
Abstract
Liver transplantation is the only definitive treatment for many diseases that affect this organ, however, its quantity and viability are reduced. The study of liver scaffolds based on an extracellular matrix is a tissue bioengineering strategy with great application in regenerative medicine. Collectively, recent studies suggest that liver scaffold transplantation may assist in reestablishing hepatic function in preclinical diseased animals, which represents a great potential for application as a treatment for patients with liver disease in the future. This review focuses on useful strategies to promote liver scaffold transplantation and the main open questions about this context. We outline the current knowledge about ex vivo bioengineered liver transplantation, including the surgical techniques, recipient survival time, scaffold preparation before transplantation, and liver disease models. We also highlight the current limitations and future directions regarding in vivo bioengineering techniques.
Keywords
Introduction
The liver is an essential organ for human body homeostasis. This organ, which is responsible for many immune and metabolic functions that are essential for the development of the body, primarily comprises hexagonal-shaped cells known as hepatocytes, which have an apical and basal domain replete with intracellular organelles. Besides being the second largest organ of the human body, the liver presents a great structural and functional complexity and intense regenerative capacity. Nevertheless, when exposed to severe injury, a huge amount of its functional and regenerative capacity is lost. Many factors, such as excessive consumption of alcoholic beverages, use of drugs, infections caused by hepatitis B and C viruses, and genetic factors, that develop severe metabolic diseases, can affect this organ. 1 Recurring injuries caused by these factors can often be irreversible in the liver, and thus it is necessary to establish strategies that can propose a therapeutic solution to diseases that affect this organ. Given this aspect, the objective of this review is to present a combination of results in the literature of the broad area of tissue bioengineering that supports the hypothesis of the use of ex vivo bioengineered liver based on extracellular matrix in regenerative medicine and transplantation context. In this review, we outline the current knowledge about ex vivo bioengineered liver transplantation, including the surgical techniques, recipient survival time, scaffold preparation before transplantation, and liver disease models. We also highlight the current limitations and future directions regarding in vivo bioengineering techniques.
Bioengineering approaches
Hepatocyte transplantation provides an alternative path for treating patients with different liver diseases. Many researchers have adopted this strategy, however, some limiting factors, such as limited cellular supplementation and efficiency in the action of these cells in the target tissue, hinder the use of this alternative. 2 Therefore, liver transplantation is currently the only therapeutic option. Recent studies in hepatic physiology, molecular biology, stem cell, and extracellular matrix have been supporting the development of tissue engineering, revealing a highly promising advance in this area of science. 3 The advances in tissue engineering have provided the development of techniques for the generation of bioartificial organs with potential applications in regenerative medicine. The main goal of this field is the substitution of human cells, tissues, or organs to restore the normal function of an organ or tissue that was damaged by many factors such as aging and even congenital disabilities. 4 Tissue engineering involves many aspects, such as the junction of cells, growth factors, and biomaterials. 5 In addition to the production of biomaterials, 6 and their use as structural scaffolds, tissue bioengineering has other alternatives, such as the creation of organ perfusion machines 7 ; 3D bioprinting techniques 8 ; organoid creation 9 ; the development of candidate molecules for growth factors 10 ; organ-on-a-chip production through microfluidics for drug testing 11 ; and the generation of extracellular matrix as a framework of organs employing decellularization techniques.
