
Abstract
Hypothalamic amenorrhoea (HA) accounts for approximately 30% of cases of secondary amenorrhoea in women of reproductive age. It is caused by deficient secretion of hypothalamic gonadotrophin-releasing hormone, which in turn leads to failure of pituitary gonadotrophin and gonadal steroid release. Functional HA (FHA) is defined as HA occurring in the absence of a structural lesion and is predominantly caused by significant weight loss, intense exercise or stress. Treatment of FHA is crucial in avoiding the long-term health consequences on fertility and bone health, in addition to reducing psychological morbidity. This article summarises our understanding of the mechanisms underlying FHA, the evidence base for its clinical management and emerging therapies.
Introduction
Hypothalamic amenorrhoea (HA) accounts for approximately 30% of cases of secondary amenorrhoea in women of reproductive age. 1 It is caused by deficient secretion of hypothalamic gonadotrophin-releasing hormone (GnRH), which in turn leads to failure of pituitary gonadotrophin and gonadal steroid release. Functional HA (FHA) is defined as HA occurring in the absence of a structural lesion, although the terms FHA and HA are often used interchangeably. FHA is predominantly caused by significant weight loss, intense exercise or stress, or a combination of such. 1 In addition, there may be a genetic predisposition for the development of FHA, such as heterozygosity for congenital hypogonadotropic hypogonadism. 2 Treatment of FHA is crucial to avoid the long-term health consequences on fertility and bone health, in addition to reducing psychological morbidity. Initial management should be focused on resolving the precipitating cause of FHA such as low weight, excessive exercise or stress. In those where FHA persists, treatments are generally limited to hormone replacement with the aim of maintaining oestrogen levels, or ovulation induction or in vitro fertilisation (IVF) in those seeking pregnancy. This article summarises our understanding of the mechanisms underlying FHA, the evidence base for its clinical management and emerging therapies.
Pathophysiology
The normal functioning of the hypothalamic–pituitary–ovarian (HPO) axis is essential for reproductive health. Gonadotropins, i.e. luteinising hormone (LH) and follicle-stimulating hormone (FSH), are secreted by the pituitary gland secondary to pulsatile stimulation by hypothalamic GnRH. HA is defined as the cessation of menstruation due to abnormal signalling between the hypothalamus and the pituitary gland due to deficient pulsatile secretion of GnRH. 3 This reduced secretion of GnRH leads to levels of LH and FSH that are insufficient to maintain full folliculogenesis and normal ovulatory ovarian function, with consequent oestrogen deficiency. Rarely, HA may be caused by a structural lesion such as a hypothalamic tumour. 