
Abstract
Background:
The number of patients ⩾65 years who require maintenance hemodialysis (MHD) is increasing. Although reduced bone turnover in older patients receiving hemodialysis, as reflected by lower serum intact parathyroid hormone (iPTH) and phosphate (P) levels, has been reported, focus on the association between abnormal bone metabolism and the risk of death in older patients receiving MHD has been limited.
Methods:
We retrospectively examined data from the Beijing Hemodialysis Quality Control and Improvement Center for 1410 older patients who underwent hemodialysis from 1 January 2012 to 31 December 2016. Baseline, time-dependent (TD) Cox proportional hazards models and Kaplan–Meier analyses were used to evaluate the association between the markers of mineral and bone disorder (MBD) [calcium (Ca), P, and iPTH] and survival. The Kidney Disease: Improving Global Outcomes (KDIGO) target ranges were included as reference values.
Results:
Serum P levels >2.49 mmol/l increased the risk of all-cause death [hazard ratio (HR): 1.46; 95% confidence interval (CI): 1.04–2.07; p = 0.030] and cardiovascular death (HR: 2.01; 95%CI: 1.21–3.34; p = 0.007); iPTH levels >600 pg/ml increased the risk of cardiovascular death (HR: 1.95; 95%CI: 1.20–3.15; p = 0.007). Baseline results and TD Cox analyses were similar. All three MBD parameters were within the respective target ranges at least once during the follow-up period in 399 (28.3%) patients, and these patients had better survival rates than those who achieved two of the three target ranges (715/1410 patients; 50.7%); those who achieved one or no target range (296/1410; 21.0%) had the lowest survival rate (all-cause death: log-rank chi square = 83.96, p < 0.001; cardiovascular death: log-rank chi square = 47.06, p < 0.001).
Conclusion:
Older patients undergoing MHD who achieved the KDIGO target levels for any two or three MBD parameters had lower risks of all-cause and cardiovascular death.
Introduction
Chronic kidney disease-mineral and bone disorder (CKD-MBD) is a systemic condition that occurs due to CKD. 1 Patients undergoing maintenance hemodialysis (MHD) often experience CKD-MBD, which is characterized by abnormal serum levels of calcium (Ca), phosphate (P), and intact parathyroid hormone (iPTH). These abnormalities increase the risk of extraosseous and vascular calcification, resulting in a higher incidence of cardiovascular disease (CVD) and mortality from CVD.2–4 The global population is aging rapidly; therefore, most patients undergoing MHD for end-stage renal disease (ESRD) will be ⩾65 years of age in the near future. Data from the United States (US) Renal Data System indicate that over 50% of patients receiving incident hemodialysis are ⩾65 years old. 5 The number of older dialysis patients is increasing in Beijing, and the percentage of older individuals among all dialysis patients increased from 28.2% to 30.9% between 2007 and 2010. 6 Age is an independent risk factor for death and affects the metabolism of Ca and P. Previous studies reported that patients ⩾75 years of age had lower and better-controlled serum P and iPTH levels than younger patients based on the Kidney Disease Outcome Quality Initiative (K/DOQI) targets; however, the mortality rates of the older patients were higher.7–10 Thus, older patients undergoing MHD tend to have better-controlled serum P and iPTH level as well as higher mortality rates. Although this phenomenon has attracted the attention of nephrologists, a smaller proportion of these studies have addressed the association between survival rate and management of serum Ca, P, and iPTH levels in older patients undergoing MHD.
Therefore, this study aimed to evaluate the association between MBD parameters (serum Ca, P, and iPTH levels) and long-term death in patients ⩾65 years undergoing MHD in Beijing. The target ranges for the MBD parameters used in this study were based on the 2017 international Kidney Disease: Improving Global Outcomes (KDIGO) guidelines.
