
Abstract
Cushing’s syndrome (CS) is characterized by excessive endogenous cortisol production and necessitates prompt intervention. We report a case of adrenocortical carcinoma (ACC) complicated by CS in a patient with a history of immune thrombocytopenia (ITP). Following treatment with metyrapone and surgical resection aimed at reducing cortisol levels, the patient experienced an ITP relapse. To our knowledge, this is the first report demonstrating the clinical impact of rapid cortisol fluctuations induced by CS treatment on ITP control. The patient required concurrent management with exogenous steroids to maintain platelet counts while correcting hypercortisolism. This case highlights the immunosuppressive role of endogenous cortisol and underscores the need for careful monitoring in patients with coexisting autoimmune disorders undergoing treatment for CS. Awareness of this interaction may inform individualized steroid tapering strategies and improve outcomes in similar clinical scenarios.
Plain language summary
We present the case of a 67-year-old woman who had two illnesses: adrenal cancer and a condition called immune thrombocytopenia. Her adrenal cancer caused her body to produce too much cortisol, a hormone that helps regulate stress. She also had a history of immune thrombocytopenia, an autoimmune disease where her body’s immune system mistakenly attacks and destroys its own platelets, which are cells needed for blood clotting. To treat her, we used medication to reduce her cortisol levels and performed surgery to remove the adrenal tumor. However, immediately after her cortisol levels dropped, her platelet count fell sharply, and she developed severe bruising on her body. To manage this relapse, we treated her with steroid medication and other therapies, and her platelet count eventually recovered. This case suggests that the high level of cortisol in her body was acting to suppress her immune system’s activity. When her cortisol level suddenly decreased, it likely triggered her immune system to become overactive, causing her immune thrombocytopenia to worsen. For patients who have both high cortisol levels and an autoimmune disease, it is crucial for doctors to carefully manage cortisol levels and closely monitor the autoimmune condition. When adjusting steroid doses, doctors should proceed with caution to prevent serious complications.
Introduction
Adrenocortical carcinoma (ACC) is a rare malignancy with a poor prognosis, often complicated by endocrine dysfunction. 1 Approximately 50%–75% of patients with ACC exhibit endocrine symptoms, most commonly hypercortisolism due to excessive cortisol secretion, leading to Cushing’s syndrome (CS). Although remission of hypercortisolism after CS treatment has been reported to exacerbate immune dysfunctions such as Graves’ disease,2–4 Hashimoto’s thyroiditis,3–5 sarcoidosis,2–6 and psoriasis,2–4 the effects on immune thrombocytopenia (ITP) remain undocumented. Furthermore, previous reports have shown that immune dysfunction typically manifests within weeks to months after CS remission without hindering surgical management.2–6
The objective of this study is to describe a case of ACC with hypercortisolism, in which ITP relapse occurred during both preoperative metyrapone administration and post-surgical reduction. This report provides insight into the interaction between cortisol fluctuations and immune dysfunction in patients with ACC.
