
Abstract
Background:
Human studies have demonstrated the beneficial effects of soy or isoflavones on bone metabolism. However, conflicting data remain. Equol is the intestinal metabolite of the isoflavone daidzein. The health benefits of soy are more pronounced in equol producers than those not producing equol. This 6-month randomized controlled trial aimed to examine the effect of whole soy (soy flour) and purified daidzein on bone turnover markers (BTMs) in Chinese postmenopausal women who are equol producers.
Methods:
A total of 270 eligible women were randomized to either one of the three isocaloric supplements as follows: 40 g soy flour (whole soy group), 40 g low-fat milk powder + 63 mg daidzein (daidzein group), or 40 g low-fat milk powder (placebo group) given as a solid beverage daily for 6 months. The following fasting venous samples were collected at the baseline and end of the trial to analyze BTMs: serum cross-linked C-telopeptides of type I collagen, bone-specific alkaline phosphatase, osteocalcin, procollagen type I N-terminal propeptide, and 25(OH)D3. Inflammation-related biomarkers, such as serum interleukin-6, tumor necrosis factor-alpha, C-reactive protein, transferrin, and homocysteine, were also tested to explore potential mechanisms.
Results:
A total of 253 subjects validly completed the study protocol. Urinary isoflavones suggested a good compliance to the treatments. Intention-to-treat and per-protocol analyses indicated no significant difference in the 6-month or percentage changes in the parameters of bone metabolism and inflammatory markers among the three treatment groups.
Conclusions:
Whole soy and purified daidzein at provided dosages exhibited no significant effect on the bone metabolism and inflammation levels among Chinese equol-producing postmenopausal women.
Trial registration:
ClinicalTrials.gov identifier NCT01270737.
Introduction
One out of three women aged over 50 years worldwide will experience osteoporotic fractures, and this number will increase to one out of two for women aged over 60 years. 1 More than 50% of osteoporotic hip fractures are projected to occur in Asia by 2050. 2 Postmenopausal estrogen loss accelerates osteoporosis, which could result in nearly 9 million fractures annually, worldwide. 3 The prevalence of osteoporosis in China also increased significantly over the past decade, affecting more than one third of adults aged 50 years and above. 4 The increasing number of fractures and their associated disability places a heavy burden on healthcare resources. Thus, effective strategies featuring public health implications are essential for the prevention of postmenopausal bone loss. Pharmacological agents for osteoporosis are often limited by potential side effects, thereby restricting their applicability, and resulting in poor adherence. Although hormone replacement therapy is effective for menopausal bone preservation, it may increase the risk of cardiovascular diseases (CVDs) and breast cancer. 5 Thus, there is considerable research interest in exploring natural food components, especially phytoestrogens, to improve postmenopausal bone health.
Soybean is a traditional Asian food containing a number of beneficial components for bone health. As an important phytoestrogen and potential alternative therapy for estrogen, 6 soy isoflavones have received considerable attention for their roles in maintaining postmenopausal bone health. Soy isoflavones comprise several subtypes, such as genistein, daidzein, and glycitein, which show structural similarity to endogenous 17β -estradiol. Several large-scale observational studies in postmenopausal women reported that high habitual soy food or isoflavone intake is associated with low prevalence of osteoporosis 7 and good bone mineral density (BMD). 8 Rat experiments also suggested that soy or isoflavones could prevent ovariectomy-induced bone loss by altering the receptor activator for the nuclear factor κB ligand/osteoprotegerin pathway (the key to the regulation of bone turnover), 9 thereby inhibiting inflammation, 10 increasing calcium absorption, 11 or inducing osteoclast apoptosis. 12 Daidzein and estradiol are equally effective, and perform better than genistein in the prevention of postmenopausal bone loss. 13
Clinical trials using soy foods or isoflavones have yielded mixed findings on bone. Most of the studies examined the effect of soy on BMD, whereas trials on bone metabolism markers are limited. Systematic reviews and meta-analyses also reported inconsistent findings on soy and bone mass.14–16 One possible reason could be the inadequate treatment duration, with several trials of less than 12 months, which resulted in the non-significant change in BMD due to the slow rate of the bone-mass remodeling process. By contrast, human trials have shown that treatment lasting less than 12 weeks can adequately exert a detectable effect on bone turnover markers (BTMs).17,18 One review reported that the daily ingestion of an average of 56 mg soy isoflavones for 10 weeks to 12 months can significantly decrease the bone resorption marker of deoxypyridinoline (DPD) by 18%. 19 However, a meta-regression indicated that the effect is unrelated to the isoflavone dosage and intervention duration. The available relevant randomized controlled trials (RCTs) on other bone biomarkers, except DPD, are limited.
