
Abstract
Early glycaemic control leads to better outcomes, including a reduction in long-term macrovascular and microvascular complications. Despite good-quality evidence, glycaemic control has been shown to be inadequate globally. Therapeutic inertia has been shown present in all stages of treatment intensification, from the first oral antihyperglycaemic drug (OAD), all the way to the initiation of insulin. The causes and possible solutions to the problem of therapeutic inertia are complex but can be understood better when viewed from the perspective of the providers [healthcare professionals (HCPs)], patients and healthcare systems. In this review, we will discuss the possible aetiologies, consequences and solutions of therapeutic inertia, drawing upon evidence from published literature on the subject of type 2 diabetes.
Keywords
Introduction
Diabetes is a common chronic condition affecting 425 million people worldwide in 2017, with 79% of cases occurring in low- and middle-income countries. 1 The prevalence is estimated to increase to 629 million by 2045. The disease affects 8.3% of adults across the world, with the greatest number of people suffering between the ages of 40 and 59 years. 1 Additionally, diabetes costs public health approximately 727 billion US dollars globally, and accounts for 4 million deaths. Type 2 diabetes mellitus (T2DM), which accounts for 90% of diabetes, is a progressive disease characterized by B-cell dysfunction and insulin resistance and without adequate control, can lead to macrovascular and microvascular complications. 2
There is good evidence that early glycaemic control leads to better outcomes, including a reduction in long-term macrovascular and microvascular complications. 3 Even though the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial was unsuccessful in showing any benefits of early tight glycaemic control, the UK Prospective Diabetes Study (UKPDS) Post Trial Monitoring Study, comprising 5102 individuals, indicated a legacy effect, where intensive control of glycated haemoglobin (HbA1c) from the initial diagnosis led to a significant decrease in the risks of both myocardial infarction [MI; 15% risk reduction, (0.74–0.97) and death from any cause 13% (0.79–0.96) reduction]. 3 Furthermore, the ADVANCE trial randomized 11,140 individuals to an intensive control group aiming for a target HbA1c ⩽ 6.5% (48 mmol/mol) with additional antihyperglycaemics, compared with a routine glycaemic-control group. The study showed a lower mean HbA1c in the intensive group (6.5%) compared with the normal control group (7.33%) after 5 years’ follow up. There was also a significant reduction in combined major macrovascular and microvascular complications in the intensive control group compared with the control group [18.1% versus 20.0%, hazard ratio (HR) = 0.90; 95% confidence interval (CI): 0.82–0.98] along with a reduction in major microvascular events (9.4% versus 10.9%, HR = 0.86; 95% CI: 0.77–0.97), principally due to a reduction in cases of nephropathy. 4 The Glucose Control and Vascular Complications in Veterans with Type 2 Diabetes (VADT) study similarly showed a reduction in HbA1c in the intensive study group (6.9%) compared with the normal control group (8.4%) and a significant risk reduction in the primary outcome in the intensive group compared with the standard therapy group (HR = 0.83; 95% CI: 0.70–0.99).5,6 A meta-analysis of these four cardiovascular (CV) trials (ACCORD, UKPDS, ADVANCE and VADT) showed a 15% reduction in MI (HR = 0.85; 95% CI: 0.76–0.94) and a 9% reduction in CV events (HR = 0.91; 95% CI: 0.84–0.99) conferring the benefits of tight glycaemic control. 7
Despite good-quality evidence, glycaemic control is shown to be inadequate globally. Guidelines suggest an ideal individualized target HbA1c level for most people with T2DM to be <7% (53 mmol/mol), using metformin as first-line pharmacological treatment at diagnosis along with lifestyle changes. The recommended HbA1c target for people with T2DM without comorbidities is 6.5% (48 mmol/mol), and if levels remain above this value, additional oral antidiabetic (OAD) agents may be added. If, however, after additional medications, the HbA1c levels are still >7.5% (59 mmol/mol), further advances in therapy are recommended, including insulin. 8 In addition to this, the American Diabetes Association (ADA) standards of care contain an algorithm of which medications to use as add-on therapy once metformin has been started, along with guidelines advising HbA1c review after 3–6 months post commencement of a new medication. 9 Glycaemic control should then be monitored 3–6 monthly subsequently. Furthermore, the new European Association for the Study of Diabetes (EASD)–ADA guidelines released in 2018 have shown an overall approach to glucose-lowering medications for patients with type 2 diabetes and the need to reassess treatment regularly to avoid therapeutic inertia. 10
Despite the evidence and recommendations, the guidelines are not translated into practice. A study showed that a third of patients with T2DM in the UK fail to achieve HbA1c levels ⩽ 7.5% (59 mmol/mol). 11 One of the key reasons for this is therapeutic inertia, previously known as clinical inertia, 12 which is the failure to advance or intensify therapy by a healthcare professional. This review explains the prevalence, causes, consequences and methods to overcome therapeutic inertia in T2DM.