Materials and methods
Study design
This retrospective cohort study was approved by the Institutional Review Board of Beijing Friendship Hospital, Capital Medical University (approval number: BJFH-EC/2016-P2-126-02) and was performed in accordance with the principles of the Declaration of Helsinki. Ethical approval, which exempted the study from the need to obtain informed patient consent, was obtained in accordance with Article 39 of China’s regulation on “Ethics review process on human-related biologic and medical research.” The study was registered at [ClinicalTrials.gov identifier: NCT03261154].
Patient data from the database of the Beijing Hemodialysis Quality Control and Improvement Center (BJHDQCIC) between 1 January 2012 and 31 December 2016 were reviewed, including information regarding patient demographics, medical history, and laboratory parameters. Baseline serum levels of Ca, P, iPTH, and albumin (Alb) for each patient included the mean levels of the available data recorded in the database between January and June 2012 (i.e., the first 6 months of the study period). Patient-level follow-up data were the first available data recorded in the database for each patient in the 12-month period of 2013, 2014, 2015, and 2016. Information regarding all-cause and cardiovascular deaths was collected throughout the study. The data were analyzed to identify the potential association between achieving target ranges of Ca, P, and iPTH according to the KDIGO guidelines and all-cause and cardiovascular deaths. To assess the effect of simultaneously achieving the KDIGO target values on survival, patients were classified into three groups based on the degree of achievement of KDIGO MBD targets: patients who achieved the target levels for all three MBD parameters at one or more points during the study period; patients who simultaneously achieved the target levels of two MBD parameters at least once during the study period; and patients who achieve one or none of the target levels of MBD parameters during the study period. A secondary sensitivity analysis, to account for race and ethnicity, was conducted with the patients classified into three subgroups based on the following target ranges: Ca, 2.10–2.55 mmol/l; P, 1.13–1.78 mmol/l; iPTH, 150–600 pg/ml. 10
Patient population
Patient data were obtained from the BJHDQCIC, which was established by the Beijing Health Bureau in 2003. A major function of the BJHDQCIC is the registration and collection of data on ESRD.6,11 In 2007, the BJHDQCIC began to collect patient-level data from 120 hemodialysis centers in Beijing, and published an annual data report. The inclusion criteria of this study were as follows: age ⩾65 years, undergoing dialysis for at least 6 months at a frequency of three 4-h sessions per week, and a dialysate Ca concentration of 1.5 mmol/l and bicarbonate level of 32–35 mmol/l. In contrast, patients were excluded due to missing demographic information, clinical history, or laboratory values. Ultimately, 1410 out of 2296 patients from the database were included in this study (Figure 1).

Patient flow chart.
CKD-MBD parameters
The following 2017 KDIGO target ranges for each MBD parameter were used in this study: serum Ca level of 2.11–2.52 mmol/l, P level of 0.85–1.51 mmol/l (the normal limit according to the Health Industry Standards of the People’s Republic of China WS/T is 404.6–2015), and iPTH level of 130–600 pg/ml (an iPTH of 2–9 times the normal upper limit is recommended by the KDIGO guidelines).8,12,13
Covariates of interest
Baseline data, including patient demographics (age, sex, and hemodialysis vintage), medical history [primary cause of ESRD, CVD (defined as peripheral vascular disease, congestive heart failure, coronary artery disease, myocardial infarction, or angina), diabetes, and cancer-related comorbidities], and laboratory parameters [including pre-dialysis serum Ca, P, iPTH, Alb, total cholesterol (TC), hemoglobin (Hb), creatinine, and dialysis adequacy (Kt/V)] were recorded. Ca levels were calculated according to the following formula:

Patient-level follow-up data (serum Ca, P, iPTH, and Alb levels) of each individual patient included the first available data for that patient in each 12-month time period of 2013, 2014, 2015, and 2016 recorded in the database.
Study outcomes
The primary outcome was all-cause death. Cardiovascular death, including deaths attributed to acute myocardial infarction, acute heart failure, cardiac arrhythmia, or cardiac arrest (causes unknown), was the secondary outcome.
