
Abstract
Background:
Knowledge of and coping with diabetes is still poor in some communities in Rwanda. While smartphone applications (or apps) have demonstrated improving diabetes self-care, there is no current study on the use of smartphones in the self-management of diabetes in Rwanda.
Methods:
The main objective of this study was to assess the needs and expectations of Rwandan diabetic patients for mobile-health-supported diabetes self-management in order to develop a patient-centred smartphone application (Kir’App).
Results:
Convenience sampling was used to recruit study participants at the Rwanda Diabetes Association. Twenty-one patients participated in semi-structured, in-depth, face-to-face interviews. Thematic analysis was performed using Mayring’s method of qualitative content analysis.
Conclusions:
The study included 21 participants with either type 1 (female = 5, male = 6) or type 2 (female = 6, male = 4) diabetes. Participants’ age ranged from 18 to 69 years with a mean age of 35 and 29 years, respectively. Eight main themes were identified. These were (a) diabetes education and desired information provision; (b) lack of diabetes knowledge and awareness; (c) need for information in crisis situations; (d) required monitoring and reminder functions; (e) information on nutrition and alcohol consumption; (f) information on physical activity; (g) coping with burden of disease, through social support and network; (h) app features. This study provides recommendations that will be used to design the features of the first Rwandan diabetes self-management smartphone application (Kir’App). The future impact of the application on the Rwandan diabetic patients’ self-management capacity and quality of life will be evaluated afterwards.
Diabetes care in Rwanda
Approximately 425 million adults (age 20 to 79 years) have diabetes worldwide. 1 In 2045, this number is expected to rise up to 629 million. In Africa, the number of patients with diabetes is expected to rise from 16 to 41 million (+156%). According to the World Health Organization, 2.8% of the Rwandan population are estimated to have diabetes. 2
Rwanda’s community-based health insurance system covers 80% of the population (2015–2016) and is further improving towards universal health coverage of the country. The healthcare system also covers country’s poorest citizens through its home-grown development programme that aims to lift the living standards of poor families and to facilitate their access to healthcare.3,4 Although Rwanda’s national programmes ascertain general access to healthcare, knowledge and perception of diabetes mellitus is still inadequate in some communities of the country. 5
Evidence on diabetes self-management
Strategies to provide education and support, for example, diabetes self-management education (DSME) programmes, for patients with type 2 diabetes mellitus (T2DM) incorporate ongoing self-monitoring of glucose levels and other diabetic outcomes as well as setting of behavioural goals. Behaviour change on the basis of these goals is the primary aim of DSME interventions, 6 for example, regular intake of fruit and vegetables or increased levels of physical activity. Recent evidence from a pre–postparallel group design study indicates that self-management reduces diabetes mellitus (DM)-associated comorbid conditions as well as healthcare utilization and, therefore, overall cost. 7 According to a meta-analysis of eight studies, DSM improved DM-related quality of life. 8 Mezuk and colleagues found significant improvements of glycated haemoglobin (HbA1c) through self-management in a group setting in which lay healthcare workers served as coaches. 9 All in all, evidence suggests that patient empowerment and behaviour change through self-management support is crucial for the success of DSM.
Self-management demands continuous medical support, as well as monitoring of disease-specific parameters. It is therefore regarded as the ideal target for telemedicine interventions.10–12 The International Diabetes Federation (IDF) published six categories of mobile applications (or apps) used in diabetes management. 13 This includes tracking of medical parameters (e.g. blood pressure, blood glucose, body weight, etc.), nutrition (healthy food choices) and fitness data (physical activity) to support improved self-management and healthy lifestyle. They also call for a strengthening of patient relationships with their friends and families using social networks and blogs. Recent analysis shows mixed results for quality, reliability and privacy of available apps, making it hard for clinicians to recommend appropriate ones to their patients. 14 In Rwanda, Kateera and colleagues have published a study proposing the introduction of mobile health (mHealth) approaches in the management of noncommunicable diseases, including diabetes. 15
Theory-grounded development and implementation of behaviour-change interventions
Due to the varying backgrounds, needs and preferences of patients with chronic diseases, the whole process of planning, design and the implementation of the included technologies should be user-centred.16,17 Therefore, knowing and understanding the individual’s predispositions towards health behaviour change is of high importance when planning and for innovation. Theories and models of behaviour change provide guidance in this endeavour. Developed by Ralph Schwarzer in 1992, the Health Action Process Approach (HAPA) combines evidence-based theories, such as the Theory of Reasoned Action, the Theory of Planned Behaviour and the Health Belief Model. Its major contribution to health behaviour research is the inherent recognition that behaviour change has to be maintained over time. Both the intention (action planning) as well as keeping up the healthy behaviour (action) depend on several predictors, as shown in Figure 1.

