
Abstract
The digitization of healthcare and its usage in the delivery of healthcare have experienced exponential growth across the world in recent times. India’s fast-growing diabetes population has been exerting immense pressure on the country’s healthcare infrastructure. Various innovative and evolving technologies are converging to impact the trajectory of digital health in diabetes. The diabetes community has been adopting various technologies such as connected glucose meters, continuous glucose monitoring systems, continuous subcutaneous insulin infusion, closed-loop systems, digitalization of health data, and diabetes-related apps for the prevention and management of the condition. India has provided some excellent examples in exploiting the potential of digital transformation in revamping the diabetes ecosystem. Yet, there are still various hurdles in technology development, healthcare delivery, as well as concerns related to data privacy, digital divide, policies by the government, role of stakeholders, attitude, and absorption by healthcare professionals, and hospitals. This article provides an overview of the digital diabetes technologies currently practiced in India and recommends the need for strong technology adaptation and policy interventions for an ideal roadmap of digitalization of diabetes care in the Indian milieu.
Introduction
The diabetes burden has progressively increased worldwide with India having the second largest numbers in the world, after China. 1 At present, India is home to 77 million people with diabetes (PwD); these numbers are based on the nationwide Indian Council of Medical Research—India Diabetes (ICMR—INDIAB) study. 2 In addition, India has a high prevalence of prediabetes and undiagnosed diabetes.2,3 Despite the advances in diabetes therapies and technologies, a substantial proportion of PwD struggle to achieve better glycemic outcomes.4,5 The complex manifestation of this disorder demands tailored treatment support for those living with diabetes. However, a personalized approach in diabetes management has been impeded by limited healthcare resources and limited individual care inherent to conventional methods. The key obstacles that patients experience in diabetes management include (1) optimizing the use of existing therapies to guarantee adequate glycemic, blood pressure, and lipid control and to decrease complications; (2) educating PwD on diabetes self-management; (3) improving treatment adherence; (4) clearing the impediments to delayed diagnosis and the early initiation of insulin when indicated; and (5) improving the healthcare delivery to people with chronic conditions.6,7
Digital health includes technologies, platforms, and systems that promote for lifestyle, wellness, and treatment of chronic diseases like diabetes; collect, store, or communicate health information; and assist life science and clinical operations. 8 The advent of social media platforms, smartphones, mobile applications, wearable devices, cloud-based data platforms, and real-world evidence studies has revolutionized digital health. The use of these technologies has seen an exponential increase over the years. Digital health can streamline how populations interrelate with national health services and also reinforce existing health systems. The data gathered using these technologies help to improve the quality of healthcare by facilitating better therapeutic decisions and eventually addressing the rising burden of diabetes.9–11
The Government of India has introduced several initiatives such as the National Digital Health Mission under the Digital India program for the adoption of digitalization in healthcare to solve complex health problems. 12 Since India is the second largest mobile phone consumer worldwide, smartphone penetration helps accelerate the effectiveness of e-governance initiatives. Digital inclusion has been anticipated to reform various phases of healthcare delivery, including health promotion, prevention, primary care, and specialized care in India. Considering its very large population, India’s healthcare needs are immense and resources are often constrained. Given the chronic nature of diabetes, however, continuous follow-up is critical to managing glycemic control and preventing future complications. Here, digital technology provides an optimal solution for tracking and management for the patient, the doctor, and the policy-maker. The use of digital technology has been effective in the prevention and treatment of diabetes by allowing consumer engagement, behavior change, and impact analytics. 6
The goal of this article is to review the status of diabetes digital health in India, to provide the main examples where digital technologies have already been used in clinical practice, and viewpoints on the challenges and jeopardies that healthcare professionals and the Government confront while implementing digital tools for diabetes management.
Methods
We have categorized this article as a literature review according to the method used for search. 13 We performed the search on PubMed database using keywords including ‘digital health’, ‘diabetes’, ‘artificial intelligence’, ‘diabetes technology’, and ‘India’ to retrieve studies specific to India.
