
Abstract
Hyperparathyroidism (HPTH) is the third most common endocrine disorder. Hypovitaminosis D affects up to 40% of the general population and about a third of hyperparathyroid patients. Such a combination may alter the classic presentation of HPTH. This report presents a premenopausal female with long history of osteoporosis, normocalcemia, and hypovitaminosis D who was initially diagnosed as secondary HPTH. After restoring vitamin D to normal using parenteral loading doses, the patient developed persistent mild to moderate hypercalcemia with persistent parathormone elevation consistent with primary HPTH associated with hypercalciuria and complicated with nephrocalcinosis. Imaging confirmed a left upper parathyroid adenoma and fulfilling several indications for surgery, the patient was operated restoring normocalcemia that was maintained for several years of follow-up. Hypovitaminosis D is common and may mask expected hypercalcemia in patients with primary HPTH, thus delaying diagnosis and proper intervention. Reevaluating patients initially diagnosed as hypovitaminosis D and secondary HPTH may reveal a masked diagnosis of primary hyperparathyroidism.
Background
Hypovitaminosis D or vitamin D deficiency is defined as serum vitamin D levels below 20 ng/mL, while levels below 10 or 12 ng/mL are considered severe deficiency. Prevalence of vitamin D deficiency is around 40% while severe deficiency is 13% in Europe. Severe vitamin D deficiency is associated with the risk of osteomalacia presenting as diffuse bone pain and tenderness. Biochemically, it is characterized by low or low normal serum calcium, phosphorus, and secondary hyperparathyroidism. 1
Primary hyperparathyroidism (HPTH) is common occurring in up to 82 cases per 100,000 people. It is characterized by normocalcemia or variable degrees of hypercalcemia associated with high or inappropriately normal parathormone (PTH). More than 80% are asymptomatic, however, up to 63% have osteopenia/osteoporosis and up to 20% have nephrolithiasis/nephrocalcinosis. 2
Familial hypocalciuric hypercalcemia (FHH) is a rare autosomal dominant benign cause of hypercalcemia. It is characterized by mild early-onset hypercalcemia, unsuppressed, or, in a quarter of patients, high PTH. It is differentiated from primary HPTH by a characteristic low urinary calcium excretion. 3
In this report, when hypovitaminosis D – an essentially hypocalcemic state – and primary HPTH – an essentially hypercalcemic state – are combined in the same patient, this will modify the initial presentation and cause a rethinking of the differential diagnosis in the course of managing this patient.
Case presentation
A 45-year-old premenopausal female presented with an impacted fracture of the base of the right fifth metacarpal bone in August 2012 [Figure 1(a)]. She has been complaining of generalized bony aches for more than 7 years. Her medical history was only remarkable for a diagnosis of low bone mineral density (BMD) for age based on Dual-energy X-ray absorptiometry (DXA) scan performed in 2005 with a Z-score of −2 in the femoral neck. No documented etiology for the low BMD was reported. She received treatment in the form of weekly alendronate for the past 7 years. DXA scan showed a mild improvement on follow-up in 2009 and 2012 to a Z-score of −1.7 and −1.6, respectively.