The HAPA model. 18
A meta-analysis on the effectiveness of the Health Action Process Approach (HAPA) in predicting health behaviour change in chronically ill patients showed an overall fit of the model. Small-to-moderate effects were found for self-efficacy beliefs in the planning as well as in the volitional phase, whereas risk perception (vulnerability) showed only small effects. No effect was found for social support. 19 Physical activity among adults with T2DM can be predicted by the HAPA, with self-efficacy again being among the most important predictors. 20 There is also evidence that the use of apps has a positive effect on the social–cognitive predictors of the HAPA for individuals engaging in physical activity. 21 Based on this evidence, the HAPA is a suitable starting point for the interpretation of the results of the current study.
Objective
The objectives of the study are presented in Table 1.
Objectives of our study.
The presented research is part of a research project called ‘Kir’App Rwanda diabetes study’ aiming to develop the first Rwandan diabetes self-management smartphone application.
Method
Study design
A qualitative study design was employed.
Target population
The target population of the study were Rwandan patients with type 1 and type 2 diabetes registered with the Rwanda Diabetes Association (RDA) at the time of the study.
Participants and eligibility criteria
The inclusion criteria for participating in the study were defined as being Rwandan, aged 18 years and above, living with type 1 or type 2 diabetes, registered with the RDA and having daily access to a smartphone.
Data collection tool and pilot test
Semistructured face-to-face in-depth interviews (February to March 2018) were used to collect the data. The interview guideline was developed based on the methodology of in-depth interviews 22 the authors’ research background and experience in diabetes care as well as IDF guidelines and protocols for diabetes care. 1
The interview guideline consisted of two parts. In the first part, participant characteristics, including biographical data as well as self-rated smartphone knowledge and frequency of use were assessed. The second part covered nine questions assessing needs and expectations of Rwandan patients with diabetes for a potential diabetes self-management smartphone application (Kir’App). It covered the following topics: willingness to use a health app, possible functions of the app and expected support in daily life or in the management of the disease. The interviews were done in two steps.
First, a discussion was initiated on the general topics presented above. In cases where respondents were hesitant with their answers or replied too broadly, questions designed to prompt more detailed answers were asked. These were questions pertaining to concrete functions of self-management systems derived from literature, for example, assistance with the maintenance of physical activity. 23
A professional translator was consulted for the translation of the interview guideline from English to Kinyarwanda. After translation, a pilot test involving five Rwandan diabetic patients was carried out to validate the guideline. It was adjusted according to their feedback. The final interview guideline is provided in the appendix section.
Sampling method
As there is no database of Rwandan diabetic patients owning smartphones in the RDA, convenience sampling was used to recruit study participants. During a period of 2 months, a researcher attended the Rwanda diabetes clinic (located within the RDA) and invited every patient fulfilling the eligibility criteria to participate in the study.
Sample size
Redundancy within the answers hinted towards theoretical saturation when interviews with 21 participants had been conducted.
Interview setting and procedure
The face-to-face interviews were conducted at the RDA. After the self-introduction of the researcher, the purpose of the study was explained and a consent form was signed prior to the interview. The permission to record during the interview was obtained and when necessary, the researcher took some additional notes. The average duration of each interview was 1 h.
Ethical implications
Permission to conduct the study was obtained from the RDA and from the Institutional Review Board of the College of Medicine and Health Sciences of the University of Rwanda (no 021/CMHS/IRB). Participants were informed about their voluntary participation in the study and their right to withdraw their consent at any time. They were not compensated for their time with incentives. Participants signed the informed consent forms before the interviews were conducted. Anonymity and confidentiality were assured by coding participants’ names and the storage of the transcript in a locked cabinet.
Analysis
Interview transcription, coding and reporting
Each interview was audio-recorded, transcribed and analysed, applying inductive category formation suggested within Mayring’s method of qualitative content analysis. 22 For the final codebook (see Appendix, Table A1), paraphrases from the transcript were used to describe each theme and subcategory.