Real-world evidence on the success metrics of digital technologies
Continuous glucose monitoring
Continuous glucose monitoring systems (CGMs) are a very good example of the absorption of digital technology in healthcare. CGMs allow the measurement of glycemic variability (GV) to monitor glucose trends in PwD. 10 Even the first CGM, CGMS Gold, was available in India, 14 iPro2(Medtronic), the blinded CGM, was the most popular one for close to a decade. 15
India was the first country to receive approval for FreeStyle® Libre Pro Flash Glucose Monitoring System in 2015. 16 In 2020, FreeStyle® Libre, the isCGM (intermittently scanned CGM), was launched in India. Despite the Covid pandemic, it was widely accepted by the physician and patient communities. Obviously, the real-time glucose values, patterns, and Time In Range (TIR) data benefit and inspire patients to keenly manage their diabetes. 17 CGMs demonstrate the accomplishment of digital healthcare by fully making use of its three components: the medical device, the data-mining engine platform, and the data-driven medical feedback. 18
Uses of CGM in clinical practice
CGM is generally used in patients with type 1 diabetes (T1D), but in India, with its huge T2D population, it is diligently used for T2D management also. A retrospective CGM study in 148 patients with T2D found that a 3-month use of iPro2 reduced the mean A1C from 8.6% at baseline to 8.0%. 14 This study provided important perceptions and prospects for introducing changes to treatment regimens and lifestyle interventions and apprised the importance of therapy compliance among the patients. Another 6-month retrospective study in 296 patients with T2D reported a clinically meaningful reduction in A1C (0.5% ± 1.4% to 7.0% ± 0.9%) among CGM users. 19 A multicenter study in a large Indian population of 5072 PwD with T1D and T2D assessed the efficiency of Ambulatory Glucose Profile (AGP) generated by FreeStyle LibrePro™ flash glucose monitoring (FGM) (Abbott) on the glycemic outcomes. The group showed that FGM-AGP resulted in a significant reduction in HbA1c in both patients with T1D and T2D. 20 It has also been reported that AGP generated from the FGM in 106 patients with T2D enabled the clinicians to reduce the GV, and frequent hypoglycemia events, resulting in improved quality of life (QoL). 21 The authors of a cross-sectional study evaluated the superiority of CGM-derived hypoglycemic indices to identify nocturnal and asymptomatic hypoglycemic episodes in 83 PwD of the exocrine pancreas. 22 Another study comprising 5901 patients with T2D used CGM to find the association between AGP indicators and diabetes-related complications. The results indicated that those with both the hypo and hyper profiles, which can only be detected by CGM, had a higher risk of non-proliferative diabetic retinopathy (NPDR), macroalbuminuria, and diabetic kidney disease. 23 The Gan & Lee Insulin Glargine Target Type (1) Evaluating Research (GLITTER) study from Mumbai, India, introduced a novel interim intervention using the professional continuous glucose monitoring system (pro-CGM) with the Freestyle Libre Pro system. The group made an interim assessment on the fifth day of CGM initiation to make diet or pharmacotherapy modifications accordingly. The method had efficiently improved glycemic outcomes in terms of average glucose, time-in-range, time-above-range, time-below range, and hypoglycemia events. 24 Another group explored the efficacy of a Twin Precision Nutrition (TPN) Program powered by CGM, Internet of Things technology (IoT), food intake data, and artificial intelligence (AI) algorithms. The Digital Twin Technology platform gathered data from the participant’s body sensors and transferred it to a mobile application to track the health status to make customized treatment decisions. CGM-based daily precision nutrition guidance enabled those patients who adhered to the program to achieve a significant reduction in the HbA1c, body weight, and time below range. 25 These studies have shown that CGMs help to generate more actionable data to introduce new intervention techniques, break clinical inertia, motivate patients for diabetes self-care, and alleviate the burden on doctors.
Insulin pumps
The raised escalation of number of diabetes cases has been propelling the demand for technologically advanced, AI-powered insulin delivery devices. Unfortunately, most of the sophisticated insulin delivery devices are still not accessible to a large proportion of PwD in India. Only insulin pumps from Medtronic are currently marketed in India although new launches of more advanced systems are expected soon.
Modern era insulin pumps were first introduced in India in 2004 and in contrast to western countries where the majority of pumps users are those with T1D, the majority of insulin pump users in India are patients with T2D.26,27 There are several publications from India demonstrating the usefulness of Continuous Subcutaneous Insulin Infusion (CSII) and these are briefly reviewed below.
