
Abstract
Prescribing antiepileptic drugs (AEDs) in pregnancy is a challenge to the clinician. A multitude of questions arise that must be addressed even prior to conception. In women with proven epilepsy, it may be dangerous to stop or even change the AED regimen during pregnancy. Changes could lead to injury or death in both the mother and the fetus. In the rare cases when discontinuing an AED is plausible, it should be done methodically in consultation with the physician prior to conception. Most women with epilepsy are consigned to continue their AEDs before, during and after pregnancy. The metabolism of AEDs may change drastically during pregnancy. These changes must be addressed by the clinician. Drug levels should be monitored consistently during pregnancy. The risks to the fetus must be delineated in terms of side effects from specific drugs as well as risks from the seizure disorder itself. Many AEDs have well known teratogenic effects, and these must be elucidated to the mother. There are risks (theoretical and evidence based) for obstetrical complications, poor neonatal outcomes, congenital malformations and even cognitive effects on the child later in life. These risks are addressed in this article with respect to individual AEDs. Recommendations include but are not limited to preconception counseling, taking folate pre and post conception, prescribing the most effective AED while minimizing risks, and avoiding polytherapy and valproate if possible.
Introduction
Epilepsy is defined by the presence of recurrent, unprovoked seizures. The typical treatment is a daily, long-term antiepileptic drug (AED) regimen. People with epilepsy expect to participate fully in life experiences, including childbearing, as the majority of them have well controlled seizures, and are otherwise healthy [Harden et al. 2009b]. According to the US Department of Health’s recent estimates of the US population and the known prevalence of epilepsy, approximately half a million women with epilepsy (WWE) are of childbearing age [Hirtz et al. 2007]. It has been estimated that three to five births per 1000 will be to WWE [Yerby, 2000]. In utero exposure to some AEDs is associated with an increased risk of major congenital malformations (MCMs), possible obstetrical complications, possible neonatal complications, impaired behavioral development, and impaired cognitive development in the child. These risks must be weighed against the risk of recurrent seizures in the mother and the complications that could come as a result of changing or stopping AED treatment [Palac and Meador, 2011].
As early as the 1960s, a relationship between the use of AEDs during pregnancy and MCMs was recognized [Meadow, 1968]. For many years the risk of MCMs in children born to WWE treated with AEDs during pregnancy has been known to be approximately two to three times higher than the 1–2% frequency in the general population [Palac and Meador, 2011]. More recent evidence suggests a special risk for valproate [Meador et al. 2008b].
The risks of obstetrical complications in pregnant WWE are uncertain but could include increased risk of cesarean delivery, preeclampsia, pregnancy-induced hypertension, pregnancy bleeding complications, premature contractions or premature labor and delivery, and spontaneous abortion [Harden et al. 2009a].
Perinatal/neonatal complications may include but are not limited to small for gestational age (SGA), low Apgar scores, and risk of perinatal death. Unfortunately, no studies have delineated many likely important contributing factors, including differences across AEDs, levels of in utero exposure, or epilepsy type.
Recently, the impact of fetal exposure to maternal AEDs on cognitive and behavioral development has emerged as an area of concern. Research efforts thus far suggest that maternal use of some AEDs during pregnancy may negatively impact cognition in the infants of WWE [Palac and Meador, 2011). Evaluation and comparison of reports on AED teratogenicity, cognitive outcomes, and behavioral outcomes are difficult, even though considerable progress has been made recently in developing pregnancy registries. Outcome data are incomplete. Registries are observational investigations, have variable methodology, deal with different cultures and populations, have different definitions, have different standardized testing (e.g. different cognitive tests), and have variable follow-up times. These registries also have different data collection timing (e.g. MCMs at birth versus at 1 year old). Lack of information about mothers as well as lack of follow up restricts usefulness of registry data. In addition, each of the individual registries has weaknesses ranging from missing data on key variables to low numbers for specific AEDs [Meador et al. 2008a, 2008b]. Given these limitations, signals for specific AEDs need to be reproduced in more than one registry to be confident of results.
Seizure frequency during pregnancy
Because the appropriate gold standard comparator group (i.e. nonpregnant WWE) has not been employed, the American Academy of Neurology (AAN) concluded that there is insufficient evidence to determine if seizure frequency changes occur in WWE during pregnancy [Harden et al. 2009a]. There has been wide variation in the reported range of women experiencing increased seizure frequency during pregnancy (9–75%). This variance may be due to differences in study populations and in other methodological issues. In addition, given the known pharmacokinetic changes during pregnancy, assessment of blood levels is needed in future studies [EURAP, 2006; Pennell and Hovinga, 2008; Pennell et al. 2008; Sabers, 2009; Sabers and Petrenaite, 2009; Petrenaite et al. 2009]. To provide more informed therapeutic strategies to maintain seizure control during pregnancy, clarification of factors that contribute to individual variance in increased seizures is important. Based on a number of studies from the literature, there is suggested increased seizure risk during pregnancy for lamotrigine and oxcarbazepine, both of which are glucuronidated for elimination [Petrenaite et al. 2005, 2009; Vajda et al. 2006b]. One positive finding concluded by the AAN found that WWE who were seizure free in the 9–12 months prior to pregnancy had an 85% chance of remaining so during pregnancy [Harden et al. 2009a].
Although some WWE can safely discontinue AEDs prior to pregnancy, most require long-term AED therapy through pregnancy to control seizures. It is of paramount importance to control tonic–clonic seizures, which can result in fetal intracranial hemorrhage, transient fetal bradycardia or heartbeat variability, miscarriage or trauma and even death to the mother and the fetus [Meador et al. 2008a]. Current treatment strategies in pregnant WWE employ AED monotherapy at the lowest dose to maintain stable blood levels and seizure control [Meador et al. 2008a].