Statistical analysis
Normally distributed continuous variables are presented as means and standard deviations (SD), while non-normally distributed variables are presented as medians and interquartile ranges (IQR). Categorical variables are presented as frequencies (percentages).
Baseline and time-dependent (TD) Cox proportional hazards models were used to analyze the associations between MBD markers and clinical outcomes. In these two models, MBD markers (Alb-corr. Ca, P, and iPTH) were defined as predicting variables, and the outcome variable was death; the adjusted covariates were age, sex, hemodialysis vintage, medical history (diabetes, CVD, or cancer), pre-dialysis serum Alb, Hb, TC, and creatinine levels, and dialysis adequacy (Kt/V). In the TD Cox analyses, serum Alb-corr. Ca, P, and iPTH were used as TD Cox covariates and were updated every 12 months. Missing data in the TD Cox models were handled using the last observation carried forward (LOCF) method. The analysis of individual patients ended at their final follow-up date if they were transferred to peritoneal dialysis and/or lost to follow up, and patients lost to follow up were assumed to be still alive at the end of the study period. The Kaplan–Meier (KM) method was used to estimate the cumulative probability of all-cause death and cardiovascular death in older patients. Similarly, KM survival estimates were obtained to assess the effect of achieving none/single or multiple KDIGO MBD target values on all-cause death and cardiovascular death.
Statistical analyses were performed using SAS version 9.4 statistical software (SAS Institute Inc., Cary, NC, USA). Statistical significance was set at p < 0.05, and all statistical tests were two-sided.
Results
Baseline clinical features
Of the 1410 patients included in this study, 796 (56.5%) were females. The mean patient age was 74.14 ± 5.62 years (range 65–94 years). Nine patients (0.6%) were transferred to peritoneal dialysis, and 23 (1.6%) were lost to follow up. The median (IQR) follow-up period was 60 (27–60) months. In total, 646 (45.8%) patients died during the study period. The primary causes of death were cardiovascular death (n = 238, 36.8%), infection (n = 159, 24.6%), and cancer/dyscrasia (n = 96, 14.9%). Patient demographic and baseline parameters are shown in Table 1.
Patients’ baseline characteristics.

Alb, albumin; Alb-corr. Ca, Alb-corrected. calcium; Cr, creatinine; CVD, cardiovascular disease; ESRD, end-stage renal disease; Hb, hemoglobin; iPTH, intact parathyroid hormone; IQR, interquartile range; Kt/V, dialysis adequacy; P, phosphate; SD, standard deviation; TC, total cholesterol.
Serum Alb-corr. Ca, P, and iPTH levels and the risk of death
The associations between serum Alb-corr. Ca, P, and iPTH levels and 5-year survival are shown in Figures 2–4 and Supplemental Table S1. The relative risks of all-cause and cardiovascular death based on adjusted Cox models with baseline data only and TD Cox models using the LOCF method are shown.