Prevalence of therapeutic inertia
Therapeutic inertia has been shown to be present in all stages of treatment intensification, from the first oral antihyperglycaemic drug (OAD), all the way to initiation of insulin. However, recent data suggest that the problem is escalating, leading to patients poorly controlling their diabetes.13,14 Inertia relating to diabetes management has been shown for over 10 years, with one of the first studies conducted by Shah and colleagues in 2005 showing less than half of the 2502 patients with T2DM and high HbA1c having intensification of their treatment. 15 A recent retrospective cohort study showed that on average, in patients with HbA1c levels above 7% (53 mmol/mol), it took 3 years to intensify treatment from one to two OADs. 16 Fu and colleagues also demonstrated a median time to intensification of treatment of 14 months in US clinical practice, for patients to receive additional antihyperglycaemic medication. 17
A further study conducted by Mata-Cases and colleagues showed that therapeutic inertia was seen in 26.2% of the patients who had an HbA1c ⩾ 7% (53 mmol/mol) and 18.1% of the patients with an HbA1c ⩾ 8% (64 mmol/mol), and failed to have intensification of medications after a median follow up of 4.2 years. 18 A further retrospective cohort study of more than 80,000 people also demonstrated the phenomenon of inertia. Intensification of treatment with an additional antihyperglycaemic in those taking one OAD took 2.9 years in those with a HbA1c ⩾ 7% (53 mmol/mol), 1.9 years in those with a HbA1c ⩾ 7.5% (58 mmol/mol) and 1.6 years in those with a level ⩾ 8.0% (64 mmol/mol). In those taking two OADs, intensification took over 7.2 years in those with an HbA1c > 7% (53 mmol/mol) and 6.9 years in those with a level of 8%. Additionally, this study showed the median time to intensify treatment with insulin was similar, with >7.1, >6.1 or 6.0 years taken to intensify for patients taking one, two or three OADs, respectively. 19 Another study of over 17,000 patients in 10 countries showed patients remaining on OAD therapy with a delay in insulin initiation. Patients in the study had a mean HbA1c of 8.9% (74 mmol/mol) at basal insulin initiation. After 24 weeks of insulin therapy, there was a significant reduction in HbA1c, with a mean value of 7.5% (58 mmol/mol) (p < 0.001) although the dose of basal insulin remained much lower than seen in randomized controlled trials.
The DUNE study further demonstrated inertia, with only 27.4% of individuals across 28 countries achieving their personalized HbA1c targets after 12 weeks. 20 The Guidance Adherence to Enhance Care (GUIDANCE) study of 7597 patients in eight European countries showed that HbA1c values were being assessed annually, with 97.6% of tests recorded correctly in the previous 12 months. 21 However, the study showed that 46.4% of individuals did not meet target values, having an HbA1c ⩾ 7% (53 mmol/mol).
A recent systematic review of 53 studies demonstrated that most studies had a median time to treatment intensification in those with a HbA1c level above target of more than 1 year, and also confirmed that the extent of therapeutic inertia increased as the number of OADs increased. 22 These consistent results show that therapeutic inertia is a major burden, and affects not just patients’ glycaemic control, quality of life and symptoms, but also the cost to the healthcare systems, as diabetes is not being managed appropriately, leading to further macrovascular and microvascular complications.
