
Abstract
Objective:
Depressive symptoms are highly prevalent in residential aged care facilities (RACFs). The prevalence of antidepressant use is increasing but the effectiveness of antidepressants in people with dementia is uncertain. The objective of the study was to investigate factors associated with antidepressant use in residents with and without dementia.
Methods:
This was a prospective cross-sectional study of 383 residents in six Australian RACFs. Data on health status, medications and demographics were collected by trained study nurses from April to August 2014. Logistic regression was used to compute adjusted odds ratios (AORs) and 95% confidence intervals (CIs) for factors associated with antidepressant use. Analyses were stratified by dementia and depression.
Results:
Overall, 183 (47.8%) residents used antidepressants. The prevalence of antidepressant use was similar among residents with and without dementia. Clinician-observed pain was inversely associated with antidepressant use in the main analysis (AOR = 0.56, 95% CI = 0.32–0.99) and in subanalyses for residents with documented depression (AOR = 0.51, 95% CI = 0.27–0.96). In residents with dementia, moderate quality of life was associated with a lower odds of antidepressant use compared with poor quality of life (AOR = 0.35, 95% C I= 0.13–0.95). In residents without dementia, analgesic use was associated with antidepressant use (AOR = 2.34, 95% CI = 1.07–5.18).
Conclusions:
The prevalence of antidepressant use was similar in residents with and without dementia. Clinician-observed pain was inversely associated with antidepressant use but there was no association between self-reported pain and antidepressant use.
Introduction
Depression and depressive symptoms are highly prevalent in residents of residential aged care facilities (RACFs) [Seitz et al. 2010]. The prevalence of major depressive disorder ranges from 5–25% and the prevalence of depressive symptoms ranges from 14–82% [Seitz et al. 2010]. Despite the high prevalence, depression has been under-recognized and under-treated in RACFs. In the United States, an estimated one-quarter of residents with depression do not receive antidepressants [Hanlon et al. 2011]. Possible reasons include staff not being trained to recognize depressive symptoms and fear of adverse drug events (ADEs). Effectively treating depression may be beneficial because depression has been associated with increased morbidity and mortality. Symptoms and factors associated with depression include pain [Ligthart et al. 2013], risk of stroke [Dong et al. 2012], increased disability [Barry et al. 2009], lower quality of life [Hoe et al. 2009], insomnia [Buysse, 2004] and poor glycaemic control [Katon et al. 2013]. Depression has also been associated with aggression in residents with dementia [Menon et al. 2001]. A recent study reported that depressive symptoms were associated with analgesic use in people with Alzheimer’s disease (AD) [Gilmartin et al. 2015]. While depression is associated with poor quality of life [Hoe et al. 2009], antidepressant use may improve quality of life. For example, paroxetine has been shown in a clinical trial to improve most domains of health-related quality of life in community-dwelling older people with depression [Dombrovski et al. 2007]. There has been limited investigation into the association between quality of life and antidepressant use in residents of RACFs.
The prevalence of antidepressant use is increasing in RACFs [Nishtala et al. 2009; Snowdon et al. 2011]. The reported prevalence of antidepressant use in the United States long-term care facilities ranges from 46–60% [Karkare et al. 2011; Shah et al. 2012]. In Europe, the prevalence ranges from 23–45% [Hosia-Randell and Pitkala, 2005; Petek Ster and Cedilnik Gorup, 2011], while in Australia the prevalence ranges from 21–33% [Snowdon et al. 2011]. The reasons for the increasing prevalence are likely to be multifactorial. First, there has been recent awareness that depressive symptoms are under-treated. Second, antidepressants are prescribed for a variety of indications. A recent Belgian study reported that depression was the indication for antidepressant use in just 66% of residents using antidepressants [Bourgeois et al. 2012]. Other indications for antidepressants included insomnia (13.4%), anxiety (6.2%) and neuropathic pain (1.6%).
It is estimated that over 50% of residents in Australian Government-subsidized RACFs have dementia [Australian Institute of Health and Welfare, 2012]. The risk-to-benefit ratio of antidepressant use may be different for residents with and without dementia. The effectiveness of antidepressants for treating depressive symptoms in residents with dementia is uncertain [Nelson and Devanand, 2011; Leong, 2014]. In people with dementia, there is minimal evidence of the effectiveness of antidepressants in reducing depression, and evidence of ADEs [Banerjee et al. 2013]. Investigating antidepressant use in residents with dementia is particularly important because depressive symptoms are common neuropsychiatric symptoms of dementia [Gao et al. 2013]. Pain and depressive symptoms are closely connected to each other [Gilmartin et al. 2015]. Studying the association between pain and antidepressant use is important given the high prevalence of pain in residents with and without dementia [Tan et al. 2015a].