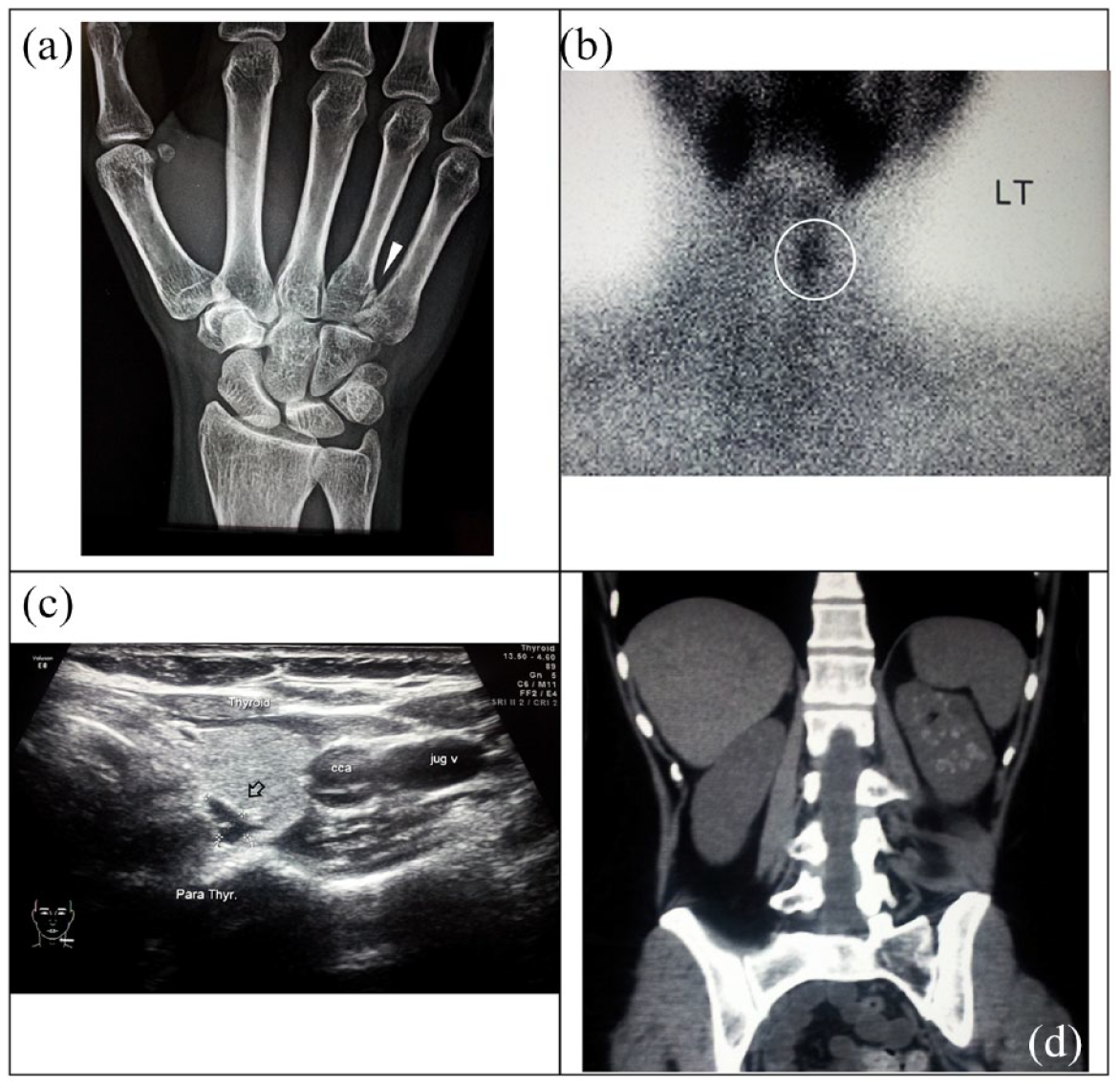
Imaging workup of the patient. (a) Plain X-ray showing an impacted fracture base of right fifth metacarpal bone. (b) Technetium-99 m (SESTAMIBI) scan showing abnormal increased radioactivity at the anatomical site of left upper parathyroid gland consistent with parathyroid adenoma. (c) Neck ultrasound showing an enlarged 10 mm × 6 mm × 3 mm left upper parathyroid gland consistent with parathyroid adenoma. (d) Non-contrast computed tomography of the abdomen showing left kidney multiple small calyceal stones and medullary nephrocalcinosis.
Causes of low BMD were explored in October 2012. She was euthyroid, TSH 0.98 µIU/L (N: 0.27–4.2), free T4 1.43 ng/dL (N: 0.9–1.9). Low normal serum calcium 8.7 mg/dL (N: 8.6–10.2) and low phosphorus 2.3 mg/dL (N: 2.5–5). Low vitamin D level at 6.4 ng/mL (N: 30–100) and high serum parathyroid hormone PTH at 208 ng/L (N: 10–65 ng/L). At this point, the first differential diagnosis was normo-calcemic HPTH, however before making this diagnosis, causes of secondary HPTH have to be excluded with vitamin D deficiency on top of the list. 4 The second differential diagnosis was hypovitaminosis D causing secondary HPTH, the patient had vitamin D deficiency according to the endocrine society guidelines, and the long-standing complaint of bony aches was consistent with osteomalacia.