Causes of therapeutic inertia
The causes of therapeutic inertia are complex and can be attributed to providers [healthcare professionals (HCPs)], patients and system barriers.
Provider level
Provider-level barriers make up 50% of the causes of inertia. 23 These include difficulties such as time constraints, competing demands, lack of knowledge and variations in guideline recommendations. In addition, HCP factors include perceptions to side effects and inexperience in the management of the condition. 24
There are many barriers related to insulin initiation, intensification and titration. One major concern for inertia is the fear of hypoglycaemia. One study reported that 75.5% of HCPs stated the risk of hypoglycaemia as a barrier to insulin therapy. 25 Insulin therapy is also delayed due to concerns with weight gain and the effect on quality of life by HCPs, with the medication therefore being used as a last resort. Additionally, HCPs may not be experienced in initiating insulin medication, or may not have the resources or skills to educate patients on insulin titration. One study demonstrated that at initiation of insulin, mean HbA1c was 9.5% for those on one OAD, 9.6% (two OADs), 9.7% (three) and 10.1% (four). 26 Another study demonstrated intensification inertia, showing that the median time from initiation of basal insulin to intensification was 3.7 years. 13 Zafar and colleagues also stated other provider-level barriers, including HCP perceptions that glycaemic control is improving, along with communication and ethnic differences between HCPs and patients. 24 Finally, barriers such as fear of weight gain and hypoglycaemia, along with fear of pain from injections and blood tests are attributed more to physician fears compared with patient fears. 27
Patient level
It has been estimated that approximately 30% of therapeutic inertia can be attributable to patient-level barriers, such as concerns over side effects, misunderstanding of treatment regimens and multimorbidity. 28 One survey stated problematic hypoglycaemia as a major factor explaining why the uptake of insulin therapy was low. Adherence to insulin regimens has also been reported as a problem, along with other concerns such as trypanophobia (the fear of needles) and injection-related anxiety, fear of self-monitoring, changing doses of insulin accordingly and psychological resistance to insulin, including anxiety and depression. 29 Pain from injections and blood tests is also a reason for noncompliance with insulin therapy; however, studies have demonstrated that this is due to provider barriers rather than patient-level barriers. 27 One study found that 25% of patients prescribed insulin suffer from ‘psychological insulin resistance (PIR)’ and may refuse treatment, with another study reporting strong PIR in 28.4% of patients and moderate PIR in 61.2%.30–32 Additionally, dietary noncompliance, socioeconomic status, acute intervening illnesses and terminal illnesses are patient-level barriers that may be difficult to address but need managing nonetheless, along with a lack of patients’ understanding of their condition. Patients sometimes also feel discouraged and frustrated, leading to discontinuation of their medication due to prolonged use, along with the failure to reach target glucose levels. 33
System level
System-level barriers are estimated to make up the last 20% of causes of therapeutic inertia. 23 These include healthcare issues and costs of new medications, including differences between healthcare settings. 34 The availability of medications in some cases is also limited. The Prospective Urban Rural Epidemiology (PURE) study showed that even cheap essential medications such as metformin and sulphonylureas are not available in many low- and middle-income countries. 35 Metformin was only available in 64.7% of pharmacies in low-income countries and less than 89% of pharmacies in upper- and lower–middle-income countries. The study also demonstrated that only 29.6% of individuals in low-income countries with a diagnosis of diabetes use medications for their conditions. Therefore, inadequacy of healthcare systems in many regions of the world are a major barrier that needs to be addressed. This also includes the differences between healthcare systems, along with the availability of specialist nurses, early diagnosis and management, and psychological support. It is vital that these services are reformed to help address the poor control of diabetes. 36 Other healthcare-system-related factors include poor care plans and lack of individualized guidelines for patients. 37 Insurance coverage, government-based plans such as the National Health Service and Medicare and copayment discrepancies between pharmaceutical companies also cause the cost of medications to increase and therefore cause further issues in supplying and prescribing these medications, therefore compromising patients’ HbA1c. 33
Consequences of therapeutic inertia
