
Abstract
Background:
Owing to the increasing popularity of smartphones in Rwanda, almost 75% of the entire population currently has access to the internet. Although it has been shown that smartphone applications can support diabetes self-management, there was no diabetes self-management application available in Rwanda until April 2019. Based on the findings of a prior study assessing the needs and expectations of potential users, ‘Kir’App’ was developed to fill that void. The aim of this study was to evaluate users’ experiences after 3 months of use of the first Kir’App prototype.
Methods:
The participants of the previous study were recruited to take part in the current study. Semi-structured, in-depth, face-to-face interviews were conducted. Findings were analysed thematically using Mayring’s method of qualitative content analysis. Both deductive and inductive approaches were used to analyse transcripts according to the original categories and subcategories of the previous study.
Results:
A total of 14 people with either type 1 or type 2 diabetes participated in the study. Age of participants ranged from 19 to 70 years, with a mean age of 34.4 years. Seven of the eight original themes and one additional theme were subjoined: diabetes education and desired information provision; increased diabetes knowledge and awareness; monitoring and reminder functions; nutrition; physical activity; coping with burden of disease; app features; use behaviour and usability. Overall, participants stated that the app increased their diabetes knowledge and assisted them with their diabetes self-management.
Conclusions:
We found that the first prototype of Kir’App meets the overall needs and expectations of participating Rwandan diabetics. Having followed a strict user-centred design process, their qualitative insights will help to further improve the app.
Keywords
Introduction
Telemedicine applications, in particular when app-based, allow for tailoring of content for each individual user, 1 continuous monitoring and direct feedback on the data provided by the user.2,3 Such app-based interventions cover basic components of diabetes self-management and education (DSME). 4
Such applications regularly deliver cues to action due to their high degree of tailoring and individualized information provision, and therefore demand proactive use behaviour of their users. 5 If the end user is unwilling to engage in continuous use of such apps and all their functionalities, the apps can never fulfil their purpose, 6 which is to serve as a tool for DSME. While usability, that is, ease of use of such applications,7,8 is one important factor prompting end user acceptance, so are performance expectancy and perceived usefulness. 9 Both refer to the users’ feelings that an application does what they hoped it would do and thereby helps them with their disease self-management.10,11
Therefore, especially when aiming to design patient-centred applications required for DSME, incorporating expectations of potential users is a necessary step in the development process. 12 Esser and Goossens propose a framework for user-centred design that incorporates patient outcomes such as acceptance and compliance, as well as several background variables, including cultural factors. 13 This is in line with the International Organization for Standardization (ISO) norm for human-centred design for interactive systems. 14
For Rwanda, especially the highly centralized and hierarchical health care system and culture are relevant. 15 Rwanda has a population of 12.21 million people, two-thirds of which live in rural areas. The median age is below 20 years. 16 The estimated share of people living with diabetes is between 2.8 and 3.4%, adding to an estimated number of 155,000 undiagnosed cases. While there is little data on the routine care for diabetes in Rwanda, the WHO recommends comprehensive coverage by pharmacological treatments (insulin, metformin, etc.). However, especially oral tests for glucose tolerance and the HbA1c-level are lacking. 17 Furthermore, a study on young diabetic patients showed that one-third of those have highly elevated HbA1c levels (above 14%) and already suffer from hypertension, a comorbidity which, given the appropriate treatment, can be prevented throughout the patient’s life course. 18 A study by Mukeshimana and Nkosi revealed knowledge gaps concerning the symptoms and pathogenesis of diabetes that were significantly correlated with the degree of education. 19 Concerning cultural aspects, studies show that traditional medicine and its religious underpinnings still are of importance to the Rwandan population. 20
Almost 75% of the Rwandan population have access to the internet, a number which has increased, according to local authorities, due to the increased use of smartphones. 21 Consequently, initiatives aiming to use mHealth applications for diabetes management are currently blooming. 22 Telemedicine applications, such as video conferencing, are already in use. 23