Several reviews15,20 suggested that soy foods/isoflavones may exert beneficial effects on bone health in postmenopausal women who are equol producers. Clinical trials that were specifically conducted among equol producers are limited. Most of the findings were obtained from non-prespecified subgroups. Equol is the end product of daidzein, produced by intestinal bacteria; it shows superiority over other isoflavones in terms of estrogenic and antioxidant activities. Setchell and colleagues have hypothesized that equol production is the key to the clinical effectiveness of isoflavones, and equol producers may derive additional benefits from soy supplementation compared with non-producers. 21 Thus, daidzein is speculated to be bone protective in equol producers. At present, no RCT has been specifically conducted among equol-producing postmenopausal women. Daidzein is the second most abundant isoflavone in soy. Several animal models and cultured cells22,23 suggest that daidzein is more efficient than other phytoestrogens, but not all, in the promotion of bone formation or prevention of bone resorption. 24 The favorable effect of purified daidzein on bone has not been reported in human controlled trials.
Bone remodeling involves a series of highly regulated steps that depend on the interaction of two cell lineages, that is, the formation of new bone by osteoblasts and resorption of old bone by osteoclasts. The activities of both kinds of cells are triggered by hormonal and non-hormonal stimulations. 25 Bone densitometry cannot be used to detect early or small treatment effects. Quantitative changes in skeletal turnover can be assessed easily and non-invasively by the measurement of biochemical markers, although limitations still exist in using BTMs alone, in assessing therapies or predicting bone loss because no standardized assays nor optimal thresholds are available for evaluating the efficacy of several BTMs. Although human studies reported that equol producers could obtain more health benefits than non-producers 26 and whole soy foods (less processed soy products, that is, soy nuts, soy flour, soy milk, and tofu, etc.) exert more favorable effect than isolated soy components, 27 the enhanced effects were primarily observed on cardiovascular and lipid parameters. To date, limited research has compared the effects of whole soy with purified isoflavones on bone health in the context of the equol-producing status of participants. In the present study, we have observed a significant decrease in inflammatory marker [high-sensitivity C-reactive protein (hs-CRP)] and lipid levels by whole soy consumption. 28 Inflammation is a primary mediator of the accelerated bone loss at menopause, 29 and cardiovascular health strongly affects skeletal health. 30 Thus, whole soy or purified daidzein may feature a potential beneficial effect on bone metabolism, especially in equol producers.
Thus, on the basis of our established RCT, we proposed to test the effects of whole soy and isoflavone daidzein on bone turnover and inflammatory markers among equol-producing postmenopausal women. We hypothesized that whole soy or isocaloric-purified daidzein may reduce bone resorption or increase bone formation in equol-producing postmenopausal women, and the effect might be mediated by the interactions with inflammatory markers.
Methods
The study was a 6-month randomized, double-blind, placebo-controlled trial. This trial was conducted among 270 equol-producing postmenopausal women with either pre- or stage 1 hypertension, with the original aim of examining the effects of whole soy and isoflavone daidzein on cardiovascular health. We used the remaining serum samples stored in an ultra-freezer for the further analysis of bone remodeling and inflammatory markers.