Improved sexual function, mitigation of peripheral neuropathic pain, and a significant reduction of HbA1c were noticed in 46 patients with T2D who were changed to CSII from multiple daily injection (MDI). 28 The efficiency of CSII was further reiterated by a statistically significant reduction in HbA1c after CSII initiation in a group of 33 patients with recalcitrant diabetes. 29 Multiple studies reported that patients experienced an improvement in QoL after using the pump.30,31 A 12-month follow-up study in 16 patients with T1D belonging to the unprivileged sections of rural India showed that judicious allocation of CSII therapy among patients would improve glycemic control. The approach was found to reduce emergency hospitalizations resulting in better QoL. 32
Most promising technologies like closed-loop insulin delivery systems are currently not easily accessible to the general population in India due to high cost and stringent regulatory procedures. Recently, the first person with T1D from India on Do-It-Yourself Artificial Pancreas reported her experience, using this system which integrates insulin pumps, CGM, and a third-party algorithm. The system has brought significant improvement in glycemic indices such as time-in-range, time-below-range, and QoL. 33
Electronic health and mobile health in managing diabetes
The term Electronic Health (E-health) is an amalgamation of medicine and the Internet that comprises the use of telemedicine, m-Health, smartphone photography, and electronic medical records (EMR). 34 The current COVID pandemic has prompted the Government of India to promote digitalization of the healthcare sector in various aspects such as e-consultations, health surveillance, health education, and other healthcare services. During the lockdown, the country witnessed a large number of patients with T2D seeking online support through YouTube, Facebook, WhatsApp, and Google search for diabetes management. The platform/media used for obtaining information included videos on disease management, Apps, blogs, voice/video call facilities, short message services (SMS), and TV channels. 35
Telemedicine
Telemedicine technology utilizes information and communication technologies for the delivery of healthcare services where distance is a critical factor. 36 In the wake of the COVID crisis, on 25 March 2020, the then Medical Council of India (MCI) published the telemedicine practice guidelines which encourage all the doctors in India to practice telemedicine. 36 In India, the vast majority of physical healthcare facilities are urban-based; thus, telemedicine offers an excellent tool for rural patients to avail quality diabetes care.
The country has many success stories in screening and managing diabetes and its comorbidities using the telemedicine approach. Telemedicine has been widely used to disseminate awareness about diabetes prevention among the urban and rural population; to enable patient monitoring; for remote real-time diabetic retinopathy screening; and in diabetes management at the primary, secondary, and tertiary levels. 37 The Chunampet Rural Diabetes Prevention Project (CRDPP) is an excellent model for the use of tele-diabetology in a cost-effective and sustainable manner to support healthcare in underserved areas in developing countries such as India by facilitating diabetes awareness, screening, and devising plans for diabetes prevention and treatment. The core of this project was a mobile van equipped with facilities for blood sampling, a digital retinal camera, a slit lamp, a computerized electrocardiogram (ECG), Doppler imaging, biothesiometry, and videoconferencing which commuted from village to village in the cluster, delivering diagnostic and screening services. The project succeeded in screening a large population, offering mass education on the benefits of glycemic control and prevention of diabetes-related complications as well as guaranteeing the availability of diabetes health services in remote areas of southern India.38–40 A comprehensive diabetes healthcare center in south India has been efficiently exploiting the Diabetes Tele-Management System (DTMS®), a telemedicine-based intervention and follow-up program for diabetes management since 1998. The DTMS® team uses telephone/email/secure website to educate patients/caregivers on insulin injection technique, diet, exercise, use of a glucometer, hypoglycemia, and compliance to medications as well as to titrate insulin and oral drug dosages according to personalized glycemic targets. 41 Telemedicine follow-up through DTMS® produced a significant reduction in HbA1c and hypoglycemia frequency in a cohort of 1000 patients with T2D. This approach ensures appropriate glycemic control, reduction in micro- and macrovascular complications, and multidrug compliance among the patients. The safety and cost-effectiveness of this system for intensive T2D treatment in the Indian population have also been demonstrated. 42 Focusing on screening and relieving diabetes, the fully digitalized hospital group in south India established a diabetes outpatient application (CURA) and an online diabetic management and care system based on the rationale that ‘a diabetologist sitting at home in front of a computer can treat 10 times more patients than seeing patients physically in clinic’. CURA application facilitated the treatment of 34,000 patients within the short span of 2 years of its launch. 43
Telemedicine has immensely supported the healthcare providers in India for diabetes management during the lockdown period. 44 A survey conducted among a population of patients with T2D during the lockdown reported that out of the patients who tried to consult the doctor, 30.6% utilized the telemedicine facility. The study confirmed the utility of telemedicine as a substitute to face-face consultation when travel restrictions were in vogue during the pandemic. 35
Virtual COVID IP(VCIP) in diabetes
Recently, during the COVID pandemic, a comprehensive diabetes hospital in south India introduced a COVID virtual in-patient concept. The preliminary data of the patients who availed the Covid virtual IP facility has been presented at the Advanced Technologies & Treatments for Diabetes (ATTD) 2021 Virtual Conference. 43 For consenting patients with diabetes diagnosed of Covid-19, Covid virtual IP care facility with 24/7 support, care and advice from a team of doctors, nurses, diabetes educators, and dietitians were provided. The care is coordinated through a dedicated WhatsApp group of patient and caretaker where a doctor and nurse are assigned duty 24/7.