Whilst antidepressants are generally beneficial in alleviating depressive symptoms they are known to be associated with ADEs. Selective serotonin reuptake inhibitors (SSRIs) have been associated with hyponatremia and falls [Coupland et al. 2011]. The risk of falls associated with SSRIs is now thought to be similar to tricyclic antidepressants (TCAs) [Darowski et al. 2009]. Mirtazapine and TCAs are known to cause daytime sedation and TCAs have anticholinergic side effects. Hyponatremia and anticholinergic side effects may cause delirium, which may be misinterpreted as worsening dementia or behavioural and psychological symptoms of dementia. It is uncertain whether antidepressant use is associated with outcomes that residents prioritize such as quality of life, pain and daytime sedation [Edelman et al. 2005]. The objective of the study was to investigate factors associated with antidepressant use in residents with and without dementia.
Methods
Study design and setting
We analysed data from a cross-sectional study of permanent residents of six low-level and high-level RACFs in metropolitan Adelaide and Mount Gambier undertaken in 2014. In Australia, RACFs predominantly cater for people who are unable to continue living independently. The overall study design and methodology have been reported previously [Tan et al. 2014, 2015b].
Participants
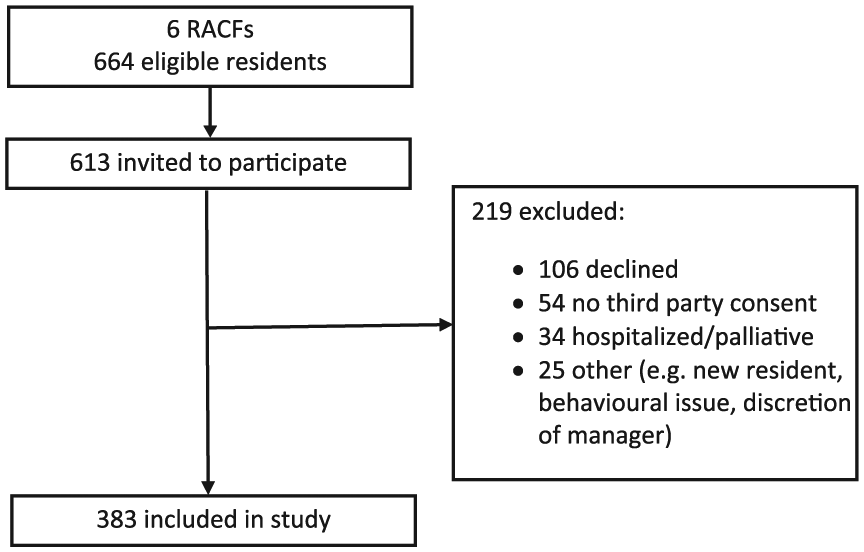
There were 664 eligible residents in the six RACFs. Overall, 613 residents were invited to participate. The resident inclusion criteria were age ⩾65 years of age and ability to participate in English. Residents who were considered to be medically unstable (e.g. delirium) or who were estimated by facility staff to have less than 3 months to live were excluded. There were 219 residents who were excluded (106 residents declined to participate, 34 residents were hospitalized or palliative at time of data collection, 54 residents could not be recruited because third-party consent could not be arranged, and 25 residents were excluded for other reasons including resident behavior or their condition precluded interview, and the discretion of director of care [see Figure 1]). The final sample comprised 383 residents. Participants had similar characteristics to all residents of the six RACFs in terms of age (mean [standard deviation (SD)] 87.5 years [SD 6.2] versus 87.3 years [SD 6.4], p = 0.66), sex (77.5% female versus 78.5% female, p = 0.90) and dementia diagnosis (44.1% versus 46.8%, p = 0.72; dementia diagnosis on among participants is 44.1% and all residents of the six RACFs is 46.8%).
Participant recruitment.