3 In the absence of a structural lesion, HA is classified as being functional; FHA is caused by a number of factors including stress and chronic illness. 1 However, the majority of cases of FHA result from a relative energy deficit within the body associated with weight loss or exercise.4–6 More rarely, FHA can occur without a precipitating cause, in which case it can be labelled idiopathic HA. The most serious consequences of HA include delayed puberty, amenorrhoea, infertility and the effects of long-standing oestrogen deficiency on bone mineral density (BMD), sexual and genitourinary health and potential effects on cardiovascular health. The link between HA on long-term cardiovascular health is ambiguous, but there is epidemiological data and studies in nonhuman primates that support the hypothesis that even mild ovulatory abnormalities in young women can accelerate development of coronary artery disease.7,8
The link between energy balance and fertility has long been recognised. In the 17th century, Richard Morten observed that amenorrhoea was a cardinal feature of the condition, which was later termed anorexia nervosa (AN). Furthermore in the 1960s, Kennedy and Mitra postulated that a critical body weight is required for reproductive function. 9 This permissive action of energy availability on fertility may represent an adaptive response to inhibit the energetic expense of reproduction during prevailing conditions of poor nutrition. A relative calorie deficiency can suppress the HPO axis, such that LH pulsatility is disrupted at a threshold of negative energy availability. 10 There is conflicting evidence as to whether low body fat is a cause of amenorrhoea when it falls below a certain threshold.11,12 Menstrual irregularities are common in women who undertake intense exercise (e.g. athletes or ballerinas).13,14 Restrictive eating and strenuous exercise are independent risk factors for HA, but are often seen concurrently, with or without a formal diagnosis of an eating disorder. The ‘female athlete triad’ refers to the interplay between energy availability, menstrual function and bone density; women who exercise frequently tend to have a relative caloric deficiency, menstrual irregularity or HA and reduced BMD, making them more prone to fractures, particularly stress fractures. Importantly, women with the female athlete triad may be of low or normal weight, but those with <85% ideal body weight have been shown to be approximately four times more likely to have menstrual dysfunction and low bone density. 13
