
Abstract
Objective:
The present study aims to analyze community pharmacists’ current knowledge and perceived barriers to adverse drug reaction (ADR) reporting systems in the Eastern region, Alahsa, Saudi Arabia.
Method:
A cross-sectional study was planned from 1 June 2012 to 15 July 2012 among the community pharmacies in the Eastern region, Alahsa. A total of 70 community pharmacists were approached using a cluster sampling method. A self-administered, 28-item questionnaire was used to attain the objectives of the study. Data analysis was done using Statistical Package for Social Science version 13. Relative index ranking was used to identify the top five barriers to the ADR reporting process.
Results:
Response to the survey was 71.43%. In terms of knowledge about ADRs, very few (four, 8.0%) pharmacists were unable to differentiate between the right and wrong definition of ADRs. About 42 (84.0%) pharmacists mentioned that patients often report adverse events. However, 45 (90.0%) were not aware of the ADR reporting system in Saudi Arabia. A deficient professional environment was the main barrier to the ADR reporting process. In addition, unavailability of the reporting forms and poor understanding of the reporting process were common barriers to the reporting process.
Conclusion:
Most of the community pharmacists were unaware of the ADR reporting system in Saudi Arabia. Logistic issues were the main barriers to the ADR reporting process.
Introduction
Globally, adverse drug events remain a major cause of morbidity and morbidity [ Pirmohamed et al. 1998]. In developed countries like the USA, adverse drug reactions (ADRs) ranked as the sixth leading cause of mortality in 2002 [World Health Organization, 2002b]. In the UK, about 6.5% of hospital admissions were due to an ADR [Pirmohamed et al. 2004], while in Sweden 12.0% of the patients’ admissions to internal medicine were the result of ADRs [Mjörndal et al. 2002]. This higher incidence of ADRs results in increased hospitalization and high economic burden to both patient and society [Lindquist, 2004].The key to reducing the consequences of ADRs, that is, morbidity, mortality and cost, is the timely identification and reporting to the relevant in-house, regional or national drug-regulating authorities. Several countries have initiated pharmacovigilance programs for the effective reporting of ADRs [World Health Organization, 2002a; Li et al. 2004; MADRAC, 2002, 2010]. Moreover, recently many countries have also adopted the Spontaneous ADR Reporting System (SADRRS) [MADRAC, 2002, 2010; Meyboom et al. 2002]. SADRRS is considered an ideal approach to prevent the occurrence of ADRs [World Health Organization, 2002a; Hartigan-Go, 2001].
However, there are some disadvantages to SADRRS: it is more applicable to newly launched products and there is a high chance of underreporting [van Grootheest and de Jong-van den Berg, 2002; The Lancet, 2002; Wiholm et al. 2000]. It has been noted that only 10.0% of serious ADRs are reported through SADRRS [Lee and Thomas, 2003]. Furthermore, it is estimated that the rate of reporting of any ADR in hospitalized patients in the USA is as low as 1–6% [Chyka, 2002]. One of the main reasons might be the reliance upon physicians to report the ADR. Certain factors might affect physicians’ attitudes towards ADR reporting, including uncertainty about whether the event is drug induced on not; thinking that the ADR is minor or too well known to report; being too busy to report an ADR; being unaware on how to report the ADR; or believing it is too hard to find the appropriate form [Bateman et al. 1992; Belton et al. 1995; Belton, 1997; Eland et al. 1999; Williams and Freely, 1999; Backstrom et al. 2000]. Considering these flaws as the main limitations of the ADR reporting system, many countries have permitted hospital pharmacists, community pharmacists, nurses and even patients to report ADRs [Davis and Coulson, 1999; van Grootheest et al. 2004, 2005; Morrison-Griffiths et al. 2003]. However, in developing nations the role of pharmacists in ADR reporting is not well established. In most developed countries, community pharmacists contribute heavily to their pharmacovigilance systems [van Grootheest and de Jong-van den Berg, 2002]. However, in developing nations, practice areas (i.e. hospital pharmacies and community pharmacies) are still in transition. Therefore, it is difficult for pharmacists in developing countries to play their role in ADR reporting [Classen et al. 2007; Evans et al. 1991; Phansalkar et al. 2007; Bawazir, 2006]. In addition, it is also essential to document pharmacists’ knowledge of ADRs and any barriers to their reporting.