Data collection
All data were collected by three experienced study nurses. The data collection scales included both resident self-report scales and observational scales. For resident self-report scales, residents answered either verbally or by circling the most appropriate response. If a resident was unable to complete one or more self-report scales these were completed by a staff informant or caregiver, with the exception of the FACES Pain Scale Revised (FPS-R) which was only completed by residents. Observational scales were completed by the study nurse or staff informant. Staff informants were required to have known the resident for a minimum of 2 weeks. The Quality of Life in AD (QoL-AD) scale was completed by a registered nurse or care coordinator. Medication data were extracted directly from each resident’s medication administration chart. Clinical diagnoses of dementia, depression, insomnia and anxiety were extracted from the electronic medical records. The level of support received by residents ranged from daily tasks and personal care (low-level care) to 24-hour care (high-level care). All data were collected from April to August 2014.
Antidepressant use
The main outcome measure was antidepressant use. A resident was considered an antidepressant user if he or she was administered an antidepressant in the previous 24 hours [Poole et al. 2015]. This included antidepressants charted for either regular or as-needed use (PRN) use. Antidepressants were defined according to the Anatomical Therapeutic Chemical (ATC) Classification System recommended by the World Health Organization. Antidepressants included nonselective monoamine reuptake inhibitors (N06AA, e.g. TCAs), SSRIs (N06AB), monoamine oxidase A inhibitors (N06AG) and other antidepressants (N06AX, e.g. mirtazapine, venlafaxine).
Clinical factors
Pain was assessed using the Pain Assessment in Advanced Dementia (PAINAD) scale and the FPS-R. The PAINAD is an observational five-item scale completed by clinicians [Warden et al. 2003], and the FPS-R is a single-item resident self-report scale [International Association for the Study of Pain, 2012]. As data were ordinal and non-normally distributed, pain variables were categorized. Residents were categorized as those who experienced no pain and those who experienced any pain. Data on analgesic use were also extracted. Residents who were administered an analgesic in the previous 24 hours were considered analgesic users. This included analgesics charted for either regular or PRN use. Analgesics were defined as paracetamol (ATC code N02BE), nonsteroidal anti-inflammatory drugs (M01AB-H, M01AX01, M02AA, M02AC, N02BA), and opioids (N02A). Low-dose (⩽250 mg/day) aspirin was not classified as an analgesic because it is primarily used as an antiplatelet. Quality of life was assessed using the 15-item QoL-AD scale for nursing homes [Logsdon et al. 2002]. The scale was categorized into tertiles based on the population frequency, with a higher score indicating better quality of life. The six-item Katz Activities of Daily Living (ADL) scale was used to assess activities of daily living [Katz et al. 1963]. Results from this scale were treated as a continuous variable. The aggression domain in the Neuropsychiatric Inventory Nursing Home (NPI-NH) version was utilized to assess agitation or aggression as evaluated by a staff informant [Wood et al. 2000]. Residents were categorized as those with agitation or aggression and those without. Daytime sedation was assessed using the Pasero Opioid-induced Sedation Scale (POSS) and the Epworth Sleepiness Scale (ESS). The POSS is a five-item clinician rated observational scale [Pasero and McCaffery, 2002], and the ESS is an eight-item resident self-report scale [Johns, 1991]. Using the POSS, residents were categorized as drowsy if they scored >1. Using the ESS, residents were categorized as experiencing daytime sleepiness if they scored ⩾11.
Statistical analyses
Data were analysed using the Statistical Package for the Social Sciences (SPSS, version 17.0, Chicago, IL, USA). Descriptive analyses were conducted using a Chi-square test for categorical variables and a Student’s t-test for continuous variables. Logistic regression was used to compute adjusted odds ratios (AORs) and 95% CIs for factors associated with antidepressant use. Self-reported pain and clinician-observed pain were analysed using separate models due to possible multicollinearity. The main analysis included all residents. A series of subanalyses were also conducted. The first subanalysis involved stratifying the sample into residents with and without dementia. The second subanalysis involved restricting the sample to only those residents with a clinical diagnosis of depression. This was done because factors that prompt antidepressant prescribing may differ between people with dementia or depression and those people without. The same covariates used in the main analysis were used in the subanalyses. Multiple imputation with five iterations was used to impute missing values for FPS-R (36.8% missing) and PAINAD (1.0% missing) [Janssen et al. 2010].
