
Abstract
Transgender and nonbinary individuals are historically underserved by healthcare systems. A crucial area for improvement is fertility preservation counseling and service delivery, as gender-affirming hormone therapy and gender-affirming surgery may negatively affect future fertility. The methods available for fertility preservation depend on the patient’s pubertal status and utilization of gender-affirming therapies, and counseling and delivery of these services are complex and require a multidisciplinary approach. Further research is needed to identify pertinent stakeholders in managing the care of these patients, as well as to better understand the optimal frameworks for delivering integrated and comprehensive care to this patient population. Fertility preservation is an active and exciting area of scientific discovery and offers a wealth of opportunities to improve the care of transgender and nonbinary individuals.
Introduction
Transgender and nonbinary individuals comprise a small but underserved population in reproductive medicine. It is estimated that 150,000 youths and 1.4 million adults in the United States identify as transgender, and an additional of 1.2 million identify as nonbinary.1,2 This population suffers a myriad of adverse mental and physical health outcomes, with nearly one-quarter of individuals avoiding engaging with the healthcare system due to concern for discrimination.3–5 Of particular concern in this population is the poor utilization of preventive health services and other future-oriented services, including fertility preservation.
Fertility preservation care has historically centered around oncofertility, and only in recent years has fertility preservation for transgender and nonbinary individuals come to the forefront. 6 This is a critical aspect of quality medical care for these patients, as many gender-affirming treatments sought by this group may negatively impact future fertility. 7 Additionally, these individuals desire biological parenting at rates similar to the general population, with estimates ranging from 18–54%.8–10 The aim of this narrative review is to summarize the existing literature regarding fertility preservation technologies for adolescents and adults, as well as to review barriers to the administration of well coordinated and timely care for transgender and gender-diverse patients (Table 1).
Terminology and definitions.

Fertility preservation options
Fertility preservation options depend primarily on the patient’s reproductive organs, whether they have experienced puberty, and whether they have utilized gonadotoxic gender-affirming therapy. Options are limited for some patient groups. Fortunately, this remains an active area of research, and currently, experimental fertility preservation methodologies may soon join the repertoire of options available for patients. Please see Table 2 for details regarding fertility preservation options for individuals based on these factors.
Fertility preservation options by pubertal status.
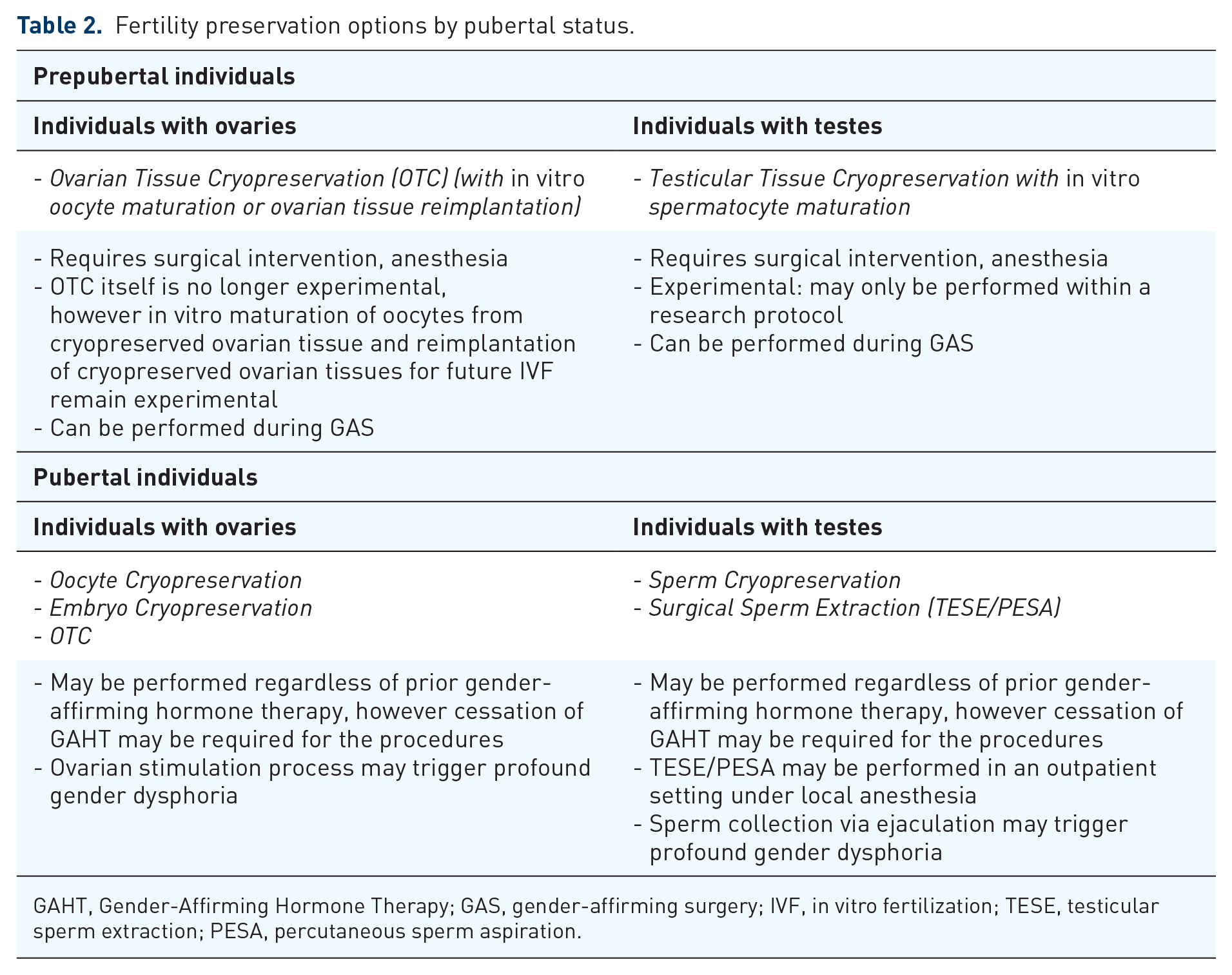
GAHT, Gender-Affirming Hormone Therapy; GAS, gender-affirming surgery; IVF, in vitro fertilization; TESE, testicular sperm extraction; PESA, percutaneous sperm aspiration.
Individuals with ovaries
Patients with ovaries have several options for fertility preservation, each of which comes with a unique set of risks and benefits. Pubertal patients with ovaries (at or beyond Tanner Stage II breast development) may consider oocyte or embryo cryopreservation. These options involve controlled ovarian hyperstimulation and a surgical procedure to retrieve oocytes. 7 This requires frequent contact with the healthcare system over a relatively short period, which can contribute to anxiety among individuals who may already be distrustful of the medical system.