First, transcription was performed by one researcher (CB). The authors (CB, LH and PT) then familiarized themselves with the transcripts and afterwards, two of them (CB and PT) independently aimed to identify initial codes (themes). In a first iteration, underlying patterns and recurring schemes were identified within the answers to all guiding questions of the in-depth interviews. Those patterns formed the first broad categories. In a second iteration, some of these categories, appearing to cover different facets of a broader theme, were subsumed and thereby became subcategories.
After discussion and relabelling of both themes and subcategories, examples taken from the transcripts were added. This process was carried out independently by three authors (CB, LH and PT). Conflicting presumptions about themes and subcategories were discussed until agreement could be achieved or a third author settled the ties. No software was used for coding.
Reporting of study results is in line with the consolidated criteria for reporting qualitative research 24 as well as recommendations following the Standards for Reporting Qualitative Research. 25
Results
Participants suffered from either type 1 (female = 5, male = 6) and type 2 (female = 6, male = 4) diabetes and were aged between 18 and 69 years (mean age of 35.29 years). Three individuals refused to take part due to lack of time. No participant dropped out before the end of the interviews.
The characteristics of participating patients are summarized in Table 2. All participants (n = 21) reported that they would like to have a smartphone application supporting them in their diabetes management, either being strongly supportive (‘it would be wonderful’; ‘yes, it would be fantastic’) or simply open minded (‘Yes, if it can help me managing my disease, why not?’). A qualitative content analysis of the transcripts resulted in seven inductively formed themes. A summary of identified themes and subcategories is provided in Table 3. A more conclusive table summarizing the seven themes, their subcategories and one to four examples each can be found in the appendix section.
Description of study participants.

SD, standard deviation; T1D, type 1 diabetes; T2D, type 2 diabetes.
Summary of recurrent themes and subcategories.
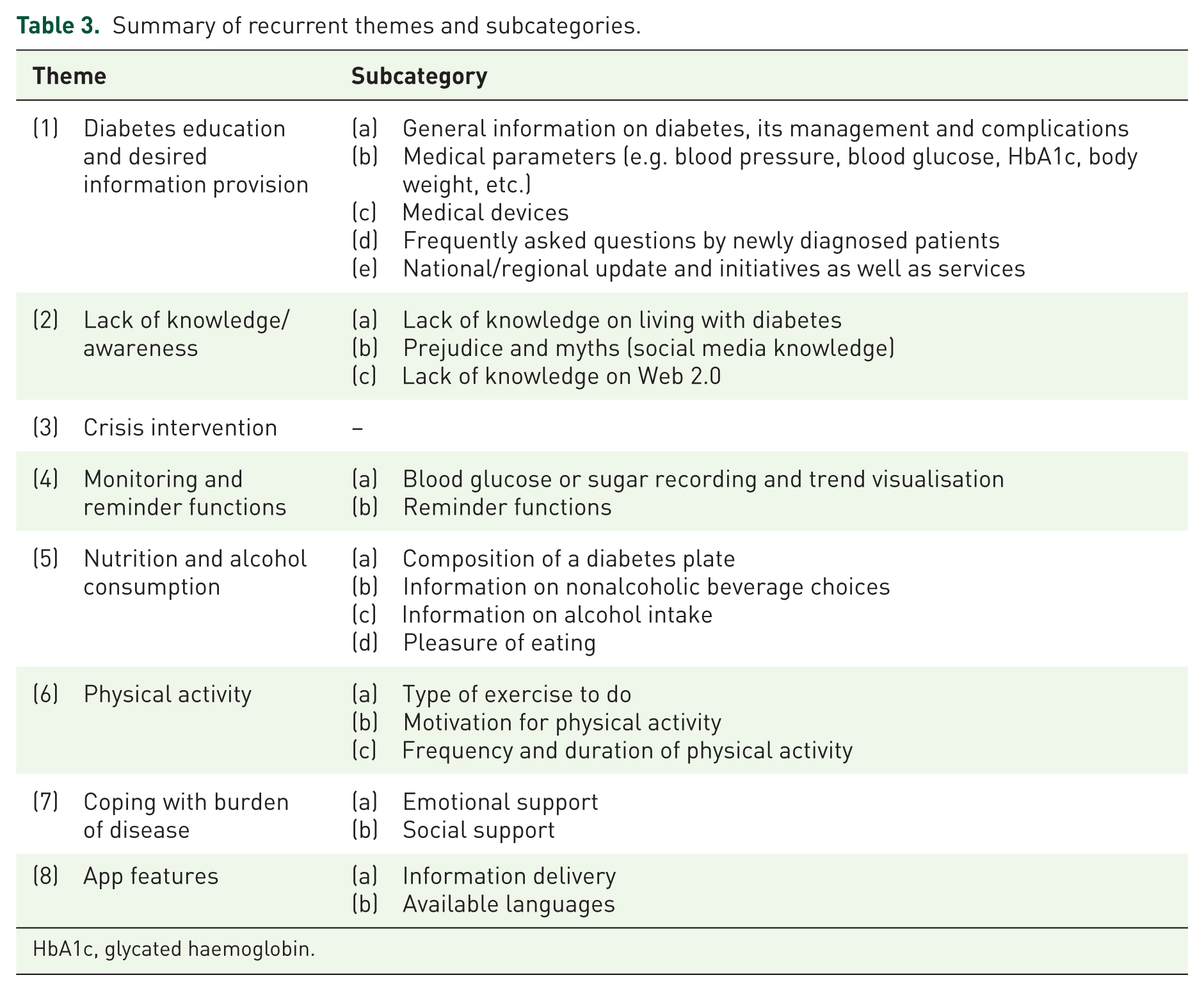
HbA1c, glycated haemoglobin.
The theme refers to the provision of information, specialized education on diabetes in general and the coping with the disease.
(a) General information on diabetes, management and complications
Participants wished to receive information from the application that can help close their gaps on diabetes knowledge.
