
Abstract
Topiramate is an antiepileptic drug (AED) with multiple mechanisms of action that has been shown to be effective in a number of neuropsychiatric disorders. However, cognitive dysfunction is frequently observed in such patients, often representing a relevant challenge in their management. Moreover, there is a long-held recognition that AEDs may profoundly affect cognitive functions. This paper reviews available data on cognitive adverse events in patients with neurological disorders treated with topiramate, discussing the role of different contributing factors such as the pharmacological properties of the drug, the specific features of the brain disorder, and other variables pertinent to the discussion. All studies agree that up to 10% of patients may complain of treatment-emergent adverse events on cognition. Such problems occur early during treatment (i.e. within 6 weeks) and emerge in a dose-dependent fashion, suggesting that such prevalence may be significantly reduced using the drug in monotherapy and adopting individualized doses and titration schedules. The magnitude of the problem is generally mild to moderate and the subjective perception of the patient needs to be taken into account. In fact, apart from language problems, data are not conclusive. Comparisons with new AEDs are limited to levetiracetam and lamotrigine, in both cases generally disfavoring topiramate, while data regarding first-generation AEDs show clear differences only for verbal fluency.
Introduction
Antiepileptic drugs (AEDs) are central nervous system (CNS) agents that are prescribed in a number of different conditions ranging from epilepsy and pain syndromes (both central and peripheral) to mood and anxiety disorders [Mula et al. 2007; Johannessen Landmark, 2008]. Cognitive dysfunction is frequently observed in subjects with CNS disorders and the relative contribution of AEDs in this regard may be of relevance [Mula and Trimble 2006]. Moreover, the fact that a considerable number of patients need AED therapy for many years, or even for a lifetime, emphasizes the need to focus on the long-term adverse effects of these drugs on cognition.
Topiramate is an AED structurally unrelated to previous and subsequent compounds. It had been initially marketed for the add-on treatment of patients with drug-resistant partial epilepsy and, through the following years, it has shown a broad spectrum of efficacy, which extends to primary generalized tonic–clonic seizures [Biton et al. 1999] and tonic–atonic seizures associated with the Lennox-Gastaut syndrome [Sachdeo et al. 1999]. Data in special populations such as elderly people [Zhang et al. 2011] and mentally handicapped children [Kluger et al. 2009] are also available. In addition to its use in epilepsy, topiramate showed therapeutic effects in a number of neurological conditions such as migraine (sporadic, chronic and migraine overuse headache) [Magis and Schoenen, 2011], pain syndromes [Tremont-Lukats et al. 2000; Backonja, 2002] and movement disorders (tics, restless leg syndrome, tremor) [Spina and Perugi, 2004]. Currently, topiramate has an approved indication in the treatment of children and adults with epilepsy, treatment of Lennox-Gasteau syndrome and the prevention of migraine.
The aim of this paper is to review data on cognitive tolerability during treatment with topiramate in neurological disorders, discussing the role of different contributing factors such as the pharmacological properties of the drug, the specific features of the CNS disorder, and other variables pertinent to the discussion. Papers about topiramate in psychiatric disorders or obesity have been excluded because the problem of cognition and treatment-emergent adverse events in this particular population would deserve a separate paper. References were identified by searches of Medline/PubMed using the terms ‘topiramate’, ‘cognition’, ‘epilepsy’, ‘headache’, ‘pain’, ‘movement disorders’. Only papers published in English in international peer-reviewed journals were considered. The reference list of relevant articles was hand searched for additional publications (e.g. book chapters or review papers) if relevant for the discussion.