Ethical considerations
Potential participants were provided information about the study both verbally and in writing. Written informed consent was obtained from either residents or their guardian, next of kin or significant other. The study was conducted in accordance with the ethical principles for involving people with cognitive impairment in research studies as outlined in the National Statement for Ethical Conduct in Human Research. The study was approved by the Royal Australian College of General Practitioners (RACGP) National Research and Evaluation Ethics Committee and the Monash University Human Research Ethics Committee, Australia.
Results
Of the 383 residents who participated in this study, 297 (77.5%) were female (Table 1). The mean (SD) age of the residents was 87.5 (6.18) years. In total, 169 (44.1%) residents had a dementia diagnosis, 230 (60.1%) a depression diagnosis and 111 (29.0%) had both diagnoses. Of all residents, 113 (29.5%) were observed by clinicians to experience any pain, whilst 230 (60.1%) were recorded as experiencing any self-reported pain. Residents used a mean of 9.3 (4.0) different regular or PRN medications in the previous 24 hours, with 229 (59.8%) residents using nine or more medications. The characteristics of antidepressant users with diagnosed dementia and depression are presented in Table 2.
Characteristics of antidepressant users and nonusers in residential aged care facilities.
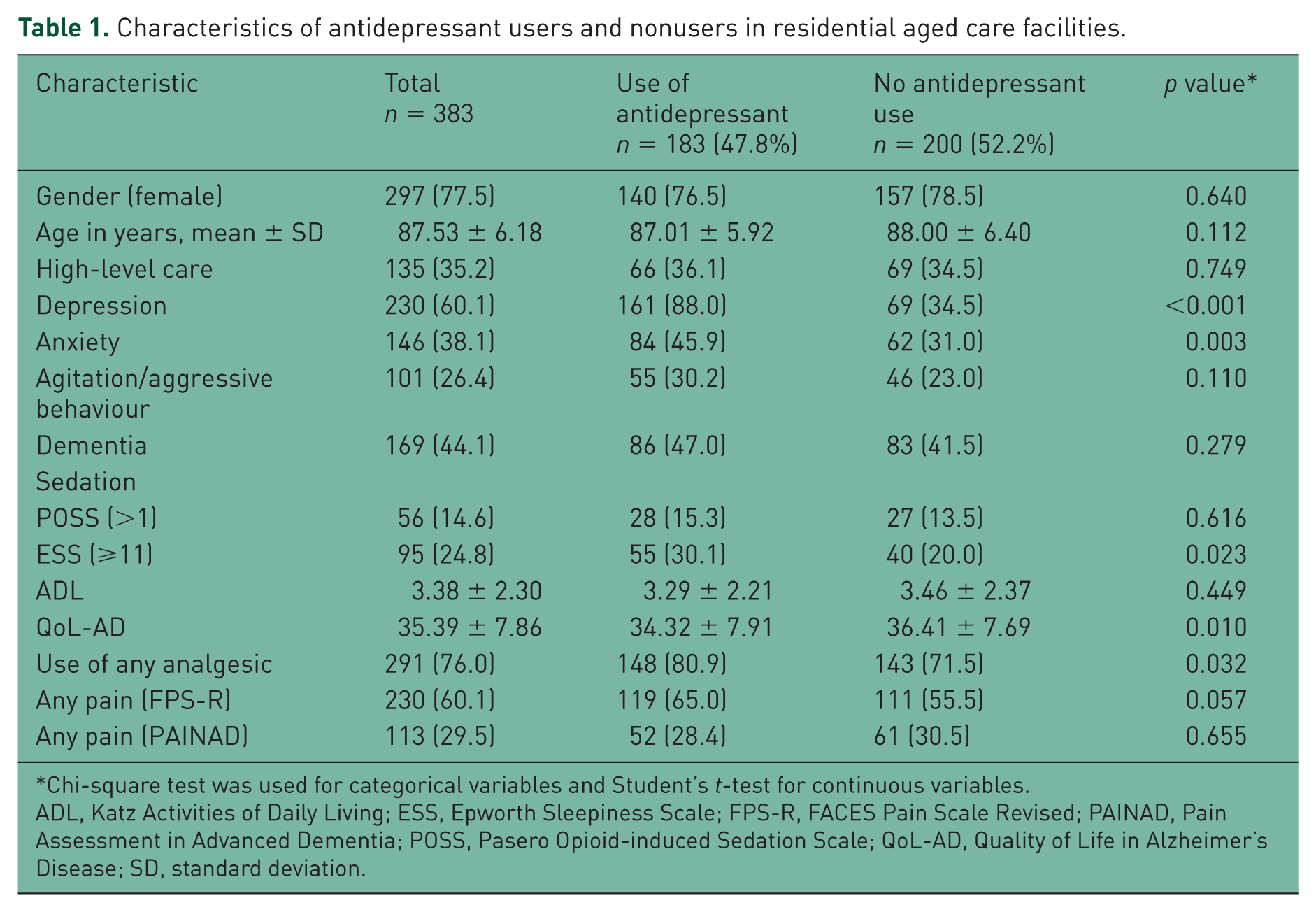
Chi-square test was used for categorical variables and Student’s t-test for continuous variables.