Stress is another powerful inhibitor of reproductive function. Psychosocial stressors, including externally imposed stress, dysfunctional attitudes and psychiatric morbidity activate the hypothalamic–pituitary–adrenal (HPA) axis, increase corticotrophin-releasing hormone (CRH) and cortisol levels, and sequentially inhibit GnRH secretion.15–17 Administration of CRH has been shown to inhibit gonadotrophin release in healthy female volunteers 18 and monkeys. 19 Conversely administration of a CRH antagonist stimulates release of GnRH, 20 and advances the onset of puberty in rats. 21 Furthermore, it has been shown in monkeys that seemingly minor stressors that alone would have minimal impact on reproductive function can interact synergistically, such that combinations of stressors cause a greater impairment of the reproductive axis than any single stressor alone. 22 There is also evidence that women’s preconception stress, as measured by salivary alpha-amylase, is associated with a longer time-to-pregnancy and an increased risk of infertility. 23
Other less common, but well recognised, causes of FHA include chronic disease, malabsorptive illnesses such as coeliac disease and hypermetabolic states such as severe burns or hyperthyroidism. 24
There is considerable inter-person variability in the degree of weight loss, exercise or stress required to result in menstrual disturbance or HA, which is why there are some athletes who are able to conceive despite gruelling training regimes, 25 while other women may miss periods secondary to seemingly low levels of nutritional or mental disruption. It is known that a number of genetic mutations can lead to HA in homozygous individuals, such as in KAL1, FGFR1, PROKR2 and GNRHR; in women particularly sensitive to menstrual disturbance many have been shown to be heterozygous for these mutations. 2 Similarly, it may be hypothesised that some women may have protective genetic mutations, which enable continuation of fertility despite stressors such as strenuous exercise or weight loss.
The processes by which GnRH is suppressed by causative agents such as weight loss, exercise or stress are multifactorial, as there are many neuromodulatory signals that alter hypothalamic GnRH function, both inhibitory and stimulatory. The HPO axis and the HPA axis are tightly linked, with the HPA axis activated by nutritional or other stress-reducing GnRH secretion and subsequent LH pulsatility from the pituitary gland. 26 GnRH may be suppressed by the common hormonal abnormalities that are associated with FHA including decreased insulin-like growth factor 1 (IGF-1), 27 increased cortisol,28,29 increased ghrelin,30,31 decreased thyroid hormone levels, especially triiodothyronine, and reduced leptin 32 (Figure 1). Kisspeptin signalling has been implicated as the common intermediate signalling factor, acting downstream of leptin and other neuromodulatory signalling systems to modulate activity of GnRH. 33
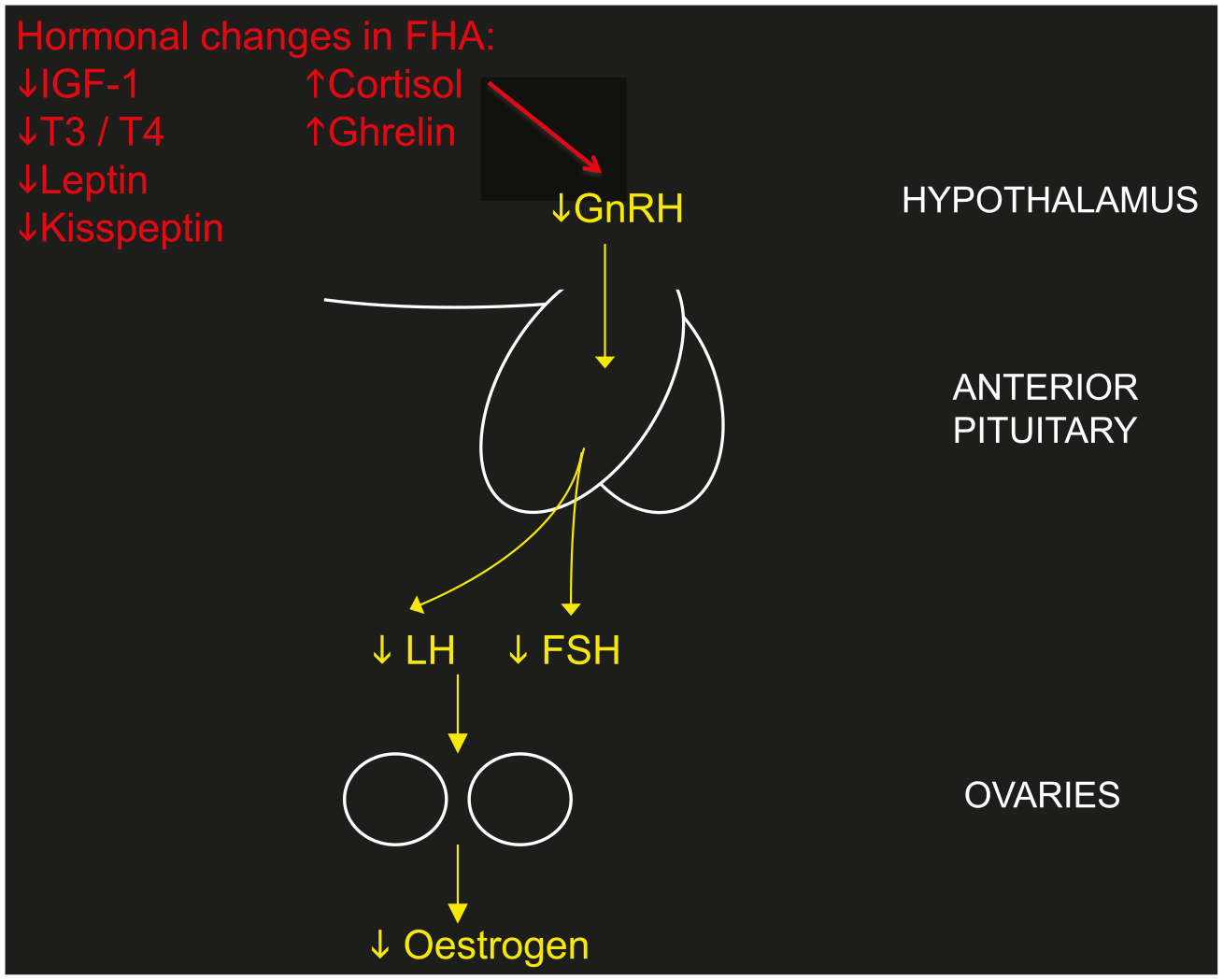
The effect of hormonal abnormalities associated with FHA on suppressing the hypothalamic–pituitary–ovarian axis.