Antiepileptic drug clearance in pregnancy
Data on AED clearance changes during pregnancy are lacking for many AEDs. For reasons largely unknown, considerable variability exists for AED clearance changes during pregnancy across AEDs and across individual patients [Harden et al. 2009c; Pennell et al. 2008a]. Of the AEDs studied, lamotrigine probably has the most marked clearance changes [Pennell et al. 2008a]. Data are inadequate for most AEDs during pregnancy on the relationship between decreased AED concentrations, seizure frequency, as well as the role of AED level monitoring. Throughout pregnancy, lamotrigine total and free clearance increased with a peak of 94% (total) and 89% (free) in the third trimester, according to one class I study [Harden et al. 2009c]. Importantly, when the lamotrigine level decreased to 65% of the preconceptional individualized target lamotrigine concentration, seizure frequency increased. Based on one class I and two class II studies [Pennell et al. 2008b; Tran et al. 2002; Pennell et al. 2004], changes in the lamotrigine levels were associated with increases in seizure frequency. These data support active monitoring of AED levels during pregnancy, in particular, lamotrigine [Harden et al. 2009c].
In addition to increased drug clearance, pregnancy causes dramatic changes in drug pharmacokinetics and leads to altered drug absorption, metabolism, and protein binding. Serial AED levels before pregnancy, during each trimester, and during the postpartum state may help guide appropriate dose augmentation or reduction [St Louis, 2009]. Unfortunately, there is no consensus as to the frequency that drug levels should be drawn during pregnancy. However, a reasonable approach could be to draw AED levels monthly and then modify this schedule appropriately based on seizure frequency.
Obstetrical risks
The AAN noted that ‘stronger evidence is needed to determine obstetrical risks for WWE, and the effect of specific AEDs on obstetrical outcomes also remains unexplored and deserves further study’ [Harden et al. 2009a]. However, subsequent to that determination, two publications reported an increase in obstetrical complications in WWE, especially if on AEDs [Kelly et al. 2009; Veiby et al. 2009]. According to the AAN, cesarean section rates were probably not increased, but a moderately increased risk could not be ruled out secondary to statistical imprecision and contradictory findings. Two recent studies noted increased risk of cesarean section with odds ratio (OR) 1.5 [95% confidence interval (CI) 1.3–1.9] in one study [Kelly et al. 2009] and OR 1.6 (95% CI 1.3—1.8) in the second study [Veiby et al. 2009]. However, these publications did not address contributing factors. The AAN stated that in WWE who do not smoke there was likely no increased risk of preterm birth but a study challenged this finding [Veiby et al. 2009]. Recently, a hospital-based, retrospective study [Borthen et al. 2011] reported an increase in obstetrical complications in WWE on AEDs compared with a control group without epilepsy. The results showed that WWE on AEDs had an increased risk of severe preeclampsia (OR 5.0; 95% CI 1.3–19.9), bleeding in early pregnancy (OR 6.4; 95 CI 2.7–15.2), induction (OR 2.3; 95% CI 1.2–4.3) and cesarean section (OR 2.5; 95% CI 1.4–4.7) adjusted for maternal age, parity, education, smoking, medical conditions and body mass index >30 kg/m2 [Borthen et al. 2011]. A number of these studies suffer from limitations, including retrospective data collection, use of national databases, and lack of specific information on AED use, dose, anticonvulsant blood levels, and epilepsy type.
Is there increased risk of pregnancy-induced hypertension in WWE? There was insufficient evidence to support or refute increased risk of pregnancy-induced hypertension based on results from two conflicting class II studies [Harden et al. 2009a]. According to a class one study [Viinikainen et al. 2006], WWE taking AEDs probably do not have a moderately increased risk of premature contractions and premature labor and delivery during pregnancy. However, according to one class II study [Hvas et al. 2000], it is possible that WWE who smoke are at substantially increased risk of premature contractions and premature labor and delivery during pregnancy compared with smokers who do not have epilepsy. It is probable that WWE on AEDs do not have substantially increased risk of late pregnancy-related bleeding complications as per one class I and one class III study [Harden et al. 2009a]. However, because of a lack of statistical precision in these studies, a moderately increased risk cannot be excluded. The data are inadequate to support or refute an increased risk of spontaneous abortion in WWE [Harden et al. 2009a].
Postpartum depression
Depression and psychological stress during and after pregnancy can have an adverse affect on outcomes in both the mother and child. This finding is supported by multiple publications [O’Connor et al. 2003; Van den Bergh et al. 2005; Alder et al. 2007; Horwitz et al. 2007; Newport et al. 2007; Deave et al. 2008; Hay et al. 2008]. According to one study, there is an increased risk for depression in WWE [Ettinger et al. 2004], and there is an even higher risk for postpartum depression suggested by three small studies [Turner et al. 2006, 2009; Galanti et al. 2009]. However, limited sample sizes and lack of comparator groups leave doubt in these three studies.
Neonatal outcomes
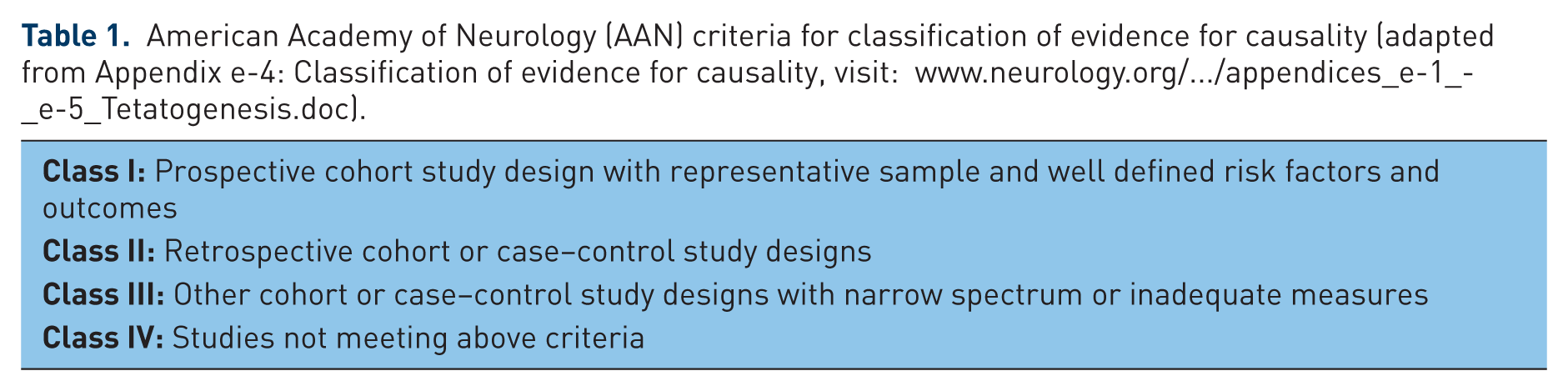
With the exception of data on malformations, data in WWE on neonatal outcomes are insufficient. SGA is important due to increased risk of infant morbidity (e.g. neurodevelopment) and mortality [Lundgren et al. 2008]. Based on two class II studies, the AAN concluded there is a probable increased risk for SGA [Harden et al. 2009b]; and three recent studies also found increased SGA risk [Kelly et al. 2009; Veiby et al. 2009; Chen et al. 2009]. See Table 1 for AAN classification of evidence of causality. Unfortunately, no studies have delineated many likely important contributing factors, including differences across AEDs, levels of in utero exposure, or epilepsy type. Based on two class II studies, the AAN concluded there is probably no increased risk of perinatal death, however a recent study did find an increased risk of fetal/infant death at 6 of 272 (2.2%) in WWE compared with 1 of 310 (0.3%) in controls (p = 0.05) [Mawer et al. 2010]. There is possibly a lower 1 min Apgar score according to the AAN based on one class II study, and one recent study found lower 5 min Apgar scores in children of WWE [Veiby et al. 2009]; however, many likely important contributing factors have not been assessed, including differential AED effects. Additionally, multiple pertinent outcomes with potential long-term implications on childhood health have not been addressed sufficiently [Meador et al. 2008a; Harden et al. 2009a, 2009b, 2009c].