ADL, Katz Activities of Daily Living; ESS, Epworth Sleepiness Scale; FPS-R, FACES Pain Scale Revised; PAINAD, Pain Assessment in Advanced Dementia; POSS, Pasero Opioid-induced Sedation Scale; QoL-AD, Quality of Life in Alzheimer’s Disease; SD, standard deviation.
Characteristics of antidepressant users and nonusers within subgroups of dementia status and depression.
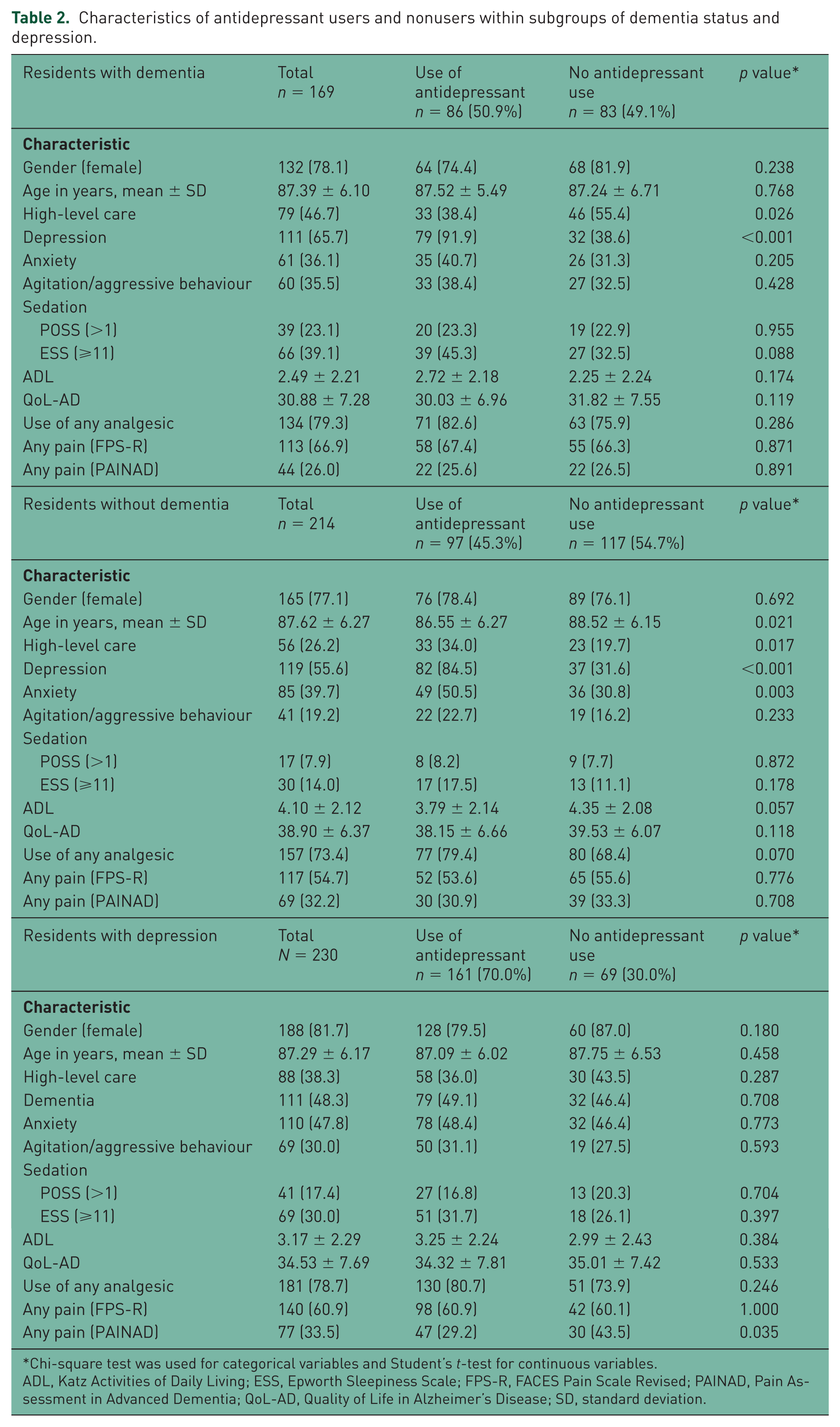
Chi-square test was used for categorical variables and Student’s t-test for continuous variables.