A whole set of methods can be applied to gain information from the potential user, all of them to be used before starting the development cycle as well as after having circulated the first prototype. 24
Therefore, a user-centred design process was chosen to develop the first self-management app for diabetes patients in Rwanda. Before beginning the development process, 21 in-depth interviews with patients suffering from both type 1 and 2 diabetes took place in order to gain insight into their expectations towards a potential application. 25 As DSME requires proactive health behaviour and therefore behaviour change, analysis of the interviews was structured using the Health Action Process Approach (HAPA) proposed by Schwarzer. 26 Within the HAPA, outcome expectations are important predictors for health behaviour chance. The following outcome expectations where formulated by the patients in the initial interviews:
(1) information, specialized education on diabetes and skills for coping with the disease;
(2) knowledge about diabetes burden in everyday life and crisis situations;
(3) information on food, drink choices and alcohol intake;
(4) right type, amount and motivational input for physical activity;
(5) monitoring and reminder functions for diabetes parameters (health check-ups), doctor’s appointments and taking medication;
(6) emotionally supportive content and the ability to connect with other people living with diabetes;
(7) bilingual support using both Kinyarwanda and English;
(8) information delivery combining written content, images, audio and videos according to user preference.
Following a user-centred design process, the results of the previous study were used to develop a prototype of the first diabetes self-management app in Rwanda (Kir’App).
Aim of the study
This study aimed to evaluate user experience after 3 months use of Kir’App. The overall aim was to check whether the outcome expectations assessed during the previous study were met by the initial prototype of Kir’App.
Study objectives
(1) To assess positive aspects of Kir’App identified by users after 3 months of use.
(2) To assess negative aspects of Kir’App identified by users after 3 months of use.
(3) To identify the users’ suggestions for improvement of Kir’App.
Following these objectives, we aimed to explore whether the outcome expectations gleaned from the first interviews were met by the initial prototype of Kir’App.
Methods
This study was done as a follow up of a previous study on the assessment of Rwandan diabetics’ needs and expectations considering a diabetes self-management app. 25
Study design
For the assessment of the first prototype from a user perspective, in-depth interviews with diabetes patients having used Kir’App over a period of 3 months were conducted. The interviews were face-to-face and followed a semi-structured interview guideline. In-depth interviews are a common method used in user-centred design processes. 24
First, biographical data and self-rated intensity of smartphone as well as app use were collected. Participants were then interviewed about their experiences with Kir’App after 3 months of use. This part of the interview was guided by three questions concerning perceived positive and negative aspects as well as challenges. Lastly, participants were asked for suggestions on how to improve the app.
While using the app, participants had the opportunity to ask questions to the diabetes expert running the app. These questions were again categorized, applying inductive thematic analysis.
Participants
To find out whether their expectations were met by the first prototype of Kir’App, participants of the previous study were asked to participate again in the current study.
Participants were recruited from patients attending the Rwanda Diabetes Association, which is visited by diabetics from different areas of the country, both urban and rural. Their age groups were diverse. They were chosen randomly without prior assessment of either their education level or their diabetes-related health literacy.
Participants had to be Rwandan, aged 18 years or older, living with type 1 or type 2 diabetes, registered with the Rwandan Diabetes Association and having daily access to a smartphone. Of the 21 participants taking part in the first study, only 14 were available and participated. Of the seven who did not participate, one had left the country, one wished not to participate without further reason, two no longer possessed smartphones (one stolen, one broken) and three had iPhones (Kir’App is available only on Android platforms). Participants were not compensated for their participation, either monetarily or with incentives.
Study procedure
Permission to conduct the study was obtained from the Rwandan Diabetes Association and from the Institutional Review Board of the College of Medicine and Health Sciences of the University of Rwanda. Ethical approval No 021/CMHS IRB/2018.