Patients often need multiple transvaginal ultrasounds to assess follicular growth, and oocytes are most commonly retrieved through a transvaginal approach, both of which may trigger dysphoria. Reproductive endocrinology and infertility (REI) specialists should also consider utilizing transabdominal over transvaginal ultrasound approaches when gonad positioning and body habitus allow.4,11 Furthermore, the increased estrogen levels experienced during this process, as well as the potential for menses to resume at its conclusion, may cause significant dysphoria. Individuals may choose to preserve oocytes through this technique or elect to preserve embryos with sperm from a partner or known or unknown sperm donor.
Exogenous testosterone exposure may simultaneously increase the ovarian follicle pool (similar to what is seen with polycystic ovary syndrome patients) and blunt the response to gonadotropins, requiring prolonged and more expensive stimulation cycles. 12 Notably, AMH levels, which may predict response to controlled ovarian stimulation, tend to decrease after exogenous testosterone exposure, consistent with the above reported trends. 13 However, the clinical significance of these changes remains under scrutiny as they are often minor. 14 One retrospective cohort study found no difference in baseline follicle count or cycle length between transgender men with and without a history of Gender-Affirming Hormone Therapy (GAHT) use; however, those with a history of GAHT use had lower peak estradiol levels and lower oocytes retrieved. 9 Still, this study reported three successful pregnancies conceived using oocytes from transgender men who had used GAHT. 15 However another study found no difference in peak estradiol levels or the number of oocytes retrieved between transgender men with a history of GAHT use, transgender men without a history of GAHT use, and cisgender females. Five of the six transgender men with a history of GAHT use achieved good-quality embryos suitable for in vitro fertilization (IVF). 16 Recent research corroborates that there does not appear to be any negative impact of exogenous testosterone exposure on preimplantation embryo quality, development, or fertilization rates. 17
Today, most fertility centers require patients to discontinue testosterone therapy for 1–3 months prior to an ovarian stimulation cycle. Gender dysphoria triggered by discontinuation of GAHT may be life-threatening, so this is a prohibitive barrier to care for many patients. There is currently one published case report of a pregnancy resulting in live birth following oocyte retrieval from a transgender man who was maintained on testosterone therapy throughout a controlled ovarian stimulation cycle. That patient had a 10-year history of testosterone use. The ovarian stimulation cycle was longer than average and the embryo aneuploidy rate was more than twice the expected rate for the patient’s age cohort. 12 Still, this case shows promise for future fertility preservation that minimizes at least one aspect of gender dysphoria. Other considerations to minimize the dysphoria associated with ovarian stimulation may include the addition of aromatase inhibitors such as letrozole to reduce estradiol elevations during stimulation cycles and random-start protocols that do not require patients to have a menses prior to beginning a stimulation cycle.