‘…the application should teach us the difference between type 1 and type 2 diabetes because most people of my age don’t know which type of diabetes they are living with. The application should also teach us more about the medications we take and why some people use tablets when others are using insulin although we all have type 2 diabetes? It should also teach us about side effects of medications…’ (P11)
(b) Medical parameters (e.g. blood pressure, blood glucose, body weight, etc.)
Some participants expressed their will to receive specialized knowledge on medical parameters of DM.
‘My blood glucose levels sometimes reach 400 mg/dl, I wish the application [would] tell me what caused it to raise that high and […] teach me how I should lower it.’ (P4)
(c) Medical devices
Participants asked for support to monitor disease-specific parameters.
‘You know many diabetics like me don’t have glucose meters […]. We take our medication without knowing our levels of blood sugar and we only come here to the clinic once […] [a] month to check it or whenever we don’t feel okay.’ (P21)
(d) Frequently asked questions by newly diagnosed patients
Others underlined the special value of a target-group-specific repository of information for those being newly diagnosed with diabetes.
‘There are some people who are newly diagnosed with diabetes and who have a million questions about it, […] so the application should have a function [called] “frequently asked questions”.’ (P13)
(e) National/regional update and initiatives
Information on national or regional initiatives on diabetes care as well as local services (e.g. diabetes meetings) were asked for by the participants: ‘I wish the application to inform me about activities concerning diabetes that are taking place in Rwanda […]. Activities […] being organized for patients because now we don’t attend many due to lack of information.’ (P5)
This theme comprised characteristics of the individual end user, mainly knowledge gaps.
(a) Lack of knowledge on living with diabetes
Participants’ responses indicated knowledge gaps concerning the everyday life with diabetes, especially concerning disease-related behaviour.
‘I didn’t know that someone could develop foot problems because of diabetes. Right now, I have athlete’s foot and I’ve never thought that it could be linked to my diabetes […]. I wish the application [would] teach us about foot problems in diabetes, [so] I can learn how to take care of them and […] use it to teach other diabetics.’ (P7)
(b) Prejudice and myths
Participants described false and misleading information being considered as true.
‘The application can teach type 1 diabetics about how to live their love life with their diabetes. Most of them are ashamed to tell […] their partners. Some people didn’t go to school or don’t know much about diabetes, they think that the person can contaminate them.’ (P6)
(c) Lack of knowledge on Web 2.0
One participant referred to gaps in digital knowledge and limited trust in technology.