A researcher installed Kir’App on the participants’ phones, along with a brief explanation of how the app works and the functionalities it includes. Data collection for the current study took place 3 months after initial use of Kir’App at the Rwandan Diabetes Association. Written consent to participate was sought before each interview, along with the assurance that it could be withdrawn at any time during the interview. All interviews were audio-recorded; however, any information on the identity of the participants was stored separately from the records in order to ensure anonymity. Interviews lasted 10–15 min. All interviews were transcribed and subsequently translated into the English language.
Along with the interviews on users’ experiences of Kir’App, a standardized usability test of the app was conducted. The results will be published elsewhere.
Data analysis
The transcripts were analysed following Mayring’s method of qualitative content analysis. 27 As the overall study aim was to see if the expectations of potential Kir’App users had been met after actual use of a prototype, the original categories from the first study 25 had to be matched. As such, the initial approach was deductive, analysing the transcripts according to the original categories and subcategories. Wherever new patterns emerged from the text material, new categories and subcategories were formed in an inductive manner, since no background information existed to structure these new results.
Matching (deductive approach) and formation of the new categories (inductive approach) were performed by three researchers (CB, PT, LH) independently. Results were discussed until consensus was reached.
Study results
Demographics of study participants
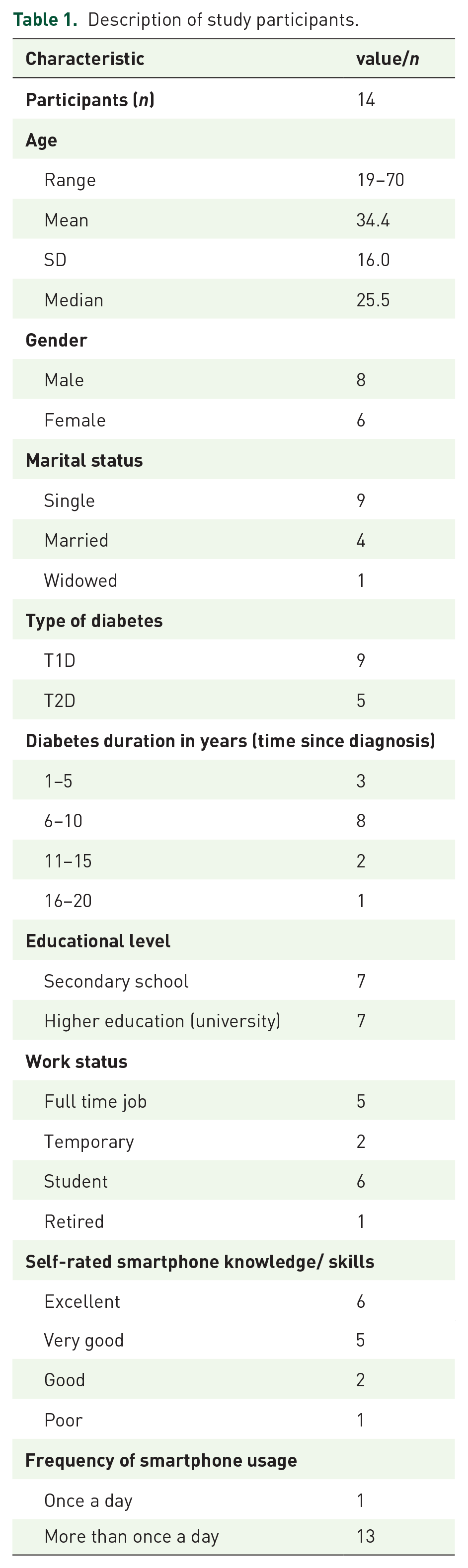
The 14 participants had a mean age of 34.4 years [standard deviation (SD) = 16 years, median age = 25.5 years); 8 were male and 6 were female (57.1% versus 42.9%) and most (9) had type 1 diabetes (Table 1). Most patients (11 out of 14) had been diagnosed at least 6 years ago. The majority of participants (11 out of 14) rated their smartphone skills as ‘very good’ or ‘excellent’. Most participants used their smartphones more than once a day.
