
Abstract
Background:
Information is inconsistent regarding the clinical role of acute elevations of blood glucose level secondary to hospital-acquired infections in nondiabetic critically ill patients during an intensive care unit stay. In this study we investigated the clinical significance of hyperglycemia related to new episodes of ventilator-associated pneumonia in nondiabetic critically ill multiple trauma intensive care unit patients.
Materials and Methods:
We analyzed the clinical data of 202 critically ill multiple trauma patients with no history of previous diabetes who developed a new ventilator-associated pneumonia episode during their intensive care unit stay. We used a time-from-event analysis method to assess whether acute changes in blood glucose levels that occurred prior to the onset of ventilator-associated pneumonia episodes had a different prognostic significance from those that occurred during such episodes. Glucose levels and other laboratory data were recorded for up to 5 days before ventilator-associated pneumonia events and for 5 days following these events.
Results:
Patients who required insulin therapy for persistent hyperglycemia related to a new ventilator-associated pneumonia event had a longer period of intensive care unit stay and a higher intensive care unit mortality rate than patients who did not require insulin for blood glucose control (p < 0.008 and <0.001 respectively). In addition, older age, administration of parenteral nutrition, and elevated mean blood glucose level parameters on the day following the day of diagnosis of a new ventilator-associated pneumonia episode were found to be independent risk factors for intensive care unit mortality.
Conclusion:
Our study suggests that persistent hyperglycemia in nondiabetic critically ill patients, even treated by early insulin therapy, is an adverse prognostic factor of considerable clinical significance.
Introduction
Acute hyperglycemia, in nondiabetic critically ill intensive care unit (ICU) patients is being increasingly recognized as a marker of a physiological ‘stress response’. The phenomenon of stress hyperglycemia is attributed to a hormonal stress reaction involving release of catecholamines, glucocorticoids, and glucagon, consequent to stress, sepsis or trauma.1,2 Unopposed elevation of these ‘contra-insulin’ hormones leads to an inability of insulin to control the level of blood glucose and to provide an intracellular glucose supply in the physiological range. The previously accepted concept that stress-related hyperglycemia in critically ill medical and surgical patients constitutes a protective physiological response to meet the increased demands of an injury has recently been challenged. 3 Postoperative hyperglycemia (defined as a blood glucose level above180 mg/dl) was found to be associated with a high incidence of surgical site infections (SSIs). 4 Richards and colleagues 5 found that stress-induced hyperglycemia was an independent risk factor for SSIs in nondiabetic orthopedic trauma patients admitted to an ICU. Moreover, the admission preoperative blood glucose level was shown to be a strong predictor of morbidity and mortality in trauma patients who require immediate surgical intervention. 6 Bochicchio and colleagues 7 reported that acute elevation of the blood glucose level to >200 mg/dl in critically ill trauma patients was predictive of new infectious events, including episodes of ventilator-associated pneumonia (VAP) and bloodstream, genitourinary and intra-abdominal infections, and was also predictive of an ultimately poor clinical outcome. On the other hand, in a population of critically ill septic patients, stress hyperglycemia was not found to be harmful and actually correlated with a lower ICU mortality than that found in normoglycemic patients. 8 The two other studies similarly found that severely ill septic patients who were normoglycemic on ICU admission had higher ICU mortality rates than hyperglycemic patients.9,10
In the present study we analyzed the clinical significance of hyperglycemia related to new episodes of VAP and its correction by insulin therapy during the ICU stay of critically ill nondiabetic multiple trauma patients.
Patients and methods
This is a retrospective, single-center study. Soroka Medical Center is a 1000-bed tertiary care trauma level I university teaching hospital located in the city of Beer-Sheva in Israel’s southern Negev region. We retrospectively collected the clinical and laboratory data of all multiple trauma nondiabetic patients who were hospitalized in the general intensive care unit (GICU) at Soroka Medical Center between January 2010 and December 2015. All the clinical data were extracted from an electronic medical record system. The study was approved by the Human Research and Ethics Committee at Soroka Medical Center (RN-0405-15-SOR).
Inclusion criteria
All mechanically ventilated multiple trauma patients aged ⩾18 years with no previous history of diabetes who were who hospitalized in our GICU for more than 72 h and who developed a new VAP event were eligible for inclusion in the study.
Exclusion criteria
Patients who did not have a VAP event during their ICU stay were excluded from the study, as were patients with a known history of type I or II diabetes mellitus; a history of acute or chronic steroid treatment; or a well-documented history of a previous hyperglycemic episode. Patients who were admitted to the GICU with pancreatic trauma or surgery or who stayed in the GICU for less than 72 hours were also excluded from the study.