Case
A 67-year-old woman with no significant family medical history was admitted to our institution. She had a past medical history of ITP, which had been diagnosed 5 years earlier and was initially treated with 40 mg of prednisolone. Prednisolone was gradually tapered and discontinued 3 years before admission, after which eltrombopag was initiated. The initial eltrombopag dose of 37.5 mg was reduced to 25 mg 8 months before admission following stabilization of platelet counts (98,000–219,000/μL; reference range, 158,000–348,000/μL; Figure 1). Four months before admission, the patient developed gait disturbance and facial and leg edema. Two months prior, hypokalemia was noted (serum potassium (K), 2.7 mmol/L; reference range, 3.6–4.8 mmol/L). One to two weeks before admission, blood pressure increased, necessitating the initiation of antihypertensive medication. Abdominal ultrasonography revealed a right adrenal mass, prompting referral for further evaluation. On physical examination, blood pressure was 116/84 mmHg while receiving amlodipine (10 mg), imidapril (7.5 mg), furosemide (20 mg), and spironolactone (25 mg). Physical examinations showed Cushingoid features, including moon facies, buffalo hump, central obesity, thin skin, and prominent weight gain. Laboratory testing confirmed persistent hypokalemia (K, 2.6 mmol/L) and diabetes mellitus (fasting blood glucose, 126 mg/dL; reference range, 73–109 mg/dL; HbA1c, 7.1%; reference range, 4.9%–6.0%). The endocrine evaluation revealed markedly elevated urinary-free cortisol (401 µg/day; reference range, 5.5–66.7 μg/day), morning plasma cortisol (25.7 μg/dL; reference range, 6.2–18.0 μg/dL), and suppressed adrenocorticotropic hormone (ACTH <2.0 pg/mL; reference range, 7.2–63.3 pg/mL). Serum dehydroepiandrosterone sulfate and testosterone were also elevated at 671 μg/dL (reference range, 12–133 μg/dL) and 1.44 ng/mL (reference range, 0.11–0.47 