American Academy of Neurology (AAN) criteria for classification of evidence for causality (adapted from Appendix e-4: Classification of evidence for causality, visit: www.neurology.org/…/appendices_e-1_-_e-5_Tetatogenesis.doc).
Mechanisms of anatomical teratogenesis
AEDs can produce both anatomical (i.e. MCM) or behavioral (i.e. cognitive) teratogenicity. Several theories have been posited for the mechanisms of teratogenesis in WWE on AEDs. Although the exact mechanisms are uncertain, current proposed mechanisms include folate deficiency, ischemia, neuronal suppression, reactive intermediates (e.g. free radicals or epoxides), and AED-induced neuronal apoptosis [Meador et al. 2007]. It seems likely that the mechanisms underlying anatomical and behavioral teratogenesis are different because the highest risk of anatomical defects is from first-trimester AED exposure, but the highest risk of behavioral defects appears to be primarily from third-trimester exposure. The leading hypothesis for the mechanism leading to anatomical malformations involves free radical formation, while the leading hypothesis for the mechanism leading to behavioral/cognitive dysfunction involves AED-induced apoptosis and associated dysfunction in surviving neurons. Genetic predisposition likely plays a role and could involve interaction of teratogens with multiple-liability genes. This, in part, may explain the observed individual variability [Finnell and Chernoff, 1987].
Pregnancy outcomes with regard to congenital malformations
In recent years, several AED pregnancy registries have been established leading to new insights into teratogenic risks of AEDs. Pregnancy outcomes and other issues for WWE were examined for the new AAN guidelines, which included recommendations for patient care and future research [Harden et al. 2009a, 2009b, 2009c].
There is an increased risk for MCMs in children of WWE versus the general population which has a frequency of 1.6–2.1% at birth [Meador et al. 2008a]. There is variability in the risk estimates among studies, but a recent publication indicates 4.5% (OR 2.6) frequency for MCMs in AED monotherapy in utero exposure and 8.6% (OR 5.1) for AED polytherapy [Meador et al. 2008a]. The most common MCMs associated with AEDs are heart malformations, orofacial defects, urologic defects, skeletal abnormalities, and neural tube defects. Specific examples include but are not limited to ventricular septal defect, cleft lip/cleft palate, hypospadias, radial ray defects, phalangeal hypoplasia, and spina bifida [Meador et al. 2008a].
Anatomical teratogenesis associated with individual antiepileptic drugs
Since the 1960s, AEDs have been known to have teratogenic potential. Since seizures carry the risk of potential injury or even death, most WWE cannot afford to discontinue AEDs. Therefore, it is important to delineate which AEDs produce the best seizure control while minimizing teratogenicity. AEDs taken during the first trimester of pregnancy may increase the risk of MCMs in children born to WWE. The AAN guidelines and a recent meta-analysis concluded that that risk is highest for valproate out of all the AEDs [Harden et al. 2009b; Meador et al. 2008b]. The recent European and International Registry of Antiepileptic Drugs in Pregnancy (EURAP) results confirmed the increased risk for valproate, but also demonstrated dose-dependent risks for other AEDs [Tomson et al. 2011].
Carbamazepine
Carbamazepine has the most data in pregnancy compared with other AEDs. The AAN concluded that carbamazepine is probably not associated with a substantial increased risk of MCMs. One class I study showed no increased risk in children born to WWE taking carbamazepine [Morrow et al. 2006]. The North American Pregnancy Registry reported in infants exposed in utero to carbamazepine a 2.6% overall risk of major malformations versus 1.62% in the general population; this difference was not statistically significant [Holmes and Wyszynski, 2004]. There was increased risk for cleft lip/palate and neural tube defect noted by the same pregnancy registry [Holmes and Wyszynski, 2004]. The recent large European Surveillance of Congenital Anomalies (EUROCAT) study confirmed the risk for spina bifida for carbamazepine monotherapy (OR 2.6, 95% CI 1.2—5.3 compared with no AED exposure). The risk for carbamazepine did not differ from other AED monotherapies but was less than valproic acid [Jentink et al. 2010a]. However, the risk of cleft lip/palate was not confirmed in the EUROCAT study. This study had 19 population-based registries of congenital malformations in Europe based on over 3.8 million births. Another study with data taken from the EURAP epilepsy and pregnancy registry (an observational cohort study representing a collaboration of physicians from 42 countries) prospectively monitored pregnancies exposed to monotherapy with different doses of carbamazepine, lamotrigine, valproic acid, or phenobarbital with primary endpoint of MCMs detected up to 12 months after birth [Tomson et al. 2011]. This study found a dose-dependent effect for carbamazepine and also found that risks of malformation were significantly higher with carbamazepine at doses greater than 400 mg per day compared with lamotrigine (see Table 2 for details).
Number of offspring with malformations for four monotherapies at different doses up to 1 year, taken from the European and International Registry of Antiepileptic Drugs in Pregnancy (EURAP), adapted from [Tomson et al. 2011].
