
Abstract
Background:
It is necessary to stimulate serum thyroid-stimulating hormone (TSH) levels either endogenously by thyroid hormone withdrawal (THW) or exogenously by administration of recombinant human TSH (rhTSH) for radioactive iodine (RAI) therapy. Thyrotropin alfa (Thyrogen) has many advantages over THW. Radiation dose to laboratory staff while drawing blood for tests on the day 5 is one of the disadvantages of preferring Thyrogen. Our aim was to compare day 3 and day 5 blood test results after Thyrogen injections.
Material and method:
In our study, Thyrogen was preferred in 32 differentiated thyroid cancer patients with a mean age of 50.5 ± 12.3 years. Thyrogen was injected on day 1 and day 2 intramuscularly in all patients before I-131 was given on day 3. A total of 22 patients received 5 mCi RAI for ablation control scintigraphy and 10 patients received 100–250 mCi RAI for ablation or therapy (high-dose group). Blood tests were performed on day 3 and day 5 after Thyrogen injections.
Results:
Mean TSH level was 98.1 mg/dl for day 3 and 29.5 mg/dl for day 5. In the diagnostic group, thyroglobulin (Tg) and anti-Tg levels were nearly the same on day 3 and day 5. In the therapy group, day 5 Tg levels were higher than day 3.
Conclusion:
After Thyrogen injection of two consecutive days, blood sampling might be enough on day 3. Day 5 blood sampling may not be necessary routinely for radiation protection of laboratory staff. For the diagnostic group, if Tg and anti-Tg is normal then 5 mCi imaging may not be necessary.
Introduction
Thyroid cancer is the most frequent type of endocrine cancer and its incidence has been increasing worldwide in recent decades. 1 The standard treatment modality for these patients includes total or near-total thyroidectomy, followed by radioactive iodine-131(I-131) therapy in selected cases and lifelong thyroid hormone suppression. 2 Eradication of normal thyroid remnants with I-131 can result in an undetectable level of serum thyroglobulin (Tg), which can facilitate biochemical follow up. In order to effectively treat differentiated thyroid cancer (DTC) with radioactive iodine (RAI), it is necessary to elevate serum thyroid-stimulating hormone (TSH) levels either endogenously by thyroid hormone withdrawal (THW) or exogenously by administration of recombinant human TSH (rhTSH), Thyrogen (Genzyme Transgenics Corp., Cambridge, MA, USA). Traditionally, thyroid hormone withdrawal for 4–6 weeks has been used to increase serum TSH level which is believed to optimize the trapping and retention of RAI in residual thyroid tissue. 3
Exogenous stimulation with rhTSH is approved for Tg level measurement, for diagnostic RAI scintigraphy in patients with thyroid hormone suppression or before RAI therapy. This offers an alternative to THW by avoiding the morbidity of hypothyroidism. Exogenous stimulation of TSH is associated with better quality of life because it obviates signs and symptoms of hypothyroidism resulting from endogenous TSH stimulation. 4
Thyrotropin alfa (rhTSH) is a heterodimeric glycoprotein produced by recombinant DNA technology. It has comparable biochemical properties with those of the human pituitary TSH. Binding of thyrotropin alfa to TSH receptors on normal thyroid epithelial cells or on well-differentiated thyroid cancer tissue stimulates iodine uptake, organification, synthesis and secretion of Tg, triiodothyronine (T3) and thyroxine (T4).
rhTSH binds to TSH receptors on normal thyroid follicular cells or well-differentiated thyroid cancer cells. Thyrogen is used with a two-injection regimen. A 0.9 mg intramuscular injection to the buttock is followed by a second same-dose injection 24 h later. Oral RAI is given 24 h after the second injection of Thyrogen (on day 3). Whole body scanning and TSH, Tg, anti-Tg blood tests are performed 48 h after the oral RAI. 5 Unfortunately, radiation dose to laboratory staff while drawing blood for laboratory tests on the day 5 is one of the problems for the Thyrogen injection.
Our aim was to compare day 3 and day 5 tests such as TSH, Tg and anti-Tg levels in differentiated thyroid cancer patients after Thyrogen administration. We also want to show day 5 tests after Thyrogen injections, which may not be necessary for routine usage.