Description of study participants.
Summary of themes and subcategories.

Results of in-depth interviews
In the following, the results from in-depth-interviews on user experiences are presented according to the categories developed in the first Kir’App study. 25 As none of the 14 participants mentioned an impact of app content on consumption of beverages in general and especially alcohol intake, the corresponding theme was relabelled to only cover issues of nutrition. It is now devoid of any subcategories, since no text answers matched the subcategory ‘pleasure of eating’. Relabelling was also done for the category and subcategories concerning diabetes-related knowledge, as participants now reported increased knowledge rather than a lack thereof.
The theme ‘coping with burden of disease’ now contains three subcategories, as answers revealed feelings of patient empowerment fostered by use of the app. The theme ‘crisis intervention’ was no longer mirrored in the results and was therefore dropped. A whole new theme now covers use behaviour and usability aspects mentioned by the participants.
In the following, each category and subcategory is described and exemplified in detail (Table 2).
Diabetes education and desired information provision
This theme refers to the availability of materials for diabetes education in the App.
General information on diabetes, management and complications. Users stated that the app supported them to fill gaps in their knowledge about diabetes.
‘[. . .] the first time when you asked me which type of diabetes I had, I said type 2 then went to ask my doctor and came back to tell you I was type 1. [. . .] The detailed explanations I found in Kir’app helped me to understand all types of diabetes [. . .].’ [P5]
Medical parameters (e.g. blood pressure, blood glucose, body weight etc.). Users expressed satisfaction with the individualized feedback on different medical parameters they received from the App.
‘Kir’App interprets my blood sugar results and shows me which action to take immediately [. . .] I can even calculate my BMI using the calculator in Kir’App [. . .] so I can keep in mind what my limit must be’ [P2]
Frequently asked questions by newly diagnosed patients. Users were pleased that the app provided a forum for posting inquiries about their individual experiences with diabetes, in addition to the section for frequently asked questions.
‘I like [. . .] the part of frequently asked questions found on every page. [. . .] It’s so helpful to click and find your question and its answer there. [. . .] even if you don’t find it [the question] there [. . .] you can even use the different forums and ask [your questions] immediately.’ [P6]
National/regional update and initiatives. Users found it helpful to have information in the app about local services (e.g. pharmacies) needed in their daily diabetes management.
‘Another thing that I liked in Kir’App is the list of pharmacies with available medicine and materials needed by diabetes people in every district of Rwanda.’ [. . .]
Increased knowledge and awareness
The theme reveals users’ experiences with the app in compensating for their knowledge gaps.
Increased knowledge on living with diabetes. Users reported the app helped them to increase their level of knowledge about diabetes self-care behaviours.
‘I also learnt about warning signs in case of foot problems, now I know that some signs that we consider as normal like having very hot or very cold feet can alert some danger and that I have to go to see my doctor whenever I feel it.’ [P9]
Prejudice and myths. Users reported that Kir’App helped them to uncover and discard false information (rumours and myths) on diabetes.
‘I’ve always wanted to ask my doctor about a rumour I heard about the effect of diabetes on sexual performance [. . .] when reading the first page of Kir’App [. . .] I saw a picture of a man with diabetes complications on different parts of his body even on sexual organs. This disease is terrible.’ [P13]
Monitoring and reminder function
This theme refers to monitoring and reminder functions of diabetes care parameters available in the app.
Blood glucose or sugar recording and trend visualization. In this subcategory, participants express their experiences with recording and monitoring of diabetes-related clinical parameters, and how this impacted their disease management.
‘[. . .] I have a record of quite all my blood sugar numbers of the last 3 months and with the option to check their variation, I can see where it went up or down [. . .] and get to manage well my blood sugar levels [. . .]’ [P7]
Reminder functions. Users were pleased to have several automated reminders for a variety of tasks relevant to diabetes care.
