
Abstract
Objective
This study aimed to examine the effect of interactions between serotonin (5-HT), brain-derived neurotrophic factor (BDNF), and kisspeptin on the reproductive potential in women receiving in vitro fertilization (IVF).
Methods
Paired serum and follicular fluid (FF) samples were obtained from 30 consecutive patients receiving IVF. Primary and secondary outcome measures were the rate of chemical/clinical pregnancy and the number of mature oocytes and embryos, respectively. Serum and FF 5-HT, BDNF, kisspeptin, and platelet-activating factor (PAF) levels were measured by enzyme-linked immunosorbent assay.
Results
In response to ovarian hyperstimulation, serum 5-HT and kisspeptin levels significantly increased, whereas serum BDNF and PAF levels remained unchanged. These factors were detected in FF, but they were unrelated to serum levels. FF 5-HT and BDNF levels were positively correlated. Serum kisspeptin levels were negatively correlated with FF BDNF and serum and FF PAF levels. Women who were pregnant had significantly lower FF BDNF levels compared with women who were not pregnant (21.96±12.75 vs 47.63±52.90 µg/mL). Multivariate stepwise linear regression and logistic regression analyses showed that only 5-HT and kisspeptin improved IVF outcome.
Conclusions
This study indicates a role of serotoninergic mechanisms in success of IVF, but the contribution of interacting neuropeptides requires additional investigation.
Keywords
Introduction
Serotonin (5-HT) regulates the hypothalamic–pituitary–gonadal axis and 5-HT is involved in female reproduction. Previous studies have shown that 5-HT axons terminate on gonadotropin-releasing hormone (GnRH) neurons in the hypothalamus 1 and 5-HT regulates GnRH gene expression and GnRH secretion2,3 by activating specific 5-HT receptors. GnRH then acts on pituitary gonadotropins to stimulate the synthesis and release of follicle-stimulating hormone (FSH) and luteinizing hormone (LH).4,5 FSH and LH are responsible for controlling steroidogenesis, folliculogenesis, and oogenesis in female ovaries.4,5 Along with their crucial role in the control of reproductive function, hypothalamic neuropeptides and neurotransmitters are intimately involved in the regulation of energy homeostasis, and emotional and feeding behaviour.6–9
Approximately 4% of patients with IVF take a selective serotonin reuptake inhibitor (SSRI). 10 The use of SSRIs before or during pregnancy is associated with reduced infertility treatment efficiency and an adverse pregnancy outcome.11,12 Although the mechanisms of unfavorable actions of SSRIs on reproductive outcome have not been clearly established, 5-HT or elements of the 5-HT pathway appear to be implicated. In addition to serotoninergic regulation of ovarian function at the hypothalamic level, direct involvement of 5-HT in intraovarian regulation has also been shown. Previous studies showed that 5-HT was detected in follicular fluid (FF) and it stimulated progesterone production in bovine luteal cells13,14 and in human granulosa cells. 15 Further evidence for the involvement of 5-HT in the reproductive process is indicated by the complex interrelationship between 5-HT and neuropeptides (brain-derived neurotrophic factor [BDNF], kisspeptin).16–19 These neuropeptides play an important role in hypothalamic or intraovarian regulation of reproduction.
The present study was performed to examine the function of the neuroendocrine–reproductive axis in women undergoing IVF treatment. This study aimed to (1) investigate the response patterns of 5-HT, BDNF, and kisspeptin to ovarian hyperstimulation, (2) to assess the relationship between serum and FF levels of these hormones, (3) to determine whether changes, if any, in these hormone levels are related to platelet activation or they are independent of platelets, and (4) to establish the effects of 5-HT, BDNF, and kisspeptin individually or in combination on reproductive performance.