Variables and measures
In our medical chart review, we recorded the patients’ demographic data and chronic treatment, the presence or absence of comorbid conditions, and the following laboratory findings: blood glucose levels; mean glucose variability; sodium, white blood cells, creatinine blood levels, pH arterial blood; and microbiological data. We also documented the patients’ diagnoses on admission; and their Acute Physiology and Chronic Health Evaluation-II (APACHE-II), Sequential Organ Failure Assessment (SOFA), Therapeutic Intervention Scoring System (TISS) scores. Therapeutic and nutritional data for the first week of the patients’ ICU stay were recorded including the details of insulin treatment, (day of initiation of insulin administration, mean daily insulin dose and duration of insulin administration). The patients’ intra-ICU and intra-hospital mortality data were also documented.
Scores
Severity of critical illness and multi-organ failure was evaluated using the APACHE-II score and SOFA score for each patient within 24 h of ICUs admission. The TISS score was calculated and recorded within 72 h of ICUs admission.
Definitions
Illness severity and presence or absence of multi-organ failure were evaluated using the APACHE-II and SOFA scores recorded within 24 h of ICU admission. The diagnostic criteria for a new VAP episode were based on the guidelines of the Centers for Disease Control (CDC) ventilator-associated events surveillance algorithm, which incorporates clinical parameters (worsening oxygenation, rising temperature and purulent respiratory secretions) and microbiological data (a positive endotracheal aspirate culture of >105 CFU/ml or an equivalent semi-quantitative result).11,12
Insulin protocol treatment, blood glucose measurements and nutritional aspects
In our GICU we use an insulin sliding scale protocol.13,14 The trigger point for initiating a continuous insulin infusion is a glucose blood level of >180 mg/dl measured at least twice over a period of 6 hours. The insulin infusion is begun at a dose of 1–3 IU/h of short-acting regular insulin, and is aimed at maintaining the blood glucose level between 120–180 mg/dl, as measured by our GICU blood gas analyzer. The patients who were treated with insulin received it by continuous infusion. Euglycemia was defined as a blood glucose concentration of less than 180 mg/dl, and hypoglycemia was defined as a documented blood glucose level of less than 60 mg/dl. All the multiple trauma study patients were begun on enteral or parenteral nutrition as soon as possible after admission to the GICU.
Primary endpoint
ICU mortality was defined as the primary endpoint.
Secondary endpoints
ICU and hospital stay were defined as secondary endpoints.
Date matching
To assess whether acute blood glucose changes prior to the development of a new VAP episode differed from those recorded during the episode, we used a time-from-event analysis method. 15 The day of a new VAP episode diagnosis was defined as day ‘zero’. The ICU days before and after the onset of a new VAP episode were designated in relation to day ‘zero’ (e.g. day ‘−1’, day ‘−2’…day ‘+1’, day ‘+2’ etc., see Figure 1). This method allowed us to determine the association between blood glucose levels and the development of a new VAP event. All the laboratory and glycemic control data in the study patients who developed a new VAP episode during their ICU stay were recorded for a period of up to 5 days before the onset of the episode to 5 days after the onset of the episode.

The dynamic changes in blood glucose levels (min, mean, max) before and after new VAP episodes. Note: patients who developed hyperglycemia had significantly higher blood glucose levels during the days when they were being ventilated after diagnosis of VAP than when they were no longer being ventilated (p < 0.001).
Statistical analysis
Distribution of continuous variables was tested, and normally and nonnormally distributed variables are presented as mean ± standard deviation. Categorical variables were analyzed using the Chi-square or Fisher’s exact test, and continuous variables were analyzed using Student’s t test or the Mann–Whitney U test. Multivariate analysis was performed using a logistic regression model with an odds ratio (95% confidence interval; CI). Potential candidate variables were those with p < 0.05 in univariate analysis. All tests were two-sided, and a p-value <0.05 was deemed to indicate statistical significance. Data were analyzed using IBM SPSS 22 (NY, USA) and Epi Info 3.5.1 (CDC, GA, USA).
Results
The clinical and laboratory data of 300 multiple trauma patients were analyzed. Of these, 98 patients were excluded from the study (see ‘exclusion criterion’). A total of 202 multiple trauma critically ill patients with no previous history of diabetes who developed a new VAP episode during their ICU stay were included in the study. After initial retrospective analysis, the 202 study patients were divided into two groups: Group 1 (‘nonhyperglycemic group patients’) consisting of 146 patients who did not developed hyperglycemia during a new VAP episode; and Group 2 (‘hyperglycemic group patients’) consisting of 56 patients who developed hyperglycemia related to a new VAP event.