Ovarian tissue cryopreservation (OTC) is an alternative option for prepubertal individuals as well as individuals with contraindications to ovarian stimulation, such as those who cannot delay or pause gonadotoxic treatment for an ovarian stimulation cycle. This technique requires an invasive procedure that comes with surgical and anesthetic risks. Until 2020, this procedure was considered experimental by the American Society of Reproductive Medicine (ASRM). While the removal of ovarian tissue is no longer experimental, the techniques to attempt future pregnancy after this do remain experimental. One technique, future autotransplantation of cryopreserved ovarian tissue, is being investigated with caution among select oncology patients. This may be a useful tool for some transgender and gender-diverse individuals, however it is critical to appreciate that reintroduction of this tissue may trigger gender dysphoria, which is often a reason for tissue removal in the first place. Alternative to this is in vitro maturation of oocytes harvested from cryopreserved ovarian tissue. To date, no successful pregnancies utilizing in vitro maturation of oocytes from cryopreserved ovarian tissue have been reported. 18 However, live births have been reported using this technique for cancer patients. The effect of testosterone exposure on in vitro maturation of cryopreserved oocytes is poorly understood, however there is evidence that the developmental capacity of such oocytes may be diminished. 19 Now that OTC is no longer experimental for transgender and gender-diverse patients, we may see this being offered to more patients, and with more data, we can improve its efficacy and outcomes.
Individuals may elect for removal of the ovaries (oophorectomy) as a gender-affirming surgery (GAS) regardless of desires for fertility preservation. Other GAS procedures for individuals with ovaries may include removal of the uterus (hysterectomy), fallopian tubes (salpingectomy), and/or breast tissue (mastectomy). Evaluation of removed ovarian tissue has identified histologic changes associated with exogenous testosterone exposure, including increased ovarian cortical stiffness, stromal luteinization, and an increased prevalence of primordial and atretic follicles.20–22 The clinical significance of these changes is under investigation. No increased rates of dysplastic or malignant changes have been observed in these samples. 23
Individuals with testes
Fertility preservation options for individuals with testes are, in general, less invasive and less time- and resource-intensive. The most widely available options include sperm cryopreservation and testicular sperm extraction (TESE), which may be used to cryopreserve gametes or embryos. Cryopreserved gametes may later be used for intrauterine insemination or IVF, and cryopreserved embryos may later be used for IVF. Sperm cryopreservation requires the patient to provide a semen sample – a noninvasive process that may trigger significant dysphoria. TESE may be done in an outpatient setting under local anesthesia. These options are available to patients who have reached Tanner Stage II or more and who have a testicular volume of at least 5 mL. 18
While current data on the effect of testosterone on oocyte maturation is conflicting, most evidence to date shows an association between gender-affirming estrogen use and sperm quality. In one study of semen specimens collected via ejaculation, specimens collected from patients on GAHT were associated with abnormal semen parameters. This effect did not appear to be permanent, as semen parameters were comparable among patients who had never used GAHT and those who had discontinued GAHT, with an average discontinuation interval of 4.4 months. 24 Several studies support these findings of the detrimental effect of GAHT on spermatogenesis and sperm quality. 25 However, other studies show continued semen parameter abnormalities even after discontinuation of GAHT, 26 and yet others show semen parameter abnormalities among transgender individuals even prior to initiating GAHT.27,28 Data regarding histologic changes after GAHT have been noted as well. 29 Because of the inconclusive data, many providers recommend fertility preservation prior to initiating GAHT with estrogen in patients with testes.24,30 Additionally, strong consideration for the use of intracytoplasmic sperm injection to increase fertilization rates in this population, regardless of prior hormonal exposure, is recommended. 28 The youngest reported age of successful specimen collection for sperm cryopreservation is 11 years.