T2DM is a chronic, progressive condition. In the context of T2DM, inertia causes various difficulties leading to poor management of diabetes, higher levels of HbA1c and therefore increased complications along with a reduction in life expectancy. Long-term elevation of HbA1c is associated with microvascular complications such as retinopathy, neuropathy, including gastroparesis and bladder dysfunction, and nephropathy, including proteinuria and microalbuminuria, and eventually macrovascular complications. 38
Better glycaemic control leads to microvascular and macrovascular benefits, and studies have shown that early tight control leads to longer-term maintenance of glycaemic control. The Efficacy and Durability of Initial Combination Therapy of Type 2 Diabetes (EDICT) study showed that early intensive therapy in newly diagnosed T2DM was more effective than conventional therapy. 39 The study demonstrated that triple therapy with metformin, pioglitazone and exenatide was superior to conventional stepped therapy with metformin followed by addition of sulphonylurea and insulin glargine. There was a significant reduction in HbA1c in those receiving triple therapy (5.95%) compared with conventional therapy (6.5%, p < 0.001). Additionally, even with the greater reduction in HbA1c in the triple-therapy group, the rate of hypoglycaemia was 7.5-fold lower than the conventional group, showing the benefits of early combination therapy. HCPs therefore need to ensure that individuals are managed aggressively from diagnosis, especially if HbA1c is more than 1% above the agreed individualized target, since most monotherapeutic approaches will seldom lead to reductions of more than this. 10
Therapeutic inertia leads to a reduced likelihood of achieving target levels later in the disease trajectory. Mauricio and colleagues demonstrated in a study of more than 40,000 patient electronic records, that failing to achieve HbA1c targets of ⩽7% (53 mmol/mol) at 3 months of initiating basal insulin was associated with the risk of not achieving target after 24 months. This prolonged hyperglycaemic burden is therefore associated with microvascular and macrovascular complications. 40
Therapeutic inertia has been associated with a reduced quality of life for the patient, along with increased risks of morbidity and mortality. Osataphan and colleagues demonstrated significantly reduced time to progression of diabetic retinopathy in a population who did not have inertia compared with those who did. 41 There was also a higher incidence of retinopathy progression in the inertia group with 10 cases per 1000 person-months compared with 2.2 cases in the noninertia group (p = 0.003).
Continued therapeutic inertia can eventually lead to macrovascular complications. It is a significant factor contributing towards failure to implement national and international guidelines and may be responsible for approximately 80% of cardiovascular events. 42 One recent study based on over 100,000 patients with newly diagnosed type 2 diabetes showed that therapeutic inertia was prevalent in 26% of patients with a HbA1c ⩾ 7% (53 mmol/mol). Additionally, it showed that there was a significant increase in macrovascular complications including MI (67% increase), heart failure (64%), stroke (51%) and CV events (62%) in patients who had a delay in intensification with OADs or insulin for more than 1 year and who persisted to have a HbA1c > 7% compared with those who were intensified. 43 Finally, a major consequence of inertia is the additional cost on healthcare systems and public health due to the deterioration of patients who suffer from additional complications. 37
Methods to overcome therapeutic inertia
Systematic review of evidence suggests early management and improved glycaemic control reduces complications and therefore there is a need in overcoming therapeutic inertia to improve longer-term outcomes. There are various approaches to overcoming inertia in diabetes. These, again, can be split into the different categories.
Provider level
Table 1 summarises the ways to overcome therapeutic inertia at the provider level (a-f). HCPs can self-critique their performance and self-educate about diabetic therapy and the risks of hyper- and hypoglycaemia, along with following guidelines in the management of the disease. 44 As previously stated, the ADA Standards of Care Treatment Algorithm has step-by-step guidance on how to initiate and add on therapy for patients with diabetes. 9 Additionally, the ADA–EASD Consensus Report gives an overall approach to glucose lowering in T2DM, stating that to avoid inertia, assessment and modification of treatment is necessary every 3–6 months. 10 Guidelines similar to these should be produced and available worldwide to reduce the poor control of T2DM globally. As stated previously, early intensification increases likelihood of glycaemic control. Another recent study showed how early treatment intensification is associated with a shorter time to subsequent glycaemic control. 45 The probability of achieving glycaemic control was 22% higher for the early-intensification group (<12 months taken for intensification) compared with the intermediate group (12–<24 months) and 28% higher for the early group compared with the late-intensification group (24–<36 months). Early intensification therefore needs to be translated into practice globally.