ADL, Katz Activities of Daily Living; ESS, Epworth Sleepiness Scale; FPS-R, FACES Pain Scale Revised; PAINAD, Pain Assessment in Advanced Dementia; QoL-AD, Quality of Life in Alzheimer’s Disease; SD, standard deviation.
In total, 183 (47.8%) residents used an antidepressant. The prevalence of dementia diagnosis was 47% (n = 86) among those using and 41.5% (n = 83) among those not using antidepressants (Table 1). The prevalence of depression diagnosis among antidepressant users was 88% (n = 161) and 34.5% (n = 69) among those not using antidepressants. SSRIs were the most prevalent antidepressants (n = 93, 24.3%). Nonselective monoamine reuptake inhibitors and ‘other antidepressants’ were used by 26 (6.8%) and 66 (17.2%) residents, respectively.
Among all residents there was no association between self-reported pain and antidepressant use. However, those with clinician-observed pain had lower odds of antidepressant use compared with those with no clinician-observed pain (AOR = 0.56, 95% CI = 0.32–0.99) (Table 3). Females were less likely to use an antidepressant compared with males (AOR = 0.52, 95% CI = 0.27–0.99). Those with a clinical diagnosis of depression were more likely to use an antidepressant (AOR = 15.03, 95% CI = 8.38–26.96) (Table 3).
Factors associated with antidepressant use.
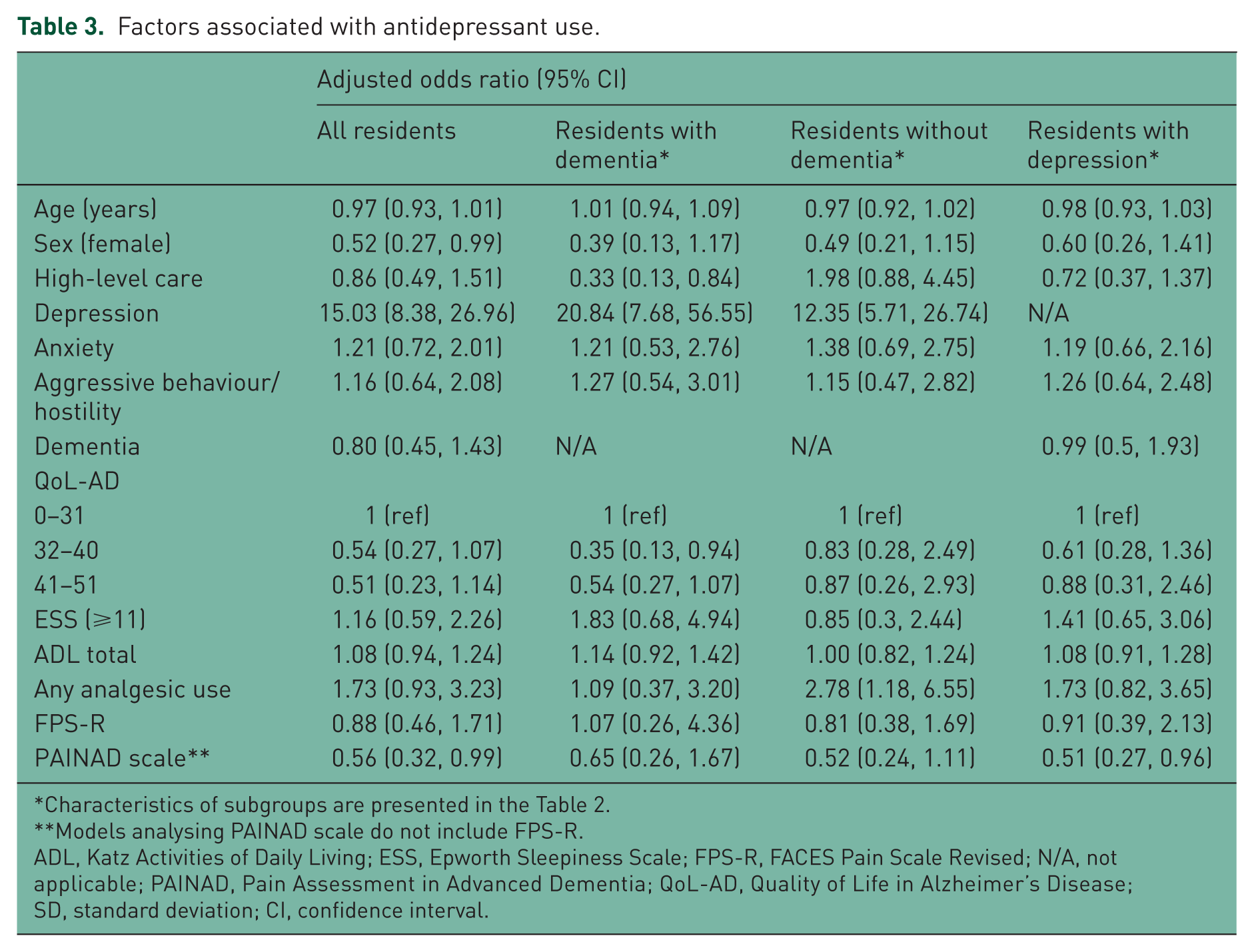
Characteristics of subgroups are presented in the Table 2.
Models analysing PAINAD scale do not include FPS-R.
ADL, Katz Activities of Daily Living; ESS, Epworth Sleepiness Scale; FPS-R, FACES Pain Scale Revised; N/A, not applicable; PAINAD, Pain Assessment in Advanced Dementia; QoL-AD, Quality of Life in Alzheimer’s Disease; SD, standard deviation; CI, confidence interval.
In residents with dementia there was no association between pain and antidepressant use (Table 3). Residents with moderate quality of life compared with those with poor quality of life (AOR = 0.35, 95% CI = 0.13–0.94) had lower odds of antidepressant use, whilst residents with depression compared with those without depression (AOR = 20.84, 95% CI = 7.68–56.55) had higher odds of antidepressant use. High-care residence was inversely associated with antidepressant use (AOR = 0.33, 95% CI = 0.13–0.84).
In residents without dementia there was no association between pain and antidepressant use. However, analgesic use (AOR = 2.78, 95% CI = 1.18–6.55) and depression were associated with antidepressant use (AOR = 12.35, 95% CI = 5.71–26.74).