With regard to the situation in Saudi Arabia, ADR reporting has been highly encouraged in recent years. The first initiative was in 1998 when the Ministry of Health established a postmarketing program. The main aim of the program was to detect ADRs and their frequency. Furthermore, training programs were held in hospital and community pharmacies and the forms relevant to the ADR reporting process were distributed [Bawazir, 2006]. There has been a spectacular growth of community pharmacists in Saudi Arabia. In the last two decades, the number has jumped from 1233 to 3244 in 2001 [Bawazir, 2006; Najjar, 2003]. In spite of this growth, the Saudi community pharmacist faces two main challenges: a lack of human resources (i.e. community pharmacists) and an overly business-oriented approach of pharmacy entrepreneurs [Al-Mohamadi et al. 2011]. These two factors might act as a challenge for ADR reporting through Saudi community pharmacies. Most community pharmacists working over the counter (OTC) in Saudi Arabia are expatriates; it is possible that their practices for ADR reporting in their country might affect their ADR reporting in Saudi Arabia. Similarly, the business-oriented focus of the pharmacy owners will also be another issue, which may prioritize revenue over ADR reporting. Earlier attempts were made to educate Saudi community pharmacists about the ADR reporting system [Bawazir, 2006]. However, there is no recent evidence of any recent ADR reporting practice by community pharmacists. Moreover, it will be essential to assess the community pharmacists’ knowledge and perceived barriers that may hinder the ADR reporting process. Hence, the present study was carried out to analyze the community pharmacists’ current knowledge and perceived barriers to ADR reporting systems.
Methodology
A cross-sectional study was planned among community pharmacies in the Eastern region, Alahsa (AH). The study period was from 1 June 2012 to 15 July 2012.
Study sample
A total of 150 pharmacies were identified in the AH region and a representative sample of community pharmacists was identified. Of these, about 100 were in urban areas and the rest were in rural areas. Bearing in mind the population, seven clusters were defined and 70 pharmacists were approached for their potential participation in the study.
Contents of the study tool
A self-administered, 28-item questionnaire was used to record participants’ views about ADRs and barriers to their reporting [van Grootheest et al. 2004; Bawazir, 2006]. The study tool was designed in the light of previously published international literature [van Grootheest and de Jong-van den Berg, 2002; Davis and Coulson, 1999; van Grootheest et al. 2004, 2005; Morrison-Griffiths et al. 2003; Classen et al. 2007; Evans et al. 1991; Phansalkar et al. 2007; Bawazir, 2006]. The questionnaire was mainly composed of three sections. Section one consisted of nine items, mainly focusing on the demographics and pharmacy-related information (Table 1). The focus of section two was to assess knowledge and perceptions of community pharmacists towards ADRs reporting, and were recorded using 10 items as shown in Table 2. Ten items were presented in this section using a nominal scale (yes/no). Section three was the last section of the questionnaire and aimed to document perceived barriers that may hinder ADR. Ten items were displayed in this section. A five-item Likert scale (strongly agree, agree, neutral, disagree, strongly disagree) was used for participants to disclose their response.
Demographic information of respondents.