Methods
Patients
This cross-sectional, observational, clinical study was carried out between 1 September 2016 and 1 December 2016 in the Assisted Reproduction Unit, Department of Obstetrics and Gynaecology, University of Pécs, Pécs, Hungary. The STROBE guideline for cross-sectional studies was used to ensure the reporting of this study. 20 The study comprised 30 consecutive patients who were indicated for fertility treatment (IVF). Eligible patients were recruited according to the date of the fertility consultation. They did not have metabolic or vascular diseases (obesity, diabetes mellitus, metabolic syndrome, fatty liver disease, and atherosclerosis), or psychiatric drug therapy. Enrolment of patients into the IVF procedure was approved by two independent physicians. 21 Superovulation treatment, fertilization methods, and embryo selection were performed according to standard protocols as described in our previous publication. 22
Collection of blood serum and FF
Blood samples were obtained from the patients before the stimulated cycle on the 21st day of their menstrual cycle and in the morning of follicle puncture, before sedation. The collected FF was centrifuged for 10 minutes at 252 × g. The supernatants were frozen and stored at −80°C for future analysis.
Laboratory measurements
Hormone measurements were performed using commercially available enzyme-linked immunosorbent assay kits. Kits for 5-HT were produced by IBL International GmbH (Hamburg, Germany). The intra- and interassay coefficients of variation (CVs) for 5-HT were 3.8% to 6.6% and 9.4% to 18.1%, respectively, with a detection limit of 2.68 ng/mL. BDNF Human kits were used (RayBiotech, Peachtree Corners, GA, USA) with intra- and interassay CVs of <10% and <12%, respectively, and a detection limit of 80 pg/mL. Kisspeptin 54 Human kits were provided by Peninsula Laboratories International (San Carlos, CA, USA). The intra- and interassay CVs of kisspeptin were <10% and <15%, respectively, with a detection limit of 3 ng/mL. For human PAF kits (Abbexa Ltd, Cambridge, UK), the intra- and interassay CVs were <10% and <12%, respectively, with a detection limit of 50 pg/mL.
Ethical approval and consent to participate
The study was reviewed and approved by the Human Reproduction Committee of the Hungarian Medical Research Council (5273-2/2012/EHR). Signed informed consent was obtained from all patients who participated in the study. The investigation conforms to the principles outlined in the Declaration of Helsinki.
Statistical analysis
Statistical analyses were performed using IBM SPSS 22.0 software (IBM Corp., Armonk, NY, USA). Normality of data distribution was tested by the Kolmogorov–Smirnov test. Depending on distribution, either the Student’s t-test or Mann–Whitney U-test was used to compare continuous variables. The association between two continuous variables was tested by using Spearman’s or Pearson’s correlation coefficients. Multiple linear or logistic regression models were used to identify the variables independently associated with IVF outcome parameters (number of oocytes, number of embryos, chemical/clinical pregnancy). Data are expressed as mean ± standard deviation and p < 0.05 was considered statistically significant.
Results
Clinical characteristics of the patients
The clinical parameters of the patients are shown in Table 1. The patients had the following main diagnoses of infertility: male factors, damaged or blocked Fallopian tubes, other female factors, combined male and female factors, severe endometriosis, and unexplained infertility.
Clinical characteristics of the patients.

Numbers in bold indicate significance. hCG=human chorionic gonadotropin.
Evaluation of serum and FF hormone levels during IVF
In response to ovarian hyperstimulation, there was a significant increase in serum 5-HT and kisspeptin levels (p<0.01), whereas serum BDNF and PAF levels remained unchanged (Table 2). FF 5-HT and BDNF levels were markedly low, while those of kisspeptin and PAF were similar to their serum levels. When patients with (n = 7) and without (n = 23) clinical pregnancies were compared, ovarian hyperstimulation did not result in significant differences in either serum or FF levels of 5-HT and kisspeptin. However, pregnant patients had significantly lower FF BDNF levels compared with patients who were not pregnant (p = 0.026). Additionally, serum and FF PAF levels appeared to be reduced in pregnant patients, but this did not reach statistical significance.
Serum and follicular fluid hormone levels during in vitro fertilization.