Clinical assessment
Diagnosis of HA is based on symptoms of amenorrhoea, biochemical findings of low oestradiol (<50 ng/ml) with normal/low gonadotrophins (LH and FSH both <10 IU/L with a ratio ~1), 32 and, usually, evidence of a causative factor. HA is a diagnosis of exclusion, and other important causes of amenorrhoea must be ruled out. 34 These include polycystic ovarian syndrome (PCOS), premature ovarian insufficiency (which may have a genetic cause, such as Turner’s syndrome), uterine abnormalities (congenital, Asherman’s syndrome), endocrine disorders (thyroid dysfunction, Cushing’s syndrome), hyperprolactinaemia, Sheehan’s syndrome (hypopituitarism secondary to major obstetric haemorrhage) and pituitary tumours. The input of a multidisciplinary team including gynaecologists, fertility specialists and endocrinologists may be required to reach a diagnosis. Women with FHA usually present with menstrual disturbance, infertility, symptoms of the cause of FHA such as stress, anxiety, weight loss or an eating disorder or, more rarely, with a consequence of FHA such as fractures or sexual dysfunction. Some cases of FHA are masked by use of hormonal contraception, for example, the oral contraceptive pill (OCP), Depo-Provera, implant or Mirena intrauterine system, and only become clinically apparent once contraception is ceased. A detailed history is arguably the most powerful diagnostic tool in determining the underlying cause of amenorrhoea. Sensitive, but thorough questioning regarding eating patterns and exercise is crucial. It is also important to explore potential stressors, such as work- or study-related stress or personal stress, in addition to psychiatric disorders such as anxiety and depression. Use of a validated questionnaire, such as the Perceived Stress Scale, 35 may be helpful in facilitating these conversations, although there is a lack of validated questionnaires specifically designed to elucidate eating and exercise patterns in FHA. Thorough clinical examination is useful. It may help point to a diagnosis of HA, with signs of AN, for example, or provide diagnostic information for other causes of menstrual disturbance (e.g. hirsutism, acne or physical characteristics of Turner’s syndrome). Height and weight should be used to calculate body mass index (BMI) and, if available, it is helpful to measure body fat percentage, using the bioelectrical impedance method, as some women who exercise strenuously or maintain a restrictive diet can have an abnormally low body fat percentage, in spite of a normal BMI, which is in itself associated with ovulatory dysfunction and amenorrhoea. 14
Subjects with HA have normal/low circulating gonadotrophins and low oestradiol levels. This reproductive hormone profile may be within the normal range for the follicular phase of the menstrual cycle and therefore needs to be interpreted by someone aware of the clinical history. The endometrial lining may be thin on transvaginal ultrasound scan, but may be normal. In a healthy premenopausal woman, the endometrial lining normally progressively thickens during the follicular phase of the menstrual cycle. It is thinnest during menstruation, with a peak thickness of up to 10 mm in the late follicular phase.36,37 In women with HA, this variability in endometrial thickness may not be observed and there is evidence to suggest that if the lining is <1.5 mm, the patient is more likely to be hypo-oestrogenic. 38 HA and PCOS are the two most common causes of secondary amenorrhoea, 39 other than pregnancy. Some women with HA may have a coexistent history of symptoms associated with PCOS, such as oligomenorrhoea, hirsutism and acne. 40 Up to 50% of women with a nonhyperandrogenic PCOS phenotype may have FHA. 41 Transvaginal ultrasound scan may therefore reveal either normal ovarian appearance or morphologically polycystic ovaries.
In patients with amenorrhoea lasting for over 6 months, or in those who have additional risk factors for low BMD, such as severe nutritional deficiency or an eating disorder, a dual-energy X-ray absorptiometry scan is advisable to indicate baseline BMD and to help guide and monitor treatment. 39
A prolonged hypogonadal state during a woman’s reproductive years has potentially wide-ranging negative impacts on health. Amenorrhoea has obvious reproductive consequences by causing infertility, but the long-term effects of oestrogen deficiency extend beyond reproduction. A longitudinal study investigating the effects of amenorrhoea and amenorrhoea plus exercise on BMD of young women over 2 years found that low BMD occurs in young women with amenorrhoea and delayed menarche, regardless of exercise status, and compromises crucial bone mass accretion. 42 Women with FHA experience more sexual function problems (caused by issues such as dyspareunia and low libido) and significantly higher depression and anxiety compared with women without menstrual dysfunction. 43 Furthermore, women with FHA have potential increases in cardiovascular disease 6 and exhibit impaired endothelial function, which may contribute to impaired vascular function. 44
Treatment
Fortunately, FHA is generally reversible, and usually resolves over a period of time after a positive energy balance is restored, or the underlying stress resolves; 45 however, this may take many months. A study evaluating the prognosis of FHA showed that 71% of patients recovered over a follow-up period of 7–9 years, and found that predictive factors of recovery included a higher basal BMI and lower serum cortisol values. 46 There is also evidence that in women who recover from FHA serum oestradiol levels gradually increase before recovery, which is preceded by the changes in plasma cortisol concentration. 47
Therefore the most successful treatment tends to focus on alleviating the underlying cause of FHA. It is important, however, that the subgroup of patients who have severe energy deficit, associated with severe bradycardia, hypotension, orthostasis and/or electrolyte imbalance are recognised and assessed for inpatient medical management. 48 As FHA is often caused by a combination of factors including low weight, excessive exercise, poor nutritional intake and stress, a multidisciplinary approach is beneficial. Table 1 summarises the current treatment options for FHA.