Participants
The participants were recruited from local communities or health centers via advertisement in newspaper or referrals. The first eligible patient was enrolled in June 2011. The detailed recruitment has been published elsewhere. 31 In brief, the eligible participants were Chinese postmenopausal women aged 45–71 years, and equol producers, as determined by a standardized method based on the ratio of 24 h urinary equol and daidzein. The participants self-reported their menopausal status, that is, they ceased menstruation for at least 1 year. The participants were excluded if they had systolic blood pressure (SBP) ⩾160 mmHg or diastolic blood pressure (DBP) ⩾100 mmHg on average or both, used certain medications (e.g. hormone replacement therapy, or agents for antihypertension, hypoglycemia, or weight reduction) within the past 6 months, suffered from several metabolic disorders or malignancies, and had known soy/milk allergy. Written informed consent was obtained from each participant prior to enrolment. The institutional review boards of the Chinese University of Hong Kong (for primary outcomes) and Sun Yat-sen University (for outcomes on bone metabolism markers) approved the study protocol.
Sample size and study power
The sample size was estimated based on the primary outcome on the changes in SBP. The planned numbers were 270 and 90 for each intervention arm. Based on the current withdrawal rate of 6.3%, a two-sided 5% significance (type 1 error), and the standard deviation (SD) of the bone markers derived from our pilot tests and published reports on soy/isoflavone intervention,32,33 the post hoc power analysis suggested an 80% power for the detection of a 5.46 ng/ml change in procollagen type I N-terminal propeptide (PINP; 7.8%, SD = 5.5 ng/ml), 4.52 ng/ml change in osteocalcin (OC; 11.3%, SD = 2.4 ng/ml), and 0.44 ng/ml change in serum cross-linked C-telopeptides of type I collagen (CTX; 10.2%, SD = 0.23 ng/ml).
Randomization, intervention, and supplement preparation
Block randomization (random block sizes of 6, 9, and 12) was applied for participant assignment. A list of random numbers was computer generated, with each random number corresponding to one of the three possible interventions. A total of 270 serial numbers were labeled on the identical-looking boxes of the supplements by personnel who were not involved in the trial and assigned to eligible women in accordance with the sequence of their visits. All the research staff, technicians, and participants were blinded to the treatment allocation. The effectiveness of blinding has been reported in our published article, 31 and revealed a good blinding efficacy.
A total 270 women were randomized to either one of the three treatment groups: 40 g soy flour (whole soy group); 40 g low-fat milk powder + 63 mg daidzein (daidzein group); and 40 g low-fat milk powder (placebo group) daily, given as a solid beverage each day for 6 months. The three kinds of supplements featured similar colors, odors, and major nutrient profiles. The daily dosage of 40 g soy flour contained 12.8 g protein and 49.8 mg total isoflavones (23.2 mg daidzein and 19.4 mg genistein, expressed in aglycone equivalents). The products were tested prior to and after packaging to ensure content uniformity. The isoflavone concentrations were provided by the manufacturers and verified based on the supplements’ formula. The supplements were mixed with 300 ml water or beverages to partially replace breakfast or snacks. The women were required to discontinue their use of other dietary and herbal supplements (i.e. soy products, dietary fiber, minerals, vitamins C and E, fish oils, and flavonoids) during the run-in and intervention period. The participants were instructed to minimize soy food intake (⩽2 servings/week), refrain from salty diet, restrict alcohol intake to less than two drinks/week, and maintain their normal dietary habits and physical activities. Empty wrappers and uneaten sachets were required to be returned and counted by the study investigators for the estimation of intake percentage. Compliance with treatment was additionally assessed by food diaries at each clinical visit, 24 h urinary isoflavone excretion at baseline and at end of the trial.