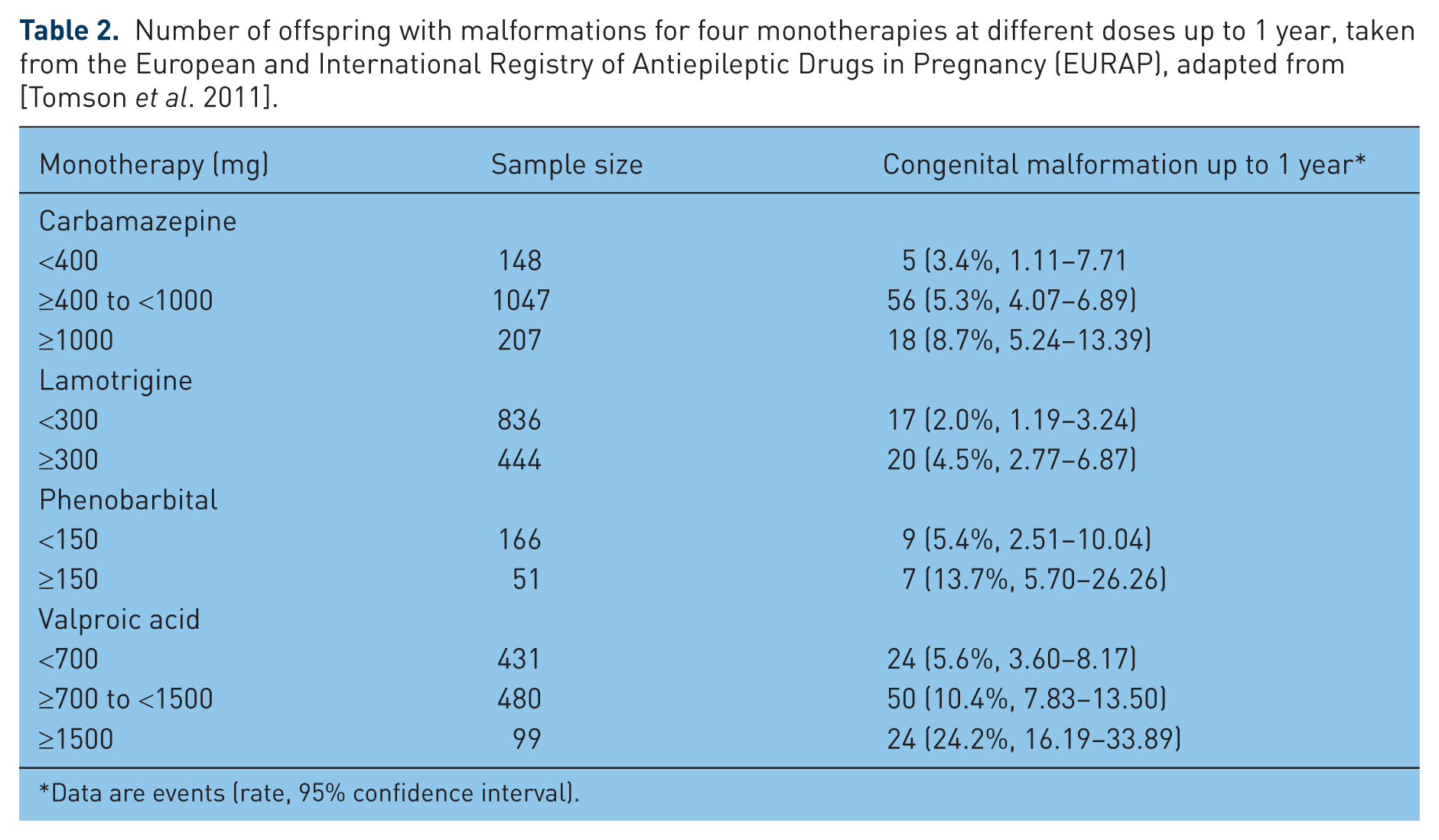
Data are events (rate, 95% confidence interval).
Lamotrigine
Of the newer AEDs, lamotrigine has the most data for pregnancy outcomes with regard to risk of MCMs. A meta-analysis found a 2.91% risk of MCM [Meador et al. 2008b]. One registry reported an increased risk of cleft lip/palate compared to a control group of over 200,000 unexposed infants from Brigham and Williams Hospital in Boston [Holmes et al. 2006], but this was not confirmed in another study [Dolk et al. 2008]. One class I study [Morrow et al. 2006] observed no increased risk of MCMs in the offspring of WWE taking lamotrigine [relative risk (RR) 0.92, 95% CI 0.41–2.05] but was insufficiently sensitive to exclude a substantially increased risk. The AAN concluded that there is insufficient evidence to determine if lamotrigine increases the risk of MCMs in the offspring of WWE [Harden et al. 2009b]. The AAN guidelines also concluded that lamotrigine probably has a lower rate of teratogenic outcomes compared with valproate [Harden et al. 2009b]. Recent analysis of data from the EURAP epilepsy and pregnancy registry [Tomson et al. 2011] assessed rates of MCMs in 1402 pregnancies exposed to carbamazepine, 1280 on lamotrigine, 1010 on valproic acid, and 217 on phenobarbital. An increase in malformation rates with increasing dose at the time of conception was recorded for all drugs [Tomson et al. 2011]. This study found that compared with lamotrigine monotherapy at doses less than 300 mg per day [2.0% (17 events), 95% CI 1.19–3.24], risks of malformations (up to a year) were significantly higher with valproic acid and phenobarbital at all investigated doses, and with carbamazepine at doses greater than 400 mg per day [Tomson et al. 2011] (see Table 2 for data on the four drugs, including doses, sample size, and ORs of congenital malformations)
Levetiracetam
Preliminary findings on levetiracetam from the UK Registry revealed 3 of 117 exposed pregnancies had MCMs (2.7%; 95% CI 0.9–7.7%) [Hunt et al. 2006]. The sample size is small so additional studies are needed to confirm these findings.
Phenobarbital
Five (6.5%) of 77 pregnancies with exposure to phenobarbital monotherapy were associated with major malformations (95% CI 2.1–14.5%), which was significantly greater than the background rate (1.62%) (RR 4.2; 95% CI 1.5–9.4) [Holmes et al. 2004]. In addition, a dose dependent effect on MCMs was found by the EURAP registry [Tomson et al. 2011].