Current treatment options for FHA.

FHA, Functional hypothalamic amenorrhoea; SSRI, selective serotonin reuptake inhibitor.
Lifestyle changes
Reversing the negative energy balance by restoration of body weight or fat mass and/or reduction in exercise intensity may be sufficient to restore menses and improve rates of conception in some patients with FHA. 49 It is not clear what degree of weight gain is required for resolution of menstruation, but common advice is to aim for at least the same weight at which point menstruation stopped, although one study has shown that patients with low-weight eating disorders were 2 kg heavier at the time their menses resumed than when they became amenorrhoeic. 57 Improving the energy deficit often requires behavioural change. In some women simply explaining the need for increased caloric intake and basic advice about how to achieve this may be adequate, whilst in others weight gain may need to be supervised, or dietary patterns discussed by a registered dietician or nutritionist. Many women with FHA have an element of disordered eating or an incipient eating disorder50,58–62 that will require psychological support in order to facilitate change in negative eating habits. In those with a formally diagnosed eating disorder, such as AN or bulimia nervosa, referral to a specialist eating disorder service is recommended to enable these patients to be appropriately treated by a multidisciplinary team, including psychiatrists.
Psychological stress is a known risk factor for the development of FHA, and whilst this may be caused by a definable stressful life event, such as bereavement, it is more commonly secondary to insidious psychological or personality characteristics, which are often associated with disordered eating. Women with FHA have been shown to have more dysfunctional attitudes (demonstrated by higher levels of control, perfectionism, rigidity of ideas and concern about judgements of others), greater difficulty in coping with daily stresses and greater interpersonal dependence than eumenorrhoeic women. 15 In addition, women with FHA more commonly have a history of psychiatric disorders and primary mood disorders than eumenorrhoeic women.16,17 Behavioural and psychological interventions, such as cognitive behavioural therapy (CBT), have been shown to reverse amenorrhoea, 50 associated with a reduction in nocturnal cortisol secretion and increased thyroid-stimulating hormone and leptin levels, independently of weight gain.62,63 In a study of 16 women with FHA, CBT resulted in a higher rate of resumption of ovarian function (88%) compared with observation alone (25%). 50 Family-based therapy has been shown to be beneficial in the treatment of eating disorders, but has been less well described for the specific treatment of FHA. Pharmacotherapy may be considered in women to treat psychological or psychiatric morbidity, such as anxiety or depression, which can be associated with FHA, either alongside behavioural therapies, or in those where behavioural therapies have been unsuccessful. For couples wishing to conceive, the diagnosis, evaluation and treatment of infertility can be profoundly stressful, with one study finding 40% of infertility patients fulfilling the diagnosis of a psychiatric disorder, most commonly anxiety disorders and depressive disorders. 64 Stress may negatively impact the success of fertility treatment, 65 as well as contribute to the discontinuation of fertility treatment before pregnancy is achieved, 66 and therefore it is essential that it is recognised. It has been found that psychosocial interventions for couples during infertility treatment, in particular CBT, may be effective both in reducing psychological distress and in improving clinical pregnancy rates. 67
Hormonal treatment
Hormone replacement therapy may be appropriate for women with FHA without menstrual recovery despite 6–12 months of nonpharmacological therapy, or in those declining behavioural or psychological treatment. Progesterone replacement is required in addition to oestrogen in order to prevent endometrial hyperplasia. Hormone replacement therapy may be administered either transdermally or orally. Whilst hormone replacement therapy provides oestrogen replacement in patients with FHA, it does not restore gonadotrophin release or stimulate ovulation, and may offer the false reassurance of regular menses despite ongoing nutritional deficiency, energy deficit or psychological stress. Studies looking at the benefit of oestrogen replacement on BMD, specifically in FHA, are lacking, and it remains unclear what the optimal preparation and optimal dose of oestrogen replacement is in these women. In other models of hypogonadism, such as Turner’s syndrome, oral oestradiol has been effectively used as hormone replacement therapy for many years. 