Mechanisms of action of topiramate
The variety of proposed clinical applications is consistent with the multiple mechanisms of action, ranging from voltage-gated calcium channel blockade to modulation of synaptic neurotransmission [Shank et al. 2000; White, 2003]. Topiramate reduces the frequency of activation of voltage-sensitive sodium channels in a state- or use-dependent manner. It produces a voltage-sensitive, use-dependent and time-dependent suppression of sustained repetitive firing (SRF) in cultured mouse spinal cord and neocortical cells [McLean et al. 2000]. However, such activity on sodium channels differs from that of other AEDs (such as phenytoin, carbamazepine and lamotrigine), in which a rapid limitation or complete block of SRF occurs. A second mechanism of action is the potentiation of the inhibitory γ-aminobutyric acid (GABA)-mediated neurotransmission through an interaction with the GABAA receptors [White et al. 1997]. Interestingly, such an effect does not involve an action on the benzodiazepine (BDZ)-binding site, as it is not modulated by flumazenil [Shank et al. 1994]. A third mechanism of action is the inhibition of neuronal excitatory pathways through a selective action at the α-amino-3-hydroxy-5-methyl-4-isoxazole-propionic acid (AMPA) and kainate subtypes of glutamate receptors [Delorenzo et al. 2000]. Some studies demonstrated a biphasic effect of topiramate on kainate-evoked currents [Gibbs et al. 2000], as revealed by an initial inhibition of the kainate-evoked currents, followed by a delayed additional inhibitory effect. A further mechanism of action is the inhibition of high voltage-activated calcium currents on L-type calcium channels, thus reducing neurotransmitter release and inhibiting calcium-dependent second-messenger systems [Zhang et al. 2000]. Finally, topiramate seems to be a weak inhibitor of type II and type IV carbonic anhydrase (CA), thus modulating pH-dependent activation of voltage- and receptor-gated ion channels [Leniger et al. 2004]. Topiramate, like acetazolamide, contains a sulfamate moiety that is likely to be responsible for its CA-inhibiting properties. However, when compared with acetazolamide, topiramate is approximately 10–100 times less potent as an inhibitor of these isoenzymes [Shank et al. 1994]. CA-inhibiting properties are considered not to be relevant to the anticonvulsant activity but they are thought to be of significance in determining some of the adverse effects, such as increased risk of nephrolithiasis and metabolic acidosis, as observed with acetazolamide [Kennedy and Lhatoo, 2008]. Finally, a proposed unifying mechanism that can possibly account for the wide range of pharmacological effects exerted by topiramate is the action on the phosphorylation state of membrane proteins [Shank et al. 2000]. Emerging evidence suggests that topiramate may bind to phosphorylation sites within AMPA, kainate, GABAA and voltage-activated sodium channels. Topiramate binds to such sites on receptor proteins only in the dephosphorylated state, exerting a possible bifold effect. Therefore, topiramate can modulate ion conductance through the channel by an immediate allosteric action, and it could exert a delayed effect by shifting the channel toward the dephosphorylated state [Shank et al. 2000].
Data from healthy volunteers
Although studies in healthy volunteers are often criticized for the lack of relevance to the clinical situation, they allow focusing on the effect of the drug on cognitive functions without all confounding variables related to the underlying brain disorder. Available data focus mainly on gabapentin and lamotrigine in comparison to topiramate with all authors agreeing that the latter has negative effects on memory, verbal and executive functions [Martin et al. 1999; Aldenkamp, 2000; Lhatoo et al. 2000; Meador et al. 2005; Salinsky et al. 2007]. Interestingly, neuroimaging studies point out that topiramate, especially when rapidly titrated, is associated to GABAergic potentiation [Kuzniecky et al. 1998, 2002]. However, neuropsychological effects of topiramate are slightly different from those reported, for example, with BDZs. In fact, the acute administration of BDZs is associated with sedation, drowsiness, psychomotor slowing and anterograde amnesia [Stewart, 2005], while long-term treatment with impairment in visuospatial and visuomotor abilities, decreased IQ, motor incoordination, slowing psychomotor speed, decreased speed of information processing, verbal learning and concentration, and delayed response times [Stewart, 2005]. Therefore, the GABAergic potentiation of topiramate during rapid titration may explain only some of the negative effects on cognition. In fact, studies investigating electroencephalogram changes in healthy volunteers suggest a unique profile of topiramate compared with other AEDs such as carbamazepine, phenytoin or gabapentin [Mecarelli et al. 2001; Wang et al. 2003; Smith et al. 2006; Salinsky et al. 2007].
Data from different neurological disorders
Epilepsy
First, it has to be stated that a variety of factors, in addition to AEDs, can affect cognitive functions in patients with epilepsy. Thus, it is imperative to realize that, in clinical practice, many cognitive problems have a multifactorial origin and different combined aspects are responsible in the individual patient [Mula and Trimble 2009].