Phenytoin
The Australian AED Pregnancy Registry reported a 10.5% risk of birth defects with fetal phenytoin exposure compared with 4.3% in those not exposed to AEDs [Vajda et al. 2006a, 2007a, 2007b]. A meta-analysis found a 7.36% risk of MCMs for phenytoin monotherapy compared with 3.26% in those not exposed to AEDs, but this difference was not statistically significant due to large variance in the data [Meador et al. 2008b]. The UK registry reported a 3.7% risk for phenytoin compared with 3.5% in those without AED exposure [Morrow et al. 2006].
Topiramate
The UK Registry examined pregnancies with topiramate monotherapy exposure and reported 3 of 70 had MCMs (4.8%; CI 1.7–13.3) [Hunt et al. 2008]. These preliminary results await confirmation. The US Food and Drug Administration recently release a warning for increase of oral cleft (1.4% versus 0.38–0.55%) versus other AEDs (www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm245777.htm). This warning is based on unpublished data from the North American AED Pregnancy Registry and the UK AED Pregnancy Registry.
Valproate
The AAN practice parameters concluded that valproate monotherapy possessed increased risk of MCMs compared to phenobarbitol, carbamazepine, phenytoin and lamotrigine [Harden et al. 2009b]. The AAN recommended avoidance of valproate in the first trimester of pregnancy due to this risk [Harden et al. 2009b]. This recommendation is supported by a recent meta-analysis, which found an overall risk of 10.73% for MCMs in children exposed in utero to valproate [Meador et al. 2008b]. Valproate’s effect appears to be dose dependent, with doses greater than 1000 mg per day posing the greatest threat [Artama et al. 2005; Vajda et al. 2007a; Tomson et al. 2011]. The recent large EUROCAT study found that use of valproate monotherapy was associated with significantly increased risks for six specific malformations; the odds ratios were, spina bifida 12.7-fold increased risk (95% CI 7.7–20.7); atrial septal defect 2.5 (95% CI 1.4–4.4); cleft palate 5.2 (95% CI 2.8–9.9); hypospadias 4.8 (95% CI 2.9–8.1); polydactyly 2.2 (95% CI 1.0–4.5); and craniosynostosis 6.8 (95% CI 1.8–18.8) [Jentink et al. 2010b]. If possible, for WWE who are pregnant, avoidance of VPA should be considered to avoid the risk of MCMs.
Benzodiazepines
Previous studies have concerned the possible teratogenic effect of benzodiazepines [Dolovich et al. 1998; Eros et al. 2002; Laegreid et al. 1989, 1990; Wikner et al. 2007]. The results of these studies are somewhat conflicting, but the largest studies with a minimum of bias indicate no marked teratogenicity [Eros et al. 2002; Wikner et al. 2007]. The main exceptions are the studies by Laegreid and colleagues which concern women who have used high amounts of such drugs.
Other antiepileptic drugs
There are insufficient data to determine the risk for other AEDs. However, a recent population-based cohort study [Molgaard-Nielsen and Hviid, 2011] of 837,795 live-born infants in Denmark from 1 January 1996 to 30 September 2008 may shed some light on this subject. Of the 1532 infants exposed to lamotrigine, oxcarbazepine, topiramate, gabapentin, or levetiracetam during the first trimester, 49 were diagnosed with a major birth defect compared with 19,911 of the 836,263 who were not exposed to an AED [3.2% versus 2.4%, respectively; adjusted prevalence odds ratio (POR) 0.99; 95% CI 0.72–1.36]. A major birth defect was diagnosed in 38 of 1019 infants (3.7%) exposed to lamotrigine during the first trimester (adjusted POR 1.18; 95% CI 0.83–1.68), in 11 of 393 infants (2.8%) exposed to oxcarbazepine (adjusted POR 0.86; 95% CI 0.46–1.59), and in 5 of 108 infants (4.6%) exposed to topiramate (adjusted POR 1.44; 95% CI 0.58–3.58). Gabapentin (n = 59) and levetiracetam (n = 58) exposure during the first trimester was uncommon, with only 1 (1.7%) and 0 infants diagnosed with birth defects, respectively. This study concluded that among live-born infants in Denmark, first-trimester exposure to lamotrigine, oxcarbazepine, topiramate, gabapentin, or levetiracetam compared with no exposure was not associated with an increased risk of major birth defects [Molgaard-Nielsen and Hviid, 2011]. However, sample sizes were small except for lamotrigine and oxcarbazepine.
Polytherapy
Polytherapy during the first trimester is probably associated with an increased risk of MCMs as per the AAN practice parameters [Harden et al. 2009b]. The AAN advised that, if possible, AED polytherapy should be avoided in pregnancy to decrease the risk for MCMs [Harden et al. 2009b]. According to a recent study, the risk of malformations was 3.1–7.8% in infants exposed to AED monotherapy, 8.3–13.5% in infants exposed to two AEDs, and more than 13.5% in infants exposed to three AEDs [Kaaja et al. 2003]. Specific AED combinations carry uncertain risk for MCMs with the exception that polytherapy with valproate has a higher risk than polytherapy without valproate [Harden et al. 2009a; Morrow et al. 2006]. A recent study of a cohort of women from the North American AED Pregnancy Registry found that the risk of malformations among infants exposed to lamotrigine and carbamazepine as polytherapy during the first trimester was higher than the corresponding monotherapies only when the polytherapy included valproate [Holmes et al. 2011].
One study [Vajda et al. 2010] that utilized statistical analysis of malformation rate and AED exposure data from the Australian Register of Antiepileptic Drugs in Pregnancy showed the calculated RR value for AED polytherapy compared with monotherapy was below 1.0 in only three of 14 literature publications. In their register, the overall risks at 1 year postnatally for fetal malformations were 5.32% of 282 AED polytherapy pregnancies, and 7.84% of 791 AED monotherapy pregnancies, a RR of 0.68 (95% CI 0.39–1.17). For pregnancies exposed to valproate, the RR of fetal malformation (0.39, 95% CI 0.20–0.89) was lower in polytherapy (7.26%) than in monotherapy (17.9%); the difference did not depend on valproate dosage. The RR values for fetal malformation were not significantly different for AED polytherapy and monotherapy when valproate was not involved. Logistic regression suggested that coadministration of lamotrigine may have reduced the malformation risk from valproate [Vajda et al. 2010]. The present results of this particular study suggest that it is therapy with valproate, rather than the number of AEDs taken during pregnancy, that is the primary factor associated with the presence of fetal malformations in the offspring [Vajda et al. 2010].