Currently, there are no fully approved options for fertility preservation for prepubertal patients with testes. Testicular tissue cryopreservation remains experimental, and can only be offered within a research protocol, so the use of this technology remains limited. 31
Considerations for adolescents
Many individuals have a strong sense of self in childhood and adolescence, and the ability to initiate gender-affirming care at an early age is important. Patients must be informed about the potential impacts of gender-affirming care on future fertility to allow them the opportunity to make decisions about fertility preservation and other aspects of their care. Fertility preservation can be a high-risk undertaking without a guarantee of desired results, and there are often multiple medically reasonable options for individuals to consider. 32 It is challenging to make future-oriented medical decisions, particularly when patients have not yet considered whether they want children in the future, whether having biological children is important to them, and when they do not know what their future financial solvency will be. Children and adolescents face additional challenges with this, as their prefrontal cortex is not yet fully developed to take on this type of complex, forward-thinking decision-making. Furthermore, providers and guardians may feel uncomfortable broaching this subject with patients. Still, this is a key population to consider, as children and adolescents are less likely to have already initiated gonadotoxic treatments and, therefore, may be more likely to succeed with fertility preservation if this is pursued. 31 Lessons can be learned from Israel, where one study showed that 100% of child and adolescent patients were offered a fertility preservation consultation during their first visit to a gender-affirming clinic. 33 It is important to remember that gender-affirming therapy aims to achieve gender euphoria rather than only to minimize gender dysphoria. Not all patients, especially children and adolescents who have not yet reached puberty will experience functional limitations because of their gender identity discordance. Yet, these individuals may still stand to improve with gender-affirming therapy. Pediatric and adolescent gynecology specialists are uniquely positioned as experts in sexual and reproductive health and development to help guide these conversations. Counseling may focus on internal and external motivations for treatment, as more externally motivated patients may be less likely to see the positive changes in their sense of identity and interpersonal reactions following the treatment. 34 Some individuals may elect to initiate gonadotropin-releasing hormone therapy prior to Tanner Stage II–III, as this can provide additional time for patients to make care decisions without simultaneously dealing with the potentially dysphoric effects of experiencing puberty in a gender-discordant body. 33
Barriers to care
Though parenting desires remain high among transgender and gender-diverse individuals, utilization of fertility preservation services remains low.8,35,36 Transgender and gender-diverse individuals face many barriers to fertility preservation care, but the two main ones are lack of awareness of this service and lack of access to it. These barriers are multifactorial. ASRM, the World Professional Association for Transgender Health Standards of Care, and the Endocrine Society Clinical Practice Guidelines recommend that all mental health professionals, hormone-prescribing physicians, and surgeons being involved in gender-affirming surgeries discuss fertility preservation options prior to initiating any medical intervention for gender-affirming therapy. 7 Yet this standard of care is far from being met,4,37 with fewer than half of transgender and gender-diverse individuals receiving fertility preservation counseling. 38 When asked, 95% of transgender respondents stated that fertility preservation should be offered to all transgender and nonbinary people. 39 In one study in Israel, 86% of transgender women and 36% of transgender men pursued fertility preservation after such counseling. 40 Recent data from Australia, Germany, and the United States suggest that 10% or fewer transgender individuals pursue fertility preservation.39,41,42 Fertility preservation options for transgender individuals are not equally available in all countries and regions. Please see Table 3 for additional details regarding fertility preservation legislation and policies in selected countries around the world.
Fertility preservation options around the globe.

GAHT, Gender-affirming hormone therapy; GAS, gender-affirming surgery; IVF, in vitro fertilization; NHS, National Health Service.