When the analyses were limited to residents with a clinical diagnosis of depression, there was no association between self-reported pain and antidepressant use (Table 3). However, clinician-observed pain was inversely associated with antidepressant use (AOR = 0.51; 95% CI 0.27–0.96).
Discussion
Our study found that the prevalence of antidepressant use was similar among residents with and without dementia. Antidepressant use was predominately limited to those with a documented clinical diagnosis of depression. Clinician-observed pain was associated with lower odds of antidepressant use but self-reported pain was not associated with antidepressant use.
The prevalence of antidepressant use in our study was similar to previous international studies [Hosia-Randell and Pitkala, 2005; Karkare et al. 2011], but higher than previous Australian studies [Nishtala et al. 2009; Snowdon et al. 2011]. The Australian Institute of Health and Welfare has estimated that 52% of permanent residents in RACFs have depressive symptoms [Australian Institute of Health and Welfare, 2013]. The higher prevalence of antidepressant use in our study may be due to under-recognition of depressive symptoms in previous Australian cohorts. Nevertheless, antidepressants have other indications including insomnia, neuropathic pain, anxiety and neuropsychiatric symptoms. We cannot exclude the possibility that antidepressants were prescribed for dual indications in residents with a clinical diagnosis of depression.
There was no significant difference in the prevalence of antidepressant use in residents with and without dementia. This was consistent with a Dutch study in which the prevalence of depression diagnosis and antidepressant use was similar in residents with and without dementia, although residents with dementia were found to have more depressive symptoms (46.4% versus 22.6%) [Van Asch et al. 2013]. In contrast, a Finnish study reported the prevalence of antidepressant use as nearly three times higher in community-dwelling people with AD compared with those without AD [Laitinen et al. 2015]. These findings highlight potential challenges in the management of depression in residents with dementia, especially considering the apparent lack of evidence of efficacy of antidepressants for treatment of depression in those with dementia and the potential for ADEs [Banerjee et al. 2013].