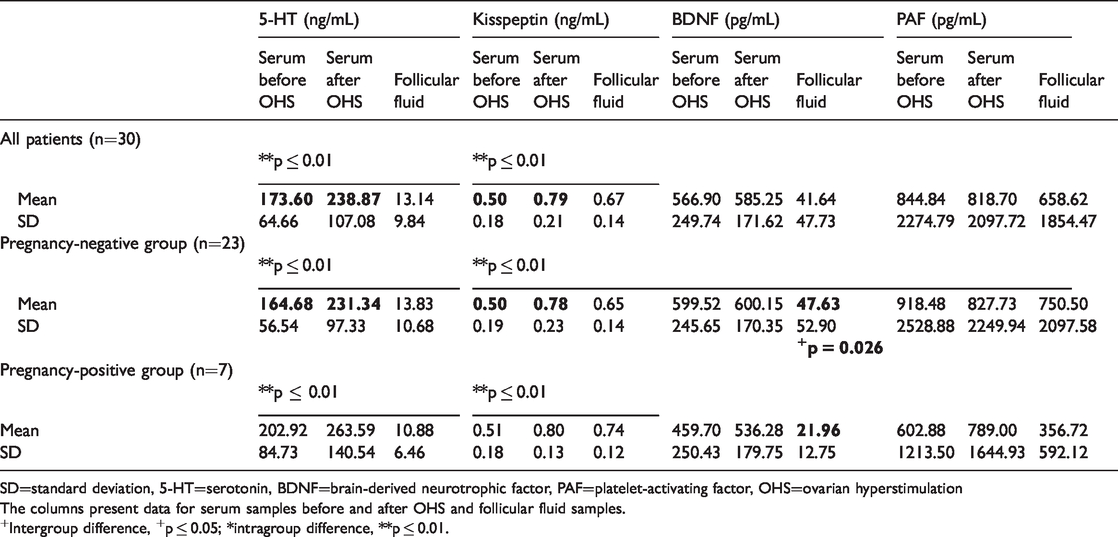
SD=standard deviation, 5-HT=serotonin, BDNF=brain-derived neurotrophic factor, PAF=platelet-activating factor, OHS=ovarian hyperstimulation
The columns present data for serum samples before and after OHS and follicular fluid samples.
+Intergroup difference, +p ≤ 0.05; *intragroup difference, **p ≤ 0.01.
Correlations between serum and FF hormone levels during IVF
To examine the possible contribution of circulating serum to FF hormone levels, we investigated the relationship between individual hormone levels that were measured simultaneously in serum and FF. Interestingly, there were no correlations between serum and FF levels of 5-HT, kisspeptin, BDNF, and PAF. Even when the patients of the pregnant group were analyzed separately, there were no significant associations between FF and serum hormone levels.
Univariate linear regression analysis of hormonal interactions showed a significant positive correlation between FF BDNF and 5-HT levels (R = 0.377, p = 0.040), but FF BDNF levels were inversely related to serum kisspeptin levels (R = −0.42, p = 0.022). Serum and FF PAF levels were negatively related to FF kisspeptin levels (R = −0.45, p = 0.013 and R = −0.43, p = 0.018, respectively) (Table 3).
Correlation between serum and follicular fluid hormone levels during in vitro fertilization (n=30).

Numbers in bold indicate significance. 5-HT=serotonin, BDNF=brain-derived neurotrophic factor, PAF=platelet-activating factor, OHS=ovarian hyperstimulation, R=correlation coefficient.
Table 4 shows the association between some selected clinical/laboratory variables and hormone levels that we measured in this study. We found that 5-HT levels were negatively affected by the age of the patients (R = −0.371, p = 0.043) and estradiol levels (R = −0.388, p = 0.041), and positively affected by the number of IVF cycles (R = 0.379, p = 0.043). Serum or FF BDNF levels were directly related to the number of IVF cycles (R = 0.469, p = 0.010) and FSH dosage (R = 0.362, p = 0.049). However, kisspeptin and PAF were independent of these variables.
Clinical and laboratory parameters affecting plasma and follicular fluid hormone levels during in vitro fertilization (n=30).

Numbers in bold indicate significance. 5-HT=serotonin, BDNF=brain-derived neurotrophic factor, PAF=platelet-activating factor, E2=estradiol, FSH=follicle-stimulating hormone, R=correlation coefficient.
