
Abstract
Background:
Each year Muslims fast from dawn to sunset for 1 month (Ramadan). In Saudi Arabia, the sleep–wake cycle during Ramadan is severely disturbed and is associated with abolition of the circadian cortisol rhythm, exposing Saudis to continuously increased cortisol levels, which may influence the immune response. In addition to cortisol, sleep and fasting affect the secretion of parathyroid hormone (PTH) and hence bone metabolism.
Methods:
Our objective was to investigate the effect of Ramadan type fasting on secretory patterns of PTH, markers of bone metabolism, and serum immunoglobulins. Blood samples from healthy young volunteers were collected at 9 a.m. and 9 p.m. (± 1 hour) before (Shaban) and 2 weeks into Ramadan. Calcium, phosphorus, magnesium, albumin, alkaline phosphatase, 25-OH vitamin D, intact PTH (iPTH), and immunoglobulin (Ig) A, M and G were measured.
Results:
During Ramadan, evening-adjusted calcium was higher (p = 0.036) and phosphate lower (p < 0.001) than the corresponding morning value. Moreover, the Ramadan mean morning phosphate was higher and the evening level lower was than Shabaan values (p = 0.010 and p <0.001, respectively), while mean iPTH level was decreased compared with the morning value (p = 0.001), and the evening mean during Shabaan (p = 0.029). Mean IgG concentration was significantly lower during Ramadan (p = 0.003 and p = 0.021 for morning and evening, respectively).
Conclusions:
Changes in dietary practices during Ramadan modulated PTH secretion to a pattern which might be beneficial to bone health. Combined effects of fasting and disturbed sleep led to a noted decrease in IgG level. Therefore, a possible beneficial effect of fasting on bone turnover is combined with decreased immune response.
Introduction
Intermittent fasting has received much attention recently, with reports of beneficial effects on various organ systems coming from different research groups [Anson et al. 2003; Bales and Kraus, 2013; Goodrick et al. 1990; Heilbronn and Ravussin, 2003; Horne et al. 2008; Mattson et al. 2002; Mattson and Wan, 2005; Sohal and Weindruch, 1996; Varady and Hellerstein, 2007]. Islam is a religion practiced by about 2 billion individuals and requires its followers to fast from dawn to sunset for 1 month a year, a practice named Ramadan. Due to the widespread nature of Muslim countries, there are Muslims from many ethnicities, with Ramadan fasting subjected to cultural influences of the host country. The Kingdom of Saudi Arabia is the center of the Islamic world. In recent decades, with increasing modernization, the sleep–wake cycle during Ramadan has been subjected to an almost complete nychtohemeral reversal compared with the rest of the year, with most residents staying up until dawn, sleeping a few hours (if any) before going to work, and sleeping again after work or when possible. This lifestyle during Ramadan is not seen in other countries and offers a unique opportunity to study the effects of circadially disturbed sleeping/eating patterns on hormonal secretion and metabolism. We previously reported that this disturbance during Ramadan was associated with loss of the circadian rhythm and increased evening levels of cortisol, a hormone that controls the expression of many hormones and inflammatory mediators, which might have deleterious effects on metabolic homeostasis [Bahijri et al. 2013].
Subclinical hypercortisolism has been associated with signs of glucocorticoid-induced osteoporosis (GIOP) [Chiodini et al. 2002; Morelli et al. 2011; Tauchmanova et al. 2001] and increased frequency of subclinical hypercortisolism was reported among patients with established osteoporosis [Chiodini et al. 2007; Kann et al. 2001]. Hence, bone metabolism might be affected during Ramadan fasting. A hormone that is important for maintaining bone integrity is parathyroid hormone (PTH) [Kroll, 2000]. PTH exhibits circadian rhythmicity [Jubiz et al. 1972; Logue et al. 1989]. This physiological variation in the circulating levels of PTH has been linked to bone formation [Nielsen et al. 1991] and is affected by sleep [Kripke et al. 1978; Logue et al. 1992]. In addition, acute fasting was reported to result in a significant decrease in serum PTH, which was suggested to be secondary to increased bone resorption [Schlemmer and Hassager, 1999].
Another major function of cortisol is to modulate immune responses during stress [McEwen et al. 1997]. It suppresses the production and activity of many proinflammatory cytokines during stressful periods and helps to return the organism back to baseline (homeostasis) after cessation of the stressor [McEwen et al. 1997; McKay and Cidlowski, 1999; Ruzek et al. 1999]. Hence, effects on the immune system function are expected due to Ramadan fasting and disrupted pattern of cortisol secretion. Therefore, we aimed to investigate the effects of this type of religious fasting in Saudi Arabia and its associated disturbance in the sleep–wake cycle and feeding patterns on bone metabolism reflected on the concentrations of bone minerals (calcium, phosphorus and magnesium), alkaline phosphatase, vitamin D and PTH, as well as levels of immunoglobulin (Ig) A, M and G.