‘I’ve seen some [diabetes self-management application] on Google Play but it requires a subscription; they are being connected to your bank account and they draw money from it. I was […] scared of hackers, I abandoned the idea of subscription.’ (P15)
The third theme refers to information provision and immediate guidance in case of disease complications in order to prevent inadequate behaviour in stressful situations. No subcategory was found here.
‘The application should teach us how to behave once you have hypos or highs because sometimes you become stressed which can raise your blood sugar levels more.’ (P12)
Theme 4 refers to the continuous monitoring of disease-specific (medication, physical activity, nutrition) parameters to be facilitated by the app. A second subcategory refers to reminder functions.
(a) Blood glucose or sugar recording and trend visualisation
The subcategory refers to digital monitoring and display of changes in diabetes parameters.
‘Another thing I wish the application to offer would be a kind of diary to record the results of our blood glucose, A1c, blood pressure and body weight checking. A diary in which we can write possible mistakes, which may have caused the results of these health check-ups to be high or low compared to the normal values.’ (P2)
(b) Reminder functions
Participants wish for automated reminders for appointments, physical activity, insulin use and food intake.
‘The application can remind me to check my blood sugar and to take my insulin injection […] and to exercise. It should also remind me of my doctor’s appointments.’ (P13)
The theme refers to information provision on food and drink choices as well as alcohol intake. Four subcategories were found.
(a) Composition of a diabetic plate
Participants expressed a need for information on the kind of food being complementary with the disease.
‘I wish the application to teach me what quantity of which food to put on my plate and the content […] in terms of glucose and other nutrients.’ (P3)
(b) Information on nonalcoholic beverage choices
This subcategory refers to diabetes-appropriate choices of beverages: ‘[…] for example, I personally like soda very much and after I was diagnosed with diabetes I had to stop [drinking] it and whenever I used to pass by shops […] I felt my heart aching remembering that I couldn’t drink [sodas] anymore. But is it true?’ (P7)
(c) Information on alcohol intake
This subcategory refers to information on the acceptable kind and amount of alcohol, as well as possible interactions of insulin with alcohol.
‘I wish to have a special page about beers diabetics can drink […]. Or a page on how to still enjoy life besides having diabetes, because some people […] [think] that beers and medications should never be mixed.’ (P18)
(d) Pleasure of eating
This subcategory refers to dietary food intake and the consequences for pleasure while eating. For instance, participants report that they ‘hate to always drink water’ (P11), or refuse to go to parties because they cannot drink soda.
‘Maybe the application can also give us tips on how to enjoy our food, because diabetics are known to always eat bitter.’ (P11)
The theme refers to information on the right kind and amount of exercise, as well as to motivational input for uptake and maintenance of physical activity.
(a) Kind of sport to do
The first subcategory refers to the kind of physical activity for people living with diabetes.
P17: ‘The application can teach us about acrobatic games that are safe for diabetics. I used to be a player of acrobatic games but when I was diagnosed with diabetes, I stopped it and this frustrates me […].’
(b) Motivation for physical activity
Participants report discouragement and lack of motivation for physical activity. They also ask for continuous support of behaviour change.
‘The doctor told me to exercise at least 40 mins a day, he said I have to walk quickly but I am not able to do so, that’s why I don’t exercise at all.’ (P14)
(c) Frequency and duration of physical activity
This subcategory refers to information on the right amount of physical activity. Participants ask for tracking and performance-based recommendations.
‘Then I decided to exercise twice a week after my job […] but I don’t know if it is enough.’ (P20)
This theme refers to emotionally supportive content and the ability to connect with others suffering from diabetes, easing the burden of disease.
(a) Emotional support
The subcategory refers to supportive content for emotionally distressing situations.
‘I wish the application could give me advice about how to control my emotions (anger, bitterness, stress, sorrow, etc.).’ (P2)
(b) Social support
The subcategory refers to social support when dealing with diabetes. Participants wish to be able to get in contact with other patients with diabetes, for example, in a forum to ‘share goals and dreams’ (P17).
‘Can the application put me in contact with other people for example when I am feeling down so they can help me feel better (a kind of disease partner who is not necessarily sick but who knows diabetes well and who can help me)?’ (P8)
Participants had difficulties imagining possible app functions. However, many referred to interactive information delivery options and the integration of different languages.
(a) Information delivery
This subcategory refers to content to be delivered via text, images, audios and videos.