ng/mL), respectively. Late-night cortisol remained high (23.7 μg/dL), and cortisol levels after the overnight 1 mg dexamethasone suppression test failed to suppress, remaining at 27.0 μg/dL. Abdominal computed tomography revealed a right adrenal mass measuring 51 × 41 mm with an attenuation value of approximately 35 Hounsfield units (Figure 2(a)). These findings raised suspicion for ACC with concurrent CS, and adrenalectomy was planned.
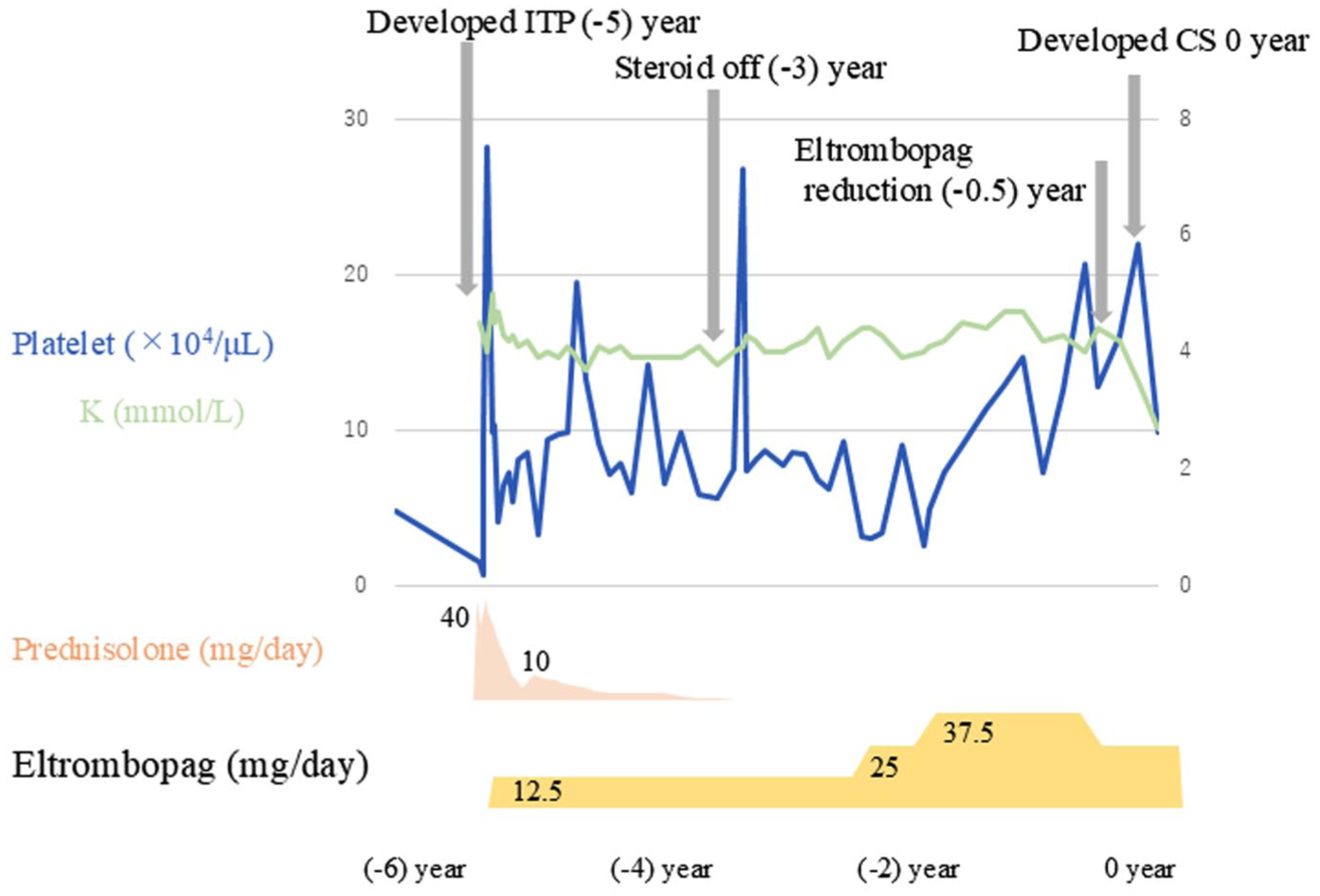
The clinical course of ITP before ACC diagnosis. The patient was diagnosed with ITP and treated with prednisolone and eltrombopag for 5 years. Platelet counts remained stable on eltrombopag monotherapy until the onset of ACC.
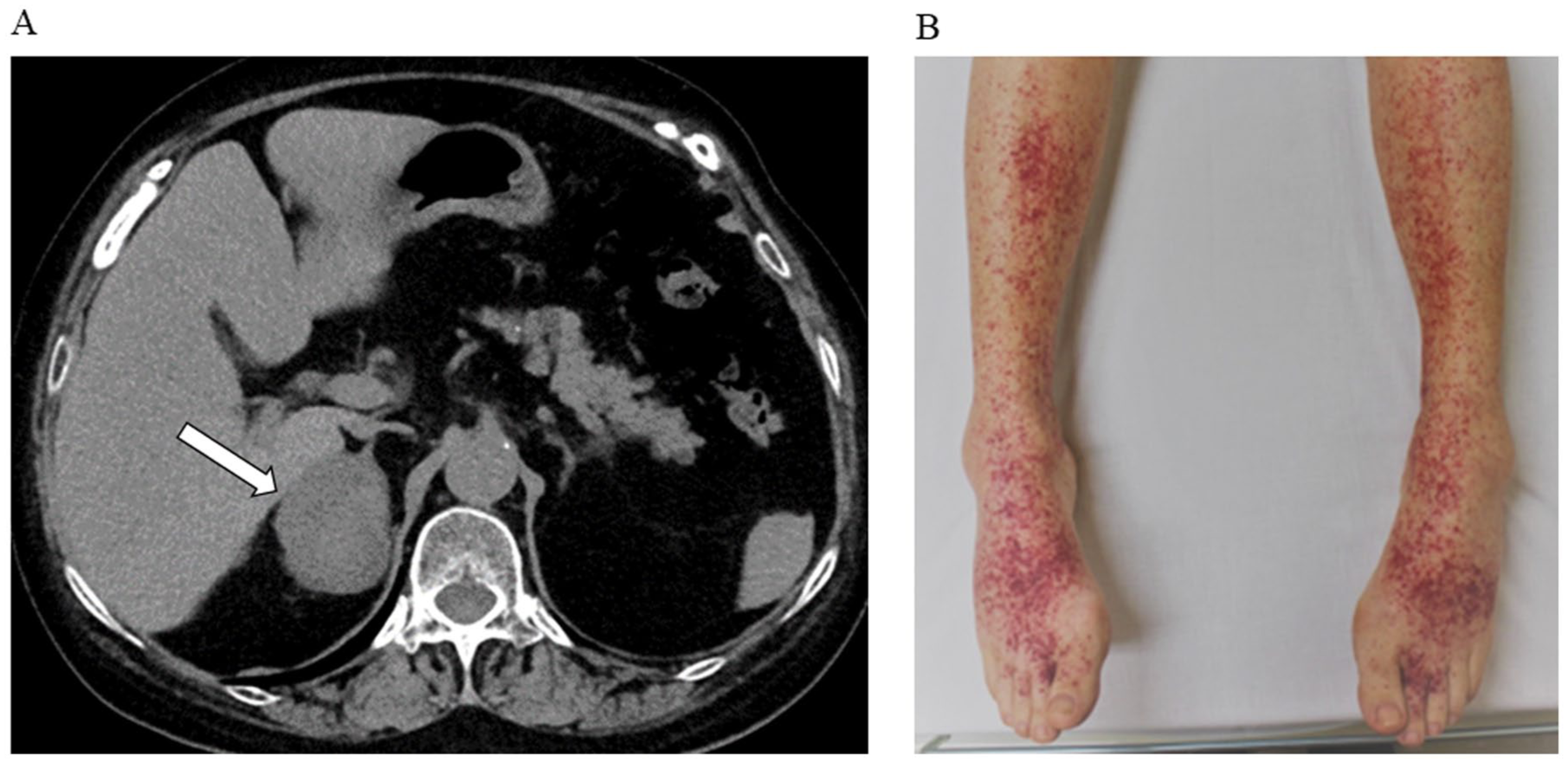
Imaging of the right adrenal mass and development of purpura. (a) Abdominal computed tomography reveals a 51 × 41 mm right adrenal mass (white arrow). (b) Purpura on both lower extremities following initiation of metyrapone treatment.
Proton pump inhibitors and trimethoprim–sulfamethoxazole were initiated upon admission. Metyrapone treatment was initiated on day 3 to manage hypercortisolism. By day 6, after the metyrapone dose was titrated to 1000 mg, urinary-free cortisol levels markedly decreased from 401 to 120 µg/day (Figure 3). However, purpura appeared on the lower extremities (Figure 2(b)), and the platelet count decreased to 21,000/μL (Figure 3), suggesting a potential relationship between rapid cortisol reduction and ITP relapse. Subsequent investigations ruled out drug-induced thrombocytopenia, thrombotic thrombocytopenic purpura, hepatitis B virus infection, and hemophagocytic syndrome. The scheduled adrenalectomy was deferred, and thrombocytopenia was treated with a platelet transfusion on day 7. High-dose dexamethasone was administered from days 7 to 10, followed by intravenous immunoglobulin from days 14 to 18. Once the platelet count exceeded 200,000/μL, right