‘Some days are very hectic and I become much stressed which makes me forget my regular health checkups but with Kir’App reminder, I don’t forget them anymore. The good thing with this reminder is that I can set alarms for different activities like blood sugar testing, taking drug, A1c checking, eye check, doctor appointment, buying a new drug and many others and each will ring at its own time.’ [P4]
Nutrition
This theme refers to the availability of information about the appropriate diet for patients with diabetes.
Composition of a diabetic plate. The content in Kir’App on how to prepare a diabetic plate helped the users to control their eating habits.
‘Kir’App taught me how to balance my food. Now it has been some weeks that I no longer get high blood sugar episodes because of food.’ [P1]
Physical activity
The theme refers to the provision of information on the kind and amount of exercise required when coping with diabetes. It also covers the motivational advice given within the app.
Kind of sport to do. Participants describe how the information about the adequate type of exercises provided in the app changed their physical activity.
‘[. . .] I have started to alternate the two categories of sport [aerobic exercise and strength training] a diabetic person has to do as described in Kir’App.’ [P1]
Motivation for physical activity. Some users reported change in their exercise behaviour due to the motivational messages within the app.
‘I used to neglect to do sport[s] mainly because of my age but when I got to know its benefits on my health, I got encouraged to do it.’ [P8]
Frequency and duration of physical activity. Users found recommendations in the App about the right amount of physical activity required.
‘[. . .]Two times a week I play volleyball or do jogging as aerobic exercises and at least once a week I lift weights in gym-tonic (fitness studio) as strength training.’ [P1]
Coping with burden of disease
Theme 6 refers to the emotional support the app content provides and the current inability of the app to connect diabetics with each other. It also covers the empowerment users felt when being able to participate in shared decision making with their doctor concerning their individual diabetes care.
Emotional support. The participants felt that the app assisted them in coping with situations of emotional distress.
‘I am widow since now 8 years, my husband left me with three kids and I am always worried about their future when I think about dying and leaving them alone. I was glad to find in Kir’App some advice given to parents who live with diabetes. [. . .]’. [P10].
Social support. Users wished the app could put them in contact with other people living with diabetes.
‘It would be good to have a social media forum in Kir’App [. . .] where type 1 could meet, exchange ideas and share experiences of our everyday life.’ [P11]
Shared-decision-making/empowerment. The information and knowledge found in the app empowered users to make shared decisions in their healthcare together with their physician.
‘I usually have good numbers of blood sugar levels. But for example, I didn’t know anything about A1c and other health checkups we need to do regularly. When I read about them in Kir’App, [. . .] I told the new one [doctor] that I needed to do all necessary health checkups and she prescribed me all of them.’ [P8]
App features
The theme refers to experiences of the participants with the app features provided for information delivery and to the availability of content in different languages.
Information delivery. Users appreciated the content organization of the app and its information delivery through texts and images but regretted the absence of audios and videos.
‘I like much how appealing Kir’App is. It has beautiful colours that attract attention. I like also how well organized it is; information about every topic (food, sport, feet, etc.) has its own page [. . .].’ [P7] ‘It is good Kir’App has images that go with the texts but it would be better if it could also have some videos. For example in physical activity; having some videos that show how to do all these exercises shown on images would be great.’ [P9]
Available languages. Users were pleased to have the app content in their local language, Kinyarwanda.
‘I appreciated having all this helpful information about my disease in Kinyarwanda. Nowadays we use much English, but being able to understand things that concern your life in a language you understand well is a very good thing.’ [P14]
Use behaviour and usability
This theme refers to the users’ general experiences with the usability of the app and to their individual use behaviour.
