
Abstract
Background:
Adult growth hormone deficiency (AGHD) is characterized by impaired physical activity, diminished quality of life (QoL), weight and fat mass gain, decreased muscle mass and decreased bone mineral density (BMD). The aim of this study was to evaluate the effects of long-term treatment (7 years) with recombinant human growth hormone (rhGH) on metabolic parameters, body composition (BC), BMD, bone microarchitecture and QoL.
Patients and Methods:
In this prospective study, BMD and BC were assessed by dual-energy X-ray absorptiometry (DXA). Bone microarchitecture was assessed with the trabecular bone score (TBS). The QoL-AGHDA test was used to assess QoL.
Results:
A total of 18 AGHD patients (mean age, 37.39 ± 12.42) were included. Body weight and body mass index (BMI) showed a significant increase after 7 years (p = 0.03 and p = 0.001, respectively). There was a significant tendency of body fat mass (BFM) (p = 0.028) and lean body mass (LBM) (p = 0.005) to increase during the 7 years of rhGH treatment. There was a significant increase in lumbar spine (LS) BMD (p = 0.01). TBS showed a nonsignificant decrease after 7 years of treatment, with a change of -0.86% ± 1.95. QoL showed a large and significant improvement (p = 0.02).
Conclusion:
Long-term rhGH treatment in AGHD patients induces a large and sustained improvement in QoL. Metabolic effects are variable with an increase in LBM as well as in BMI and BFM. There is a positive effect on BMD based on the increase in LS BMD, which stabilizes during long-term therapy and is not associated with a similar increase in bone microarchitecture.
Introduction
The syndrome of adult growth hormone deficiency (AGHD) is characterized by the variable presence of impaired physical activity, diminished quality of life (QoL), increased fat mass, decreased muscle mass and decreased bone mineral density (BMD) [De Boer et al. 1995]. Benefits of treatment with recombinant human growth hormone (rhGH) in AGHD patients have been reported in BMD, body composition (BC) and QoL [Hazem et al. 2012].
Short-term rhGH replacement in AGHD patients has shown an anabolic effect, after an initial BMD decline [Molitch et al. 2011]. After the first 12 months of rhGH treatment some authors reported no improvement and even a reduced BMD [Holmes et al. 1994; Appelman-Dijkstra et al. 2013]. Other studies reported that 18–24 months of GH replacement were necessary to get an increase in BMD [Biller et al. 2000; Bex et al. 2002]. Results from a 15-year study have shown a sustained increase in lumbar spine (LS) BMD with a peak of femoral neck (FN) BMD at 7 years and a following decrease towards baseline values [Elbornsson et al. 2012].
It has recently been reported that in GH-deficient mice, rhGH treatment fully restored bone microarchitecture, with bone partially recovering its mechanical properties [Kristensen et al. 2012]. In humans, the only noninvasive technique to study bone trabecular microarchitecture is the Trabecular Bone Score (TBS), which evaluates pixel gray-level variations in the Dual-energy X-ray absorptiometry (DXA) image [Silva et al. 2013]. TBS has been used to evaluate the impact of short-term rhGH replacement in AGHD patients on bone microarchitecture [Kužma et al. 2014]. Authors found an increase in the TBS score, suggesting a positive effect of rhGH on bone quality. To our knowledge, there are no available studies about the effect of long term replacement on TBS.
Regarding BC, rhGH therapy in ADGH patients has favorable effects, reducing body fat mass (BFM) and increasing lean body mass (LBM) in short and long-term studies [Appelman-Dijkstra et al. 2013; Bravenboer et al. 1996]. It has been found that rhGH replacement improves QoL, but studies have shown a high degree of variability [Reed et al. 2013; Diez and Cordido, 2014]. QoL improvement has neither been observed in all patients nor in all psychological dimensions [Koltowska_Haggstrom et al. 2009; Moock et al. 2009; Spielhagen et al. 2011]. As AGHD is a chronic disease in which GH replacement is recommended to continue for years, long-term studies are mandatory.
The aim of this prospective, open-label study was to evaluate the effect of 7 years therapy with rhGH on BMD, BC, TBS and QoL in a group of patients with AGHD from a single center, followed up in our unit.
Material and methods
Patients
A total of 25 AGHD White patients were invited to participate in the study. A total of 18 of them (9 men and 9 women), voluntarily agreed to participate in this long-term study and signed the consent form. All of them were diagnosed with untreated AGHD, after the age of 18 years, due to a hypothalamic-pituitary disease (seven pituitary adenomas, five craniopharyngiomas, two postoperative, one postirradiation and three idiopathic). Diagnosis of AGHD was confirmed by using an insulin tolerance test (gold standard test) and glucagon test, according to the National Health Service in Spain, which requires two tests. A serum GH value < 5 µg/l at any time during the testing was the criterion for the presence of GHD. All patients also had concomitant pituitary hormone deficits and were receiving adequate stable pituitary hormone replacement therapy, when necessary. Patients with acromegaly or Cushing’s disease were excluded from the study to avoid interference with the BMD value at baseline (because of an excess of GH or cortisol effect).