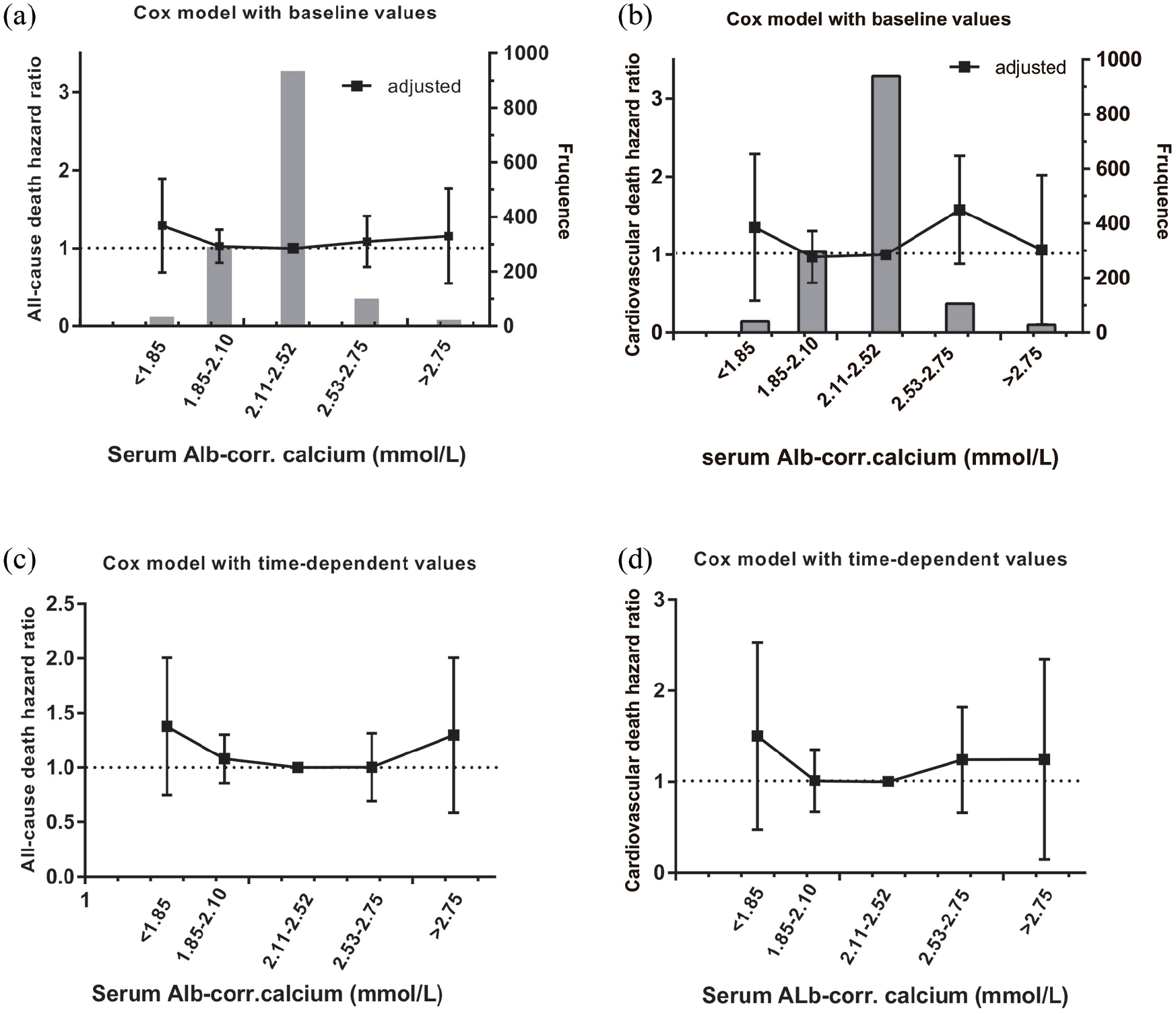
The association between albumin-adjusted serum calcium values and the relative risk of death in 1410 older patients undergoing maintenance hemodialysis (MHD) over a 5-year period using adjusted Cox modeling. (a) Baseline values and all-cause mortality HRs. (b) Baseline values and cardiovascular death HRs. Panels (a) and (b) similarly include a background bar diagram to reflect the patient population frequency in each group. (c) TD Cox model and all-cause death HRs. (d) TD Cox model and cardiovascular death HRs.

Association between serum phosphate values and relative risk of death in 1410 older patients undergoing MHD over a 5-year period using adjusted Cox modeling. (a) Baseline values and all-cause death HRs. (b) Baseline values and cardiovascular death HRs. Panels (a) and (b) similarly include a background bar diagram to reflect the patient population frequency in each group. (c) TD Cox models and all-cause death HRs. (d) TD Cox models and cardiovascular death HRs.

Association between serum iPTH values and relative risk of death in 1410 older patients undergoing MHD over a 5-year period using adjusted Cox modeling. (a) Baseline values and all-cause death HRs. (b) Baseline values and cardiovascular death HRs. Panels (a) and (b) similarly include a background bar diagram to reflect the patient population frequency in each group. (c) TD Cox models and all-cause death HRs. (d) TD Cox models and cardiovascular death HRs.