Conclusions for anatomical teratogenesis
Valproate poses special risk for MCMs (10.7%). Phenobarbital has possible increased risk (6.5%). Topiramate increases risk of oral cleft (1.4%). The risk of spina bifida is increased for valproate (12.7 times) and carbamazepine (2.6 times). Dose-dependent risks have been demonstrated for several AEDs, and could possibly exist across AEDs as a drug class. The absolute risks of most AEDs and specific polytherapy combinations are unknown.
Pregnancy outcomes with regard to neurodevelopment
Mechanisms of behavioral teratogenesis
Ethanol is known to produce widespread neuronal apoptosis leading to neurobehavioral deficits in the developing brain [Ikonomidou et al. 2000]. There is also neuronal dysfunction found in the remaining neurons [Medina et al. 2003]. These findings led to use of the apoptotic model in studies with AEDs. AEDs that have been observed to produce widespread neuronal apoptosis in neonatal rat brain include clonazepam, diazepam, phenobarbital, phenytoin, vigabatrin, and valproate [Bittigau et al. 2002, 2003; Asimiadou et al. 2005; Stefovska et al. 2008; Ikonomidou and Turski, 2010]. The effect is dose dependent, occurs at therapeutically relevant blood levels, and can occur with single dose exposure. It is also a synergistic effect since two AEDs, given at below threshold dosages, can still trigger the full apoptotic response. Many AEDs, which do not produce apoptosis in monotherapy, can enhance apoptosis induced by another AED [Katz et al. 2007]. These include carbamazepine, lamotrigine, or topiramate [Glier et al. 2004; Manthey et al. 2005; Kim et al. 2007]. This finding may suggest that polytherapy could increase the risk. The only AED of those tested thus far that does not produce apoptosis in monotherapy or enhance apoptosis of other AEDs is levetiracetam [Manthey et al. 2005]. However, most AEDs have not been tested. Animal experiments like these naturally raise concern that some commonly utilized AEDs could produce similar adverse effects in children of WWE exposed in utero, but clinical studies are needed to confirm if similar effects occur in the human brain.
Another proposed mechanism that could potentially induce teratogenesis is AED alterations to neurotransmitter systems. This can affect both neuronal proliferation and migration. Multiple AEDs inhibit glutamate action, including felbamate and topiramate. Gamma-amino butyric acid (GABA) agonists include phenobarbital, benzodiazepines, and valproate. Neuronal differentiation and migration are largely regulated by the neurotransmitter medium in the developing brain. According to animal studies, blockade of N-methyl-
Cognitive effects of maternal epilepsy in absence of antiepileptic drugs during pregnancy
Based on a prospective, blinded, and observational study [Gaily et al. 2004] and a blinded retrospective study [Holmes et al. 2000], no IQ difference was found between children of untreated WWE and healthy controls.
Cognitive effects of maternal seizures during pregnancy
In children exposed in utero to self-limiting (i.e. no status epilepticus) generalized tonic–clonic seizures, two prospective population-based studies found no IQ impairment [Gaily et al. 1988, 2004). However, verbal IQ was significantly reduced in children exposed to more than four generalized tonic–clonic seizures based on a retrospective study [Adab et al. 2004]. It has been documented in case reports that prolonged seizures and status epilepticus are a serious threat to both mother and fetus [Hiilesman, 1996].
Effects of fetal antiepileptic drug exposure on neurodevelopment
Animal studies have shown that fetal exposure to AEDs at doses lower than the threshold required to produce congenital malformations is known to produce cognitive and behavioral abnormalities [Meador et al. 2011].
Neurodevelopmental effects of individual antiepileptic drugs
Carbamazepine
In a prospective, evaluator-blinded, observational study with matched controls, no effect of fetal carbamazepine exposure on IQ was reported [Scolnik et al. 1994]. In a population-based, longitudinal follow-up study of preschool children, no adverse effects of fetal carbamazepine exposure were seen [Wide et al. 2002]. A retrospective, blinded study controlling for maternal IQ in 52 children of WWE exposed to carbamazepine versus 80 unexposed children found no IQ difference [Adab et al. 2004]. In a prospective, population-based, blinded, observational study controlling for maternal education, no difference in IQ was seen in 86 children of WWE exposed to carbamazepine monotherapy versus 45 children of WWE on no AED or 141 healthy control children [Gaily et al. 2004]. When these data were pooled with data from another prospective population-based study, mental retardation occurred in only 1 of 84 children exposed to polytherapy [Gaily et al. 1988, 2004]. In a population-based, evaluator-blinded study, again no IQ difference was seen in children of WWE exposed to carbamazepine versus no AED [Eriksson et al. 2005]. A retrospective population-based study on autism spectrum disorder in 80 children exposed to carbamazepine monotherapy showed no difference in frequency from the general population [Rasalam et al. 2005]. At age 3 years, children exposed in utero to carbamazepine did not differ from lamotrigine or phenytoin, but had better IQ outcomes than valproate in a prospective observational multicenter study [Meador et al. 2009]. Based on the same study, a follow-up investigation showed fetal exposure to carbamazepine was associated with a dose-related reduction in language abilities at age 3 years, but this finding requires replication [Meador et al. 2011].
Lamotrigine
Children at age 3 years exposed in utero to lamotrigine did not differ from those exposed to carbamazepine or phenytoin, but had better IQ outcomes than those exposed to valproate at age 3 in a prospective observational multicenter study [Meador et al. 2009]. In a follow-up investigation, dose-related effects of fetal AED exposure on verbal and nonverbal cognitive measures were assessed in exposed 3-year-old children [Meador et al. 2011]. This study sought to determine if differential long-term neurodevelopmental effects exist across four commonly used AEDs (carbamazepine, lamotrigine, phenytoin, and valproate). Cognitive outcomes were calculated in 216 children from the Differential Ability Scales, Preschool Language Scale, Peabody Picture Vocabulary Test and Developmental Test of Visual-Motor Integration. Verbal abilities were lower than nonverbal in children exposed in utero to each drug. No dose effects were seen for lamotrigine and phenytoin [Meador et al. 2011].