The team follows up with the patient to assess parameters such as body temperature, blood glucose, blood pressure and saturation of peripheral oxygen (SpO2), and general well-being every 3–6 h. In addition, the intervention involves the use of remote monitoring technologies, timely initiation of steroids, injectable low-molecular-weight heparin, and so on at home itself by training patients via telemedicine. This technology-based intervention has produced excellent outcomes; a success rate of 99.5% was obtained among 220 patients. This approach offers a viable strategy to prevent the overwhelming of the hospitals during a pandemic and identification of those patients who need emergency hospitalization. 44
Mobile health (m-Health)
Since the number of mobile subscribers is high in India, healthcare interventions through mobile phones seem to be attractive. m-Health includes intervention and follow-up using text messaging, video messaging, voice calling, and Internet connectivity. 45
The applicability of SMS to introduce behavioral change in diabetes prevention and management programs in India has been widely explored. mDiabetes is a program implemented by Arogya World among 1 million Nokia subscribers to improve diabetes risk behaviors. The intervention group received 56 text messages in their choice of 12 languages over 6 months. The messages were intended to stimulate improvement in diabetes risk behaviors and increase awareness about the etiology and manifestations of diabetes. The messaging intervention improved the health behavior of the participants, resulting in an 11% increase in daily exercise, 15% increase in the intake of 2–3 servings of fruits a day, and 8% increase in 2–3 servings of vegetables per day. The outcomes showed a cumulative 15% improvement in the behavioral modifications postintervention. 46 Another study conducted at eight Arogya World Healthy Workplaces, based in Bengaluru, India, investigated the effectiveness of the Arogya World mobile phone application (myArogya app) in the primary prevention of diabetes through lifestyle changes. The intervention group received noncommunicable disease prevention messages twice a week for 6 months as modules. The prediabetes patients in the intervention group showed a greater reduction in the HbA1c levels (−1.9%) and blood pressure levels (systolic −2.7% and diastolic −3.1%), and a significant hike in the number of exercisers (8%) compared with the non-intervention group. 47 Another television-based lifestyle intervention program with weekly coach calls for 12 weeks was delivered to 1500 high-risk patients with T2D. The participants were Android smartphone users from three Indian cities namely, Chennai, Bengaluru, and New Delhi. The use of m-Health technology produced significant weight loss, improvement in cardiometabolic risk factors, and improvement in physical activity, QoL, and dietary habits. 48 The intervention group who exhibited more adherence to the program by watching the videos produced better weight reduction (2.4 kg) than those who merely attended the coach calls (0.9 kg). 49 A multicentric, randomized controlled trial conducted among newly diagnosed patients with T2D evaluated the impact of text messaging as a tool to improve glycemic outcomes. Here, the intervention group received personalized text messages at regular intervals (three times/week). The intervention supported HbA1c, and LDL-c reduction through personal empowerment and sustained behavioral changes. 50
Practo, mfine, DocsApp, 1mg, Netmeds, Lybrate, MediBuddy, and Medlife are m-Health applications that offer online doctor consultation or offline appointment booking through chat, audio, and video calling. These platforms have gained extensive popularity during the COVID pandemic. The absorption of these platforms reiterates their incorporation into our healthcare system in order to meet the growing medical needs of our country. 51
Diabetes-related apps
India’s high smartphone use statistics opens up possibilities for wider acceptance of digital diabetes technologies. India has the second highest number of smartphone users (439.42 million), next only to China. 51 Mobile applications and dosing algorithms provide appropriate lifestyle guidance, inspiration, and support to PwD as well as simplify communication with the healthcare provider. 34 A large number of digital health apps that help in the prevention and management of T2D are available in India through Google Play. These contain clinician-directed apps, education/training apps, diabetes management apps, insulin titration apps, medical consultation apps, diet/exercise apps, calorie tracker apps, apps that track and display health information, and social forums/blogs.
Titration inertia, or the delay to dose-titrate, is one of the main obstacles to augmented insulin therapy in India. Implementation of a patient-centric approach where all clinical decisions are guided by patient considerations has been proposed to produce favorable results. 52 Sanofi’s My Dose Coach mobile App has an in-built insulin dose calculator for patients with T2D to self-titrate basal insulin via automated dosing suggestions. 53 MyStar Plus (Sanofi) app helps in diabetes management by displaying all the diabetes-related data to facilitate precise and prompt clinical decisions. mySugr App (Roche) supports PwD in diabetes management by synchronizing with Accu-Chek blood glucose meter and transmitting the data to Apple and Android devices. 54
Recently, a study evaluated the quality of the commercially available diabetes apps in India. The results suggested two apps ‘Google Fit: Health and Activity Tracking’ and ‘HealthifyMe—Diet plan, Health and Weight Loss’ as being user-friendly and reliable quality. 55 Nevertheless, substantial evidence on the efficiency of these apps is still lacking.