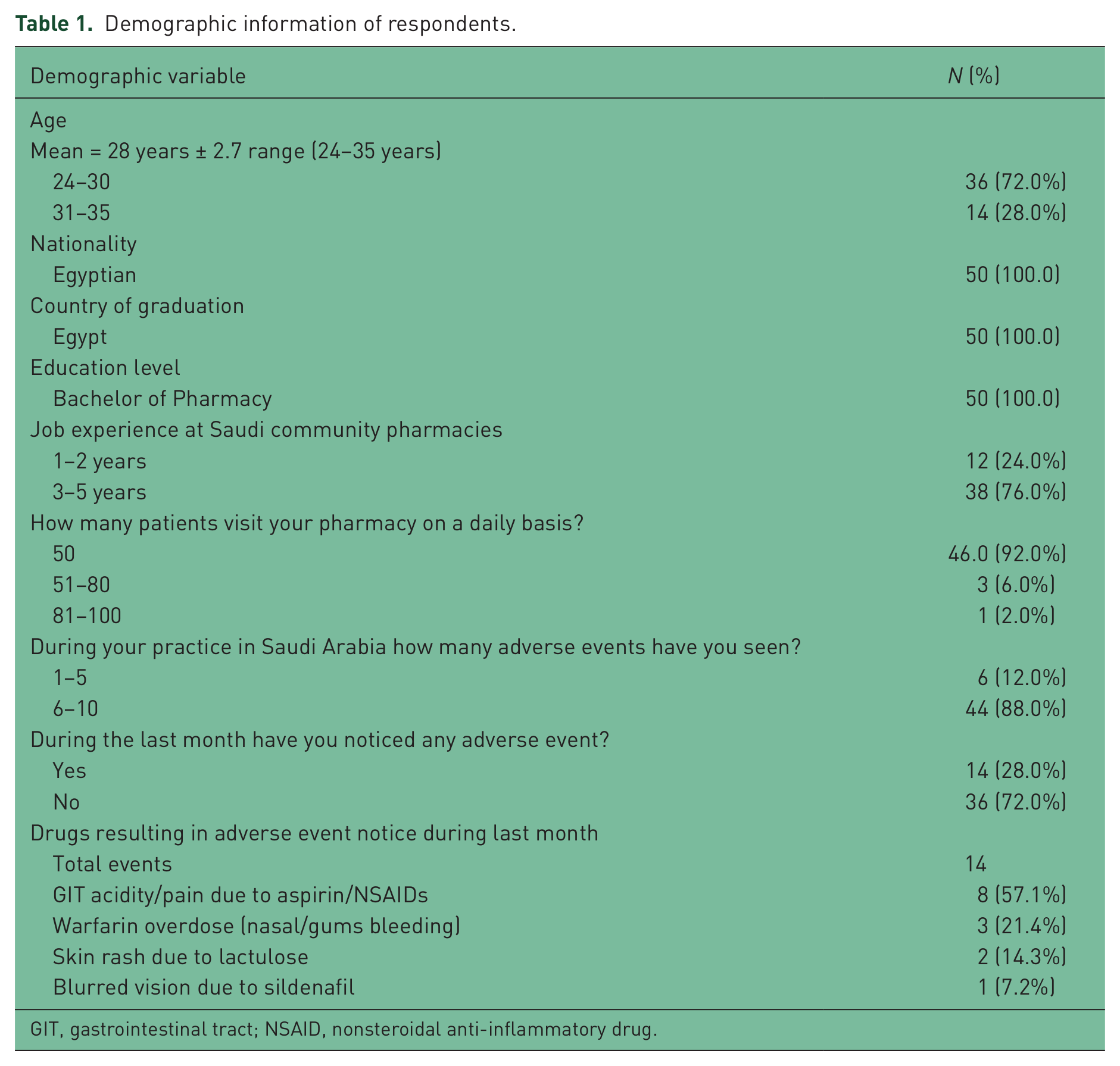
GIT, gastrointestinal tract; NSAID, nonsteroidal anti-inflammatory drug.
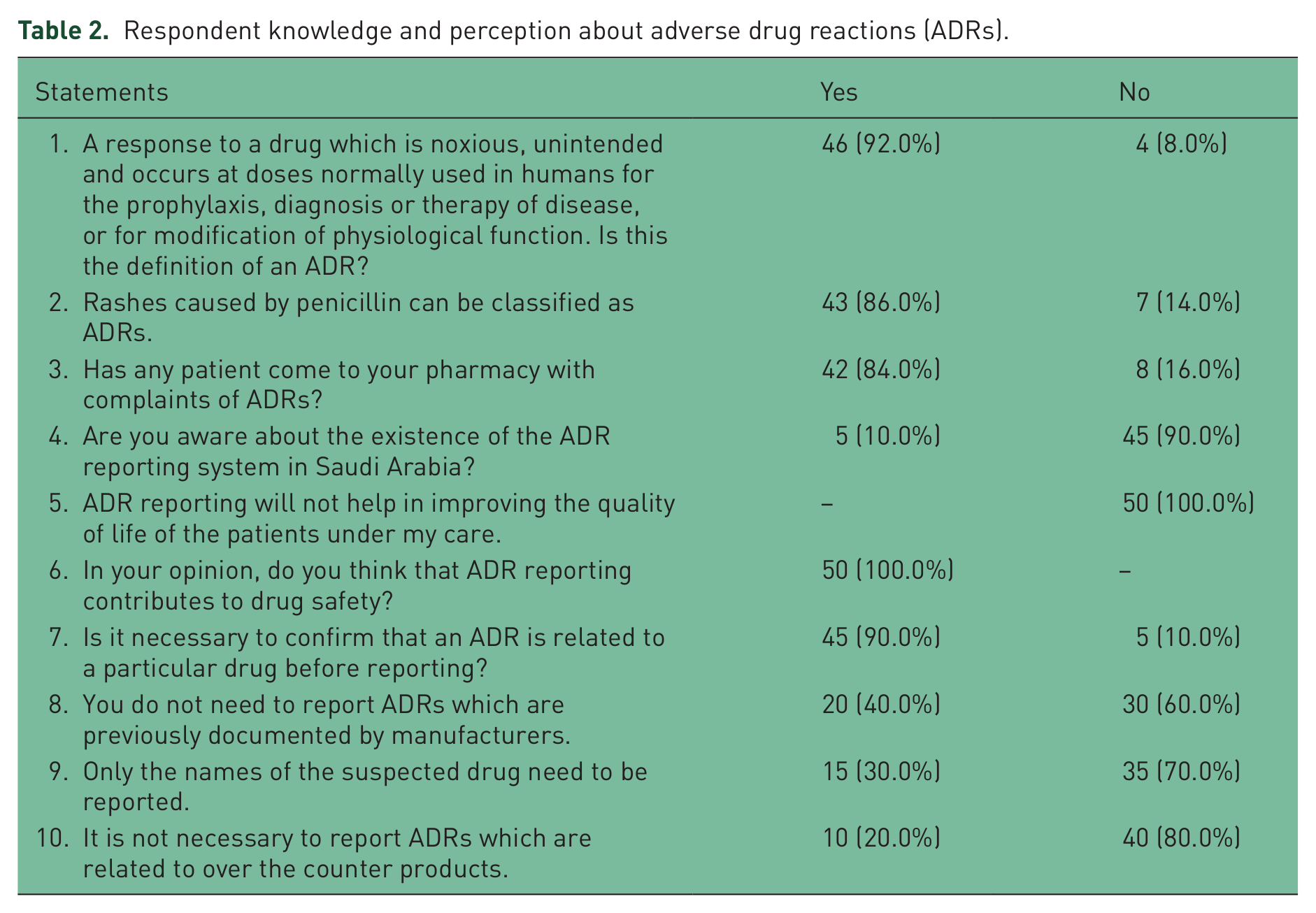
Respondent knowledge and perception about adverse drug reactions (ADRs).
Content validity and reliability of the tool
A pilot survey was done among 10 pharmacists to assess the face validity of the tool. The items that best suited the Saudi scenario were selected and translated into Arabic using the forward backward method. Some slight translation modifications were recommended to clarify the meaning of the statements. Furthermore, Cronbach’s α was calculated using the reliability scale. The overall α value was 0.63.
Ethical approval
The study protocol was approved by the college research committee chaired by the Dean of the college of clinical pharmacy, King Faisal University. Institutional approval was granted by the Deanship of scientific research, King Faisal University. Furthermore, written consent was also requested from the respondents. Questions that may disclose the personal identity of the pharmacists or pharmacies (i.e. names, contact numbers, name of pharmacy) were avoided.
Data analysis
Data analysis was done using the Statistical Package for Social Science version 13. Descriptive statistics was applied to calculate the frequencies and percentages. Relative index (RI) ranking was used to identify the top five barriers to the ADR reporting process. Routine ranking is done using the denominator (less than 1 and decreasing) RI rank.
Results
The overall response to the survey was 71.43%. Like other parts of Saudi Arabia, the majority of community pharmacists practicing in the Eastern region of Saudi Arabia are expatriate pharmacists, that is, Egyptians. All of them hold a bachelor’s degree in pharmacy with the majority (38, 76.0%) having work experience of 3–5 years. About 44 (88.0%) pharmacists disclosed that they had observed about 6–10 adverse events during their practice in Saudi Arabia. Moreover, 14 (28.0%) disclosed that they had observed an adverse event during the last month. Detailed information about the demographics and observed adverse events are shown in Table 1.