While comprehensive counseling is certainly a critical step in allowing patients to make appropriate and fulfilling healthcare decisions for themselves, other barriers limit the uptake of this service. All insurance companies are required to offer coverage for necessary medical care. Though gender-affirming care is essential and cost-effective, insurers may consider gender-affirming therapies to be experimental in some cases and, therefore, outside of coverage obligations. Providers may use the ‘equivalent care’ clause, which states that services covered for one medically necessary reason (such as fertility preservation prior to chemotherapy) should be covered for other medically necessary reasons (such as fertility preservation prior to gender-affirming therapy). This can be challenging, however, as the gonadotoxic effects of hormone therapies are in general less well understood than those of chemotherapy agents. Proving medical necessity to insurers can be an emotionally and psychologically draining process, even more so when the care in question is intimately related to an individual’s identity. 43 Adolescents and young adults covered by their caregivers’ insurance may be forced to disclose their gender identity to their loved ones when managing such insurance hurdles, taking away their agency in an important process. Finally, fertility preservation is rarely covered by insurance and is cost prohibitive for many. 37
Beyond the cost and uncertainty of outcomes, fertility preservation comes with a significant psychological toll in many cases.3,37,42 As discussed previously, patients may experience significant dysphoria with transvaginal ultrasound and transvaginal oocyte retrieval. They may also experience bothersome changes in secondary sex characteristics associated with the elevated estrogen levels experienced with controlled ovarian hyperstimulation. While sperm preservation is generally less invasive and a shorter process than oocyte preservation, patients may still experience significant dysphoria with ejaculation, and many may not be able to do this at all. Patients may fear delaying or discontinuing GAHT, which is often required for, and likely improves the efficacy of fertility preservation. For some, the fear of these possibilities is enough to prohibit the pursuit of fertility preservation, even when biological parenthood is desired.
Finally, as discussed above, many individuals begin the process of gender affirmation early in life, well before they are considering parenthood, well before they are partnered, and well before they have the financial means for either parenthood or fertility preservation. Likely, many of these individuals never receive fertility preservation counseling at all.
Future directions
Just as in many other populations, many transgender and gender-diverse individuals desire to build families and have biological children.4,31,38,41,44 Parenthood is associated with decreased rates of suicide, better mental health outcomes, and greater perceived self-efficacy. 7 Transgender and gender-diverse individuals are at high risk for all of these and more adverse health outcomes. Improving awareness of and access to safe, feasible, and desirable fertility preservation opportunities may contribute to better mental health in this population.
Further research is needed to determine the optimal format for optimizing fertility preservation counseling. Integration of services, including counseling, initiation, maintenance of GAHT, and GAS, may increase access to care by establishing clearly designated safe spaces for patients and providing a single location for all the needed services. 31 Whether this is best done by stand-alone transgender and gender-diverse care clinics or through coordination between relevant units within hospital systems remains in question. Providers involved in treating transgender and gender-diverse patients may also benefit from viewing and connecting patients to comprehensive fertility preservation counseling as being within their scope of practice and critical to providing optimal care for their patients. Table 4 details the role of various medical specialists in providing comprehensive fertility preservation and gender-affirming care for transgender and gender-diverse patients. Notably, the role of regret in fertility preservation care for these patients has not yet been well studied and is worthy of close examination.
Stakeholders in fertility preservation.

GAHT, Gender-affirming hormone therapy; OTC, Ovarian tissue cryopreservation; TESE, testicular sperm extraction.
Regarding treatment options, more research is needed to determine how to safely perform controlled ovarian stimulation and oocyte cryopreservation without requiring patients to discontinue testosterone. Conversely, research is needed to determine whether the gonadotoxic effects of estrogen exposure may be reversed in vitro after sperm extraction or if there are options to combat the effects of estrogen locally within the testes to allow for the extraction of high-quality sperm for preservation. Ovarian and testicular tissue cryopreservation remain active and promising areas of future research, as these techniques may be available to children and adolescents who currently have very limited options for fertility preservation. 32 In vitro maturation of gametes from cryopreserved gonadal tissue may soon become available, with recent studies showing successful techniques for both oocytes45,46 and spermatogonia. 47 Admittedly, the strongest data in this realm come from animal studies, and human data remain limited.48–50 The development of these techniques is particularly critical for fertility preservation in transgender and nonbinary patients, for whom reimplantation of cryopreserved gonadal tissue may not be acceptable.
While the number of transgender and gender-diverse patients is unlikely to be increasing, the healthcare needs of this population are receiving increased and much-needed attention, as these individuals suffer a wide array of health disparities. 6 Fertility preservation should be considered a critical aspect of high-quality, comprehensive gender-affirming care and should be made accessible to all patients.
Supplemental Material
sj-docx-1-tae-10.1177_20420188231178371 – Supplemental material for Fertility preservation options for transgender and nonbinary individuals
Supplemental material, sj-docx-1-tae-10.1177_20420188231178371 for Fertility preservation options for transgender and nonbinary individuals by Jensen Reckhow, Hakan Kula and Samir Babayev in Therapeutic Advances in Endocrinology and Metabolism
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.