Smartphone-based retinal photography
Diabetic retinopathy (DR) is one of the most common diabetes-related complications and its prevalence rates are increasing rapidly in India. 56 Four-field fundus photography using a retinal camera has been the golden standard for screening and assessment of DR. 34 Inadequate knowledge among clinicians about DR, incomplete awareness of patients, lack of adequate infrastructure for DR screening due to the higher cost and cumbersome installation procedures, and unskilled ophthalmologists are the major challenges to optimal DR management in India. 57 Scarcity of DR screening facilities at the primary and secondary level and lack of efficient referral mechanisms often put an overload on tertiary healthcare facilities. 57 Retinopathy screening using Smartphone-mounted retinal cameras [fundus-on-phone (FOP) cameras] has been considered as a promising alternative to alleviate these difficulties. The AI-powered smartphone FOP has shown very high sensitivity for DR and sight-threatening DR (STDR) against ophthalmologist’s grading. 58 The study in 301 patients (602 eyes) with T2D at a tertiary care diabetes center in south India showed that the specificity, sensitivity, and image quality of the smartphone FOP camera was comparable to 7-field mydriatic fundus photography. The Zeiss camera estimated NPDR 43.9%, Proliferative DR (PDR) 15.3% while the FOP camera estimated NPDR 40.2% and PDR 15.3%. 59 Comparison Among Methods of Retinopathy Assessment (CAMRA) Study in 300 patients with diabetes from south India reported the sensitivity and specificity of smartphone fundus photography compared with 7-field mydriatic fundus photography for the detection of DR as 50% and 94%, respectively, and that of nonmydriatic fundus photography were 81% and 91%, respectively. 60 The use of a smartphone-based nonmydriatic (NM) retinal camera before mydriasis presented good accuracy, sensitivity, and specificity in the detection of DR and STDR in comparison to a standard 7-field fundus photography with a desktop mydriatic fundus camera after mydriasis. 61 Similarly, NM retinal images captured using the Remidio NM FOP camera were analyzed with an offline smartphone-based Medios AI algorithm and compared with the image diagnosis of five retina specialists to reveal its high sensitivity and specificity in the detection of DR. 62 Smartphone-based retinal screening allows low-cost examination of retinopathy without compromising image quality, accuracy, and specificity. It has the potential to take DR screening to rural and remote settings and thereby lessen the burden of DR screening in low- and middle-income countries (LMIC) like India. 63
Electronic medical records
EMR is a systematized assortment of patient and population electronically saved health information in a digital format. 64 The technology enables sharing of a large collection of data across networks that was not possible with paper documentation. EMR has been an integral part of quality care in several diabetes clinics in India. A tertiary care center in south India has been utilizing diabetes electronic medical record (DEMR) for storage and tracking of the demographic and clinical details of a large number of patients. The study involving 139,906 male and 86,322 female patients with diabetes reported the usefulness and credibility of the system in diabetes care and research. 65 EMR has been the core of DTMS®, a telemedicine-based diabetes intervention platform utilized at a comprehensive diabetes care center in south India. Here, the patient details collected via voice messages/SMS/E-mail/live streaming audio or video over the Internet are incorporated in the EMR for clinical evaluation and data mining for clinical research. 39 These facts indicate that EMR and computerized clinical decision-support systems (CDSS) can help the clinicians and patient community of LMIC to conquer system-level challenges to refining evidence-based health care delivery. A systematic study showed that diabetes intervention through EMR-CDSS has provided the patients with a feeling of empowerment and benefits from better provider concentration and feedback. The study also identified several factors such as limited resources, individual economic adversities, and dearth of structured systems or trained personnel that can impede the wide implementation of EMR in therapeutic decision making for diabetes management. 66
Table 1 comprises the major digital technologies currently practiced in India for diabetes management.
The major digitalized technologies currently practiced in India.