In terms of knowledge, very few (4, 8.0%) pharmacists were unable to differentiate between the right and wrong definition of ADRs (Table 2). Forty-two (84%) pharmacists reported that their patients had told them about a possible adverse events due to medicine use. However, 45 (90.0%) were not aware of the ADR reporting system in Saudi Arabia. In terms of reporting adverse events, 30.0% were willing to report the drug name only instead of the event. In addition, 10 (20.0%) believed that there was no need to report any adverse event associated with the use of OTC drugs.
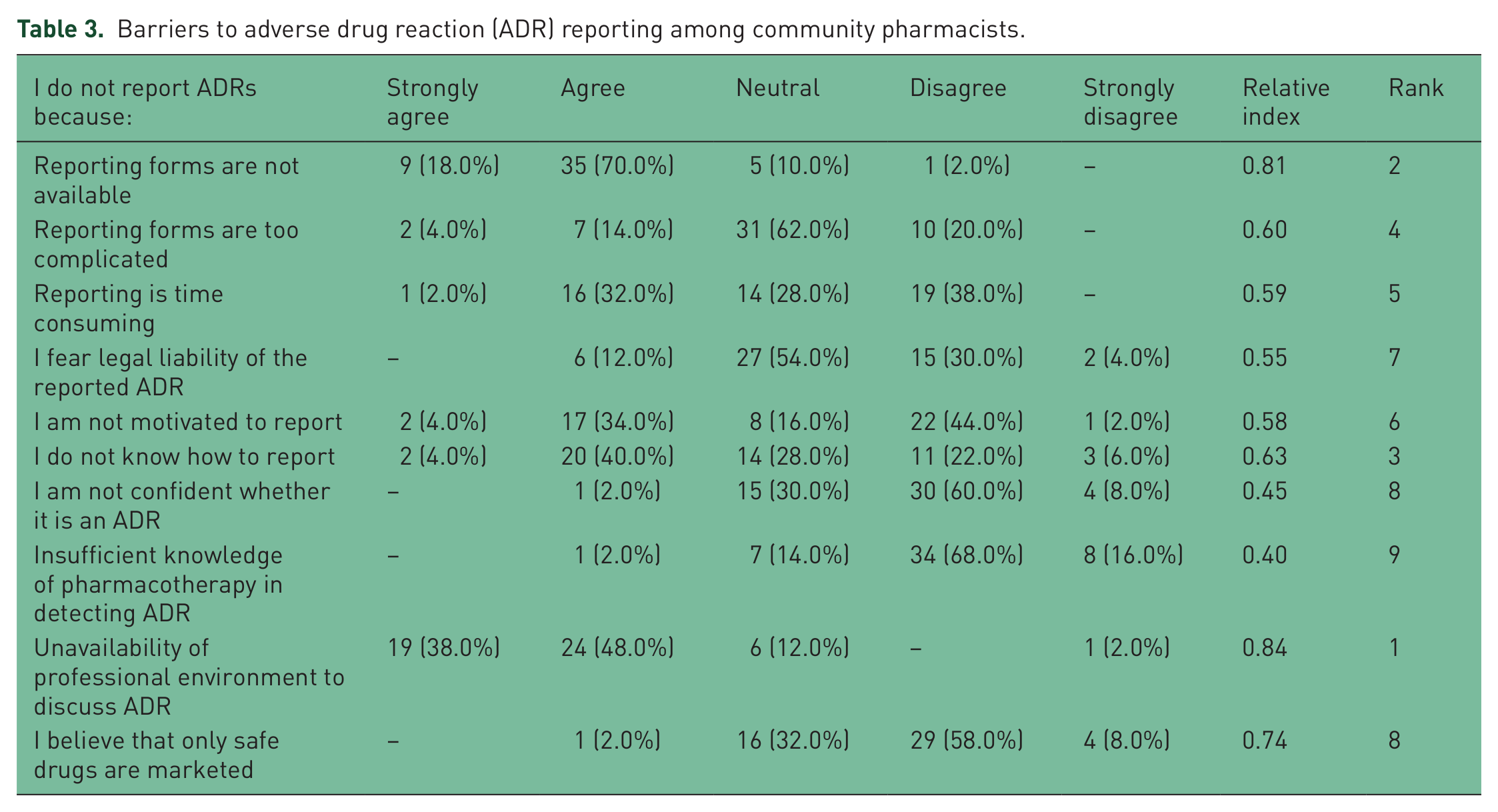
The last section of the study focused on identification of barriers to reporting adverse events. The unavailability of a professional environment to discuss ADRs was the first barrier to the reporting process (RI = 0.84). Other barriers were the unavailability of ADR reporting forms and poor understanding of the ADR reporting process, with most pharmacists believing it is a time-consuming process (Table 3).