‘In general, using Kir’App is like seeking pieces of advice from a friend, you cannot come just like that, get what you want and go back. You need to give it time because, the more you spend time using it, the more you get more interesting information and the more you understand more about diabetes and get ideas about your self-care.’ [P6]
Discussion
The present study applies a user-centred design approach to validate previously identified (sub)categories representing needs and expectations of Rwandan patients towards their first diabetes self-management smartphone application (Kir’App). In general, the majority of categories and subcategories were identified again when analysing the transcripts. Interestingly, ‘use behaviour and usability’ was the only category that appeared in addition to the original ones. This underlines the importance of an iterative user-centred design process, as issues with usability and specific usage patterns can only manifest when a first prototype of an application can be tested. 14 The availability of diabetes health education and frequently asked questions was appreciated by Kir’App users in general, which fits the qualitative results on user perceptions of mobile health apps gained by Peng and colleagues. 28 Especially the need for diabetes-related information early after diagnosis, when symptoms are not well known to the patient, is an important component of DSME, 4 and can be delivered by an app. 29 Fittingly, the provision of the desired information was mentioned as the most common use of Kir’App. Furthermore, users said to have gained knowledge about diabetes in general, and on strategies to live with it, which corresponds to survey results on reasons for technology use among adolescents with type 1 diabetes. 30 In a systematic review, Rush and colleagues show that virtual education approaches can improve clinical indicators as well as surrogate parameters such as disease-related knowledge and quality of life in patients with a variety of chronic diseases, among them diabetes. 31
Users claimed that reminder functions, recording and trend visualization of medical parameters, especially blood sugar, offered by Kir’App helped them to be more aware of and accountable for their diabetes self-management activities, which is in line with results of pilot test of a self-management app provided by Dobson and colleagues. 32 These results are especially important for further analysis of the effectiveness of the app, as a meta-analysis by Cui and colleagues has demonstrated that using apps for self-management can improve glycaemic control. 33 Including a positively rated and well-used reminder function into a self-management app, therefore, is of vital importance. Tracking of food intake and physical activity by using diaries were rated important by the participants, which is in line with review results by Williams and colleagues. 34 Goyal and colleagues demonstrated that the logbook function within their app significantly increased self-management behaviour, which, in turn, led to decreased levels of HbA1c over a time period of 12 months. 35
Kir’App users stated to have found useful pages in the app with advice for daily life, not only for themselves but also for relatives and family members. The pieces of advice were appreciated as a means of coping with the burden of disease as they provided emotional support. The involvement of family members and peers in diabetes self-management interventions has been found to be important in several current reviews.36,37 Interactive forums and social media functions are nevertheless missing from the app, yet have proven effective in reducing HbA1c due to the support they can provide. 38
Users also appreciated having the app in both English and their mother tongue, which, as they say, allows them to better understand the information and therefore leads to more comfortable app use. This proves that having potential users participate in the design process of future digital diabetes interventions is worthwhile, as it helps overcome language and cultural barriers. 39 The fact that some participants stated now being able to better distinguish myths from facts about diabetes further underlines this point.
However, some users pointed out how complicated it could be for people with poor education to use the app. Indeed, low health as well as overall literacy can be an obstacle to telemedicine use, 40 yet can be overcome by the use of visual rather than text material and, where necessary, simple language, as suggested by the German guideline for evidence-based health information. 41
As self-management applications should support behaviour change as modelled in the HAPA, 26 it is encouraging that the app actually helped participants not only in forming an intention to be more physically active but also in making the transgression from intention to action. As participants stated that the app also helped them to log physical activity levels, it also served as a tool for self-monitoring as a form of action control, which is an important predictor for the maintenance of healthy behaviour according to the HAPA. 42 In general, outcome expectancies and whether they are met is an important variable in the process of behaviour change. As such, the results of the interviews show that the main outcome expectancies towards a diabetes self-management app were met.
The categories we identified were almost identical to those found in our previous study. Feedback allowed initial users to report whether their expectations towards the application have been met; such feedback is not only recommended by the ISO Norm for the user-centred design of interactive systems but is also a common standard in user-centred design frameworks for digital health solutions.13,24,43
Limitations
As described in the previous manuscript 25 semi-structured interviews have several limitations, mainly because they do not allow for standardization and quantification of results, and rely on the recollection of participants. 44 The low number of participants and the fact that their recruitment resulted from convenience sampling further limits external validity of findings.