Subjects and methods
Study design
The study design, physiological measurements and anthropometry were described in detail in our earlier report [Bahijri et al. 2013] and are summarized below. Studying the same subjects at different times helped us to avoid group variability at the study baseline and in reducing the number of subjects needed. Sample size was calculated to avoid type II statistical error [Eng, 2003] by employing reference ranges for intended measurements, as well as laboratory quality control data.
The study received approval from the Committee on the Ethics of Human Research at the Faculty of Medicine, King Abdulaziz University. Written informed consent was obtained in all cases. Of the recruited volunteer healthy subjects, 2 dropped out of the study, leaving 23 (18 males, 5 females), aged 18–42 years, to complete it. Volunteers were studied twice, during their regular life (Shaban) before, and again 10–15 days into the fasting period (Ramadan). All but one were <30 years of age, taking no medications or nutritional supplements; 3 subjects were obese [body mass index (BMI) ⩾30 kg/m2], 4 were overweight (BMI 25 to <30) and the rest had a normal BMI (<25). One male subject of normal weight was found to have a slightly elevated blood pressure (154/94) before taking the second blood sample. To avoid effects of diet and sleeping patterns on measured parameters, subjects were instructed to have meals as usual on the day of testing and to record their usual sleeping and waking times for the previous 3 days.
Blood samples were drawn twice daily at 9 a.m. ± 1 hour and again 12 hours later. Thus, the first and third samples were obtained while fasting (at least 10 hours for the first sample and 6–7 hours for the third sample), while the second and fourth samples were obtained 2–5 hours after meals. Separated serum samples were stored at -80ºC until measurements were performed.
Biochemical and endocrine assays
All serum biochemical and endocrine parameters were assayed in the accredited clinical chemistry laboratory at the National Guard Hospital, King Abdulaziz Medical City-Jeddah, Kingdom of Saudi Arabia. Calcium, albumin, magnesium, inorganic phosphorous and total alkaline phosphatase were assayed by a spectrophotometric method, while IgG, IgM and IgA were measured using an immunoturbidimetric method. An Abbott Architect c8000 auto-analyzer was used. An Abbott Architect i2000 auto-analyzer was used to measure intact PTH (iPTH) and total 25-OH vitamin D using a two-step sandwich chemiluminescent microparticle immunoassay (CMIA) technique.
Statistical analyses
Analyses were performed using SPSS statistical package version 19. Descriptive statistics, such as mean ± standard error of the mean (SEM), were calculated for all estimated parameters. The paired Student’s t-test was employed for comparison of means between days and nights. Significance was assigned at p < 0.05.
Results
The results of estimated biochemical, endocrine and immunological parameters are presented in Table 1, Figure 1 and Figure 2. No significant differences between morning and evening albumin concentration were noted during Shaban or Ramadan. However, both morning and evening Ramadan levels were significantly decreased compared with pre fast values (p = 0.001 in both cases) (Table 1).
Serum biochemical, endocrine and immunological parameters during Shaban and Ramadan.

Reported previously [Ajabnoor et al. 2014].
ALP, alkaline phosphatase; Ig, immunoglobulin; SEM, standard error of the mean.
Note: significant differences are indicated in bold

Serum morning and evening phosphate and adjusted calcium concentrations during Shaban and Ramadan.