Studies reporting methods on how to overcome therapeutic inertia at the provider level.

See supplementary file for full references.
Proactive approaches with patients are also shown to be beneficial, as patients respond better when they believe they are contributing to a positive outcome. 30 Therefore, building the HCP–patient relationship and giving support to patients is vital for tight glycaemic control. The use of practice nurses and pharmacists in the management of the disease has also been proven beneficial, and frees up general practitioners’ (GPs) time for other aspects of their consultations with patients. 46 Moreover, education is one of the key techniques for reducing inertia, by educating not just HCPs but also students at earlier stages of both undergraduate and postgraduate levels. By teaching these professionals and students early on in their career paths, one can convey an increased awareness of inertia and therefore reduce the long-term consequences. In addition to education, up-to-date information about new medications, including efficacy and adverse reactions, needs to be available continuously for HCPs worldwide, along with, as Omebah and colleagues stated, ‘a readily accessible central resource, for example, the ‘Wise List’ in Sweden.’ 47 A resource such as this would help maintain clear guidance to providers and increase confidence levels in prescribing medications for T2DM.
With regards to insulin inertia, trained nurse practitioners may be effective HCPs to help overcome the problem. Seidu and colleagues demonstrated how HbA1c levels can be managed and reduced by multicomponent strategies. 48 This involves using multidisciplinary team members such as dieticians, pharmacists and nurses to help address patients’ needs and issues regarding their conditions. Various studies showed how diabetes specialist nurses, and HCPs interested in diabetes can help with management strategies. Nurse practitioners are well placed in a practice to help deliver insulin initiation, with ongoing support for patients having concerns or problems. Nurse-led insulin therapy would be acceptable to patients, as firstly it would be an extension of their traditional role of administering injectable therapies. 