Early clinical studies of topiramate as add-on treatment in patients with drug-refractory partial epilepsy report concentration and memory problems in up to 10% of subjects [Ben-Menachem et al. 1996; Privitera et al. 1996] with a two- to fivefold increased risk of developing cognitive complaints compared with placebo [Jette et al. 2008]. However, as adverse events usually occur during controlled trials, they can be explained by the forcedly rapid titration schedule adopted, the increased vulnerability of the investigated population (difficult-to-treat patients) and the likelihood of developing pharmacodynamic interactions. In fact, cognitive complaints decrease to 3–4% when topiramate is prescribed in monotherapy [Arroyo et al. 2005] or flexible, individualized doses are adopted [Krakow et al. 2007]. In this regard, Ramsay and collaborators point out that even a very rapid titration schedule (i.e. 100 mg on the first day) can be successfully used in monotherapy with a relatively low discontinuation rate due to adverse events [Ramsay et al. 2010].
One of the first studies specifically designed to investigate the impact of topiramate on cognitive functions was conducted in 10 patients with epilepsy evaluated at weekly intervals over a period of 3 months [Burton and Harden, 1997]. The authors suggested that high topiramate doses are associated with a poor performance for attention. A retrospective study evaluated neuropsychological tests in 18 patients before and during at least 3 months of topiramate treatment, comparing them with 18 matched controls [Thompson et al. 2000]. The authors reported a progressive decline in verbal functions, especially verbal fluency, and reassessment of eight patients after discontinuation shows improvement in all measures [Thompson et al. 2000]. That topiramate may selectively affect language functions has been replicated by a number of studies [Mula et al. 2003b; Gross-Tsur and Shalev, 2004, Cappa et al. 2007] and seems to be related to a specific underactivation of Broca’s area induced by the drug [De Ciantis et al. 2008] in a specific subset of more vulnerable patients [Mula et al. 2003b]. This is further confirmed by the lack of association with the starting dose or the titration schedule [Mula et al. 2003b], being reported also with very low doses (less than 100 mg) or in long-term treatment [Lee et al. 2006].
Data about topiramate in comparison to older AEDs come from two multicenter, double-blind, randomized, parallel-group studies comparing topiramate with valproate as add-on therapy to carbamazepine [Aldenkamp et al. 2000; Meador et al. 2003]. On a number of neuropsychological measures, the two compounds displayed slight differences favoring valproate on measures of speech [Meador et al. 2003] and short-term memory [Aldenkamp et al. 2000]. Regarding new AEDs, a multicenter, double-blind, randomized, prospective study compared lamotrigine and topiramate as an adjunctive therapy with carbamazepine or phenytoin [Blum et al. 2006]. Topiramate again showed a detrimental effect on specific measures of language compared with lamotrigine [Blum et al. 2006]. An unblinded observational study explored cognitive functions in 51 patients with focal epilepsy treated with levetiracetam or topiramate as add-on or monotherapy [Gomer et al. 2007]. The authors observed detrimental effects of topiramate in attention, short-term memory and verbal fluency.
Neuropsychological studies of patients taking topiramate in monotherapy are very limited, with a single 12-month follow-up study suggesting some negative effects on memory, information processing and verbal fluency [Baker et al. 2011].
Of great clinical relevance are data coming from populations of children with epilepsy. In general terms, clinical studies suggest an acceptable tolerability profile with low dropout rates for cognitive problems [Novotny et al. 2010; Pina-Garza et al. 2011]. A double-blind, dose-controlled study examined efficacy and tolerability of topiramate monotherapy in newly diagnosed children and adolescents with epilepsy [Glauser et al. 2007]. The incidence of treatment-emergent adverse events seems to be clearly dose dependent with concentration/attention difficulties occurring only in a limited number of subjects. A 12-week, open-label study explored cognitive outcomes of 53 children treated with topiramate as monotherapy or add-on therapy, reporting no significant changes in measures of memory [Brandl et al. 2010]. A multicenter, randomized, open-label, observer-blinded, parallel-group clinical trial examined cognitive functions and behavioral problems with topiramate compared with carbamazepine in monotherapy for children with benign Rolandic epilepsy [Kang et al. 2007]. On a neuropsychological test battery, arithmetic is the only variable with a significant worsening after 28 weeks of treatment. However, looking at children treated at the minimum target dose (from 12.5 to 75 mg according to weight), no significant difference between topiramate and carbamazepine could be observed.