The patients’ demographic and medical characteristics are presented in Table 1. The patients in Group 2 were older than those in Group 1 (p = 0.02, Table 1). There were no differences in weight, sex, past medical history and chronic treatment between the two study groups.
Patient demographics and underlying conditions.

Data are considered statistically significant when p < 0.05.
ACE, angiotensin-converting enzyme inhibitors; CI, confidence interval; CIHD, chronic ischemic heart disease; HTN, Hypertension; NA, not available; OR, odds ratio; SD, standard deviation.
Patients in both study groups had similar ER and laboratory data parameters on the day of onset of the new VAP episode (Table 2). The Group 2 patients had a more prolonged period of mechanical ventilation while in the ICU compared with the Group 1 patients (p = 0.01, Table 2). Otherwise, the therapeutic management and number of daily glucose measures were similar in both study groups.
Laboratory data and therapeutic management during the ICU stay (mean ± SD, %).

Data is considered statistically significant when p < 0.05.
ER- on admission to the emergency room.
Laboratory data on the day of onset of the new ventilator-associated pneumonia event (day ‘zero’).
White blood cell count.
CI, confidence interval; ICU, intensive care unit; OR, odds ratio; SD, standard deviation; WBC, white blood cells
The Group 2 patients were started on insulin therapy on the day after diagnosis of VAP (see Figure 1) and continued to receive this treatment during the next 11 ± 2.8 days. No hypoglycemic episodes were documented.
The APACHE-II, SOFA and TISS scores within the first 24 h after admission to the ICU were similar in both study groups (Table 3). The Group 2 patients had longer periods of ICU stay and higher ICU mortality rates compared with the Group 1 patients (p = 0.008 and <0.001, Table 3).
Clinical outcome endpoints (mean ± SD).
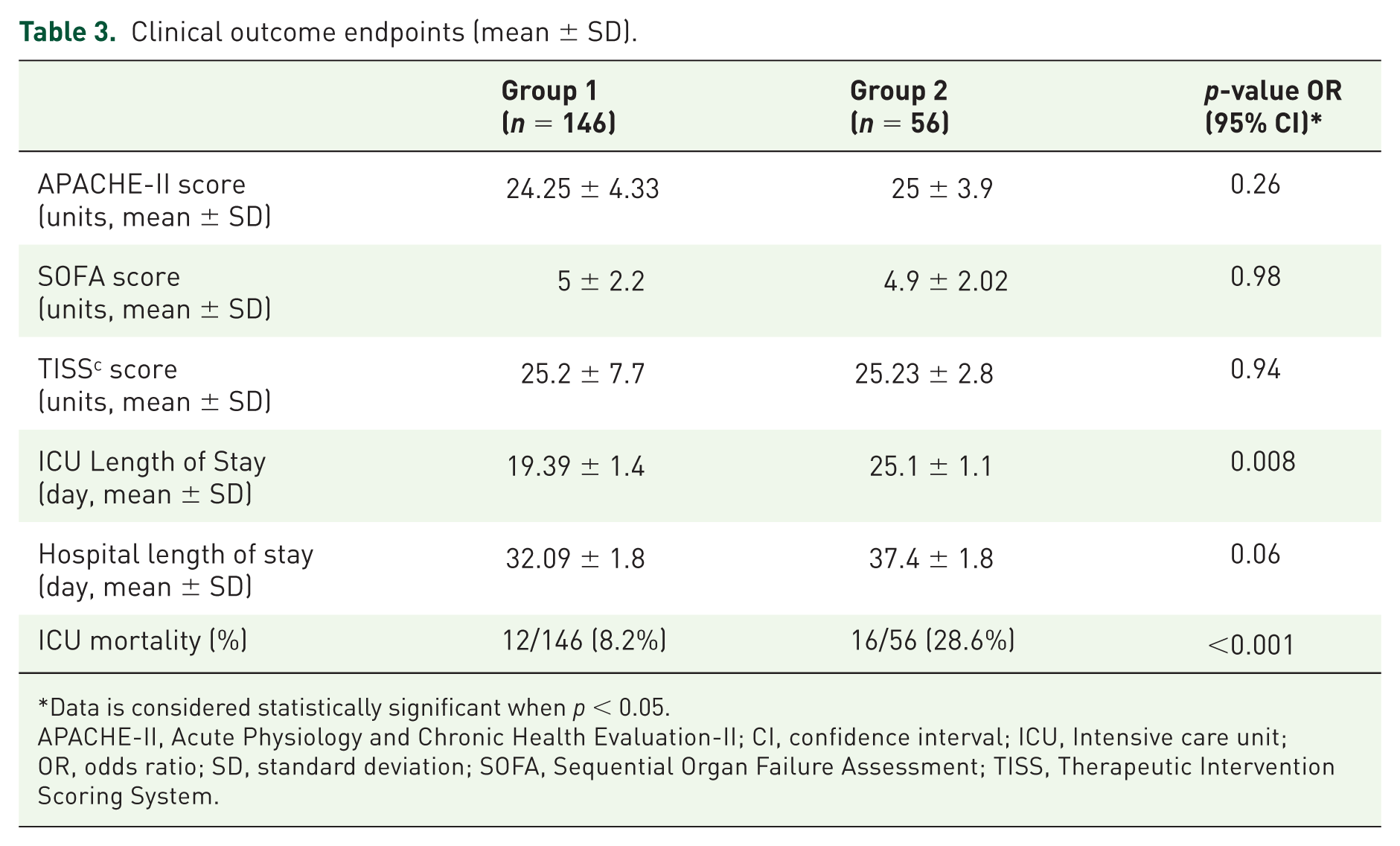
Data is considered statistically significant when p < 0.05.
