiating DOACs have been reported in other studies, with regard to increased stroke risk. Two studies using Danish nationwide registry data from AF patients, initiated on either warfarin or a DOAC, have reported older age and prior stroke were associated with a greater likelihood of being prescribed a DOAC, with a 35% increased likelihood of prior stroke (OR 1.35, 95% CI 1.28–1.43) in those initiated on a DOAC compared with warfarin.26,27 However, contrasting prescribing patterns were reported in a US study of almost 7000 AF patients from a commercial health fund, where preferential prescribing of DOACs to healthier patients (lower stroke and bleeding risk) compared with warfarin users was observed. 28
A recently published Polish study of 1556 patients with AF, reported that patients at high risk of bleeding (defined by HAS-BLED score) were less likely to receive an oral anticoagulant, even if stroke risk (CHA2DS2VASc score) was high. Similar to our findings, they reported that those with a high bleeding risk were less likely to be prescribed a DOAC. 29 However, none of these studies assessed the overall risk of bleed and stroke as in the current study. Using the ratio of the HAS-BLED/CHADS2 scores to estimate the patient’s annual risk of stroke and major bleed, we were able to class treatment as inappropriate when the risk of major bleeding outweighed the risk of stroke. Whilst the proportion of patients with a higher bleeding than stroke risk declined after the introduction of the DOACs, bleeding risk was still higher for half of the study cohort. Prescribers may accept a higher bleeding risk in patients with a definitive indication for anticoagulation (e.g. valves, VTE) where the thrombotic risk is high. However, similar trends were observed in patients prescribed oral anticoagulation for AF indications only and again it is likely that prescribers may be willing to accept a higher bleeding risk because this is potentially reversible, whereas the effects of stroke are permanent and can be debilitating. One study has shown that the average number of excess bleeds for treatment with warfarin in AF over 2 years that was considered acceptable by doctors was 10.3, though there was little consistency. 30 Patients were willing to accept even higher risks of bleeding to avoid a stroke. 30 Hence, assessment of risk of stroke and bleeding with these tools may indicate overall risk, but the decision for a patient may be very specific based on their individual characteristics and preferences.
There were several limitations of this study. Recruitment occurred at a single site, and the results may not be generalisable to other settings or locations. Not all potentially eligible patients were able to be recruited within the within the time period of 4 weeks from commencing oral anticoagulation, due to delays in identifying and contacting the patients in some instances. Recall bias may have also been an issue with regard to self-reporting of medication adherence and health status prior to admission. Whilst the introduction of DOACs in Australia has led to an increase in the rate of dispensing of anticoagulation therapy and types of patients being anticoagulated, 15 which was also observed in the current study, the potential for selection bias was limited by using the same method for patient recruitment between the pre- and postperiods. Similarly, the strategies were similar for patient recruitment in the postperiod for the warfarin and DOAC groups. Renal function was measured by eGFR rather than Cockcroft–Gault calculation due to a lack of weight measurements in many patients and eGFR may overestimate renal function in the older population. HAS-BLED scores may be underestimated in some people, as uncontrolled hypertension could not be evaluated from the data available and has not been validated for DOACs.
Conclusion
This study showed that a significantly increased number of older stroke patients with comparable bleeding risk and level of frailty were being prescribed an anticoagulant, following the introduction of the DOACs. As a consequence, there is potential for a significant improvement in health outcomes, specifically reduced risk of stroke, for this population. Importantly, those patients who were at greatest risk of bleed were less likely to receive a DOAC. Whilst the balance between the risks of stroke versus the risk of bleed is a complex interplay of clinical factors and patient preference, it highlights the need for pharmacovigilance by the prescribing clinician to minimise all risk ensuring the appropriate use of these medicines in clinical practice.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.