Barriers to adverse drug reaction (ADR) reporting among community pharmacists.
Discussion
This is the first survey in AH to explore pharmacists’ attitudes to ADRs and their self-reported behavior in private community pharmacies in Saudi Arabia. The findings of this study are similar to previous studies conducted in the Saudi capital [Bawazir, 2006]. Most community pharmacists surveyed (90.0%) were not aware of the ADR reporting program in Saudi Arabia. The main reason for this might be the lack of human resources in community pharmacy practices in Saudi Arabia. Most of the practicing pharmacists are expatriates, who have a working contract of 3–5 years. Moreover, community pharmacy in Saudi Arabia is significantly business oriented. Therefore, the concept of services and reporting of ADRs might be regarded as a second priority by pharmacy entrepreneurs. However, globally, native pharmacists in Hong Kong, Holland and the UK were not aware of the ADR reporting programs in their countries [Lee et al. 1994; van Grootheest et al. 2002; Green et al. 1999]. In addition to awareness among community pharmacists, the role of regulatory authorities is also questionable due to the lack of enforcement of regulations in community pharmacy practice [Bawazir, 2004]. Furthermore, 40.0% of the pharmacists in this study were not willing to report ADRs and 30.0% reported the drug name only not the event. In addition, 20.0% disclosed that it was not necessary to report any events associated with the use of OTC products. The entire sample agreed that ADR reporting would help to improve drug safety but not the quality of life of patients visiting community pharmacies. Routine checks by the health authorities in Saudi Arabia to ensure a robust ADR reporting will be the only way to ensure medication safety for patients and to identify any drug-related threats to the Saudi population. Moreover, appropriate training for pharmacists about ADR reporting before they are issued with a license would be one way to create awareness among foreign pharmacists about the Saudi ADR reporting system.
In terms of barriers, most of the pharmacists agreed that lack of a professional environment is the main reason for failing to report ADRs (RI = 0.84). In addition, unavailability of the reporting form ranked as the second main barrier to the ADR reporting process (RI = 0.81), followed by not knowing how to report the event (RI = 0.63), ADR reporting forms being too complicated (RI = 0.60), and reporting being time consuming (RI = 0.59). These findings are similar to previous findings that report logistic barriers as a main reason for underreporting [Bawazir, 2006]. However, community pharmacists were found to be motivated to report ADRs because they thought that they had a better knowledge of pharmacotherapy and were confident to classify events. This finding is contradictory to other studies that report poor clinical knowledge, lack of confidence and fear of liability as the main barriers to reporting ADRs among healthcare providers [Belton, 1997; Backstrom et al. 2000; Lee et al. 1994; Generali et al. 1995].
Effective ADR reporting systems in community pharmacies are an essential element in any healthcare setup. Education and frequent training for pharmacists would be an ideal way to establish a spontaneous ADR reporting system among community pharmacies in Saudi Arabia [Generali et al. 1995; Green et al. 1999; Toklu and Uysal, 2008]. An acknowledgment and rewards system (i.e. financial incentives) would also help to improve ADR reporting in Saudi Arabia [Green et al. 1999; van Grootheest and de Jong-van den Berg, 2002]. Furthermore, pharmacy owners could permit the use of internet services in community pharmacies for online ADR reporting to drug-regulating authorities.
Conclusion
Community pharmacists practicing in AH were found to be unaware of the ADR reporting system in Saudi Arabia. The unavailability of reporting forms, a deficient professional environment to discuss ADRs and poor understanding of the ADR reporting system were found to be the main barriers in this study. Establishing a user-friendly process will be an ideal way to improve ADR reporting among community pharmacies in Saudi Arabia.
Limitations
A small sample size may be one of the main limitations of this study. Future studies should aim to conduct studies on a larger scale. Furthermore, the entire study sample consisted of expatriate pharmacists. Therefore, the findings cannot be generalized to all Saudi pharmacists.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The author declares no conflict of interest in preparing this manuscript.