AGHD patients were treated with rhGH (Genotropin; Pfizer Inc., New York, NY, USA) subcutaneously once a day. They were monitored quarterly during dose titration and then semiannually. Dose titration was based on insulin-like growth factor-1(IGF-1) level with the aim of normalizing the IGF-1 standard deviation (SD) score, clinical response and side effects. When required, if patients had any other pituitary hormonal deficiency, they received adequate and stable therapy and were monitored at every visit. None of the patients died during the study.
Study design
This study was performed in our Endocrinology Unit, Madrid, Spain, between 2001 and 2012. The Ethics Committee of our Hospital approved the study and informed consent was obtained from all the patients. All patients were evaluated at baseline (without treatment) and then at years 1, 2, 3, 5, and 7 of the treatment. The following parameters were assessed at every visit: body mass index (BMI), BMD, BC, TBS and QoL. BMI was calculated as the weight in kilograms divided by the height in meters squared. Also, fasting blood samples were obtained and analyzed for IGF-1. TBS was assessed from previously collected DXA spine images.
Bone mineral density, trabecular bone score and body composition
BMD was assessed by DXA, (densitometer QDR 4500, Hologic, Waltham MA, USA) at LS and FN and expressed in g/cm2. Precision error was less than 1.5%. Values were expressed as absolute values (g/cm2) or T-score, which is the difference of SDs from the sex-matched young healthy subjects. A Spanish Caucasian reference population of the same age and sex was used for calculations [Díaz Curiel et al. 1997]. Diagnoses of osteoporosis and osteopenia followed World Health Organization (WHO) criteria (osteoporosis ⩽ -2.5 SD, osteopenia -1 to -2.49 SD and normal ⩾ -1 SD) [World Health Organization 1998]. BC including BFM and LBM was also assessed by DXA in the same densitometer.
TBS measurements were performed applying retrospectively the TBS iNsight2.0 software (Med-Imaps, Switzerland) to DXA exams. TBS exams were performed by the same author. Lumbar TBS was calculated as the mean value of individual measurements for vertebrae L1–L4. TBS ⩾ 1.35 is considered normal; between 1.20–1.35 is consistent with partially degraded microarchitecture, and ⩽ 1.20 with degraded microarchitecture [Silva et al. 2013].
Quality of life
QoL was assessed using the QoL-AGHDA, a questionnaire designed specifically to evaluate quality of life in adults with GHD. It was validated in a study performed with 356 AGHD patients and 963 patients (reference population) in 37 Spanish hospitals [Badia et al. 1998]. The questionnaire consists of 25 unidimensional items measuring QoL. All the items in the QoL-AGHDA are expressed as unsatisfied needs. A score of 0 indicates absence of problems, and a score of 1 or more indicates the presence of a problem. A high score represents poorer QoL.
Biochemical analysis
Serum samples for biochemical analyses were obtained between 8 and 9 a.m. after overnight fast and immediately kept frozen at -70ºC. Serum levels of IGF-1 were quantified using an automated chemiluminescent immunoassay by Immulite® 2000 Immunoassay System (Siemens, Germany). ImmuliteR IGF-1 is a two-site, solid-phase, chemiluminescent enzyme immunometric assay and is standardized according to the WHO’s 2nd IS 87/518 [Bristow et al. 1990]. Individual IGF-1 values were compared with age and sex values from a reference population.
Statistical analysis
Data analysis was performed with SPPS (version 21.0; IBM, Armonk, NY, USA). Descriptive results are presented as the mean and SD. A normally distributed population was confirmed with the Shapiro–Wilks test. Statistical analysis was performed using the Student’s t-test between baseline and 7-year measurements. We studied the evolution (from baseline to 7 years of treatment) applying MANOVA analysis for repeated measures. Correlations were calculated using Pearson’s test. A p-value < 0.05 was defined as the level of significance.
Results
Baseline characteristics of AGHD patients are shown in Table 1.
Baseline characteristics of AGHD patients.

AGHD, adult growth hormone deficiency; BMD, bone mineral density; BMI, body mass index; IGF-1, insulin-like growth factor-1.
Serum IGF-1 concentration
IGF-1 increased significantly, compared to the baseline, until the end of the study (p = 0.003). A MANOVA test showed a significant tendency to increase (p < 0.001) over the 7 years of rhGH replacement. Similar findings were found in both genders. No correlation was found between IGF-1 and QoL or TBS.