Data collection
Biological samples were collected in a standardized procedure. Overnight fasting (10–12 h) venous blood samples and 24 h urine samples were collected at the baseline and after 6 months. Blood collection for participants with acute inflammation or taking anti-inflammation drugs (i.e. aspirin or antibiotics) was postponed 1 week after the cease of treatment. Serum was centrifuged at 3000g for 15 min at 4°C and isolated within 2 h post collection. Each participant’s serum samples were divided into several aliquots and stored at −85°C until analysis. All samples from each subject were run in the same assay or batch to avoid inter-assay variability. Structured questionnaire interview and anthropometric measurements were administered at baseline and at end of the trial.
BTMs and inflammatory markers
We tested the CTX for bone resorption marker and PINP, N-mid OC, and bone alkaline phosphatase (BALP) as bone formation markers. The coupling index 34 was calculated as the ratio of Z scores of resorption marker (CTX) and formation marker (PINP). We also tested serum 25 hydroxyvitamin D [25(OH)D3] and inflammatory markers, including interleukin-6 (IL-6), tumor necrosis factor-α (TNF-α), transferrin (TFR), and homocysteine (Hcy).
BTMs were measured on freshly thawed aliquots by a sole analyst who was blinded to clinical allocation. Except BALP, which was tested by Immunoassay Analyzer Access 2 (Beckman Coulter, Inc., Brea, CA, USA), the other serum BTMs were measured by electrochemiluminescent immunoassay using the Cobas 6000 analyzer (Roche Diagnostics, Auckland, New Zealand) following the manufacturer’s instructions. The inter- and intra-coefficients of variations (CVs) for β-CTX (Roche Diagnostics), PINP (Roche Diagnostics), OC (Roche Diagnostics), and 25(OH)D3 (Roche Diagnostics) were all less than 4%. Serum IL-6 (Siemens Healthineers, Erlangen, Germany) and TNF-α (Siemens Healthineers) were measured by electrochemiluminescent immunoassay on the Immulite 2000 Immunoassay System (Siemens Healthineers). Serum TFR (Roche Diagnostics) was measured by turbidimetric inhibition immunoassay on the Cobas 6000 analyzer. Serum Hcy (Jiu Qian Inc., Beijing, China) was measured by enzymatic method on an autoanalyzer (Hitachi 7180, Hitachi High-Tech Corporation, Tokyo, Japan). The intra- and inter-assay CVs for all inflammatory markers were all less than 10%.
Covariates
Individual information was collected by trained interviewers via face-to-face interview on the basis of a series of validated and structured questionnaires on sociodemographic data, years since menopause, medical history, medications, dietary habits, and physical activities. Dietary intakes over the intervention course were evaluated by 3-day food diaries, which were administered to participants at baseline and at end of trial. 31 Women received a 30 min training on the estimation of food amounts, portions, and utensil sizes. Dietary nutrients (energy, protein, total fat, calcium, and vitamin D) and soy isoflavones were calculated based on the Chinese Food Composition Table. Habitual physical activity was assessed by a modified Baecke questionnaire. 35 Urinary sodium, potassium, and creatinine (Hitachi 917 autoanalyzer, Roche Diagnostics) levels had been tested previously. Body weight, height, waist and hip circumferences, and blood pressures (BPs) were measured in accordance with standard protocols. Body fat percentage and fat-free mass were measured using a bioimpedance method (BIA, TBF-410-GS Tanita Body Composition Analyzer, Japan). Urinary isoflavones were tested by high-performance liquid chromatography. 31
Statistical analysis
Statistical analysis was performed by IBM SPSS 21.0 (IBM SPSS Statistics, IBM Corp., United States) statistics software. Two-tailed p <0.05 was considered statistically significant for all analyses. Skewed variables or variables with heterogeneity in variance were corrected by log transformation. The primary analysis was intention-to-treat analysis that included all 270 subjects who were randomized. The last value that was carried forward was used to process the missing data during follow up. A secondary per-protocol analysis was performed on 253 subjects showing good compliance. The major approach of analysis was one-way analysis of variance to compare the changes in biomarkers and their percentages after 6 months among the three groups. The Bonferroni test was used for post hoc multiple comparisons. We tested the effect of modification by adding interaction terms of intervention and subgroup variables to the univariate models. The subgroup variables included post-menopause years (<5 versus >5 years), baseline body mass index (BMI, <24 versus >24), and 25(OH)D level (<25 versus >25). Partial bivariate correlation was examined by Spearman’s correlation tests, with adjustment for menopausal years and total physical activities to examine the associations between the 6-month changes in bone biomarkers and inflammatory markers to explore the potential mechanisms.