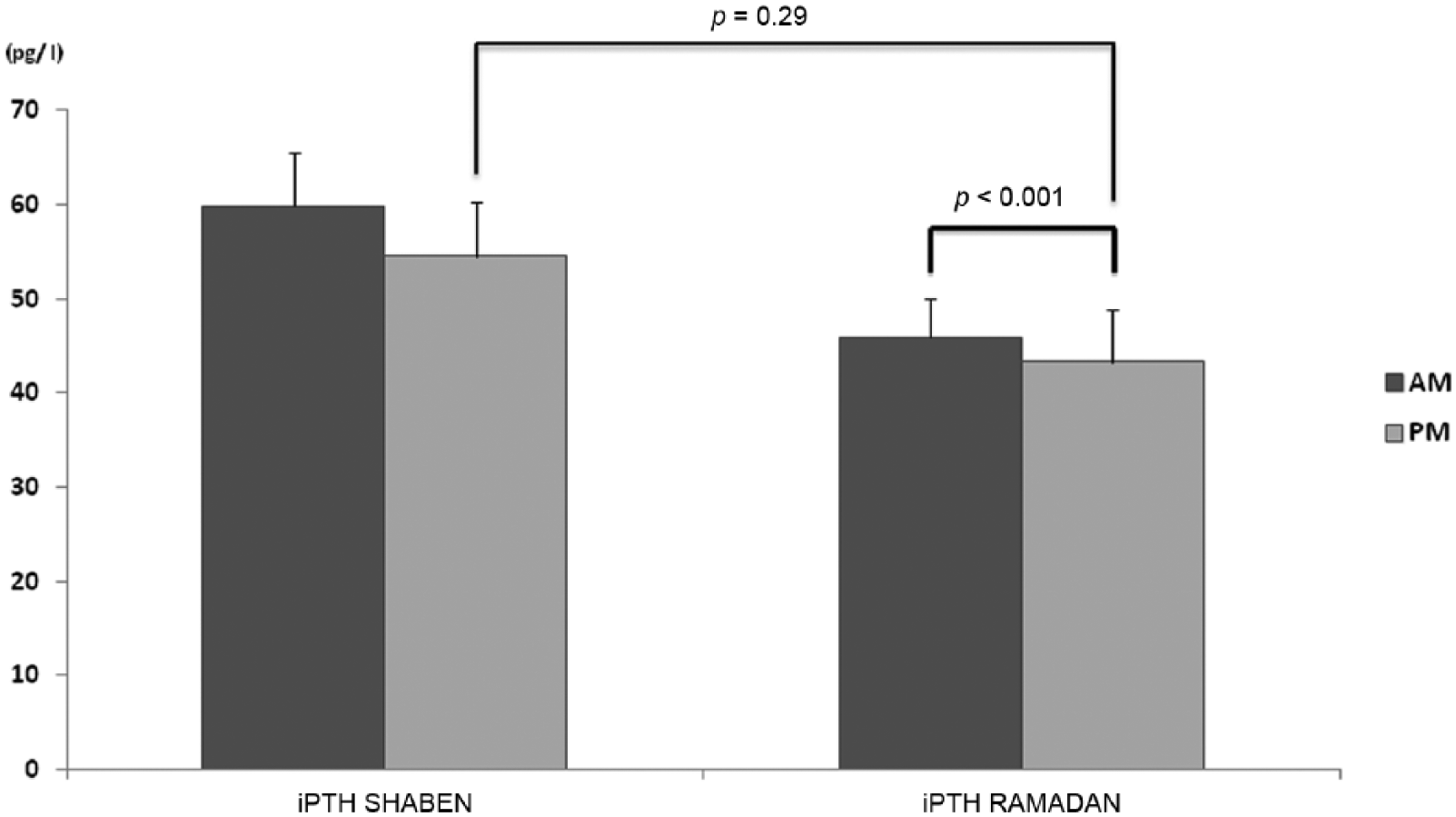
Serum morning and evening intact parathyroid hormone (iPTH) concentration during Shaban and Ramadan.
After correction for albumin concentration, evening-adjusted calcium was higher only during Ramadan (p = 0.036), with no significant differences between Shaban and Ramadan values in the morning or in the evening (Figure 1). In contrast, evening phosphate level was significantly lower than the morning value during Ramadan only (p < 0.001). In addition, during Ramadan, the morning level was higher and the evening level was lower than the Shaban corresponding values (p = 0.010 and p < 0.001, respectively) (Figure 1). Associated with these changes, there was a significant decrease in the evening mean level of circulating iPTH during Ramadan compared with the morning mean level (p = 0.001) and compared with the evening mean values during Shaban (p = 0.029) (Figure 2). In addition, during Shaban three subjects had slightly elevated concentrations of the hormone either in the morning or the evening sample, and two had more than double the top normal range in the morning and evening. During Ramadan, a slight elevation was noted for four subjects in the morning samples and for one subject in the evening sample. Only one subject with more than double the top normal range values during Shaban continued to have an elevated level during Ramadan.
According to the latest suggested classification of vitamin D status [Thacher and Clarke, 2011], 4 subjects had 25-OH vitamin D levels below the recognized severe deficiency cutoff level of ⩽10 ng/ml or ⩽25 nmol/l during Shaban, with 2 more falling into this category during Ramadan. However, during Shaban and Ramadan, the remaining subjects were in the vitamin D insufficiency range (>10–20 ng or >25 to <50 nmol/l) and none had serum concentrations ⩾30 ng/ml or 75 nmol/l, suggested as the cutoff value for defining optimal vitamin D status [Kennel et al. 2010; Prentice et al. 2008]. No significant difference was found in mean concentration of 25-OH vitamin D between Shaban and Ramadan values.