Levetiracetam
A recent study comparing levetiracetam to valproate and to a control group reported that children exposed to levetiracetam obtained higher developmental scores at less than age 24 months compared with children exposed to valproate (n = 51 levetiracetam; n = 44 valproate; p < 0.001). The levetiracetam group did not differ from control children (n = 97; p = 0.62) [Shallcross et al. 2011]. Limitations of the study included young age at assessment, retrospective approach, and completer rates of only 58% for levetiracetam and 37% for valproate. So, replication of the findings is needed. Given these limitations and that this is the only study on neurodevelopment effects of levetiracetam, caution should be exercised when utilizing this source for clinical application.
Phenobarbital
According to a study done in 1976, no difference in IQ was seen in 35 children of WWE exposed in utero to phenobarbital monotherapy versus 4705 children of mothers without epilepsy [Shapiro et al. 1976]. In contrast, two studies of separate cohorts of 114 adult men of mothers without epilepsy, exposed in utero to phenobarbital, found approximately 0.5 standard deviation lower verbal IQ scores in the exposed men [Reinisch et al. 1995]. Young children exposed to phenobarbital have also been shown to have statistically different IQ scores than control groups. While not a study of fetal exposure, one investigation of phenobarbital in young children with febrile seizures offers insights into the effects of phenobarbital on the immature brain. A total of 217 children with febrile seizures were randomized to a phenobarbital or placebo, and tested 2 years later; those exposed to phenobarbital had lower IQ [Farwell et al. 1990]. Avoidance of phenobarbital in WWE during pregnancy, if possible, may be considered to reduce the risk of poor cognitive outcomes (level C) [Harden et al. 2009b].
Phenytoin
In two prospective, blinded, population-based studies that controlled for socioeconomic class or maternal educational level, no effect of fetal phenytoin exposure on IQ was seen [Shapiro et al. 1976; Gaily et al. 1988]. Another study drawn from a different patient pool but of the same design noted lower IQ at age 7 years in children of WWE exposed to phenytoin versus healthy control children of mothers without epilepsy [Hanson et al. 1976]. In a population-based longitudinal follow-up study of preschool children, slightly lower scores for locomotor development were reported in phenytoin-exposed children versus fetal carbamazepine-exposed children and unexposed children [Wide et al. 2002]. In a case– control, blinded-evaluator study, phenytoin-exposed children had significantly lower IQ scores [Vanoverloop et al. 1992]. Although a prospective, blinded observational study reported lower IQ for children with fetal phenytoin exposure compared with matched control [Scolnik et al. 1994], no effect was seen when maternal IQ was considered [Loring et al. 1994]. Children at age 3 who were exposed to phenytoin in utero had better IQ outcomes than those exposed to valproate but did not differ from those exposed to carbamazepine or lamotrigine in a prospective observational multicenter study of monotherapy [Meador et al. 2009]. The AAN recommended avoiding phenytoin in WWE during pregnancy based on level C evidence [Harden et al. 2009b], but firm conclusions on the risks of phenytoin will require additional studies.
Valproate
Two prospective, population-based, evaluator-blinded studies demonstrated lower verbal IQ or full-scale IQ in children of WWE exposed in utero to valproate monotherapy compared with children with carbamazepine monotherapy or no AED exposure [Gaily et al. 2004; Eriksson et al. 2005]. Unfortunately, the size of the sample valproate monotherapy group limited these studies (n = 26 across the two studies). In addition, the studies showed significantly lower maternal education or IQ in the valproate group compared with other WWE. In a retrospective study, there was an increased need for special education in children exposed to valproate monotherapy compared with other monotherapies or the unexposed group [Adab et al. 2001]. In a large retrospective investigation that controlled for maternal IQ, lower verbal IQ (about 10 points) was seen in children exposed in utero to valproate (n = 41) versus other monotherapy groups and versus an unexposed group [Adab et al. 2004]. The decrease in IQ in the valproate group was a dose-dependent effect. Another study showed children exposed in utero to valproate had lower IQ (7–9 points) at age 3 years compared with other AEDs (carbamazepine, lamotrigine, or phenytoin); this was a prospective, observational, evaluator-blinded, multicenter study, which enrolled pregnant WWE on AED monotherapy [Meador et al. 2009]. The adverse effect of valproate was dose dependent [Meador et al. 2009]. According to a follow-up analysis in the same study, verbal and nonverbal cognitive outcomes were reduced in children exposed in utero to valproate monotherapy versus carbamazepine, lamotrigine, and phenytoin. Again, the effect was dose dependent, and the impact of the effect appeared greater in verbal than in nonverbal abilities [Meador et al. 2011]. Two retrospective and one prospective study have posited an increased risk for autistic spectrum disorder or behavioral abnormalities in valproate-exposed children [Rasalam et al. 2005; Bromley et al. 2008; Vinten et al. 2009]. In a recent study [Nadebaum et al. 2011], IQ was evaluated in school-aged children exposed to valproate and polytherapy during pregnancy (using the Wechsler Intelligence Scale for Children – fourth edition). The study results suggested that valproate has a dose-dependent negative impact on verbal intellectual abilities, and may also affect working memory. In addition, the possibility that inclusion of valproate in polytherapy regimens may underlie reduced mean scores was discussed [Nadebaum et al. 2011]. Avoiding valproate in WWE during pregnancy, if possible, should be considered to reduce the risk of poor cognitive and verbal outcomes (level B) [Harden et al. 2009b].
Benzodiazepines
The risks of fetal exposure to cognition and behavior due to benzodiazepines are largely unknown secondary to a lack of adequate data in human studies.
Other antiepileptic drugs
The risks of fetal exposure to cognition and behavior due to other AEDs are largely unknown secondary to a lack of adequate data in human studies.
Polytherapy
No difference in IQ was found among children exposed to phenytoin and phenobarbital polytherapy versus other children of WWE according to one prospective study done in the 1970s [Shapiro et al. 1976]. Subsequent prospective studies have found otherwise. Children exposed in utero to AED polytherapy had lower cognitive scores than healthy controls and children of WWE exposed to monotherapy [Lösche et al. 1994]. Children exposed in utero to AED polytherapy had impaired verbal and nonverbal IQ compared with children exposed to monotherapy alone [Koch et al. 1999; Gaily et al. 2004]. If possible, AED polytherapy should be avoided in WWE to reduce the risk of poor cognitive and verbal outcomes.