Results
A total of 270 eligible women were randomized into three intervention arms, and 265 attended the final visit. There were only five participants required for last value carried forward method. Detailed study flow and reasons for withdrawals were reported previously. 31 Seventeen (6.3%) participants withdrew during the study course. No significant differences were observed in the dropout rates among the three study groups (p = 0.172). Baseline characteristics (Table 1) were similar among the three groups; these characteristics comprised age, menopausal year, BMI, education attainment, medical history of diabetes and CVDs, medications, dietary habits, and physical activity. No significant differences were noted in the baseline and follow-up dietary intakes among the three study groups (Table 2). The baseline values of the bone and inflammatory biomarkers were comparable among the three study groups. No significant differences were observed in the changes and percentage changes in all biomarkers within the three study groups from the baseline to 6 months (Tables 3 and 4). Additional analyses of the data, with the exclusion of women on lipid-lowering therapy (n = 6) or poor compliance (n = 17), showed minimal change in the results (data not shown).
Baseline characteristics of 270 Chinese postmenopausal women by the three study groups.

Data are presented as mean ± SD for continuous variables with comparison by one-way analysis of variance or number (%) for categorical variables, with comparison by Chi-square test. Regular drinking means habitual drinking of alcohol, tea, or coffee more than once per week. METs are multiples of resting metabolic rates and a MET-min is computed by multiplying the MET score of an activity by the minutes performed.
BS, baseline; DBP, diastolic blood pressure; HRT, hormone replacement treatment; PA, physical activity; SBP, systolic blood pressure; SD, standard deviation.
Dietary intakes at baseline and 6 months after treatment among the three study groups.
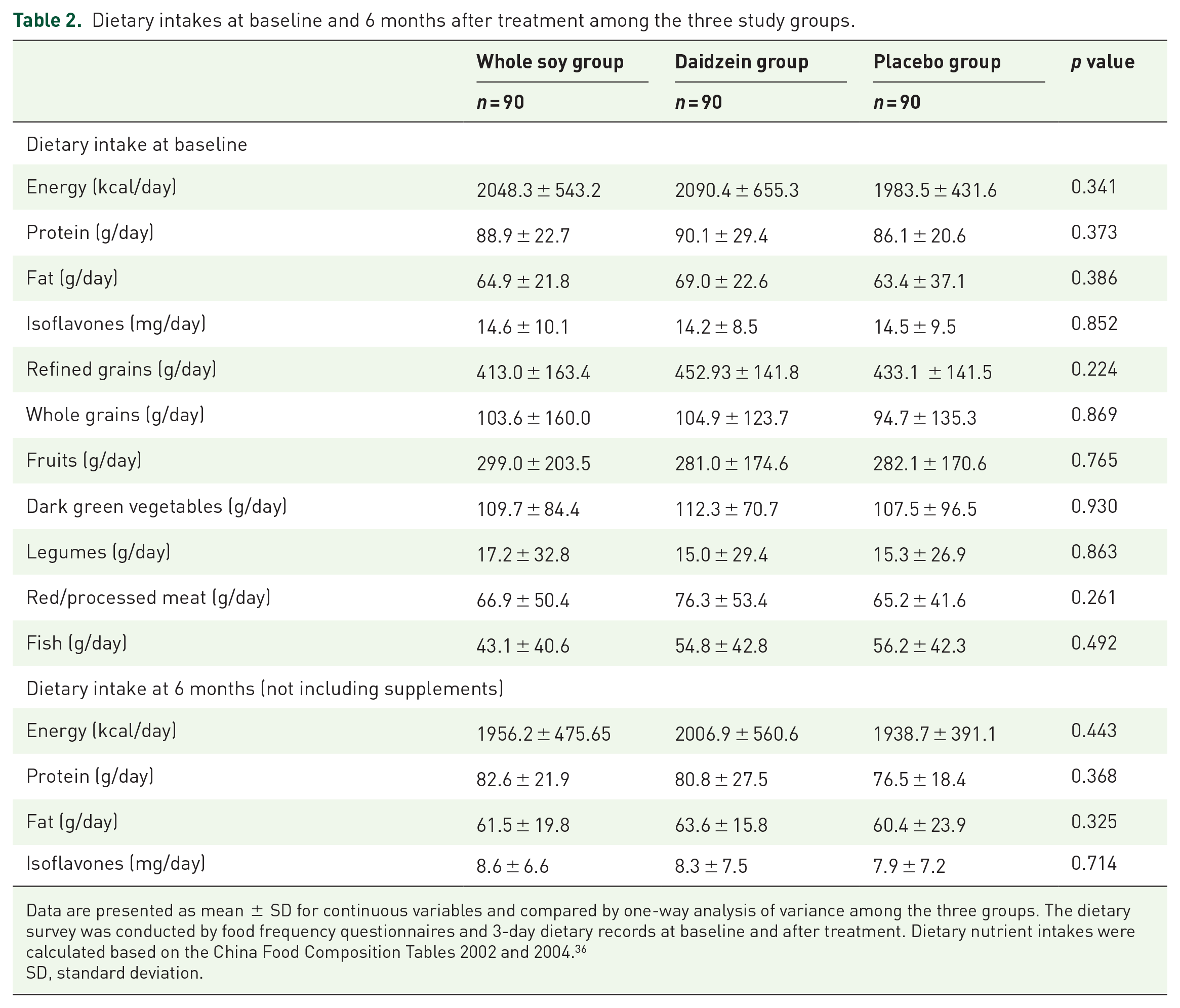