By contrast, data in children with learning difficulties, especially severe ones, suggest poor cognitive and sometimes behavioral tolerability. An observational open study in children with multiple disabilities (aged 1–15), with difficult-to-treat epilepsy, investigated efficacy and tolerability of rapid oral initiation of topiramate (starting dose 1 mg/kg/day) [Kluger et al. 2009]. Although no serious adverse events were reported, the rapid dose escalation is associated with a very low tolerability. In fact, 17 out of 19 patients reported adverse events, with behavioral disturbances occurring in 15.8%. An open study examined the behavioral and cognitive effects of topiramate as add-on treatment in children and adolescents with mild to severe mental retardation [Coppola et al. 2008]. The authors reported a significant cognitive deterioration in about 70% of patients at 3 months, persisting in about 20% at 12 months.
Data about older patients with epilepsy are mixed. Cognitive complaints are reported in the region of about 10% in a context of dropout rates of about 46% [Groselj et al. 2005; Stefan et al. 2008]. However, older patients with newly diagnosed epilepsy are often sensitive to their initial drug treatment [Rowan et al. 2005]. Moreover, older subjects may be particularly sensitive to the cognitive effects of AEDs and a clearly dose dependency is not always evident [Ramsay et al. 2008].
Headache
Data from controlled studies in adult patients with migraine show a prevalence of impaired concentration or memory in around 10% [Silberstein et al. 2007, 2009; Lipton et al. 2011]. However, an analysis of pooled safety data obtained from over 1500 patients who participated in four randomized, double-blind, placebo-controlled, clinical trials points out that the majority of adverse events are usually mild to moderate in severity and occur during the titration phase rather than during the maintenance period [Adelman et al. 2008]. In fact, difficulties with concentration are reported in the region of 1% during the maintenance period at different target doses (50 mg, 100 mg and 200 mg), against prevalence rates of 3%, 6% and 9% during the titration phase. Interestingly, a double-blind, randomized, controlled study of topiramate and amitriptyline, either alone or in combination, reported that the combination of the two drugs is not only more effective then the single treatment but also better tolerated with fewer adverse events [Keskinbora and Aydinli, 2008].
In difficult-to-treat patients, such as chronic migraine or medication overuse headache (MOH), topiramate displays not only a good tolerability but also a positive impact on quality-of-life measures [Diamond et al. 2005]. An open-label, prospective study compared topiramate (100 mg) and pregabalin (150 mg) in patients with MOH, showing similarities in terms of efficacy and tolerability [Rizzato et al. 2011]. A large randomized, double-blind, placebo-controlled trial of topiramate in chronic migraine demonstrates a significant improvement in migraine-related limitations on daily activities and emotional distress beginning as early as week 4 and continuing up to week 16 after treatment [Dodick et al. 2007].
The different pattern of adverse events reported in migraine populations treated with topiramate, compared with patients with epilepsy, represents another interesting point. A randomized, double-blind, placebo-controlled study of topiramate in chronic migraine reported paraesthesias in 53% of patients treated with topiramate versus 6% of attention problems [Diener et al. 2007]. An open-label, flexible-dose, clinical trial in patients with episodic migraine showed a premature discontinuation rate (37.6%), mainly due to adverse events (23.6%) [Malessa et al. 2010]. Interestingly, all studies suggest that paraesthesias represents the most common and disabling adverse event (sometimes up to 50%), with memory impairment occurring in 10.2% of subjects. Data from noninterventional studies in patients with episodic migraine in a general practice setting have confirmed assumption [Nelles et al. 2009, 2010]. A meta-analytic comparison of topiramate-related adverse drug reactions in epilepsy and migraine shows that patients with migraine have a two- to threefold increased risk of developing paraesthesias [Luykx et al. 2009].
As for patients with epilepsy, particular attention needs to be paid to pediatric patients. Randomized, double-blind, placebo-controlled studies of topiramate in children with migraine have reported low rates of somnolence or other cognitive complaints [Winner et al. 2005; Lewis et al. 2009]. Pandina and colleagues specifically investigated the impact of topiramate 100 mg daily on learning, memory and executive functions and observed a significant decrease in psychomotor reaction times [Pandina et al. 2010]. However, a review of five papers on pediatric migraine treated with topiramate (two randomized, controlled trials and three post hoc subset analyses of adolescents who were included in three randomized, controlled trials conducted in adults) shows somnolence and concentration problems in rates similar to those reported in adults (around 8%) [Ferraro and Di Trapani, 2008]. In general terms, available data, although limited, seem to suggest that topiramate is well tolerated in pediatric populations of patients with migraine. Adverse events may occur early during treatment and tend to decline over time while a significant improvement in terms of school absenteeism and disability can be seen. Nevertheless, adverse events such as somnolence of subjective concentration problems may be particularly distressing for children and adolescents; therefore, the decision to initiate such a treatment must be carefully considered for the individual patient.