BMI and BC
Baseline BMI was in the overweight range at baseline and increased significantly to 32.07 ± 8.30 kg/m2 after 7 years (p = 0.001) (Table 2). Both male (p = 0.47) and female groups (p = 0.02) showed a significant increase in BMI at the end of the study. A MANOVA test showed no significant evolution in BMI. A MANOVA test showed a significant tendency of BFM (p = 0.028) and LBM (p = 0.005) to increase during the 7 years of rhGH treatment (Table 2). Changes in LBM showed a sustained increase in the total group, from 47.31 ± 11.67 kg at baseline to 52.02 ± 12.41 kg at the end of the study (Figure 1). The female group had similar results with a significant sustained increase throughout the study (p = 0.04). BFM showed a nonsignificant increase from 27.77 ± 12.15 kg at baseline to 31.85 ± 13.93 kg after 7 years of treatment (Figure 2).
Evolution of BMI, BFM, LBM, LS BMD, FN BMD and TBS during the study.

BFM, body fat mass; BMI, body mass index; FN BMD, femoral neck bone mineral density; LBM, lean body mass; LS BMD, lumbar spine bone mineral density; n.s., not significant; TBS, trabecular bone score.
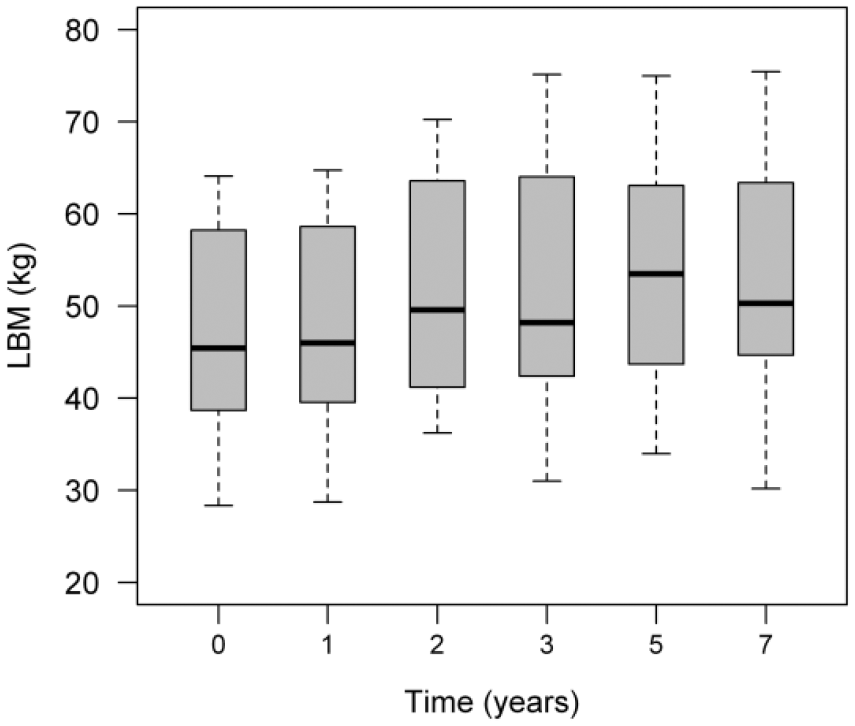
Lean body mass change after 7 years of rhGH therapy (MANOVA, p = 0.005).

Body fat mass change after 7 years of rhGH therapy (MANOVA, p = 0.028).
BMD and TBS
Baseline LS T-scores were in the osteopenia range in the total, male and female groups and FN T-scores, normal in the total and male group, but in the osteopenia range in the female group. LS BMD increased throughout the study, and after 7 years of rhGH treatment there was a significant increase compared to baseline (p = 0.01), with a percentage change of +4.73% ± 2.91. Male and female groups showed no significant differences. During the 7 years of rhGH treatment, FN BMD values tended towards stabilization, without significant improvement in the total, male and female group. A MANOVA test showed no significant tendency in LS and FN BMD (Table 2).
Baseline TBS (1.36 ± 0.11) was in the upper normal range (1.35) in the total, female and male group. TBS showed a nonsignificant decrease after 7 years of treatment (1.32 ± 0.10). Gender differentiated groups showed similar results. No significant correlation was found between TBS and BC or BMD values. A MANOVA test showed no significant tendency over the 7 years of treatment.
QoL
The baseline QoL-AGHDA score was 11.94 ± 6.70. After the first year of rhGH treatment the score showed a large improvement, which lasted until year 7 of treatment (p = 0.02) (Figure 3). A MANOVA test showed a significant temporal tendency (p = 0.03) over the years of the study in the total group, but not in the male and female subgroups. No correlations were found between improvement in QoL-AGHDA score and increase in BLM or in lumbar spine BMD.