Materials and methods
Thirty-two differentiated thyroid cancer patients with a mean age of 50.5 ± 12.3 years were included in our study. Nearly 1 month before, when patients are using levothyroxine (LT4) before Thyrogen injections, all patients’ suppressed TSH, Tg, anti-Tg, free T3 and free T4 levels were measured. We also compared these results after Thyrogen injection blood test results.
For Thyrogen injection, all patients gave verbal consent. Thyrogen was requested for all patients and patients did not stop their thyroid drugs. Thyrogen was injected on day 1 and day 2 intramuscularly in all patients before I-131 was given on day 3 for therapy or for diagnostic imaging. These patients were divided into two groups for I-131 doses. The first group was the diagnostic group and 22 patients were administered 5 mCi for whole body imaging (WBI). The second group was the therapy group and 10 patients were administered high-dose I-131 for therapy. In the therapy group, three patients’ dose was 150 mCi, four patients’ dose was 200 mCi and two patients’ dose was 250 mCi. In one patient, 100 mCi I-131 dose was administered for ablation. Blood tests were performed on day 3 and day 5 after the first injection day of Thyrogen.
On day 5 after Thyrogen injections, there was blood sampling, and whole body scan (WBS) was performed with Siemens E-CAM gamma camera (Siemens Medical Solutions, Illinous, USA). After WBS, single-photon-emission computed tomography (SPECT)/CT (computed tomography) imaging was performed from neck and thorax with the same gamma camera. Imaging results were compared with day 3 and day 5 blood tests.
Day 3 and day 5 TSH and Tg results were compared with paired t tests and the Wilcoxon test with Statistical Package for Social Sciences (SPSS) software version 15 (SPSS, Chicago, IL, USA).
Results
Patient list, characteristics and laboratory results can be seen in Table 1.