The adjusted baseline and TD analyses showed that Alb-corr. Ca levels greater than the target range had no effect on the risk of all-cause or cardiovascular death (Figure 2, Supplemental Table S1). In the baseline Cox analysis, patients with high serum P (>2.49 mmol/l) levels had a higher risk of all-cause death than those with serum levels within the target range (0.85–1.51 mmol/l) [hazard ratio (HR): 1.46; 95% confidence interval (CI): 1.04–2.07; p = 0.030]. Similar results were observed in the TD Cox model (HR: 1.40; 95%CI: 1.00–1.97; p = 0.050) (Figure 3a, c). A high serum P (>2.49 mmol/l) level was correlated with a high risk of cardiovascular death at both baseline (HR: 2.01; 95% CI: 1.21–3.34; p = 0.007) and in TD Cox models (HR: 2.04; 95%CI: 1.24–3.35; p = 0.005) (Figure 3b, d).
The risk of all-cause death was not higher in patients with serum iPTH levels above or below the KDIGO target range (Figure 4a, c). Patients with a serum iPTH level of 600.01–1000 pg/ml showed an increased risk of cardiovascular death (HR: 1.95; 95% CI: 1.20–3.15; p = 0.007), as did patients with a serum iPTH >1000 pg/ml (HR: 1.99; 95%CI: 1.17–3.40; p = 0.012). Similar results were observed in the adjusted TD Cox analysis for patients with a serum iPTH level of 600.01–1000 pg/ml (HR: 1.85; 95% CI: 1.14–2.99; p = 0.012) and those with a serum iPTH >1000 pg/ml (HR: 2.07; 95% CI: 1.21–3.53; p = 0.008) (Figure 4b, d).
Achievement of KDIGO target values
Patients with serum Alb-corr. Ca, P, and iPTH levels within the target ranges and those with any two of the three parameters within the target ranges had higher survival rate than those with one or no parameters within the target ranges (all-cause death: log-rank chi square = 83.96, p < 0.001 and cardiovascular death: log-rank chi square = 47.06, p < 0.001) (Figure 5). As shown in Figure 5, the event curves of patients with two or more parameters within the target ranges diverged from those of patients with no parameters within the target range at the 12-month time point and continued to diverge throughout the duration of the study.

Kaplan–Meier curve indicating the survival rate of older patients undergoing MHD over the study period. (a) Survival estimates (all-cause death) for older MHD patients. (b) Survival estimates (cardiovascular death) for older MHD patients. Tri-target: patients who achieved all three MBD targets (Alb-corr. Ca, phosphorus, and iPTH) based on the 2017 KDIGO guidelines; two of three targets: patients who achieved any two of the three MBD target parameters; off-target: patients who achieved one or no MBD targets.
Age, diabetes mellitus, serum albumin, and the risk of death
Each 1-year increase in patient age resulted in a 5% increase in the risk of all-cause and cardiovascular deaths. The presence of diabetes was significantly associated with a higher risk of death (Supplemental Table S1). Furthermore, the serum Alb level was significantly associated with a decreased risk of death (Supplemental Table S1).
Sensitivity analysis
When patients were classified into subgroups based on different target ranges of Ca, P, and iPTH levels, the results aligned with the results obtained using the KDIGO target ranges (all-cause death: log rank chi-square = 160.94, p < 0.001; cardiovascular death: log rank chi-square = 47.82, p < 0.001) (Supplemental Figure S1).