APACHE-II, Acute Physiology and Chronic Health Evaluation-II; CI, confidence interval; ICU, Intensive care unit; OR, odds ratio; SD, standard deviation; SOFA, Sequential Organ Failure Assessment; TISS, Therapeutic Intervention Scoring System.
Table 4 shows the results of multivariate logistic regression analysis of risk factors for ICU mortality among the multiple trauma critically ill patients with no previous history of diabetes. Older age, administration of parenteral nutrition and elevated mean blood glucose level parameters on the day following the day of diagnosis of a new VAP episode (day ‘+1’) were found to be independent risk factors for ICU mortality.’
Multivariate logistic regression analysis of risk factors for ICU mortality.
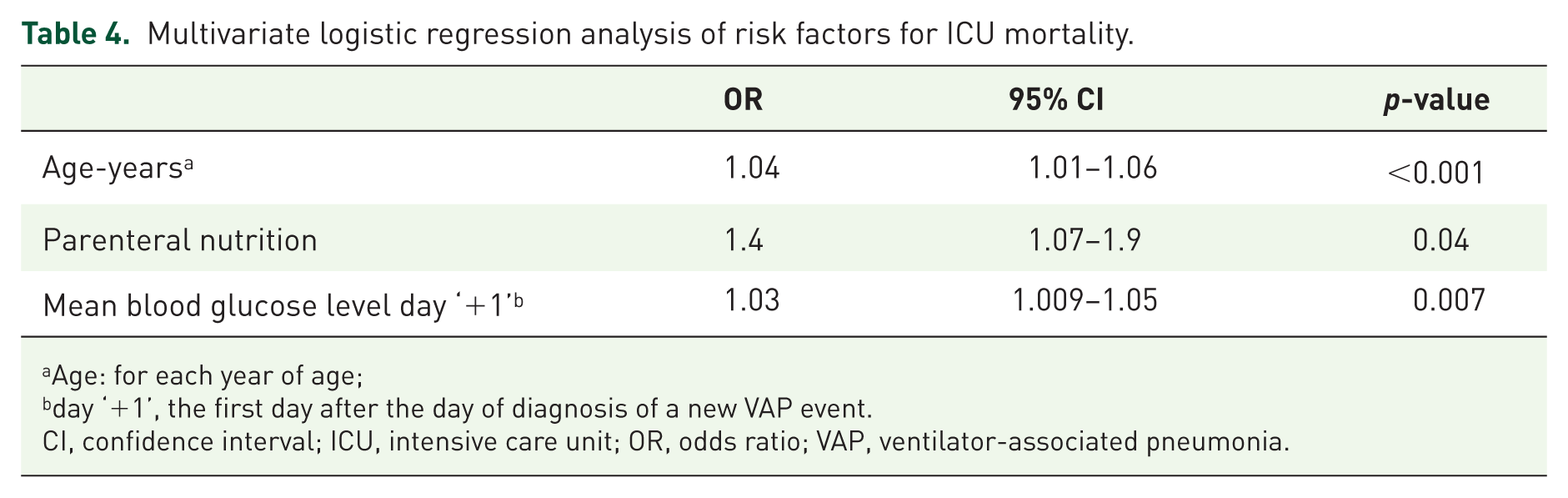
Age: for each year of age;
day ‘+1’, the first day after the day of diagnosis of a new VAP event.
CI, confidence interval; ICU, intensive care unit; OR, odds ratio; VAP, ventilator-associated pneumonia.