adrenalectomy was performed on day 35 (Figure 3). Perioperative steroid replacement with 150 mg of hydrocortisone was administered and gradually tapered to 50 mg on day 37 and to 30 mg on day 39 (Figure 3). Following this tapering, the platelet count progressively declined and showed a marked decrease to 41,000/μL on day 41 (Figure 3), indicating that ITP exacerbation was attributed to a decrease in endogenous cortisol following tumor resection together with a rapid postoperative taper of steroids. Eltrombopag was resumed on day 41, and prednisolone was initiated at 30 mg on day 42 with discontinuation of hydrocortisone, resulting in a progressive rise in platelet count. The patient was discharged on day 65 with a platelet count of 132,000/μL and prednisolone reduced to 20 mg. Histopathological examination revealed five Weiss criteria—mitotic activity, atypical mitoses, necrosis, venous invasion, and capsular invasion—confirming a diagnosis of ACC. The Stage, Grade, Resection status, Age, and Symptoms (S-GRAS) score was 6 (European Network for the Study of Adrenal Tumors stage II, Ki-67 index of 35%, R1 resection, older age, and symptomatic presentation), and mitotane treatment was initiated and increased to 3 g/day. 7 Despite treatment, hypercortisolism recurred within 1 month (cortisol 28.0 µg/dL; ACTH <2.0 pg/mL), suggesting ACC recurrence. Imaging confirmed tumor relapse, and the patient was transferred for palliative care due to clinical deterioration. She died 6 months after the initial admission.

Clinical course following the diagnosis of adrenocortical carcinoma. After initiation of preoperative metyrapone, purpura developed on both lower extremities by day 6. The patient was treated for an immune thrombocytopenia exacerbation, and a right adrenalectomy was performed on day 35. Postoperatively, metyrapone was discontinued, though further treatment was required for recurrent thrombocytopenia.