Discussion
This cohort study with a large sample size was designed to evaluate the association between the international KDIGO target ranges for CKD-MBD parameters and death in patients ⩾65 years of age undergoing MHD in Beijing. We observed that a high serum P level (>2.49 mmol/l) leads to an increased risk of all-cause death and cardiovascular death, while a high iPTH level (>600 pg/ml) lead to an increased risk of cardiovascular death. Similarly, we assessed the interdependency of Ca, P, and iPTH levels for all-cause death and cardiovascular death. The survival rate of patients who achieved the target ranges for all three parameters was higher than that of patients who achieved the target ranges for two parameters. Patients who achieve one or none of the target ranges for the MBD parameter had the lowest survival rate.
In recent years, many studies have specifically assessed imbalance in the metabolism of Ca, P, and iPTH and their relationships with the outcome in patients undergoing hemodialysis. Although numerous studies have shown a U-shaped relationship between different levels of serum Ca, P, and iPTH and the risk of death, the thresholds of Ca, P, and iPTH that lead to increased risk of death are different. We observed that high serum P levels (>2.49 mmol/l) increased the risk of all-cause death and cardiovascular death in older patients undergoing MHD and that Ca and iPTH levels outside the target ranges were not associated with all-cause death; however, an iPTH level >600 pg/ml increased the risk of cardiovascular death. These results may be attributable to several factors. First, vascular calcification is commonly observed in patients undergoing dialysis and contributes to CVD and increased mortality rates among patients with CKD. The major risk factors for vascular calcification in patients with CKD include age, dialysis vintage, hyperphosphatemia, and positive net Ca and P balances. The serum P plays a key role in vascular calcification. 4 Cardiovascular or all-cause outcomes are less frequently correlated with the serum Ca level than with the serum P level in patients with CKD. 14 Serum iPTH activity, as a defense mechanism, can prevent increases in serum P levels. Therefore, the effect of serum iPTH on vascular calcification or all-cause death is not as direct as that of serum P. Second, our study differs from previous studies in that we examined older patients undergoing MHD. The causes of ESRD, comorbidity, and risk factors for mortality differ between older and younger patients. 15 Older patients exhibited lower serum P, iPTH, and albumin levels and reduced protein intake compared with younger patients undergoing hemodialysis.9,15 Results from previous studies supported the significant association between the markers of MBD and risks of both cardiovascular and all-cause death; however, cardiovascular deaths accounted for approximately 50% of the total deaths in the study.3,16 Our study showed that cardiovascular death accounts for approximately one-third (36.8%) of total deaths in older patients undergoing MHD. In addition, factors less strongly associated with iPTH, including infection, cancer, and dyscrasia, 17 are more frequent causes of death in older patients (40%). The difference in the studied population may cause the difference between our study and other related studies. Moreover, serum phosphate levels, besides being correlated with vascular calcification, are positively associated with nutritional biomarkers. 18 Lower serum P levels may be due to a lower daily P intake and are consistent with the lower rate of bone turnover in older patients undergoing hemodialysis. 9 The serum albumin level has been shown to predict all-cause, cardiovascular, and infection-related mortality rates in dialysis patients. 19 Consistent with these findings, the serum Alb level was a risk factor for all-cause and cardiovascular death in older patients undergoing MHD (Supplemental Table S1). Results from adjusted Cox analysis did not indicate that hypophosphatemia increases the risk of death, and this may have been because only a few older patients in this study had serum P level <0.85 mol/l (Figure 3).