QoL-AGHDA score temporal evolution after 7 years of rhGH treatment (MANOVA, p < 0.01).
Discussion
AGHD is a syndrome in which structural pituitary disease or cranial irradiation are recognized in the etiology and therefore, usually occurs in the context of additional features of hypopituitarism. The fact that GH replacement therapy may favorably alter these clinical features provides considerable surrogate evidence for GH deficiency as a major causal factor [Littley et al. 1988].
Most of the recent studies and systematic reviews have reported an increase in LBM, and a decrease in BFM with rhGH long-term supplementation [Gotherstrom et al. 2007; Gibney et al. 1999]. We observed a sustained and significant increase in LBM over the 7 years of treatment. However, our study shows a significant tendency of BFM to increase over the years of treatment. We cannot find a reason to justify the increase in BFM and this could be related to the small population of our study. A previous meta-analysis reported a significant and consistent reduction in weight after long-term rhGH supplementation [Hazem et al. 2012]. On the contrary, a more recent systematic review has shown weight gain [Kristensen et al. 2012; Gotherstrom et al. 2007]. In agreement with this, our results show a significant increase in body weight at the end of the study, compared to the baseline. The mean baseline BMI of our patients was in the range of overweight, and significantly increased after 7 years of treatment, reaching the obese range. Our results support that metabolic risk is increased in AGHD patients, irrespective of long-term substitution with recombinant rhGH [Van der Klaauw et al. 2007].
AGHD is associated with decreased BMD and increased fracture risk [Tritos and Biller, 2009]. In our group, LS T-score baseline was in the osteopenia range for the total group and the male and female subgroups, which highlights the BMD decrease in AGHD patients. An initial transient decrease in BMD had been previously described in the first year of treatment [Tritos and Biller, 2009] but in our results neither LS nor FN BMD showed this decline during the first year of treatment. Several studies reported increase in BMD mainly in LS, after rhGH treatment [Snyder et al. 2007; Appelman-Dijkstra et al. 2014]. Mean LS BMD of our patients was significantly above baseline level after 7 years of rhGH therapy. FN BMD increase has also been reported to a smaller extent than LS BMD [Appelman-Dijkstra et al. 2013]. In our group, FN BMD showed no increase above baseline. A recent article has proposed a decrease and another one a stabilization of FN BMD values during 10–15 years of rhGH treatment [Elbornsson et al. 2012; Appelman_Dijkstra et al. 2014], which is consistent with our results. FN (predominantly cortical bone) may respond less to GH with time than with lumbar spine (rich in trabecular bone). During the 7 years of follow up no fracture was registered, although this was not evaluable given the short number of patients.
At baseline our patients showed mean TBS in the normal range, which, decreased nonsignificantly after 7 years of treatment. In short-term AGHD treated patients, Kužma and colleagues reported a significant increase in TBS after 2 years of replacement, but this increase did not reach normal values and was lower than the increase in BMD [Kužma et al. 2014]. In our study, however, baseline TBS was normal and 2 years after rhGH supplementation there was just a nonsignificant decrease in TBS. Therefore our study does not support a significant positive effect on bone microarchitecture in these patients. IGF-1 is considered to be a positive predictor of cortical bone microarchitecture [Bredella et al. 2012]; nevertheless, in our group, the progressive improvement in IGF-1 values showed no correlation with TBS.
Several tools have been used to assess QoL in AGHD patients. The QoL-AGHDA is a disease-specific QoL assessment questionnaire which has been validated for AGHD patients in Spain [McKenna et al. 1999]. Regarding QoL, KIMS database studies showed improvement within the first year of treatment and subsequent progress towards normalization [Spielhagen et al. 2011]. In our experience, the Spanish version has proven good reliability, internal consistency and construct validity [Sanmarti et al. 1999]. Similar findings in another long-term treated Spanish AGHD population were reported by Cabo and colleagues [Cabo et al. 2011]. Likewise, our results show low health-related QoL at baseline and a large and significant improvement after the first year of treatment, which continues to improve until the end of the study.
The strength of this study is that it provides information on many aspects of the effect of long-term rhGH replacement. Only well characterized AGHD patients were included in the study and none of them discontinued rhGH therapy or stopped the monitoring during the 7 years. Likewise, the study provides bone microarchitecture information, something which, to our knowledge, had never been studied in long-term AGHD treated patients. This study has some limitations like the small population, which limits the statistical power of the study and the lack of a control group, due to ethical reasons.
In conclusion, we have observed that 7 years of rhGH treatment in AGHD patients induces a large and sustained improvement in QoL. Metabolic effects are variable with an increase in LBM as well as in BMI and BFM. There is a positive effect on BMD based on the increase in LS BMD, which stabilizes during long-term therapy and is not associated with a similar increase in bone microarchitecture.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.