Other neurological disorders
Although topiramate has no indication in other neurological conditions, a number of studies have shown interesting applications, especially in essential tremor and neuropathic pain.
A 24-week, multicenter, double-blind, placebo-controlled, parallel-design study examined the efficacy and safety of topiramate (400 mg) monotherapy in patients with essential tremor reporting concentration and memory difficulties in only 3% of patients [Ondo et al. 2006]. An analysis of three randomized, double-blind, placebo-controlled, crossover trials of topiramate in patients with essential tremor describes cognitive complaints in around 10% of patients [Connor et al. 2008].
A 10-week, randomized, double-blind, placebo-controlled study of topiramate in patients with low back pain showed very good tolerability, with a significant improvement in terms of mood and quality of life [Muehlbacher et al. 2006].
Discussion
Treatment-emergent cognitive adverse events have a multifactorial origin with a number of variables implicated (Table 1). Furthermore, one of the major limitations in reviews of the literature in this area is that neuropsychological tests used in the studies are not uniform [Mula and Trimble 2009]. In fact, many different test batteries have been used, and the administration of tests and reporting of test results differ across all presented studies, which makes it impossible to formulate a qualified comparison of the results. Neuropsychological tests must also meet the criteria of reliability, validity and sensitivity to change. Further, they should have been standardized in the epilepsy population. The results of studies adopting neuropsychological tests that have not been standardized, with respect to epilepsy, may expose clinicians and patients alike to unreliable information regarding specific AEDs.
Mechanisms of action of topiramate (TPM) in comparison to selected old and new anticonvulsants.
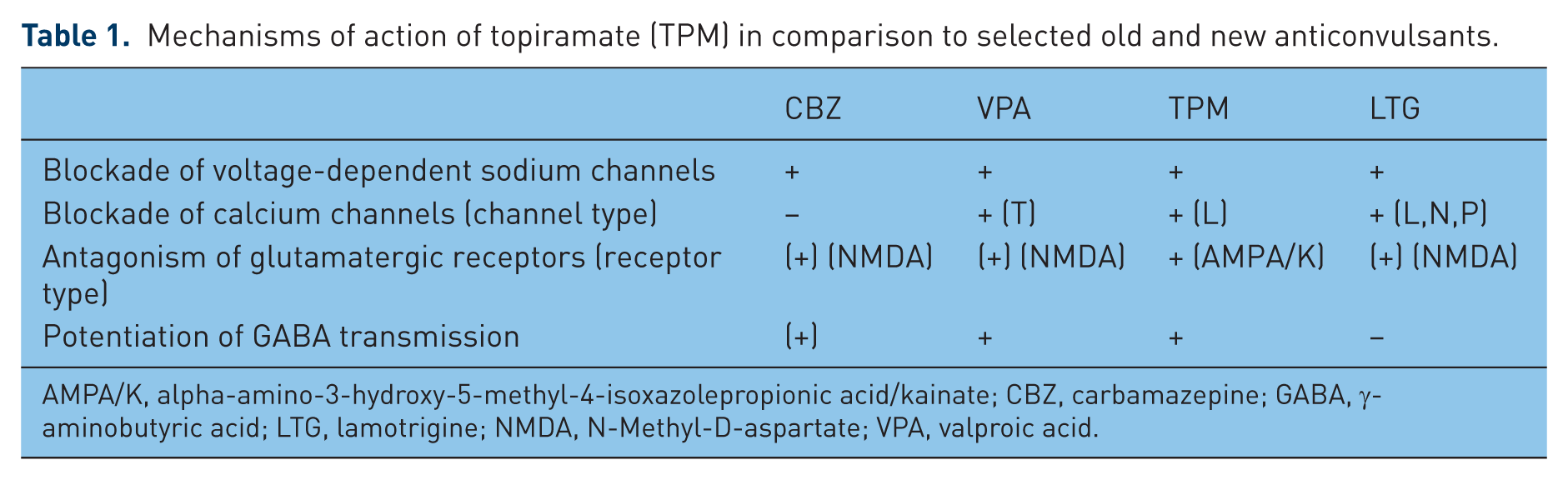
AMPA/K, alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid/kainate; CBZ, carbamazepine; GABA, γ-aminobutyric acid; LTG, lamotrigine; NMDA, N-Methyl-D-aspartate; VPA, valproic acid.