Conclusions on cognitive outcomes from human studies
From the current literature, the most salient point regarding a specific AED is that fetal valproate exposure poses a special risk for cognitive development in the child, and that this effect is dose dependent. As mentioned earlier, valproate also carries the risk of anatomical teratogenesis in addition to the behavioral/cognitive risks. Carbamazepine and lamotrigine appear to have low risk based on current studies. Due to inconsistent or absent data, the risks for other AEDs are uncertain. It appears that polytherapy exposure poses a risk to cognitive development based on limited studies; however, the risks of specific AED combinations are unclear. A myriad of questions remain unresolved, and there is a critical need for more research.
Folate effects
According to one study, folate deficiency during pregnancy reduces neurogenesis and increases apoptosis [Craciunescu et al. 2004], but folate nutritional status during pregnancy has not been proven to impact neurodevelopment [Tamura et al. 2005; Meador et al. 2007]. Does preconceptional folic acid supplementation in WWE reduce the risk for MCMs in the fetus? In the current literature, there are insufficient data to answer this question. The risk for MCMs in offspring of WWE is possibly decreased by folic acid supplementation based on two adequately sensitive class III studies [Betts and Fox, 1999; Kaaja et al. 2003]. The current recommendation in WWE is that preconceptional folic acid supplementation may be considered to reduce the risk of MCMs (level C) [Harden et al. 2009c]. In one study [Wyszynski et al. 2005] of a sample from the North American Antiepileptic Drug Pregnancy Registry, 149 valproate-exposed women (all of whom were on folic acid supplementation) during the first trimester of pregnancy had 16 children with neural tube defects identified (proportion 10.7%; 95% CI 6.3–16.9%). The prevalence in the internal comparison group was 2.9% (95% CI 2.0–4.1%; OR 4.0, 95% CI 2.1–7.4; p < 0.001). Assuming a 1.62% prevalence in the external comparison group, the RR of having an affected offspring for valproate-exposed women was 7.3 (95% CI 4.4–12.2; p < 0.001). The mothers of all 16 infants took either prenatal vitamins/multivitamins or supplemental folic acid in the periconceptional period with a dose average of 1.36 mg and a range of 0.4–5 mg. These findings demonstrate the occurrence of neural tube defects in spite of periconceptional supplementation with folic acid. This finding in this case series should not be considered a definitive assessment of whether or not periconceptional supplementation with folic acid reduces the occurrence of neural tube defects when the mother is taking valproate as monotherapy [Wyszynski et al. 2005].
In one prospective, observational, registration and follow-up study [Morrow et al. 2009], 1935 cases reported to have received preconceptual folic acid (patients were included whether or not they were on AEDs), 76 MCMs (3.9%; 95% CI 3.1–4.9) and eight neural tube defects (0.4%; 95% CI 0.2–0.8) were identified. For 2375 women who were reported to have received folic acid but not until later in the pregnancy (n = 1825) or not at all (n = 550), there were 53 outcomes with an MCM (2.2%; 95% CI 1.7–2.9) and eight neural tube defects (0.34%; 95% CI 0.2–0.7). This study [Morrow et al. 2009] supports the view that the increased risk of MCMs recorded in this group may occur through mechanisms other than that of folic acid metabolism.
In a case–control study [Jentink et al. 2009] with data from a population-based registry (EUROCAT Northern Netherlands) of congenital malformations the risk for spina bifida was decreased with folate use in AED unexposed pregnancies (OR 0.5; 95% CI 0.3–0.7), but not among valproate-exposed pregnancies (OR 1.0; 95% CI 0.1–7.6). Further research is needed to establish the most effective form and dose of folic acid in women who use valproate [Jentink et al. 2009].
The result concerning folate supplementation from the EURAP study [Tomson et al. 2011] showed folate supplementation was associated with a greater risk of MCMs. However, this possibly shows confounding by indication because women at greater risk are more likely to take folate. The UK registry (Morrow et al. 2009] reported rates of MCMs in offspring of women on AEDs with appropriate folate intake that were at least as high as those in women on AEDs without appropriate folate intake.
Though the data are insufficient to show that folic acid supplementation is effective in WWE, it is generally recommended to reduce risk of MCMs during pregnancy. There is no evidence of harm. Therefore, the current recommendation is that women with or without epilepsy be supplemented with at least 0.4 mg folic acid daily prior to and during pregnancy. The current literature is insufficient to address the dosing of folic acid and does not address if there is a dose effect protective benefit to WWE taking AEDs [Harden et al. 2009c].
Vitamin K
In neonates born to WWE taking AEDs, what is the risk of hemorrhagic disease? The evidence is not sufficient to determine if the risk of neonatal hemorrhagic complications in the newborns of WWE taking AEDs is substantially increased (one inadequately sensitive class II study) [Harden et al. 2009c]. Does prenatal vitamin K supplementation reduce the risk of hemorrhagic complications in the newborns of WWE taking AEDs? The evidence is insufficient to determine the answer. In newborns of WWE, there is inadequate evidence to support or refute a benefit of prenatal vitamin K supplementation for risk reduction of hemorrhagic complications. Newborns exposed to enzyme-inducing AEDs in utero should routinely receive vitamin K at delivery, as is the routine practice for all newborns [Harden et al. 2009c].
Conclusions
Though discontinuing AEDs prior to pregnancy may be an option in some WWE with mild seizures, most are unable to safely stop AEDs. Therefore, of necessity, their fetus must be exposed. Present guidelines are constructed to minimize risk to the fetus and the mother while obtaining maximal benefit of seizure control. This includes optimizing epilepsy treatment prior to conception, choosing the most effective AED to control seizures, using monotherapy and lowest effective dose if possible, and supplementing with folate. The guidelines also recommend avoiding valproate when possible. Sudden cessation or lowering of AEDs should not be done by a WWE without consultation with her physician [Meador et al. 2008a]. Once it is determined that a WWE is to continue on AEDs during pregnancy, she must be informed of the relative risks and guided appropriately in her therapy. Delineation of these risks should be placed in the context that most children born to WWE are normal.
Footnotes
The authors have received no sources of financial or material support for this article.
The authors declare no conflicts of interest in preparing this article.