Numbers 1, 2, and 3 designate serum samples before (1) and after ovarian hyperstimulation (2), and follicular fluid samples (3).
The effects of clinical and hormonal parameters on the outcome measures in our patients with IVF were also evaluated. The numbers of oocytes, matured oocytes, and embryos, as well as serum human chorionic gonadotropin (hCG) levels on day 12 and clinical pregnancy, were used as indices of outcome. We found that serum and FF BDNF levels significantly negatively affected these outcome measures (oocytes: R = −0.384, p = 0.038; mature oocytes: R = −0.432, p = 0.017; embryos: R = −0.384, p = 0.036). However, serum and FF 5-HT, kisspeptin, and PAF levels appeared to be independent of the outcome. Furthermore, there were significant negative associations of the FSH dosage for hyperstimulation with the number of mature oocytes (R = −0.422, p = 0.020), the number of embryos (R = −0.434, p = 0.017), and hCG levels on day 12 (R = −0.399, p = 0.032). Similarly, serum hCG levels were negatively related to maternal age (R = −0.388, p = 0.038) and to the number of IVF cycles (R = −0.402, p = 0.034). Serum estradiol levels and the patients’ body mass index did not affect the outcome measures (Table 5).
Hormonal and clinical parameters affecting reproductive potential during in vitro fertilization (n=30).

Numbers in bold indicate significance. 5-HT=serotonin, BDNF=brain-derived neurotrophic factor, PAF=platelet-activating factor, BMI=body mass index, E2=estradiol, FSH=follicle-stimulating hormone, hCG=human chorionic gonadotropin, R=correlation coefficient.
Numbers 1, 2, and 3 designate serum samples before (1) and after ovarian hyperstimulation (2), and follicular fluid samples (3).
Further evaluation of the results by using multivariate stepwise linear regression showed (Model 1, R2 = 0.336) that the number of oocytes, as the dependent variable, was significantly affected by post-stimulation serum 5-HT levels (β = 0.447, p = 0.015) and FF 5-HT levels (β = −0.433, p = 0.016), as well as by the hyperstimulation-induced increase in serum kisspeptin levels (Model 2, R2 = 0.159, β = 0.398, p = 0.029). When clinical pregnancy was considered as the dependent variable, multivariate logistic regression showed (Model 3, R2 = 0.595) significantly elevated serum 5-HT levels in pregnant women (β = 1.028, p = 0.047) and a tendency for a lower FSH dosage (β = 0.997, p = 0.076) compared with non-pregnant women.
Discussion
The present study showed that in patients undergoing IVF, serum 5-HT and kisspeptin levels were significantly increased in response to ovarian hyperstimulation, whereas BDNF and PAF levels remained unchanged. All of these hormones/factors were detected in FF, but FF levels were unrelated to serum levels. Furthermore, a significant positive correlation was found between FF 5-HT and BDNF levels, and serum kisspeptin levels were negatively correlated with FF BDNF and with serum and FF PAF levels. Importantly, multivariate stepwise linear regression and logistic regression analyses showed that only 5-HT and kisspeptin affected outcome measures (oocyte number, clinical pregnancy).
The role of 5-HT in human reproduction has received renewed interest because of widespread use of SSRIs in women of reproductive age.10–12,23,24 SSRI use is associated with the potential of reproductive failure. However, the neuroendocrine mechanism(s) of SSRI-induced reproductive dysfunction is not clearly defined.