Study group and patient characteristics.
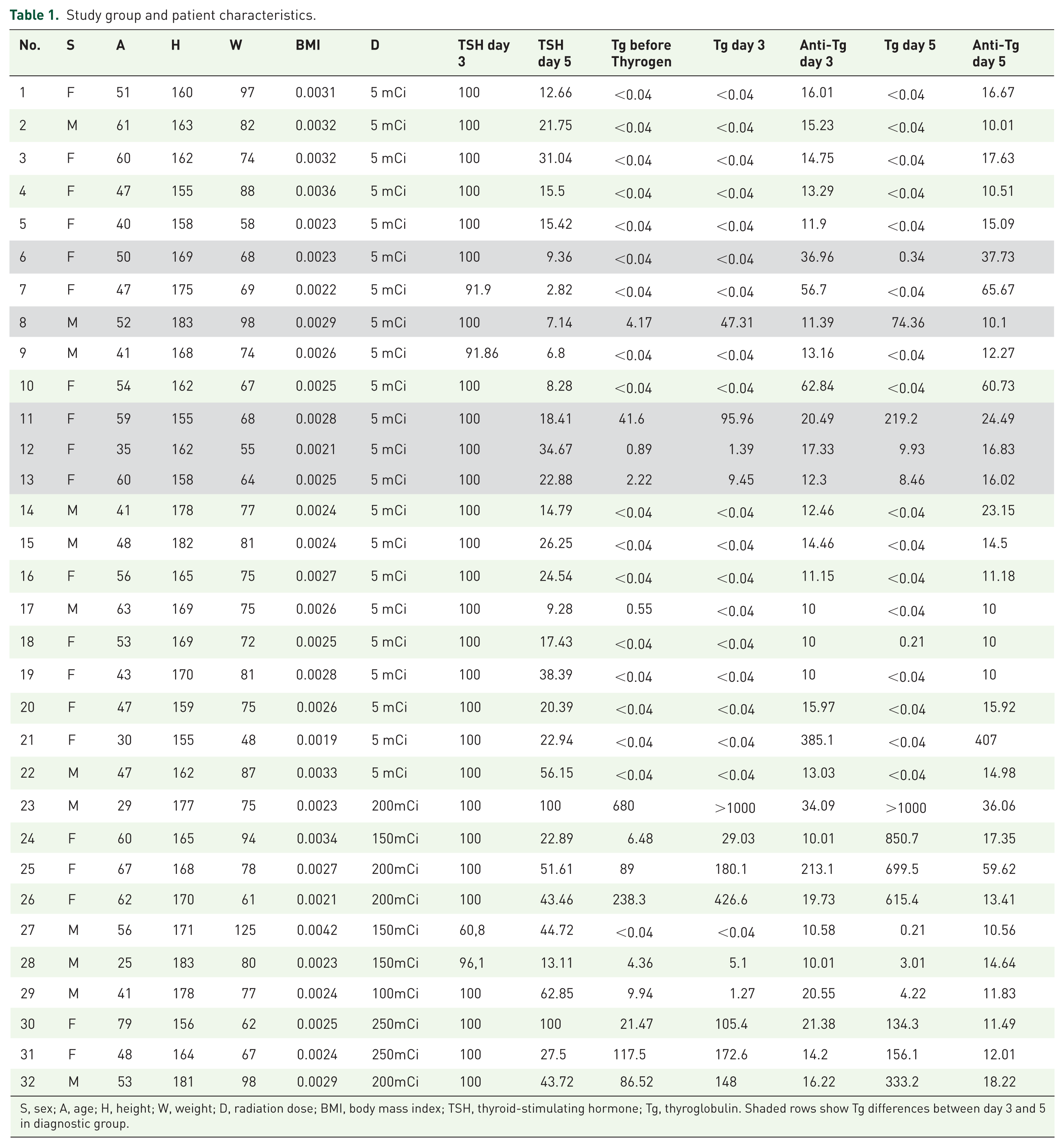
S, sex; A, age; H, height; W, weight; D, radiation dose; BMI, body mass index; TSH, thyroid-stimulating hormone; Tg, thyroglobulin. Shaded rows show Tg differences between day 3 and 5 in diagnostic group.
All laboratory tests were performed with the same standards. TSH levels were elevated after Thyrogen injection, in all patients, as expected. TSH results were greater than 30 mg/dl on the day 3 blood test. Day 3 TSH levels were higher than day 5 levels in all patients because of Thyrogen injection, as expected. The mean TSH level was 98.1 mg/dl for day 3 and 29.5 mg/dl for day 5. When we compare day 3 and day 5 TSH levels after Thyrogen injections, a statistically significant difference between TSH test results (p < 0.005) was seen.
In the diagnostic group, Tg and anti-Tg levels were nearly the same on the day 3 and day 5 blood tests. There were no significant differences between both days’ Tg and anti-Tg levels (p > 0.05). Also, if Tg level was <0.04 ng/ml on day 3, there was no increase on day 5. In the therapy group, day 5 Tg and anti-Tg levels were higher than day 3 Tg and anti-Tg levels. The mean Tg level was 87.3 ng/ml for day 3 and 207.2 ng/ml for day 5 in the therapy group.
In the diagnostic group, 20 patients had negative WBS, but 2 patients had positive scans with increased RAI activity in the neck area due to remnant tissue. In the therapy group, all patients had positive scans in which seven had RAI activity in the neck region and three (patient number 23, 25 and 26) had distant metastatic uptake other than neck (Table 1, Figure 1 and Figure 2).

Whole body 150 mCi I-131 imaging of patients with papillary thyroid cancer on day 5 imaging.

Whole body 5 mCi I-131 imaging of patients with papillary thyroid cancer on day 5 imaging.