68 However, these women are generally of normal weight and therefore it may be more helpful to compare women with FHA to those with a low-weight form of hypogonadism, such as AN. In AN it has been shown that administration of the oral contraceptive pill (OCP), providing relatively high oestrogen doses (usually ethinyloestradiol), does not improve BMD.51,69,70 In contrast, physiological transdermal oestradiol replacement may have a more positive effect in maintaining BMD. 52 A potential reason for this discrepancy may be that OCPs further suppress IGF-1, an important bone trophic hormone, which is already decreased in this condition.71,72 It is plausible that OCP preparations containing the endogenous hormone oestradiol might increase BMD more effectively in women with FHA when compared with an ethinyloestradiol-containing OCP preparation. The evidence for the effectiveness of hormone replacement on BMD in exercise-associated FHA is mixed.73–77
Nonhormonal treatment
To date, there is no clear role for nonhormonal treatment in the management of FHA. Administration of naltrexone, an opioid receptor antagonist, has been shown to improve hormonal status and restore menses in HA 78 and a more recent study has shown that administration of neuroactive compound acetyl-L-carnitine in combination with L-carnitine may have a positive effect on increasing LH levels in FHA. 79 However, more work needs to be carried out to confirm these findings.
Treatment of infertility
Hormonal treatment, with the intention to stimulate ovulation, is only clinically indicated when pregnancy is desired. It is crucial that fertility treatment is not initiated until attempts have been made to treat the underlying nutritional or psychological stress, and women have achieved, and maintained, a BMI of at least 18.5 kg/m2 in order to prevent the increased likelihood of poor obstetric and neonatal outcomes associated with low maternal weight, 80 including pregnancy loss, preterm labour, 81 low birth weight 82 and need for caesarean section. 83 Clomiphene citrate is a selective oestrogen receptor modulator and has mixed agonist and antagonist activity at oestrogen receptors at the level of the hypothalamus. 84 By interfering with the oestradiol-mediated negative feedback on pituitary gonadotrophin release, clomiphene citrate increases circulating gonadotrophin levels, which stimulate ovarian folliculogenesis, leading to development of a dominant follicle and ovulation. However, clomiphene has limited efficacy in FHA since circulating levels of oestradiol are characteristically low in this form of hypogonadotrophic hypogonadism. Pulsatile GnRH therapy is an effective method of restoring menstrual cyclicity in patients with HA and has the advantage of driving the development of a single dominant follicle and therefore minimal risk of multiple pregnancy. 85 However, there is currently no commercially available pump internationally. The predominant therapy used to induce ovulation in patients with HA is exogenous gonadotrophins. 53 Daily FSH-containing gonadotrophin injections are administered to the patient, usually following a step-up protocol. Women with FHA are deficient in both FSH and LH and successful ovulation induction requires some exogenous LH, which is crucial for androgen steroidogenesis (substrate for oestrogen biosynthesis), alongside FSH. Preparations such as highly purified human menopausal gonadotrophin provide sufficient LH. Alternatively, if recombinant FSH is used, recombinant LH should be administered concurrently. Follicle tracking is performed using ultrasonography, and ovulation is induced using human chorionic gonadotrophin when the follicle is over 18 mm in diameter. Ovulation induction can be used in combination with timed intercourse or intrauterine insemination to achieve pregnancy, although the latter is usually reserved for those unable to have vaginal intercourse or requiring donor sperm. While gonadotrophin-based therapies are efficacious, they confer the risk of multiple pregnancy due to ovarian over-response and as a result cycle cancellation rates can be as high as 25%. 86 Ovarian hyperstimulation syndrome (OHSS) occurs in a minority of cases of ovulation induction, 87 but is much more prevalent with the controlled ovarian hyperstimulation protocols used for IVF. OHSS is a potentially life-threatening condition, which results from increased vascular permeability, subsequent fluid accumulation in the peritoneal and pleural spaces, renal and hepatic failure and a prothrombotic state leading to an increased risk of venous thromboembolism as a direct consequence of the pharmacological circulating gonadotrophin levels associated with therapeutic injections.