In general terms, all presented data suggest that up to 10% of patients treated with topiramate may complain of cognitive problems. However, it is important to state that cognitive complaints do not necessarily reflect a negative effect on cognitive functions. A nonrandomized, open-label, parallel-group study comparing the long-term cognitive effects of topiramate and levetiracetam as add-on treatment in patients with intractable epilepsy showed that memory does not represent a concern despite the high incidence of memory complaints and that topiramate may not necessarily have absolute deteriorating effects even in subjects with mesial temporal lobe epilepsy and baseline poor cognitive performance [Huang et al. 2008]. Nevertheless, topiramate is perceived by patients (and as a consequence by clinicians) to have a worse tolerability profile than other AEDs [Arif et al. 2010] and this is further confirmed by retention rate studies [Marson et al. 2007a, 2007b]. Subjective preference for CNS drugs is quite an unexplored topic with very limited data. A double-blind, randomized, crossover study tried to examine the subjective preference for either topiramate or lamotrigine in healthy volunteers [Werz et al. 2006]. A large majority of subjects (70%) were shown to prefer lamotrigine and such preference was consistent with a better performance on a number of neuropsychological and behavioral measures, mood state in particular. In this regard, an established finding is that the subjective perception of treatment-emergent cognitive adverse events may be related more to the mood state rather than to the objective performance [Kanner et al. 2003; Marino et al. 2009]. A number of studies point out that topiramate may have a negative impact on mood [Mula et al. 2003a; Mula et al. 2009] and such an effect may consequently have an influence on the subjective perception of tolerability, increasing rates of cognitive complaints [Kanner et al. 2003; Mula et al. 2006].
The contribution of the mechanisms of action of topiramate to the overall cognitive tolerability is difficult to establish (see Table 2 for a comparison with other AEDs). As previously discussed, neuroimaging studies in healthy subjects have demonstrated a significant GABAergic potentiation with topiramate [Kuzniecky et al. 1998, 2002], but neurophysiologic data are not along the same line [Mecarelli et al. 2001; Wang et al. 2003; Smith et al. 2006; Salinsky et al. 2007]. What is becoming evident is that topiramate preferably affects frontal lobe functions [Kockelmann et al. 2003; Jansen et al. 2006; Gomer et al. 2007] and such preference is particularly reflected by the effect on verbal fluency. Topiramate is a sulfamate and specific language toxicity has been reported with other compounds containing a sulfa moiety [Ojemann et al. 2001], such as zonisamide [Wilensky et al. 1985], sulthiame [Dodrill, 1975] or sulfasalazine [Hill et al. 1994]. Therefore, it is tempting to speculate that there may be a specific sensitivity of the Broca’s area to sulfa-containing compounds [Ojemann et al. 2001]. Further studies in this area are needed.