The patient was prescribed vitamin D3 200,000 IU ampoules by intramuscular injections, every 2 weeks for 2 months and the tests were reevaluated in December 2012. Vitamin D showed some improvement and rose to 18 ng/mL and calcium rose up to 11.8 mg/dL. The patient repeated the same treatment protocol for two more months and tests were reevaluated once more in March 2013. Vitamin D normalized to 51.4 ng/mL, calcium remained elevated at 11.5 mg/dL, phosphorus low normal at 2.5 mg/dL, and PTH remained high at 161 ng/L. The decision was to stop vitamin D injections and reevaluate in 1 month.
In April 2013, calcium showed persistent elevation at 12.7 mg/dL, low normal phosphorus at 3.2 mg/dL, and PTH persistently elevated at 231 ng/L. At this point, the differential diagnosis was primary HPTH versus FHH. A final laboratory assessment was ordered in May 2013 to reach a definite diagnosis. Normal vitamin D at 65.3 ng/mL, high ionized calcium at 6.4 mg/dL (N: 4.6–5.2), low phosphorus at 2.1 mg/dL, high 24 h urinary calcium excretion at 577 mg/24 h (N: 100–400), and high PTH at 176 ng/L, a combination consistent with primary HPTH that was initially masked by hypovitaminosis D.
A Technetium-99 m (SESTAMIBI) scan revealed a left upper parathyroid adenoma, that was also confirmed in an ultrasound examination of the neck measuring 10 mm × 6 mm × 3 mm [Figure 1(b) and (c)]. Creatinine was normal at 0.61 mg/dL (N: 0.5–0.9), but an abdominal CT scan revealed left kidney medullary nephrocalcinosis and nephrolithiasis as multiple calyceal stone averaging 6 mm in maximum dimension [Figure 1(d)]. Based on the following clinical, laboratory, and imaging data: <50 years of age, serum calcium more than 1 mg/dL above normal range, low BMD, nephrocalcinosis and nephrolithiasis, and urinary calcium excretion >400 mg/24 h, the decision was surgery. 5 The patient was operated on in June 2013. Immediately postoperative PTH went down to 14.7 ng/L and ionized calcium to 3.98 mg/dL. Within weeks, serum ionized calcium, phosphorus, and PTH normalized and remained within normal for the past 8 years.
Discussion and conclusions
The present case is an example of hypovitaminosis D initially masking classic hypercalcemia of primary HPTH, thus delaying the diagnosis and proper surgical intervention. One-third of patients with primary HPTH have serum vitamin D below 20 ng/mL at the time of presentation. 6 The initial presentation of the present case with normocalcemia, hypophosphatemia, high PTH, and marked hypovitaminosis D, may be interpreted by either primary HPTH with hypovitaminosis D or hypovitaminosis D with secondary HPTH. Correction of vitamin D deficiency was a must to differentiate between the two diagnoses. 7 Correcting hypovitaminosis D in patients with primary HPTH is safe, reduces PTH, and improves BMD before surgery. 8
After correcting vitamin D status, a frank presentation of hypercalcemia, low (normal) phosphorus, and high PTH consistent with either primary HPTH or FHH. Urinary calcium excretion below 100 mg/24 h is consistent with FHH while urinary calcium excretion of more than 200 mg/24 h is consistent with primary HPTH. Taking into consideration that overlap between the two conditions exists for values between 100 and 200 mg/24 h, only 40% of patients with primary HPTH will present with hypercalciuria while only 75% of patients with FHH will have urinary calcium excretion below 100 mg/24 h.6,7 A markedly elevated urinary calcium excretion in this patient confirmed the diagnosis of primary HPTH.
Three similar cases were previously reported.9–11 Two females and one male, middle aged between 21 and 43 years. They showed multiple similarities to the present reported case. They presented as recurrent, fragility, or insufficiency fractures. They all had severe vitamin D deficiency with levels <10 ng/mL. They all had normocalcemia at presentation that evolved into hypercalcemia after correcting hypovitaminosis D in two of the cases.9,11 Two cases were either osteopenic or osteoporotic as determined by DXA. One major difference is a markedly elevated PTH at presentation ranging from 1560 to 1704 ng/L, whereas the current case showed PTH levels ranging between 161 and 231 ng/L.
In conclusion, hypovitaminosis D is common, coexists in one-third of patients with primary HPTH, and may mask expected hypercalcemia in such patients, thus delaying diagnosis and proper intervention. Reevaluating patients initially diagnosed as hypovitaminosis D and secondary HPTH may reveal a masked diagnosis of primary HPTH.