Discussion
While acute hyperglycemia in critically ill ICU patients with pre-existing diabetes is known to be an adverse prognostic finding, the clinical significance of high blood glucose levels in nondiabetic ICU patients remains controversial. Currently accepted guidelines4,5,12 regarding acute blood glucose elevations in critically ill ICU patients recommend maintaining the blood glucose level at below 10 mmol/l (180 mg/dl) by continuous insulin administration. A further set of clinical guidelines 14 is relevant in that it was based on an analysis of a mixed population of trauma and nontrauma critically ill diabetic patients. The two additional studies have demonstrated that in critically ill nondiabetic patients with hyperglycemia,6,7,16 high glucose variability5,16,17 and early hyperglycemia are indeed associated with highly predictive of new infectious events and high ICU mortality rates. However, there are still insufficient data evidence that continuous insulin treatment of hyperglycemia might change clinical outcome of nondiabetic critically ill patients during the ICU stay. Similarly, Richards and colleagues 5 demonstrated an association between stress-induced hyperglycemia and SSIs in nondiabetic orthopedic trauma patients.
Mukherjee and colleagues 15 described a finding of increased insulin resistance which preceded the diagnosis of new VAP episodes in nondiabetic trauma patients. In that study 15 all the trauma patients, irrespective of whether or not they developed new VAP events, received continuous insulin therapy from the day of their admission to the ICU. The patients who developed VAP events had lower blood glucose levels than those who did not develop such events; however, the rate of increase in insulin requirement was higher in the trauma patients who developed VAP events. 15 The authors 15 did not present data regarding the patients’ clinical outcome.
In the present study, we restricted our analysis solely to nondiabetic trauma patients who developed acute persistent hyperglycemia related to a new VAP episode during their ICU stay. It is noteworthy that none of the study patients required insulin treatment on admission to the ICU. Subsequently, only the Group 2 patients developed persistent hyperglycemia related to the onset of new VAP episodes and therefore received continuous insulin therapy. Despite receiving constant insulin infusions, the Group 2 patients still had higher mean blood glucose levels both before and after the onset of the VAP episodes than did the Group 1 patients. We demonstrated a higher ICU mortality rate in the critically ill trauma patients with persistent hyperglycemia related to a new episode of VAP who required continuous insulin therapy compared with patients who did not develop VAP-associated hyperglycemia (28% versus 8 %). Importantly, there was no difference between the two study groups in the degree of severity of critical illness on admission to the ICU as determined by their respective APACHE-II and SOFA scores. Additional multivariate analysis demonstrated that older age, administration of parenteral nutrition and elevated mean blood glucose levels on the day following the day of diagnosis of a new VAP episode (day ‘+1’) were independent risk factors for ICU mortality.
The onset of infection tends to increase stress-induced insulin resistance, leading to hyperglycemia.17–19 Moreover, persistent hyperglycemia has been shown to accompany and to precede the diagnosis of VAP.17,19 Continuous insulin therapy for blood glucose control in critically ill patients has been shown to improve clinical outcomes.1,2,11,14 In the present study, irrespective of whether or not continuous blood glucose control was maintained, the ICU mortality rate was significantly higher in the Group 2 patients. Theoretically, persistent hyperglycemia might simply be a marker of the severity of the inflammatory process rather than constituting an isolated and predominant cause of a more adverse clinical outcome. Future studies need to be undertaken so as to better understand the clinical role of persistent hyperglycemia in nondiabetic critically ill patients. Moreover, the question of whether there is need for a continuous insulin therapy protocol in nondiabetic hyperglycemic critically ill patients is still unresolved.
Our study has a number of limitations. The main limitation was its retrospective design. There was no definite evidence that the strategy of distribution and stratification of the data in accordance with the two groups of insulin treatment was precise and optimal. The impact of elevated ICU blood glucose levels on long-term outcomes is unclear because the study did not incorporate follow up of the study patients after hospital discharge.
Conclusion
We showed a higher ICU mortality rate in nondiabetic critically ill trauma patients with hyperglycemia related to a new VAP episode who received continuous insulin therapy than in a comparable group who did not develop VAP-related hyperglycemia. However, the clinical effect of controlling blood glucose levels in critically ill patients by administering a continuous insulin infusion on the mortality rate of these patients is still unclear. Further studies on nondiabetic critically ill patients are required to better understand the clinical significance of persistent hyperglycemia in such patients and to determine whether there is a need to develop a management strategy to control their blood glucose levels.
Footnotes
Acknowledgements
The authors thank Daniel Koyfman, the project and graphical manager, for his kind assistance. Drs Koyfman and Brotfain contributed equally to the paper.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.