Recent discoveries of the interactions of 5-HT and neuropeptides have allowed further insight into serotoninergic regulation of reproduction.19,25,26 A possible role of BDNF has been established. The brain is the major source of BDNF production, although several peripheral tissues, including vascular endothelium, smooth muscle cells, and activated mononuclear white blood cells, also contribute. Transport of BDNF is achieved by platelets, and in response to platelet activation, BDNF is released into the plasma together with 5-HT. Feedforward regulation has been demonstrated between BDNF and 5-HT release.27–30
With regard to BDNF and its receptor in reproduction, neurotrophic tyrosine kinase B (TrkB) has been detected in the ovaries and it is thought to modulate ovarian function. 31 The autocrine/paracrine BDNF/TrkB signaling system is required for folliculogenesis, oocyte maturation, implantation, and early embryo and placental development.16,17,32–34 In women undergoing IVF, circulating estradiol levels are positively associated with BDNF levels. 35 BDNF that is secreted by cumulus and granulosa cells is responsive to hCG, LH, and to a lesser extent, FSH stimulation.36,37 A recent study showed that serum BDNF levels before initiation of the IVF cycle predicted pregnancy outcome. 38 This study also showed that patients who became pregnant had significantly reduced BDNF levels compared with those who did not become pregnant. Our study showed a significant negative effect of BDNF levels on the number of oocytes and embryos and on the rate of chemical and clinical pregnancy. The significant association between FF 5-HT and FF BDNF levels can be regarded as evidence for an indirect contribution of BDNF to improvement of reproductive potential via stimulating 5-HT production. Interestingly, neither 5-HT nor BDNF levels were related to PAF levels, which suggested that their release was independent of platelet activation.
The hypothalamus-based kisspeptin/KISS IR signaling system is a major positive regulator of reproduction. 39 Kisspeptin and its receptors are expressed in the ovary and they are thought to be implicated in the regulation of follicular maturation, oocyte survival, embryo implantation, and placentation.18,40 Interestingly, ovarian-derived kisspeptin and BDNF are assumed to act together to promote oocyte survival, 19 and low neurotrophic receptor tyrosine kinase 2/KISS 1R signaling in oocytes causes premature ovarian failure. 41 In our clinical setting, FF kisspeptin levels were not correlated with FF BDNF, but 5-HT and kisspeptin levels had a beneficial effect on the number of oocytes and on the rate of clinical pregnancy. These findings are consistent with recent observations, which showed that kisspeptin-54 administration in a single dose or in repeated doses improved oocyte maturation by inducing a controlled LH surge in women at high risk of ovarian hyperstimulation syndrome.42,43
Study limitations
Only a limited number of patients with IVF were included in our study. Therefore we could not create homogenous subgroups according to the causes of infertility. Furthermore, only a few individual biomarkers were selected and measured in our study. Therefore, we were not able to examine the complex network of interrelated biologically active compounds relevant to the success of IVF. Further randomized, controlled studies with a larger sample size of patients with homogenous diagnoses need to be conducted to better define the concept of “brainwork in the ovary”. Moreover, a more reliable diagnostic test needs to be developed to assess the IVF success rate and to introduce more targeted therapy to improve efficiency of IVF.
Conclusions
In patients undergoing IVF, we evaluated serum and FF levels of 5-HT, kisspeptin, BDNF, and PAF. There is a positive correlation between FF BDNF and FF 5-HT levels, and inverse correlations between serum kisspeptin levels and FF BDNF and serum and FF PAF levels. Importantly, only 5-HT and kisspeptin affect outcome measures (oocyte number, clinical pregnancy). These observations suggesting that ovarian 5-HT, BDNF, and kisspeptin act in concert to improve reproductive potential need to be further substantiated in the future.
List of abbreviations
5-HT serotonin
BDNF brain-derived neurotrophic factor
BMI body-mass index
CV coefficient of variation
FF follicular fluid
FSH follicle-stimulating hormone
GnRH gonadotropin-releasing hormone
hCG human chorionic gonadotropin
IVF in vitro fertilization
LH luteinizing hormone
PAF platelet-activating factor
SSRI serotonin reuptake inhibitor
TrkB tyrosine kinase B
OHS ovarian hyperstimulation
Footnotes
Acknowledgements
We thank the women who underwent IVF treatment at the Assisted Reproduction Unit, Department of Obstetrics and Gynaecology, University of Pécs, for participating in our study.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by EFOP-3.6.3-VEKOP-16-2017-00009, Development of Scientific Workshops of Medical, Health Sciences and Pharmaceutical Educations. The funding source did not have any role in the study design; in collection, analysis and interpretation of data, or in writing and submitting this manuscript.