In the present study, clinician-observed pain was inversely associated with antidepressant use in the main analyses and in residents with depression. This may be partly because of difficulties in identifying pain and differentiating it from depressive symptoms in persons with dementia [Gilmartin et al. 2015]. Antidepressant use may have alleviated these depressive symptoms. In residents without dementia, analgesic use was associated with antidepressant use. This may be explained by the association between pain and depression [Miller and Cano, 2009]. In addition, some antidepressants have beneficial effects in the management of neuropathic pain [Trivedi et al. 2013]. Therefore, the association may be partly explained by antidepressant prescribing for pain management. Conversely, self-reported pain was not found to be associated with antidepressant use across groups. This may suggest that the self-reported scale measures a different aspect of pain compared with the clinician-observed scale. It has been suggested that self-reported measures capture expressive pain behaviour and may thus be influenced by an individual’s mood, compared with observed measures that capture more automatic behaviour [Australian Institute of Health and Welfare, 2012]. In addition, the ability to accurately self-report pain may have been diminished, especially in those with dementia.
Women were less likely to use antidepressants than men, even though women were more likely to have a diagnosis of depression. In contrast, a Finnish study reported women in aged care facilities were more likely to use antidepressants than men [Hosia-Randell and Pitkala, 2005]. Menon and colleagues found that aggressive behaviour was more prevalent in men with dementia compared with women [Menon et al. 2001]. It has also been suggested that antidepressants might be effective for treating other neuropsychiatric symptoms like agitation and aggression [Seitz et al. 2011]. This may partially explain the higher use of antidepressants in men. However, there was no significant difference in the prevalence of aggressive behaviour in men and women with dementia in our study.
In residents with dementia, moderate quality of life was associated with lower odds of antidepressant use compared with poor quality of life. The QoL-AD scale includes a range of items related to resident’s mood [Edelman et al. 2005]. Therefore, it is likely that residents experiencing depressive symptoms received lower QoL-AD scores. Due to the cross-sectional nature of this study it was not possible to determine whether antidepressants caused low quality of life, or whether lower quality of life prompted the prescribing of antidepressants. A previous population-based study suggests that poor health-related quality of life as well as cognitive impairment are associated with future antidepressant use among community-dwelling older people [Poole et al. 2015]. Further longitudinal studies are needed to address this topic among people with dementia living in RACFs.
In this study, 30% of residents did not use antidepressants even though they had a clinical diagnosis of depression. There are a range of possible explanations. First, residents may have been receiving nonpharmacological treatment. Second, residents may have no longer been experiencing any depressive symptoms despite having a depression diagnosis recorded in their medical notes. Finally, residents may have previously taken antidepressants but found them ineffective or have decided to discontinue them due to ADEs.
Strengths and limitations
This was the first study to investigate antidepressant use, pain and quality of life in residents with and without dementia in RACFs. Data were collected using validated and dementia-specific scales, with all medication data extracted directly from each resident’s medication chart [Tan et al. 2014]. We analysed the prevalence of antidepressant administration in the previous 24 hours rather than the prevalence of antidepressant prescribing or dispensing. Medication exposure was reported in accordance with the ROMEO Statement [Poole et al. 2015]. Diagnostic data were extracted from each resident’s current electronic medical record. However, we did not validate the clinical diagnoses listed in the medical records. Because the study was cross-sectional we were not able to determine causality. Although we adjusted our analyses for a range of clinically important parameters, as with all observational studies there remains the possibility of confounding.
We established that the characteristics of residents who participated in the study were similar to all residents of the six participating aged care facilities. However, the results may not be generalized to other settings or countries.
Conclusion
The prevalence of antidepressant use was similar in residents with and without dementia, with antidepressants predominantly used by those with depression. Clinician-observed pain was inversely associated with antidepressant use in all residents and in residents with depression.
Footnotes
Acknowledgements
The authors thank Resthaven staff and residents for their participation in this study. The authors would also like to thank Ms. Jessica Hughes and Ms. Sarah Moawad for their assistance with data management.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Alzheimer’s Australia Dementia Research Foundation via the Resthaven Incorporated Dementia Research Award, with additional funding provided by Resthaven Incorporated. Jenni Ilomäki is supported by an NHMRC Early Career Fellowship.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.