‘Videos are better, because you can see and understand what the doctor is explaining. At my age, reading may be tricky. I think that having both may be better.’ (P5)
‘Sometimes we cannot even raise our hand when we are in a hypo, so the idea of having an audio would be to instruct us on what to do in case of a hypo crisis. Otherwise you can neither read nor watch a video.’ (P3)
(b) Available languages
This subcategory refers to desired languages to be supported by the app. Participants either wish to include local language, Kinyarwanda, or to also include English.
‘Kinyarwanda is better because even if you think you speak English, you may start reading and be confused with medical or scientific terminology, though you needed to understand everything well.’ (P7) ‘It would be great to have an option to change the language like for Facebook (the application should be both Kinyarwanda or in English for the choice of the use).’ (P3)
According to the qualitative analysis, the following functions were either mentioned by the participants (see above) or can be deducted from their mentioned needs and expectations:
(1) Education provision tool using Kinyarwanda and English (including informational content on disease in general, medication and medication adherence, physical activity and nutrition, and their respective impact on coping with the disease and disease-related complications);
(2) Monitoring system for disease-related para-meters such as HbA1c as well as medication and nutrition intake and amount of physical activity;
(3) Reminder functions based on monitored data, for example, for medication adherence and physical activity behaviour, as well as disease management, for example, appointments with physicians;
(4) Crisis intervention function providing easy-to-access information in case of hyper- and hypoglycaemic events;
(5) Social network function providing access to other patients and self-help groups, in order to offer social support as a coping mechanism for the burden of disease;
(6) Combine written content with images and support it with both audio- and video-based information delivery.
Discussion
The assessment of expectations and needs of Rwandan patients with diabetes will be used to develop the first diabetes self-management smartphone application (Kir’App) for Rwandan patients with T2DM.
Eight main themes were identified: (a) diabetes education and desired information provision; (b) lack of diabetes knowledge and awareness; (c) need for information in crisis situations; (d) required monitoring and reminder functions; (e) information on nutrition and alcohol consumption; (f) information on physical activity; (g) coping with burden of disease; and (h) app features. Table 4 summarizes the study participants’ expectations that will guide the App development (functionalities and content) and table 5 shows the suggested future use of this study results.
Study participants’ expectations guiding the app development: functionalities and content.

Future use of this study’s results.
T2DM, type 2 diabetes mellitus.
Theory-grounded user-centred development
A recent systematic review concludes that mHealth studies for behaviour change in low- and middle-income countries are insufficiently based on behaviour-change theories. 26 Evidence on the HAPA shows that while all patients with T2DM should be presented with means to increase their self-efficacy, support during behaviour-change processes depends on the stage a person is at. 27 Accordingly, our results are discussed in reference to the single predictors and stages included in the HAPA. 18
Risk perception, outcome expectancy and health literacy
Outcome expectancies cover most of the answers received in the semistructured interviews. As indicated in theory, outcome expectancies are said to increase the success rate of coping responses. 28 Outcome expectations and pretreatment self-efficacy predict greater intention to engage in health behaviours, 29 as they allow for carrying out plans. 30 Among the expectations towards the potential smartphone application is a special feature for the provision of education on diabetes in general and coping strategies with disease-related complications. Participants also expect the application to provide response to their lack of knowledge and awareness about coping with the diabetes burden in everyday life, which is often impaired by common diabetes myths and rumours. This is noteworthy as disease-related literacy is an important predictor for risk perception. 31 Furthermore, patients with knowledge deficits or low health literacy are expected to benefit most from mHealth interventions. 32
Health literacy is the basis for a successful self-management, as also stated by Saha and colleagues. 33 This is supported by guidance published by the American Diabetes Association, the American Association of Diabetes Educators, and the Academy of Nutrition and Dietetics. 34 A survey of people in Rwanda revealed that general knowledge and perceptions of T2DM was low, highlighting the need for education campaigns. 5 Therefore, adequate education corresponding to the individuals’ level of heath literacy is needed, even more so as increased health literacy has been shown to improve self-efficacy and therefore coping behaviour in an Iranian sample of diabetes patients. 35
Diabetes self-management, monitoring and crisis intervention
Study participants also wished to have a diabetes self-management application with the capacity to assist them with crisis intervention. By providing information in case of disease complications, such as episodes of low and high blood sugar values, patients can be empowered to prevent wrong behaviour in stressful situations. As for community-based strategies, Gallé and colleagues found proof for benefits from improved diabetes self-management on the management of hypoglycaemic crisis. 36 For diabetic patients enrolled in a telehealth programme, Chen and colleagues found improvement in problem solving through a teleconsultant service. 37 Overall, crisis intervention may refer to recovery self-efficacy, as well as action control predictors of the HAPA. It is well known that during the phase of intention and action planning, coping strategies for potential setbacks need to be included. 18 However, evidence is missing for what conditions are required to maintain a new behaviour and to prevent relapse, as well as how to re-establish the new behaviour after relapse. 38