36 The existing confidence and trust will provide a strong foundation for a therapeutic relationship between nurses and patients. Secondly, nurses may review patients more frequently than GPs. This would help reduce noncompliance and also help GPs use their time more efficiently during their consultations, managing any other concerns patients may have. In addition, there have been trials looking at how clinical pharmacists may be able to contribute to patients with T2DM. 49 The use of the whole multidisciplinary team (MDT) has been shown to have a beneficial effect on patients with poorly controlled T2DM.
Patient level
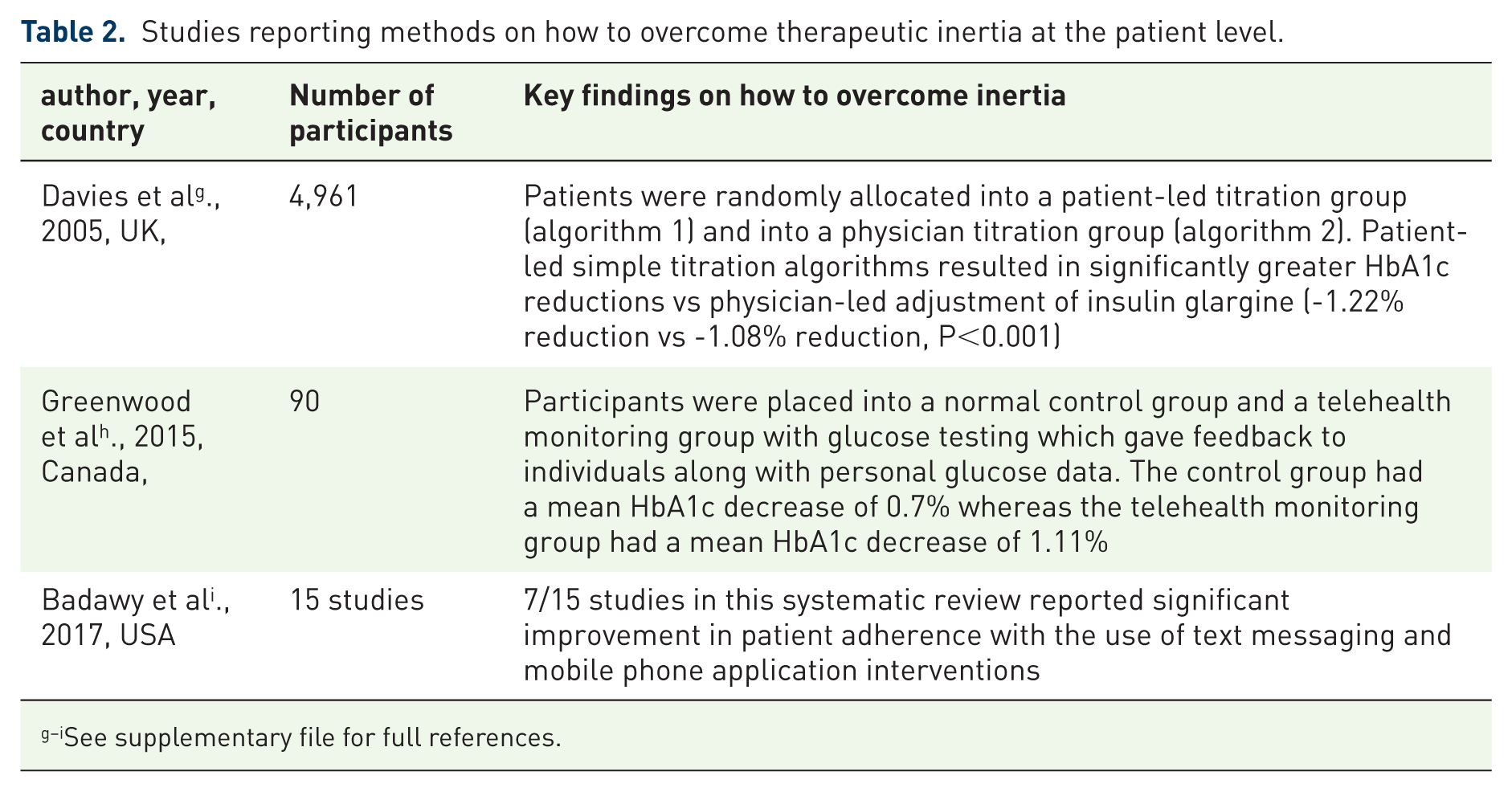
Table 2 summarises the methods of overcoming therapeutic inertia at the patient level (g-i), call–recall systems reminding patients about their appointments are effective methods to help adherence, as well as education on taking medications. Nurse practitioners, as stated above, can help with noncompliance and may also help to reduce anxiety with medication issues, especially with appropriate self-administration of injectables. 36 Other methods include more education on insulin therapy, including titration algorithms for patients, and education to HCPs on initiation and intensification of therapy. Titration algorithms and self-management programmes are paramount to overcoming insulin inertia. New devices with in-built dose-adjustment algorithms have been produced for patients with diabetes, which could help patients self-manage their conditions and reduce time spent with HCPs. Additionally, mobile applications are now being used to help manage diabetics, with in-built blood-glucose monitoring. A recent review showed a significant reduction in HbA1c with the use of diabetes self-management applications. These, at present, are costly; however, if they improve long-term outcomes, they may prove cost-effective options for patients experiencing difficulties in management. 50 Finally, psychological support for patients is necessary to reduce fears and anxiety in those patients not adhering to treatment or for those who need additional support with their condition. 51
Studies reporting methods on how to overcome therapeutic inertia at the patient level.
See supplementary file for full references.