IgM mean concentrations did not show diurnal variation, neither was there a difference between means in Shaban and corresponding Ramadan means. However, means of IgA and IgG showed a significant increase in the evening during Shaban and Ramadan, with those of IgG being significantly lower during Ramadan than their corresponding Shaban means (Table 1).
No significant changes were noted in the means of other estimated parameters, and all values were within normal reference ranges.
Discussion
In normal healthy subjects, adequate sleep quality and duration associated with intermittent fasting, even without or little overall decrease in calorie intake, has been reported to increase lifespan [Anson et al. 2003; Goodrick et al. 1990] and improve health [Heilbronn and Ravussin, 2003; Mattson et al. 2002; Sohal and Weindruch, 1996]. However, studies on Muslims practicing Ramadan fasting gave conflicting results, with some reporting beneficial effects on metabolism [Adlouni et al. 1997, 1998; Maislos et al. 1993), and others reporting increased metabolic and endocrine dysregulation [Chennaoui et al. 2009; Fedail et al. 1982; Gumaa et al. 1978]. The Islamic world extends over a wide range of geographic locations, with different dietary habits and social practices. Therefore, studies carried out in different locations on Ramadan practitioners are likely to produce different results [Chandalia et al. 1987; El Ati et al. 1995].
Short-term fasting was reported to cause a significant decline in bone formation, independently of changes in acid–base status [Grinspoon et al. 1995]. Furthermore, changing dietary patterns were reported to have an effect on bone turnover in the rat, with division of intake into portions leading to decreased resorption [Muhlbauer and Fleisch, 1995]. In addition, there is circadian variation of biochemical markers of bone formation [Eastell et al. 1992b; Hassager et al. 1992; Nielsen et al. 1990; Pedersen et al. 1995] and is thought to be dependent on the circadian fluctuation in serum cortisol [Nielsen et al. 1988, 1992; Schlemmer et al. 1997]. Furthermore, biochemical parameters of bone resorption also show circadian variation, with the peak during the night/early morning and the nadir late in the afternoon [Schlemmer et al. 1994]. Therefore, in view of the high prevalence of osteoporosis in Saudi Arabia [El-Desouki, 2003; El-Desouki and Sulimani, 2007; Sadat-Ali et al. 2012], we considered it is important to study the effects of Ramadan type fasting, with its associated disruption of sleep/wake cycle and feeding pattern, in the Kingdom. We evaluated biochemical markers commonly used to study bone metabolism, namely 25-OHvitamin D, PTH, alkaline phosphatase and the bone minerals calcium, phosphorus and magnesium.
Total vitamin D levels were not affected by fasting and disturbed sleep pattern, as the mean 25-OH vitamin D level did not change significantly. Hence, noted changes in calcium and phosphate concentration are likely to be due to other factors such as changes in PTH concentration and feeding patterns.
PTH plays an important role in bone turnover, with studies indicating that continuous hypersecretion of PTH is associated with bone resorption, while intermittent administration of the hormone at a low dose has a positive effect on bone volume and micro-architecture [Kroll, 2000]. Moreover, changes in the circadian rhythms of PTH were reported in patients with postmenopausal osteoporosis [Fraser et al. 1998]. Thus, manipulation of PTH secretion has been suggested as a way of increasing bone strength and treating osteoporosis [Fraser et al. 2004; Silver and Bushinsky, 2004]. The impact of sleep on the circadian pattern of PTH is controversial [Kripke et al. 1978; Logue et al. 1992], with one study reporting that a large component of its diurnal rhythm is not effected by sleep–wake cycles [El-Hajj Fuleihan et al. 1997]. Normally, PTH peaks in the early morning hours, with a nadir in the late morning before noon [Kitamura et al. 1990], a secondary peak in the late afternoon, and a secondary nadir in the late evening before midnight. In our study, sampling was performed at 9 a.m. ± 1hour, and again 12 hours later; hence higher levels were expected in the morning samples. Indeed, this was found both during Shaban (pre-fasting) and Ramadan, with the latter reaching statistical significance (p = 0.001). Thus, sleep disturbance did not seem to have a marked effect on the circadian rhythm of the hormone, most likely due to the reported sleep-independent endogenous nature of the rhythm [El-Hajj Fuleihan et al. 1997]. However, the noted increased difference between morning and evening concentration during Ramadan could be beneficial to bone health, since the amplitude in the diurnal rhythm of intact PTH levels was reported to be greater in normal subjects than in osteoporotic subjects [Eastell et al. 1992a].