Data are presented as mean ± SD for continuous variables and compared by one-way analysis of variance among the three groups. The dietary survey was conducted by food frequency questionnaires and 3-day dietary records at baseline and after treatment. Dietary nutrient intakes were calculated based on the China Food Composition Tables 2002 and 2004. 36
SD, standard deviation.
The effect of whole soy and purified daidzein on bone turnover markers among the three study groups.

p value.
Data are presented as mean ± SD and compared by one-way analysis of variance. Variables with significant heterogeneity in variances which cannot be adjusted by data transformation were compared by Kruskal–Wallis non-parametric analysis. Coupling index was calculated as normalizing resorption (CTX) and formation marker (PINP) as Z scores and expressed as the ratio of the two markers.
β-CTX, beta C-terminal telopeptide of type I collagen; BALP, bone alkaline phosphatase; OST, N-mid osteocalcin; P1NP, N-terminal propeptides of type I procollagen; SD, standard deviation; 25(OH)D3, 25-hydroxyvitamin D.
The effect of whole soy and purified daidzein on inflammatory markers among the three study groups.

p values.
Data are presented as mean ± SD and compared by one-way analysis of variance. Variables with significant heterogeneity in variances which cannot be adjusted by data transformation were compared by Kruskal–Wallis non-parametric analysis.
Hcy, homocysteine; Hs-CRP, high-sensitivity C-reactive protein; IL-6, interleukin-6; SD, standard deviation; TFR: transferrin; TNF-α: tumor necrosis factor alpha.
Subgroup analysis showed that post-menopause years, BMI, and 25(OH)D3 caused no alteration in the conclusions (Table S1). The partial correlation analysis (Table S2) indicated that the 6-month change in Hcy resulted in a significant and positive correlation with the changes in bone remodeling markers, such as β-CTX, PINP, BALP, OC, and 25(OH)D3 (all p <0.05). The changes in serum TFR were also positively correlated with the changes in BALP, OC, 25(OH)D3, and coupling index. Adverse events and compliance were reported previously. 31 A total of 99 participants were randomly selected for the final 24 h urinary isoflavone testing for compliance check. The urinary isoflavone levels indicated good compliance among participants.