System level
Table 3 summarises the methods of overcoming therapeutic inertia at the system level (j-l). As stated earlier, there is a pressing need to improve services, including those in primary-care settings, globally. One such method in a primary-care setting is by improving the partnership between doctors and practice nurses using a multidisciplinary approach. This would increase the confidence and skills of both, as shown by the Step Up model-of-care trial. 52 This study involved a change in primary care practices, modifying roles of HCPs, demonstrating an increase in insulin initiation (70% versus 22%, 95% CI, p < 0.001). Furthermore, the study showed a higher proportion of individuals reaching target HbA1c in the intervention group (36% versus 19%, 95% CI, p = 0.02) along with a significant reduction of 0.7% in HbA1c in the intervention group (95% CI, p < 0.001). This MDT method is therefore a viable strategy to help reduce healthcare-system barriers. Seidu and colleagues also suggested additional to the integrated MDT approaches and providers adopting a continuous relationship with patients globally; there may also be a benefit in shifting models of care closer to home instead of in specialist units, which should be reserved for emergency admissions from diabetes or complications. 53 These ‘new enhanced models’ would provide a cost-effective alternative which would assist healthcare systems. The article suggests HCPs with an interest in diabetes are crucial in the running of these diabetes services, not only managing patients’ diabetes but also their comorbidities. Regular updates with other members of the MDT about patients’ care would be integrated to the service delivery plan. Finally, further guidelines such as those individualized to overweight and obese patients need to be implemented worldwide in all healthcare systems to help intensify therapy appropriately.
Studies reporting methods on how to overcome therapeutic inertia at the system level.

See supplementary file for full references.
Conclusion
T2DM is an ever-increasing problem for patients and HCPs and the wider economy. There is sufficient evidence that the newer therapies have positive outcomes; however, there is also significant evidence that there are barriers to intensifying therapies appropriately when monitoring indicates poor control. Improving glycaemic control early in the disease trajectory helps to provide a legacy effect in delaying the onset of complications. It is therefore paramount that HCPs facilitate intensification of management in well-informed and empowered patients. One must remain mindful of personalized care plans and know the outcomes of intensification for individual groups of patients; the acceptable targets for a young patient with diabetes and no comorbidities are going to be tighter than those for an elderly patient with multiple comorbidities and polypharmacy. Lipska and colleagues demonstrated how intensification in the second group is likely to lead to severe hypoglycaemia, therefore increasing the risk of falls and cognitive dysfunction. 54 In light of this, therapeutic inertia is not just the failure to intensify therapy, but also failure to de-intensify therapy appropriately. 34 Quaternary prevention is required to reduce the risk of treating patients too aggressively, leading to risks of hypoglycaemia. Nonetheless, aggressive treatment in appropriate patients early on in their disease will help to improve their wellbeing and ability to remain active and supporting their families and the economy. Overcoming inertia and reducing HbA1c must be achieved to ensure longer-term benefits for patients with T2DM. We therefore need to ensure that therapeutic inertia is overcome through education, and accept that this is a high-risk phenomenon that impacts adversely on patient care.
Supplemental Material
REFERENCES_FOR_TABLES – Supplemental material for Therapeutic inertia in type 2 diabetes: prevalence, causes, consequences and methods to overcome inertia
Supplemental material, REFERENCES_FOR_TABLES for Therapeutic inertia in type 2 diabetes: prevalence, causes, consequences and methods to overcome inertia by Sachin Khunti, Kamlesh Khunti and Samuel Seidu in Therapeutic Advances in Endocrinology and Metabolism
Footnotes
Author contribution
SK led the writing of the first draft KK proposed the outline of the manuscript and suggested the reference list used for the review article. He participated in the proof-reading of the draft SS participated in the writing of the first draft, refined the format, suggested reference lists and led the submission and response to the reviewers.
Funding
SS and KK acknowledge support from the National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care (NIHR CLAHRC), East Midlands and the NIHR Leicester Lifestyle Biomedical Research Unit.
Conflict of interest statement
KK has acted as a consultant and speaker for Novartis, Novo Nordisk, Sanofi-Aventis, Lilly and Merck Sharp & Dohme. He has received grants in support of investigator and investigator-initiated trials from Novartis, Novo Nordisk, Sanofi-Aventis, Lilly, Pfizer, Boehringer Ingelheim and Merck Sharp & Dohme.
SS has acted as consultant, advisory board member and speaker for Novo Nordisk, Amgen, Sanofi-Aventis, Lilly, Merck Sharp & Dohme, Boehringer Ingelheim, AstraZeneca and Janssen, NAPP and Novartis. He has received research grants Jansen.
Ethical Approval
Ethical approval was not required for this review.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.