Since the KDIGO guidelines have been used in clinical practice in China since 2012, the KDIGO target ranges for Ca, P, and iPTH were used in this study. We performed a sensitivity analysis using the target ranges adopted by practitioners in the US and Europe to account for differences in race and ethnicity. 10 The results of the sensitivity analysis were consistent with those of our primary study. The survival rate of patients in whom all three parameters were within the target ranges was 18% higher at 12 months and 32% higher at 48 months than that of patients in whom one or no parameter was within the target ranges (Figure 5). Similar results were obtained for cardiovascular death rates (Figure 5). Our results are consistent with those of previous studies.13,20,21 We believe that the effects of bone metabolism disorders on the risk of death progress over time and that achieving the KDIGO target ranges for two or three parameters improves long-term survival in older patients undergoing MHD. Previous studies support our hypothesis.13,22 One study with a 3-year follow-up period concluded that continuous control of bone metabolism based on the K/DOQI targets was a strong predictor of survival in patients undergoing hemodialysis. 13 In contrast, a 2-year study did not recommend the use of K/DOQI bone mineral target ranges as quality indicators of dialysis care. 22 The conflicting results of these two studies may be due to the differences in the length of the study periods. A recent study reported that patients with two MBD parameters above the target range had an increased risk of mortality than patients with all MBD parameters within the target ranges; meanwhile, patients ⩾65 years of age with two MBD parameters above the target range had a higher risk of mortality than those aged <65 years. 10 The mortality risk associated with each parameter may be due to statistical over-adjustment, which can obscure both biologic inter-relationships and therapeutic treatment effects. Furthermore, since the MBD parameters are interrelated, there may be bias in the observed effect estimates.20,23 Although serum iPTH and P levels are typically lower in older patients,9,15 a higher mortality risk has been reported for older patients. 10
Although MBD medications were not analyzed in this study due to the unavailability of such information in the database, we hope that our findings will result in further studies focusing on older patients undergoing MHD to improve the long-term survival rate of older patients. Older patients undergoing hemodialysis may similarly experience undiagnosed osteoporosis and may benefit more from individualized CKD-MBD management than younger patients. 24 The therapeutic decisions of CKD-MBD are based on trends rather than on a single laboratory value, considering all available CKD-MBD assessments. 12
This study has some limitations. First, its retrospective and observational nature may have introduced bias. Second, complete hemodialysis components, such as vascular access, high-efficiency dialyzer, and high-flux and low-flux dialyzers, were not examined in this study and should be incorporated in future research. Third, the effects of medications, such as vitamin D supplements and calcium-containing phosphorus binders, could not be assessed since data regarding supplements were not recorded. Other drugs, such as lanthanum carbonate sevelamer and cinacalcet, were not included in the Beijing Medical Insurance List before 2016; hence, they were not widely used during the study period; therefore, the effects of those drugs were not assessed.
Conclusion
Older patients who achieved the KDIGO target ranges for two or three MBD parameters showed better 5-year survival rates than patients who achieve one or none of the KDIGO target ranges for MBD parameters. Since this is a retrospective and observational study, additional research is required to further validate our results. The present findings may help us refine future recommendations for the treatment of older patients undergoing MDH.
Supplemental Material
sj-eps-2-tae-10.1177_20420188211025161 – Supplemental material for Association between the risk of death and serum calcium, phosphate, and intact parathyroid hormone levels in older patients undergoing maintenance hemodialysis: a cohort study in Beijing
Supplemental material, sj-eps-2-tae-10.1177_20420188211025161 for Association between the risk of death and serum calcium, phosphate, and intact parathyroid hormone levels in older patients undergoing maintenance hemodialysis: a cohort study in Beijing by Dishan Li, Wenhu Liu, Hongdong Huang, Wang Guo, Zongli Diao, Xinpan Chen and Weiwei Wangs in Therapeutic Advances in Endocrinology and Metabolism
Supplemental Material
sj-pdf-1-tae-10.1177_20420188211025161 – Supplemental material for Association between the risk of death and serum calcium, phosphate, and intact parathyroid hormone levels in older patients undergoing maintenance hemodialysis: a cohort study in Beijing
Supplemental material, sj-pdf-1-tae-10.1177_20420188211025161 for Association between the risk of death and serum calcium, phosphate, and intact parathyroid hormone levels in older patients undergoing maintenance hemodialysis: a cohort study in Beijing by Dishan Li, Wenhu Liu, Hongdong Huang, Wang Guo, Zongli Diao, Xinpan Chen and Weiwei Wangs in Therapeutic Advances in Endocrinology and Metabolism
Footnotes
Author contributions
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Beijing Municipal Administration of Hospitals Clinical Medicine Development of Special Funding Support (Code: ZYLX201824).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.