Discussion
We report a case of recurrent thrombocytopenia in a patient with a history of ITP and overt CS due to ACC, following metyrapone treatment and surgical intervention, both of which resulted in decreased endogenous cortisol levels. ACC is a rare malignancy with a poor prognosis; adrenalectomy remains the mainstay of treatment. 1 Postoperative adjuvant therapy with mitotane is recommended, particularly in patients with a high risk of recurrence. 8 In cases of ACC with concurrent CS, pharmacological therapies such as metyrapone may be used to control hypercortisolism. 1 ITP is an autoimmune disorder characterized by decreased blood platelet counts, with treatment options including corticosteroids, rituximab, thrombopoietin receptor agonists (TPO-RAs), splenectomy, and others. 9
In this case, ITP was diagnosed 5 years before admission and initially treated with corticosteroids and TPO-RA. Steroid therapy was discontinued 3 years before admission, and platelet counts remained stable with TPO-RA monotherapy. Although the precise duration of hypercortisolism before admission was unclear, clinical symptoms such as weight gain, edema, and elevated blood pressure suggested a duration of at least 3 months. The suppression of endogenous cortisol following metyrapone administration was temporally associated with a thrombocytopenia relapse. Given that suppression of hypercortisolemia in CS is known to unmask or exacerbate autoimmune disorders,2–6,10–12 we diagnosed the observed thrombocytopenia as an ITP relapse. To our knowledge, there are no prior reports of autoimmune hematologic disease exacerbations following CS treatment. In most reported cases, exacerbation of autoimmune disease after CS remission occurs several weeks to months postoperatively.2–6,10–12 However, in this case, ITP relapse occurred during the preoperative phase, necessitating postponement of surgery. This observation suggests that elevated circulating cortisol, whether endogenous or exogenous, may be essential for maintaining platelet counts in patients with ITP. Other differential diagnoses, including drug-induced or malignancy-associated thrombocytopenia, were considered. Metyrapone-induced thrombocytopenia was deemed unlikely, as thrombocytopenia also occurred postoperatively in the absence of metyrapone. Thrombocytopenia in malignancy is typically associated with disseminated intravascular coagulation or the adverse effects of chemoradiotherapy, 13 neither of which was applied in this case. In addition, a study comparing hematological parameters between adrenal adenomas and ACC in patients with CS revealed no significant differences in platelet counts, 14 suggesting thrombocytopenia is not commonly associated with ACC. Although a rare case of CS with ITP due to adrenal adenoma has been reported, 15 and platelet counts in that case improved after adrenalectomy, the platelet count also increased after platelet transfusion both before and after surgery, suggesting that the course may have reflected spontaneous remission of coexisting ITP rather than a causative link with the adrenal tumor. 15
Treatment of hypercortisolism in CS requires consideration of conditions such as immune reconstitution inflammatory syndrome (IRIS). IRIS is classically observed in patients with human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome or other immunocompromised systems at the initiation of antiretroviral therapy. As the immune system recovers, an exaggerated inflammatory response may be mounted against previously subclinical or controlled opportunistic infections. A similar phenomenon, termed non-HIV-IRIS, 16 has recently been reported in other contexts, such as during the treatment of CS. Rapid correction of hypercortisolism in CS can lead to immune reconstitution, which results in clinical deterioration due to manifestation of underlying opportunistic infections such as pneumocystis pneumonia. 17 Although the underlying mechanisms differ, this case involved autoimmune activation due to relative steroid deficiency, resulting from abrupt suppression of endogenous cortisol. Therefore, careful monitoring is necessary during CS treatment.
Treatment of hypercortisolism in CS can lead to unexpected complications. In patients with ITP previously responsive to steroid therapy, suppression of endogenous cortisol may precipitate relapse, potentially affecting the treatment strategy. Therefore, careful monitoring is essential during therapeutic interventions to suppress cortisol levels.
Footnotes
Acknowledgements
The authors express their gratitude to the Department of Molecular Endocrinology and Metabolism, Institute of Science, Tokyo, for their valuable support.