Mechanisms for cognitive adverse effects of antiepileptic drugs.
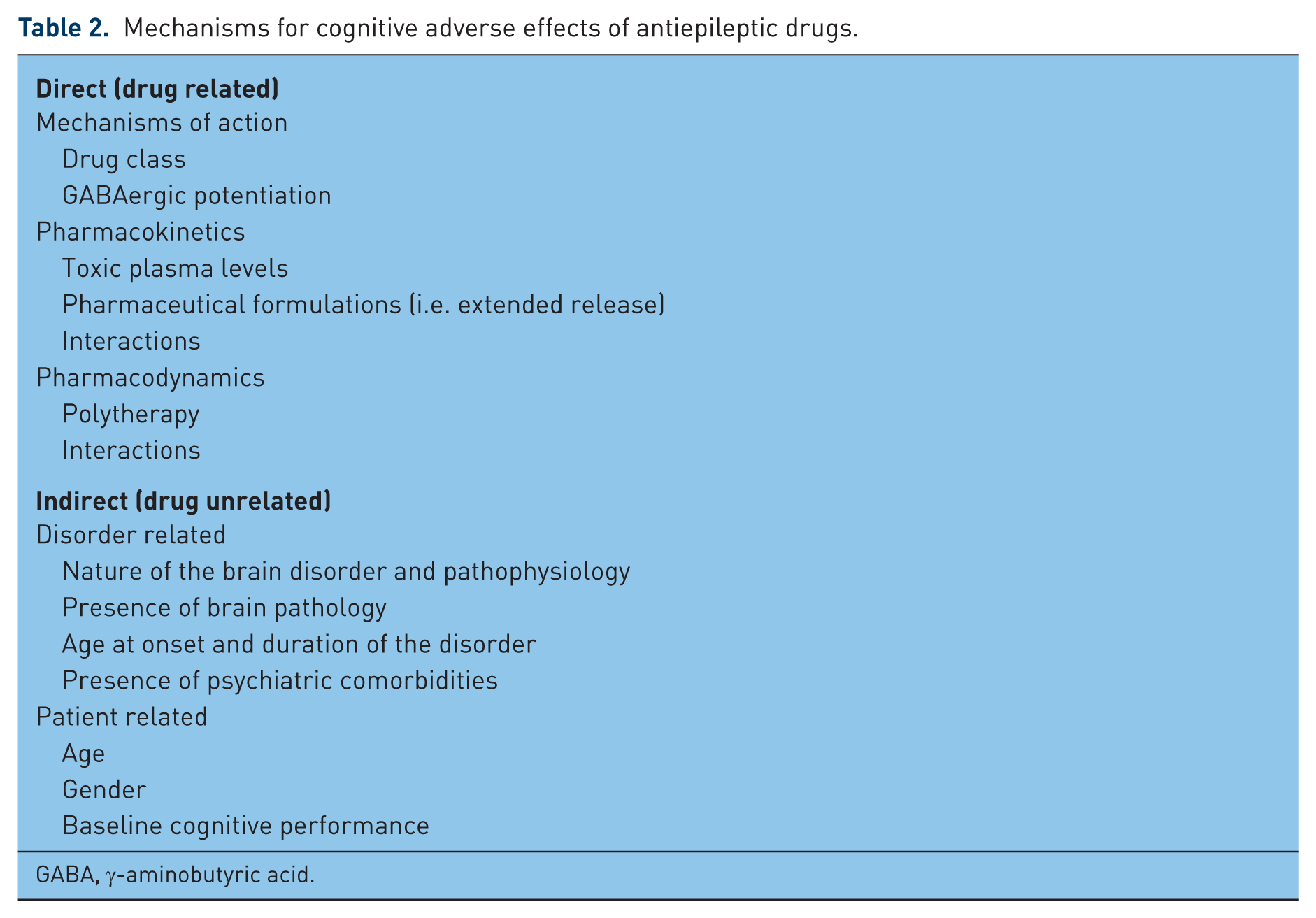
GABA, γ-aminobutyric acid.
Another relevant issue relates to the timing of the adverse events. All studies agree that cognitive problems with topiramate can be identified early during treatment (i.e. within 6 weeks) and emerge in a dose-dependent fashion [Loring et al. 2011]. This is reported with almost all CNS drugs, and after a short period (i.e. a few days or weeks), normalization usually occurs. This phenomenon, also known as tolerance or habituation, needs to be carefully considered to avoid an overestimation of the negative effects of a drug on cognition. As pointed out by Aldenkamp, in clinical assessment, we should conclude that a drug has significant ‘cognitive side effects’, only if these persist during long-term treatment [Aldenkamp et al. 2003].
Finally, the possible association with drug serum levels needs to be discussed. Data on topiramate are more than scanty. A prospective study in poorly controlled patients with epilepsy examines the relationship between adverse events and serum topiramate concentrations [Froscher et al. 2005]. The authors suggest a maintenance level below 4 µg/ml to avoid psychomotor slowing or abnormal thinking.
Conclusions
All presented data suggest that up to 10% of patients treated with topiramate, either for epilepsy or migraine, may complain of cognitive problems but such prevalence may be significantly reduced using topiramate in monotherapy and adopting individualized doses and titration schedules. Although the magnitude of such treatment-emergent adverse events is generally mild to moderate, the subjective perception needs to be considered. In this regard, it has to be taken into account that, in some selected cases, topiramate may negatively impact on mood. In fact, apart from language problems, data are not conclusive. Comparisons with new AEDs are limited to levetiracetam and lamotrigine, in both cases generally disfavoring topiramate, while data regarding first-generation AEDs show clear differences mainly for verbal fluency. The case of topiramate clearly points out that a careful use of the drug is always mandatory to maximize compliance and not to deprive patients of an effective treatment.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
In the past, the author has received travel grants or consultancy fees from various pharmaceutical companies, including Pfizer, UCB-Pharma, Janssen, that are involved in the manufacture of antiepileptic drugs.