Fasting is reported to decrease the circulating PTH concentration [Schlemmer and Hassager, 1999]. Ramadan iPTH values were lower than corresponding Shabaan values, with evening mean concentration being significantly lower (p = 0.029) and fewer subjects having higher than normal levels. This could be attributed to fasting and the altered feeding pattern. During Ramadan, food (including dairy products) was ingested 2–3 hours before taking the evening sample; hence, the lower iPTH mean concentration corresponded with an increased post absorptive calcium concentration and a decreased phosphate concentration with increased carbohydrate metabolism (Figures 1 and 2), both acting to repress PTH secretion. Thus, it seems that the change in dietary patterns during Ramadan helps modulate PTH secretion by increasing evening calcium concentration, hence decreasing bone resorption during the night. Furthermore, changes in measured parameters are not due to fasting leading to hemoconcentration (dehydration) or acidosis, granted that electrolyte concentrations in the morning and evening samples did not change significantly during Shaban and Ramadan, as reported earlier [Bahijri et al. 2013].
Both factors of fasting and sleep deprivation have an effect on immune system function and responses. Debate is still ongoing regarding the benefits of fasting in relation to health and immunity [Varady and Hellerstein, 2007]. Both the specific and nonspecific immune responses are affected by fasting and the effect is dependent on age [Walrand et al. 2001] and nutritional status [McMurray et al. 1990; Wing et al. 1983]. During fasting, the number of B lymphocytes was significantly decreased, but an increase was described after the refeeding period, which was suggested to promote Ig production and to contribute to the induction of immune function after meal absorption [Walrand et al. 2001]. The effects on immune variables were attributed at least in part to changes in adrenal gland-related hormones [Komaki et al. 1997].
Ramadan type fasting modulates the levels of some cytokines involved in the regulation of the immune response [Mohammed and Mahmood, 2010]. Serum IgA, IgG and IgM levels in healthy Iraqi subjects and in patients with type 2 diabetes mellitus were reported to be slightly decreased towards the end of Ramadan [Al-Jewari et al. 2007]. Another study on healthy adult Turkish males found decreased concentrations of serum IgG and salivary IgA during Ramadan compared with pre-fast levels, but the IgG concentration remained within the normal range [Develioglu et al. 2013]. However, a study on Tunisian judo athletes maintaining training during Ramadan found increased IgA, which remained high 3 weeks later, with no change in leukocyte count [Chaouachi et al. 2009]. Those studies did not include the effects of sleep disturbance and deprivation factors which are common in Saudi population during Ramadan.
Studies indicate that sleep deprivation has deleterious effects on regulation of cytokine production and immune cell function [Bryant et al. 2004]. Sleep deprivation in rats increased the production of IgM [Everson, 2005; Zager et al. 2007] and IgG [Everson, 2005; Gumustekin et al. 2004] and IgA [Everson, 2005]. In humans, 24 hours of sleep deprivation increased the level of serum IgG and IgA [Hui et al. 2007]. Similarly, in another study on healthy young males, sleep deprivation due to land travel increased the concentration of serum IgG and IgA, but had no significant effect on IgM concentration [Abolhasan et al. 2012]. This was associated with a decrease in serum cortisol. In contrast to these reports, decreased sleep duration lowered the antibody response to various vaccines [Benedict et al. 2012; Lange et al. 2011; Prather et al. 2012; Spiegel et al. 2002] and to increase susceptibility to infection [Cohen et al. 2009; Mohren et al. 2002].
A close link between sleep deprivation and activity of the hypothalamic–pituitary–adrenal (HPA) axis and the circulating concentrations of cortisol has been reported [Wu, 2008]. In our study, the effects of disturbed sleep–wake cycle and sleep deprivation was combined with the effects of fasting, resulting in an altered cortisol secretion pattern as reported earlier [Bahijri et al. 2013] and leading to the noted significant decrease in IgG level during Ramadan (Table 1) (p = 0.003, and 0.021 for morning and evening values, respectively). Thus, subjects practicing Ramadan fasting in Saudi Arabia might have an increased risk of infection and a lower response to vaccines. Therefore, more studies are required to investigate the immune system status during Ramadan.
In conclusion, Ramadan fasting in Saudi Arabia might have some beneficial effects on bone turnover; however, it is associated with a decrease in the immune response. This should be considered when planning activities during this month, especially in the elderly, and chronically diseased or malnourished individuals.
Footnotes
Acknowledgements
The authors acknowledge with thanks DSR technical and financial support. The authors would also like to thank the Abuzinadah Hospital in Jeddah for help with sample collection.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Deanship of Scientific Research (DSR) at King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia under grant number (HiCi/1432- 6-2) as part of research activities conducted by the Saudi Diabetes Study Research Group.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.