An automated monitoring system that facilitates continuous monitoring of disease parameters, such as blood glucose tracking, was among the most cited potential features in the present study. In a cross-sectional study by Borges and colleagues, 111 participants were in favour of using continuous glucose monitoring provided it was easy to use and did not produce information overload. 39 Both preconditions support the importance of early-user integration in the design process of the Kir’App. Also, feedback and monitoring are among the most frequently applied behaviour-change techniques in theories applied to mHealth interventions. 26
Along with a monitoring of disease parameters, patients expressed the need for knowledge on behaviours related to everyday life with diabetes, such as foot care, for example. For rural diabetic patients in Montana, Ciemins and colleagues found higher adherence rates for regular foot care when applying a telehealth self-management programme. 40 Such cues to action are important in behaviour-change theories as well, 41 which is why Schwarzer subsumes them under barriers and resources in the HAPA. 18
Participants wish for an application feature that offers specific information on food, nonalcoholic drink choices and alcohol intake to facilitate their daily diabetes-related nutritional choices. The potential of telehealth applications to improve dietary behaviour are, again, supported by Chen et al., 37 as well as by a randomized controlled trial carried out by Fernandes et al. 42 Again, the presented findings support the link between health literacy and self-efficacy. Within theory, task self-efficacy describes the extent to which an individual is convinced to be able to successfully take up a particular behaviour. 43
Enhanced motivation through emotional and social support
In order to comply with diabetes-specific physical activity recommendations, participants expected the application to give them information on the right type, amount of and motivational input for physical activity. This strongly relates to maintenance and recovery self-efficacy during the action planning and action control. 18 Dobson and colleagues found improved patient adherence to diabetes and health behaviours, as well as better HbA1c values when using motivational text messages to support DSM. 44 In the present study, patients expressed their loneliness and they found that it could be addressed by an application feature that offers emotionally supportive content and the ability to connect with other people living with diabetes. This is an especially important contribution, given that Koetsenruijter and colleagues found a strong association between social support by emotional networks (family and friends) and successful diabetes self-management. 45
Our findings are supported by the qualitative results of Desveaux and colleagues calling for a balanced consideration of self-efficacy, competing priorities, previous behaviour change, and beliefs about Web-based solutions. 46
Implications
In a systematic review comparing 55 healthcare systems of sub-Saharan African countries in the management of diabetes, Rwanda was assessed among countries with health partnerships and systematic care that facilitate patient access to diabetes information, care and adherence to treatment. 47 Decentralization, focus on community health and insurance scheme are traditionally seen as strengths for the Rwandan health system. 48 These aspects may be a support to test, evaluate and roll out the innovative self-management application developed in the Kir’App Rwanda Diabetes study project.
The expectations and needs of Rwandan diabetic patients were collected using a strongly user-centred study design. Coresearch, defined as research in partnership with older people, is said to enrich results derived from research based on older peoples’ interpretations of their own lives. 49 This method is said to foster an improved understanding of heterogeneous target populations and presents a promising approach for partnerships at the community level. 50 In addition to the fact that there is no current diabetes app available for Rwandan diabetes patients, qualitative findings from patients in Canada describe how currently available apps inadequately address the needs of patients. 51
Limitations
Qualitative methods such as focus groups or in-depth interviews are commonly used for user-centred design processes in the domain of health technologies. 52 However, the study design, using a semistructured interview guide for qualitative research, has well-known limitations. Although a pretest was conducted, back-and-forth translation from English to Kinyarwanda may have led to misinterpretations or loss of information. Additionally, analysis was theme based and interpretative. Therefore, the individual backgrounds of the researchers may have had an impact on the final results. In order to address this risk of confirmation bias, analysis of data was independently carried out by two of the authors and coding was later supervized by another. 22
As databases for patients with diabetes are missing, convenience sampling in a professional setting, the RDA, was used. Using this method, patients not attending this association at all were missed, or if not attending on a regular basis, were less likely to be included. This especially applies to patients living in rural communities, having limited health literacy (indicated by not visiting the RDA on a regular basis) or those being unaware of their conditions. Although attempts were made to recruit diverse patients, those that refused to take part may have provided additional insights. Therefore, participants of the interviews may be generally more responsive to health services and studies.