Discussion
This 6-month RCT among equol-producing postmenopausal women indicated that the consumption of whole soy and purified daidzein showed no beneficial effects on bone remodeling and inflammation status. This work is the first RCT specifically conducted among equol-producing postmenopausal women, who are a population at high risk of bone loss and fracture due to estrogen deficiency, and most likely to benefit from soy intervention due to equol-producing capacity, to examine the effect of soy on bone metabolism. One novel aspect of the study was the comparison of the commonly used whole soy foods (soy flour and potentially active soy component of daidzein) in one study. This work is also the first RCT testing the independent effect of daidzein on bone remodeling markers. This study featured a relatively large sample size, effective randomization and blinding, low dropout rate, and good participant compliance, as indicated in our published article. 31 In this trial, equol status was defined by a standardized method via consecutive several days of daidzein challenge to ensure sufficient daidzein exposure. Rigorous strategies have been implemented for standardization to minimize the possible variations from preanalytical and analytical biological sources, which include the following: biological samples collected under the same conditions to reduce circadian variance, block randomization that reduced the error from seasonal variance, and exclusion of the participants with limited mobility. Although current results were secondary outcomes, the study showed sufficient power to detect expected changes in BTMs and inflammatory markers and accounted for dropouts. The measures of the BTMs offer advantages in clinical practice, such as reflecting the metabolic activity of the entire skeleton, with the major change occurring in a relatively shorter time (3–6 months) following treatment, than that of BMD (at least 1–2 years). 37 Bone markers also aid in understanding the pathogenesis and mechanism of osteoporosis. BTMs perform important functions in fracture prediction, and the predictive value is independent of bone mass. 38 Thus, the routine measurement of BTMs is important in clinical practice. 39
Current evidence on soy or isoflavones on bone metabolism remains uncertain and limited by considerable heterogeneity across trials. 19 The latest research suggests that different isoflavones forms (aglycone/glycoside), isoflavone composition and dosages, as well as equol status (gut microbiota) may have a crucial impact on the bioavailability, metabolism, and, ultimately, efficacy of bone health. 40 Isoflavone aglycones exhibit enhanced bioavailability and efficacy for treating estrogen-deficient bone loss. 16 Providing bioavailable isoflavone aglycones together with probiotics may maximize uptake and minimize the influence of inter-individual differences in microflora on metabolism. 41 Future clinical trials prespecifying these factors are necessary to investigate the therapeutic effect of isoflavones on bone loss.
The lack of significant effect on bone markers in our study is unlikely to be due to inadequate duration or relatively high habitual soy intake of Chinese women. Compared with BMD, the evident changes in BTMs can only occur in 3–6 months following treatment. 37 Although several long-term RCTs (>6 months) indicated the remarkable effect of soy on BTMs,41,42 clinical trials with shorter duration (50 days to 6 months) than our study also reported a significant effect on bone remodeling markers.43,44 Soy isoflavones show weak estrogenic activity with an effectiveness that is incomparable with that of medications for osteoporosis. Thus, long duration is required to acquire favorable effect on the bone remodeling process. The relatively high background soy intake in our participants also cannot explain the nil effect in our study. The participants were given instructions on the restriction of habitual soy intake to less than two servings per week since the run-in period. The subsequent dietary survey during follow up suggested a good compliance of our participants on the required lifestyle modifications. We have also specifically recruited equol-producing women who are supposed to obtain more health benefits from soy treatment than non-producers.