Some additional limitations arise from qualitative content analysis as a method. For example, the individual backgrounds and subconscious expectations of the authors may have impacted the deductive coding process. Although it is a strength of user-centred design processes that they iteratively allow for user involvement, the validated and slightly enhanced (sub)categories may be seen as self-fulfilling prophecy, as they were used to mirror the initially identified expectations.
Despite the overall positive findings, the authors admit that the pioneer character of this work does not allow for a comparison with similar apps or devices in Rwanda. As such, one participant argues, ‘It would be difficult to find something negative in Kir’App as there is no other similar App we were using before to compare with it.’ [P10] This can be seen as an indicator that participants may have difficulties to imagine functionalities going beyond the presented Kir’App content and features.
Future research and next steps
According to the results presented here, changes will have to be made in the content of Kir’App and its presentation. More visual elements (either pictures or videos) will have to be used to deliver basic concepts of diabetes self care. Along with that, some sections within the app will have to be presented in rather plain language. As participants wished for some modality to interact with other diabetes patients, a social media platform or chat room within the app is intended. For example, the ‘bant’ app for adolescents with type 1 diabetes contains a chat room called ‘banter’, which can serve as a role model. 45
In a next step, results of the quantitative usability testing conducted parallel to the semi-structured interviews will be analysed statistically. The main focus will be on the time it takes to perform certain tasks within the app, and in how far participants are satisfied with the effort they have to put into the completion of these tasks.44,46
Conclusion
The results of the 14 semi-structured and guideline-based interviews show that major expectancies towards a self-management app mentioned by Rwandan diabetics were met by the first prototype. In addition, responses of the participants serve as a first indicator that the use of Kir’app can instigate behaviour change, which should be investigated in future effectiveness studies. Statements about actual use behaviour show that it took time to get used to the app and that visual presentation of content would be welcomed.
All in all, the results will allow for improvements of the first prototype, as intended by the user-centred design process, and form the basis of further, quantitative usability testing.
Supplemental Material
TAE-19-11-107_Annex_1._Comparison_of_themes_2.1 – Supplemental material for A qualitative study of users’ experiences after 3 months: the first Rwandan diabetes self-management Smartphone application “Kir’App”
Supplemental material, TAE-19-11-107_Annex_1._Comparison_of_themes_2.1 for A qualitative study of users’ experiences after 3 months: the first Rwandan diabetes self-management Smartphone application “Kir’App” by Claudine B. Kabeza, Lorenz Harst, Peter E.H. Schwarz and Patrick Timpel in Therapeutic Advances in Endocrinology and Metabolism
Footnotes
Acknowledgements
Authors Claudine B. Kabeza and Lorenz Harst contributed equally. The authors would like to acknowledge the Rwandan Diabetes Association for providing permission and for allowing use of the association’s facilities. They also wish to thank the Rwandan diabetics whose participation made this study possible. The authors also would like to thank Kristin Kemple for proofreading this manuscript.
Authors’ note
C.K and P.S. conceived the study. C.K. collected the data. L.H., P.T and C.K. contributed to the analysis and interpretation of data. L.H., C.K and P.T. wrote the manuscript. P.T. reviewed and edited the manuscript. L.H., C.K., P.T. and P.S. approved the version for submission.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: For the research work; by the Ministry of Education of Rwanda, the University of Rwanda and the German Academic exchange service (DAAD). For authorship; partly by the European Social Fund and the Free State of Saxony (Grant no. 100310385). For article publication; by the Open Access Funding by the Publication Fund of the TU Dresden. The funding organizations above mentioned are employers and funding agencies of the authors. None funded Kir’App development directly. The App was developed at an educational public organization in Rwanda and will stay a free product for the population of Rwanda.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.