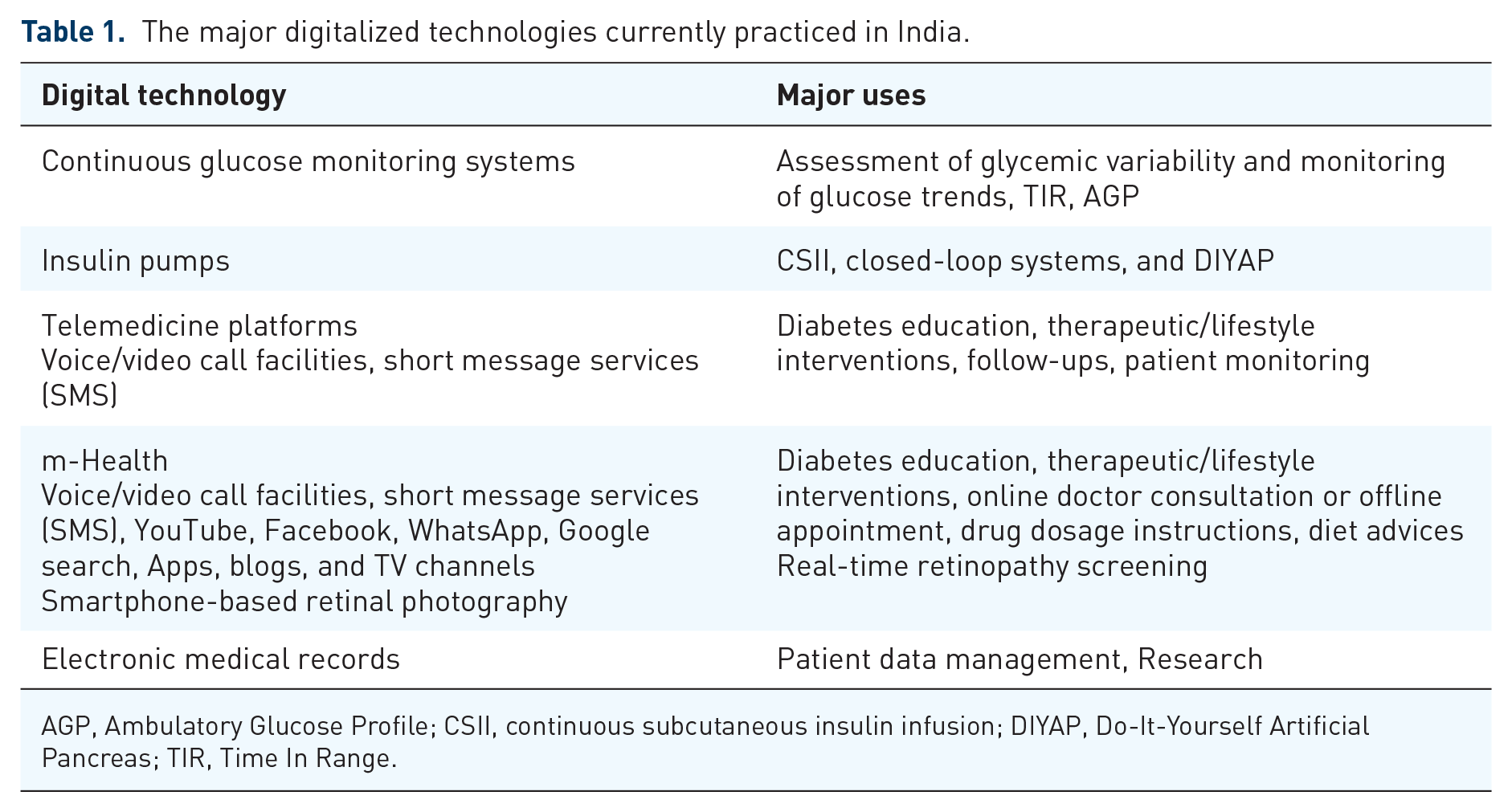
AGP, Ambulatory Glucose Profile; CSII, continuous subcutaneous insulin infusion; DIYAP, Do-It-Yourself Artificial Pancreas; TIR, Time In Range.
Digital health through start-ups in India
Recently, many start-ups centering on digital health-based diabetes screening and management have come into existence through financial support from different branches of the Government of India such as the Technology Development Board (TDB), the Department of Science & Technology (DST), the Department of Biotechnology (DBT), BIRAC, Millennium Alliance (an initiative backed by the DST, FICCI & USAID) and the Indo USA Science & Technology Fund (IUSSTF), Bill & Melinda Gates Foundation, and the Wellcome Trust. Yostra, a Medtech start-up, has developed a product, NeuroTouch™, for the screening and detection of peripheral neuropathy in PwD. These are hand-held, battery-operated, wireless, screening device with an in-built algorithm for analysis, interpretation, and transfer of data. This product has been currently validated at several hospitals and research institutes in India. 41 Artelus develops innovative screening gears to diagnose diseases such as diabetes, tuberculosis, and breast cancer. Companies such as Artelus, Chironx, and DRISTi exploit deep learning algorithms and AI-based interventions to screen patients with diabetes for the early recognition of DR from retinal image scans.67–69 BeatO is an AI-based app, specifically designed for Indian middle-class patients with diabetes. The app provides appropriate nutritional tools to advise the users about diabetes-friendly foods, the amount of food, and to identify the glycemic index of the patient. The app also has a smart glucometer that can be connected to a smartphone and the glucose readings can be used for making therapeutic decisions. 69 However, the surveillance accuracy of this smartphone-dependent glucose meter (SDGM) should be further evaluated. 70 HealthifyMe, another AI-based start-up, concentrates on lifestyle diseases such as obesity, hypertension, and diabetes. Here, the AI-enabled nutrition coach Ria interacts with the users to support them with diabetes-related queries. 71 A systematic study has reported HealthifyMe as being good quality and user-friendly for the prevention of T2D among Asian Indians. 55 A healthcare start-up, Orbuculum, uses AI on genomic data to forecast the risk of developing diabetes. 69 Wealthy, another venture, offers affordable AI-based digital diabetes coaching solution to motivate Indian patients with T2D for diabetes self-management and to improve their QoL. 69
Opportunities and limitations
Diabetes digital health offers an optimal solution for reforming India’s primary health ecosystem. It effortlessly interconnects multiple components of diabetes care including clinicians, patients, diabetes educators, nurses, and caregivers via smartphones and other communication devices. Digital technology platforms motivate the patients for diabetes self-management through constant follow-ups, suggestions, feedback, and alerts. The role of digital technologies in initiating better interventions and diet/lifestyle modifications is slowly gaining acceptance. This role has utmost significance in a country like India where 54.4% of the population are inactive and less than 10% engage in recreational physical activities. 71
The role of Telehealth was established in India during the COVID pandemic as it strengthens the healthcare systems by meeting the huge treatment needs while avoiding unnecessary clinic visits and face-to-face consultations. Telecare has provided superior outcomes in access to medical professionals, diagnosis rates, and treatment adherence. This model posed to become a pillar of diabetes care as more patients are affected by multiple chronic conditions that necessitate immediate attention.