Although isoflavones possess an anti-inflammatory property, clinical trials assessing the effects of soy on inflammatory markers offer inconclusive results. 45 Our study showed that whole-soy consumption marginally reduced the hs-CRP level, but no effects on other inflammatory markers were observed. Our findings agree with those of a recent meta-analysis, 45 wherein soy foods or isoflavones showed no significant effects on inflammatory markers, including IL-6 and TNF-α. The non-significant findings in inflammatory markers in our trial could be due to the relatively healthy status of our participants, although they presented with slightly increased BPs. The clinical trials conducted among patients with ischemic stroke, 46 overweight and obese menopausal women, 47 or menopausal women with metabolic syndromes 48 all reported improved anti-inflammatory effects. Inflammatory status may interfere with isoflavone metabolism. Thus, healthy and diseased individuals may metabolize flavonoids differently. Our results also reveal a significant correlation between the pre–post changes in BTMs, and inflammatory markers of Hcy and TFR. The findings were consistent with those of previous reports indicating that Hcy could modulate bone remodeling through the generation of reactive oxygen species, 49 and increased iron stores can be a risk factor for oxidative damage and bone resorption. 50
The present study features several limitations. First, we did not determine the basal bone mass status of the participants. Although the study was not specifically conducted among women with osteopenia or osteoporosis, remarkable bone loss is common in women after menopause, 51 with the prevalence of osteoporosis and osteopenia accounting for nearly two thirds in Chinese women (Hong Kong and Beijing) aged 50–79 years.52 Stratification analysis also showed that women in early menopause (less than 5 years after menopause), who are supposed to present with higher bone loss than late-year post-menopausal women, showed no significant difference among the three study groups. Thus, the basal bone mass status of participants may be insufficient to completely explain the null findings. Additional RCTs specifically conducted in women with remarkable bone loss are necessary. Second, the participants were volunteers with either pre- or early hypertension and had relatively high education attainment. Thus, the participants may be more health conscious than the general population of similar ages, which may influence the study generalizability. Third, the trial was conducted among equol producers, and we did not compare the effects on bone biomarkers between equol and non-equol producers. Future clinical trials including different equol phenotypes in one trial would validate our findings. Fourth, the participants in this study belonged to different menopausal age groups. Estrogen and follicle-stimulating hormone were also not assessed when defining the menopausal state. Therefore, differences in the estrogen levels in these women may have affected the results of this study. Finally, certain biomarkers reflecting bone metabolism and regulation were present. However, given the budget limit, we only tested the biomarkers that are often applied in clinical practice. Soy or isoflavones may affect the untested biomarkers.
Conclusion
This 6-month RCT among equol-producing postmenopausal women indicated that the consumption of whole soy and isocaloric isoflavone daidzein in the provided dosages caused no significant effects on bone remodeling and inflammatory markers.
Supplemental Material
sj-pdf-1-tae-10.1177_2042018820920555 – Supplemental material for Effect of whole soy and isoflavones daidzein on bone turnover and inflammatory markers: a 6-month double-blind, randomized controlled trial in Chinese postmenopausal women who are equol producers
Supplemental material, sj-pdf-1-tae-10.1177_2042018820920555 for Effect of whole soy and isoflavones daidzein on bone turnover and inflammatory markers: a 6-month double-blind, randomized controlled trial in Chinese postmenopausal women who are equol producers by Zhao-min Liu, Bailing Chen, Shuyi Li, Guoyi Li, Di Zhang, Suzanne C. Ho, Yu-ming Chen, Jing Ma, Huang Qi and Wen-hua Ling in Therapeutic Advances in Endocrinology and Metabolism
Footnotes
Authors’ note
Neither the Natural Science Foundation of Guangdong Province and Hong Kong Research Grant Committee-General Research Fund, nor soy and dairy company had any role in the design and conduct of the study; the collection, analysis, and interpretation of the data; or the preparation, review, or approval of the manuscript.
Author contributions
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The trial was supported by the Natural Science Foundation of Guangdong Province (grant number 2017A030313797) and Hong Kong Research Grant Committee-General Research Fund (grant number RGC-GRF465810).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.