Experimental avenues of treatment
Leptin is an adipokine hormone secreted in proportion to fat mass. Circulating leptin levels positively correlate with fat mass, and levels of leptin secretion are significantly reduced following weight loss 88 and acute starvation. 89 Furthermore, patients with genetic leptin deficiency have hypogonadotrophic hypogonadism. 90 Research has implicated recombinant leptin as a potential therapy in FHA. FHA is commonly associated with low body weight or weight loss, and subjects with HA have reduced mean circulating levels of leptin when compared with healthy female subjects. Two randomised control trials have demonstrated the potential efficacy of leptin treatment in FHA. Administration of twice daily recombinant leptin in women with FHA resulted in ovulatory menstrual cycles in 38% of women, restored LH pulsatility and significantly increased levels of oestradiol, IGF-1, thyroid hormone and bone-formation markers. 54 A second study has shown that 70% of women receiving recombinant leptin therapy developed menstruation during the course of the study and significantly increased levels of oestradiol and progesterone. 55 These data suggest that activity of the GnRH pulse generator is stimulated in subjects with HA following leptin administration. Interestingly, GnRH neurons do not express the leptin receptor; it is likely that kisspeptin acts as an intermediate signalling factor to mediate the stimulatory action of leptin on GnRH pulsatility. 91 Subcutaneous bolus injection of kisspeptin-54 stimulates gonadotrophin secretion in healthy female subjects92,93 and acute subcutaneous administration of kisspeptin-54 potently stimulates pituitary–gonadal function in human females with HA. 56 However, significantly reduced gonadotrophin responses to kisspeptin-54 administration were observed after 2 weeks of twice-daily kisspeptin-54 injections, suggesting desensitisation. 94 The most promising role for kisspeptin as a therapeutic option in FHA comes from the use of a continuous infusion of kisspeptin at variable doses over 10 hours, which was associated with an increase in LH pulsatility in all women, without evidence of desensitisation. 95
Oestrogens are required for pituitary responsiveness to GnRH. A recent study observed that a 10-day course of oral oestriol significantly increased LH and FSH secretion following GnRH bolus in women with FHA. 96 It is possible that physiological hormone replacement therapy could provoke ovulation in women with FHA bordering on recovery. However, there is a paucity of data directly comparing ovulatory frequency in women with FHA taking hormone replacement therapy versus women with FHA not taking hormone replacement therapy.
Conclusion
HA is a common cause of amenorrhoea in women of reproductive age, which can go unrecognised. Thorough clinical evaluation is crucial in order to diagnose these women, establish the causative factor and initiate treatment appropriately. Treatment options need to be personalised and tend to focus on alleviating the underlying nutritional or psychosocial stress by lifestyle and behavioural interventions. Emerging hormonal therapies may prove useful in the future, especially in those women who do not respond to first-line behavioural treatment.
Footnotes
Author contribution(s)
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.