Education and training through web portals, blogs, videos, and structured online modules are beneficial for patients/caregivers and healthcare practitioners to improve their knowledge and skills on diabetes technologies and quality care. For LMIC like India, digital health provides an opportunity for intelligent and efficient resource management. All these outcomes have the potential to reduce the cumulative costs of diabetes care.
While diabetes digital health offers immense possibilities for a country like India, several key obstacles are preventing its full utilization. Any assessment to quantify the growth in economic output credited to digitalization in India must be adjusted for the intrinsic negative pull-on productivity due to the country’s fragmented health system. Wider implementation of digital platforms or technologies requires upgradation and customization of existing practices/protocols/hardware and the consumers have to pay a high initial cost. Lack of insurance converge on advanced digital technologies and devices may also restrict their use in India.
Improper understanding or training on digital technologies in diabetes care is another limiting factor. The ignorance about the technology may lead to the patient community resisting the adoption of digital care and thus they may still prefer the traditional methods. Independent practitioners particularly in remote rural areas may not have EMRs. Developing faith in the new user interface between doctors and patients is highly essential in this context. Ethical concerns over cybersecurity, data privacy, and ownership are the biggest challenges of telemedicine and digital health. 72 It should be the responsibility of the users to confirm the authenticity of the providers especially since personal identifiable data about the disease condition and well-being is collected and stored in interconnectable networks. Scientific evidence supporting the quality, safety, and efficiency of digital health technologies may further delay its wide adoption. 9
The long-standing digital divide that exists between the rural and urban areas in India needs to be addressed on a priority scale. Lack of connectivity ascribed to limited access to high-speed broadband Internet and poor telecommunication infrastructure can impede the implementation and growth of telehealth programs that need live-video connections between patients and providers. 72 Dropped calls and delays in the video can interfere with care delivery and result in patient frustration with telehealth. However, many of these obstacles can be addressed effectively through well-defined policies, programs, and research studies. This requires massive investments in basic/clinical research, product development, Information Technology, and various other industries. A well-strategized mandate to develop and conduit diabetes digital technologies will have a positive impact on the health of our society in the future. A pictorial representation of the above identified opportunities and obstacles is given in Figure 1.