Discussion
Radioactive iodine (I-131) therapy has been used in DTC after total thyroidectomy for a long time. It is necessary to elevate serum TSH levels either endogenously by THW or exogenously by administration of rhTSH. Thyrogen can be used like this. Unfortunately, a radiation dose to laboratory staff while drawing blood for TSH, Tg and anti-Tg tests on day 5 after RAI therapy or scintigraphy is one of the main disadvantages of preferring Thyrogen. Radiation safety is an important topic and many guidelines or recommendations demonstrate important issues of radiation safety in nuclear medicine. Medical staff radiation doses have increased over the past decade due to increased need for radiation in medicine, both for therapeutic or diagnostic purposes. 6 In daily nuclear medicine practice, there are many studies to fulfill the basic principles of radiation protection. 7
For DTC patients, following near-total or total thyroidectomy, RAI is administered after TSH level elevation to destroy any microscopic deposits of carcinoma tissue and any remaining normal thyroid tissue. 8 Stopping LT4 and switching it to liothyronine (LT3) for 2–4 weeks, followed by withdrawal of LT3 for 2 weeks, or discontinuation of LT4 for 2–3 weeks without any use of LT3 is the method used for THW. 9 A second method for elevating serum TSH levels is using rhTSH, which can elevate serum TSH levels immediately after intramuscular injection. rhTSH is preferred as an adjunctive diagnostic tool for serum Tg level measurement in patient follow up and for pretherapeutic stimulation.9,10
I-131 Whole body scan (WBS) is used to detect thyroid remnants, regional or distant metastases, and the serum Tg level is preferred for detecting residual or recurrent disease in DTC patients. 9 TSH stimulation is needed to increase iodine uptake for RAI therapy or I-131 WBS. 11 Also, detection of a smaller foci of cancer cells requires stimulation of Tg production by high serum TSH concentrations. 12 In a meta-analysis of randomized-controlled trials, ablation success rates using rhTSH and THW to increase TSH levels in patients with DTC were compared. 13 Tg was measured after rhTSH injection or by THW but different cutoff values were used. Ablation success rates between rhTSH and THW were checked. Tg cutoff value of 1 ng/ml alone or Tg cutoff value of 1 ng/ml plus imaging modality, Tg cutoff value of 2 ng/ml alone or Tg cutoff value of 2 ng/ml plus imaging modality and only a negative 131 I-WBS were accepted as successful ablation control and no significant difference was found between both methods. 11
Although the financial cost of rhTSH is high, preferring rhTSH preserves a better quality of life by preventing side effects of hypothyroidism due to THW, such as fatigue, cold intolerance, weight gain, constipation, depression, cardiac and renal problems.12,14 Also, it is suggested that, impairment of renal clearance during hypothyroidism is prevented and lower radiotoxicity is achieved with preferring rhTSH.15,16 From this point of view, in our study, we preferred using rhTSH in our DTC patients.
While using rhTSH for Tg level measurement, different time schedules are recommended. Weiss and colleagues suggested the highest mean Tg level was achieved more than 48 h after the final rhTSH injection and most patients had a peak serum Tg level 72 h after the second rhTSH injection. 17 Also, it is shown that after rhTSH injection, the mean Tg values continued to increase for 3 days, and declined by day 7. 18 But in our study, we had found no statistical significance between day 3 and day 5 Tg and anti-Tg levels in our low-dose group.
On the other hand, it is also reported that serum TSH level measurement is not necessary for understanding the Tg response with rhTSH due to the quick increase and decrement of TSH levels which does not impact efficacy of rhTSH.18,19 Response of TSH levels shown in our study are also similar to a previously mentioned report. 20 From this point of view, TSH level measurement may be enough on day 3 after the first injection of rhTSH, in selected cases. In our study, we demonstrated that after Thyrogen injection and before RAI administration on day 3, blood sampling is enough for the high-dose group and in many of the cases, sampling is also enough for the low-dose group. It may not be necessary to measure, routinely, Tg on day 5 in those patients with undetectable Tg before stimulation, or those with already-high Tg before stimulation (that would indicate persistent disease). By this protocol, radiation primary protection of laboratory staff can be achieved.
Larger series with more patient populations are needed for routine day 5 blood tests. Also, high- and low-risk groups of DTC patients must be studied prospectively to clarify which day is most appropriate for drawing the Tg level in response to TSH stimulation by rhTSH.
Conclusion
In conclusion, after Thyrogen injections on 2 consecutive days, blood sampling is enough on day 3. On day 5, blood sampling may not be necessary routinely for radiation protection of laboratory staff. Whole body I-131 imaging should be performed on day 5, routinely. For the diagnostic group, if Tg and anti-Tg levels are suspicious, a blood test can be repeated on day 5. For the therapy group, the Tg level is not necessary and TSH level on day 3 might be enough to assess the Thyrogen effect.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.