Data were collected from 21 individuals, derived from a highly heterogeneous study population (Table 2) in terms of age, sex, time since diagnosis and working status, and cannot be generalized to a larger population.
The study aimed to assess needs and expectations of Rwandan diabetic patients as potential users of the first Rwandan diabetes self-management app. Though specific functions would have been a valuable help to design this first app of its kind in Rwanda, participants may have been overstrained to imagine possible functions, as they never used a comparable app or device before.
Conclusions
The outcomes of this study have provided recommendations that are currently being used to develop the first Rwandan diabetes self-management smartphone application, Kir’App. Kir’App is expected to strengthen the empowerment of Rwandan diabetic patients using smartphone applications in their diabetes self-management capacity. The expectations and needs of patients with diabetes is the strong focus on functions and design of a future smartphone application and is in line with the present call for user-centred development of health interventions. The qualitative insights provide a prototype of the first diabetes self-management smartphone application (Kir’App). The respondents highlight the importance of combining knowledge-oriented components with monitoring functions. They call for connecting their own living with diabetes with both social support derived from peers, as well as regional/national initiatives.
Supplemental Material
INTERVIEW_GUIDE – Supplemental material for Assessment of Rwandan diabetic patients’ needs and expectations to develop their first diabetes self-management smartphone application (Kir’App)
Supplemental material, INTERVIEW_GUIDE for Assessment of Rwandan diabetic patients’ needs and expectations to develop their first diabetes self-management smartphone application (Kir’App) by Claudine B. Kabeza, Lorenz Harst, Peter E. H. Schwarz and Patrick Timpel in Therapeutic Advances in Endocrinology and Metabolism
Footnotes
Appendix
Summary of recurrent themes and subcategories with examples.

| Theme | Subcategory | Examples |
|---|---|---|
The theme refers to the provision of information, specialized education on diabetes in general and coping with the disease |
(a) General information on diabetes, management and complications This subcategory refers to information that should be provided by the app in order to close general knowledge gaps on disease characteristics, management (through medication and behaviour change) and complications |
|
| (b) Medical parameters (e.g. blood pressure, blood glucose, HbA1c, weight, etc.) |
||
| (c) Devices |
||
| (d) Frequently asked questions by newly diagnosed patients |
||
| (e) National/regional update and initiatives, as well as services |
||
| (a) Lack of knowledge on living with diabetes |
||
| (b) Prejudice and myths (social media knowledge) |
||
| (c) Lack of knowledge on Web 2.0 |
||
| (a) BG/BS recording and trend visualization |
||
| (b) Reminder functions |
||
| (a) Composition of a diabetic plate |
||
| (b) Information on nonalcoholic beverage choices |
||
| (c) Information on alcohol intake |
||
| (d) Pleasure of eating |
||
| (a) Type of sport |
||
| (b) Motivation for physical activity |
||
| (c) Frequency and duration of physical activity |
||
| (a) Emotional support |
||
| (8) App features |
(a) Information delivery |
|
| (b) Available languages |
BG, blood glucose; BS, blood sugar; HbA1c, glycated haemoglobin; IT, information technology.
Acknowledgements
The authors wish to thank the Rwanda Diabetes Association for facilitating the process of the research. We also thank Rwandan diabetes patients for participating in our study and for providing rich insight. The authors also wish to thank Kristin Kemple for her linguistic editing.
Author Contributions
CK and PS contributed to the initial conceptual planning of the project and design of questionnaire. CK researched data. CK, PT and LH contributed to the analysis and interpretation of data. PT and LH contributed to the discussion, reviewed and edited the manuscript. CK, PT and LH wrote the manuscript. PS approved the version to be published.
Funding
This work was supported by the Ministry of Education of Rwanda and the German Academic exchange service (DAAD).
Conflict of interest statement
The authors declare that there is no conflict of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.