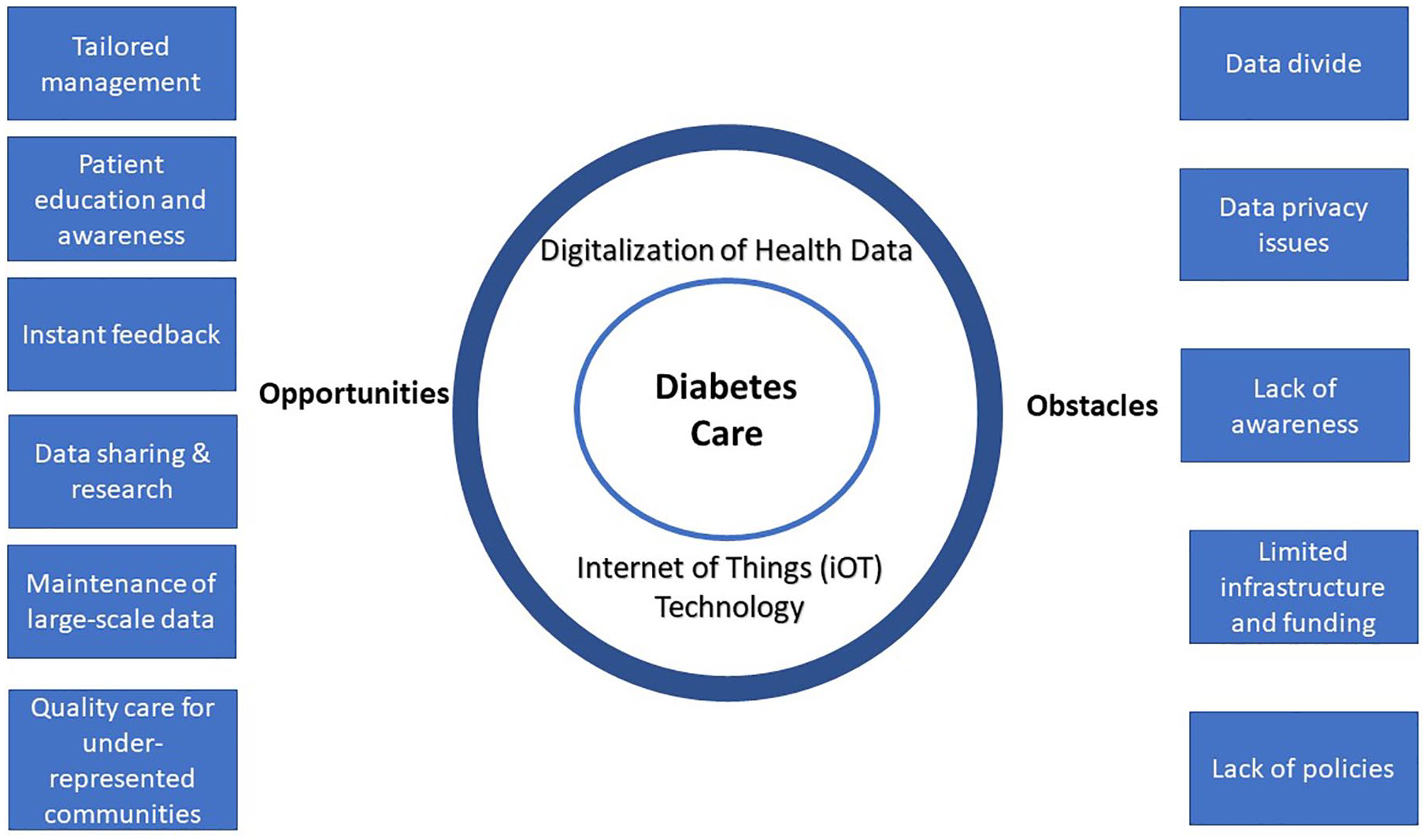
The main opportunities and obstacles implicated in the wider implementation of digitalization of diabetes health in India.
The lack of easy access to quality health care facilities in the country contributes to an increased number of patients who fail to achieve recommended glycemic targets and a higher risk of long-term complications. The same factor results in lower levels of self-reported diabetes observed in people with diabetes living in low socio-economic groups. Digital diabetes health approaches overcome the digital divide and help improve access to medical care irrespective of the patients’ locations. Intensified country-wide training programs for healthcare providers, patients, and caregivers on the latest digital technologies can speed up the acceptability of these technologies among the population. Compared with many other countries, computer literacy and smartphone usage are very high in the Indian population. Therefore, technology adoption along with extended infrastructure and competencies from process improvements could aid in advancing health care accessibility and affordability. Digitalization of diabetes care in India has to help overcome the several obstacles including inadequate access, low insurance penetration, and an increasing disease burden. Many domestic initiatives have helped in decreasing the prices of diabetes care products. Parallelly, changes in policy by regulators and supporting technological interventions is the need of the hour.
Conclusion
The slow but steady progress toward the digitalization of diabetes care has been the innovation of this decade. Emerging technologies such as real-time continuous glucose monitoring, automated insulin delivery systems, EMRs, m-Health, and telemedicine are steadily picking up in the country.
Indeed, the COVID pandemic era has witnessed the wide acceptance of telehealth, electronic, and mobile health platforms for diabetes care. The growing diabetes population is putting immense pressure on India’s healthcare and economic infrastructures. The Government has understood that without the digitization of health care services, the country cannot accomplish its growth potential. Digital solutions have supported patients with diabetes to improve their glycemic outcomes and to avail high-quality and cost-effective care. But the country has to ensure digital equivalence across the urban and rural regions by bridging the gap between technology start-ups, hospitals, manufacturers, and other stakeholders. It is hoped that the outcomes, information, knowledge, and services generated using digital health technologies will initiate further innovations in diabetes care and thus help to improve the lives of people with diabetes. The time to act is NOW!
Footnotes
Acknowledgements
The authors thank all those who helped in manuscript preparation.
Author contributions
JK and GK wrote the initial draft and VM helped to revise several versions of the manuscript.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.