Decellularization
The generation of a specific acellular tissue matrix was initiated in 1979. 12 After this period, we can observe the use of the decellularization process applied to tissues of low complexity and highly complex organs such as the liver. Currently, human organs that would be discarded have had critical applications in tissue bioengineering. Organs such as the heart, 13 lungs, 14 liver, 15 and kidney 16 have been decellularized so that they can be used as bioartificial organs. 17 One of the most common acellular tissue matrices is the small intestinal submucosa (SIS) which is prepared from porcine by the mechanical removal of tunica mucosa and muscularis, and serosal layer. 18 In addition, this matrix maintains various bioactive molecules present in the extracellular matrix, such as fibronectin, glycosaminoglycans (GAGs), and growth factors. And today, the acellular scaffolds are not restricted to basic research and many companies such as Cytograft and Humancyte work with decellularized tissues. Many decellularized tissues have been reaching the market, and regulatory approvals are underway for the clinical use of xenogeneic decellularization-processed products. 19
Decellularization is a process in which all tissue cells and cell remnants are removed from the tissue or organ originating from an acellular and non-immunogenic scaffold. 15 The decellularization technique uses different methodologies and decellularization agents to remove cellular content from the tissue to leave only the extracellular matrix (ECM) and bioactive molecules. 17 These approaches generate a three-dimensional scaffold that keeps the biochemical, physicochemical, biological properties and structural integrity of the original tissue or organ. 20 Currently, the main methodologies used for decellularization include physical, chemical, or enzymatic methods. 12 The protocols are optimized to promote successful cell remotion while preserving the ECM composition and function. To address this issue, the methodologies can be combined to form an ideal decellularization protocol. Regarding the physical methodologies, organs and tissues can be decellularized after successive freezing and thawing steps, followed or not by sonication steps. 20 In enzymatic methodologies, different enzymes such as trypsin, endonucleases, and exonucleases are generally used to obtain a decellularized organ or tissue. 20 Chemical methodologies involve decellularization agents including acidic, basic, hypotonic, hypertonic, in addition to ionic, or non-ionic, and zwitterionic detergents. 20 The choice of decellularization methodologies will depend on several factors such as size, thickness, and composition of the organ or tissue, access to organ vasculature, and subsequent cannulation.12,15,17
Quality standarts for tissue decellularization
The decellularization protocols can be evaluated to confirm the efficiency in cell content removal. The satisfactory protocol to remove cell content of an organ or tissue must eliminate cellular components leaving no more than <50 ng DNA/mg ECM dry weight. Furthermore, the absence of nuclear content in hematoxylin and eosin staining (H&E) and immunostaining with a nuclear marker DAPI (4′,6-diamidino-2-phenylindole) are other evaluation criteria. 21 Other aspects can be evaluated, such as xenogeneic antigen reduction into acellular liver scaffolds obtained from by pig liver, for example. 22 An insufficient cell and epitopes removal can generate a macrophage phenotype response in the host that represents a problem to biological scaffold use. 23
Liver decellularization
The first successful decellularization of a liver was reported by Lin et al. 24 Besides decellularization through Triton X-100 and ammonium hydroxide perfusion, the authors also demonstrated that an acellular scaffold was suitable for cell engraftment and able to ensure an appropriate environment for the promotion of tissue formation. After that, other strategies were applied to obtain ECM from the liver, such as the use of detergents, enzymatic reagents, and physical methods.25,26 Since 2008, many studies aiming to improve the production of decellularized livers have been described.27–30 Initially, the main objective was to produce an efficient decellularization protocol that could generate a completely decellularized liver ECM. Then, the scientific community began to look for methods not only to produce decellularized livers but also to seek approaches to decellularization that would allow the entire original vasculature of the organ to be maintained. 30
In general, the beginning of the decellularization starts with perfusion of the whole liver with 1× PBS or distilled water as demonstrated by Robertson et al. 28 in the production of liver scaffolds from rat livers and by Lang et al. 29 in the production of liver scaffolds from pig livers. Then, the chemical detergents in various concentrations are perfused to promote cell remotion. Among the alterations in the protocols, there are different types of detergent solutions such as SDS (Sodium dodecyl sulfate), Triton X-100, Sodium deoxycholate; duration of perfusion and vessels used to perform the perfusion of the substances in the decellularization process. 27 Baptista et al. 30 developed an efficient protocol for decellularization of the rat liver with an association of Triton X-100 and SDS, able to preserve the intact vasculature of the organ. This perfusion-decellularization-based protocol is currently the main method used in basic research to produce whole decellularized liver from the rat and pigs. 31 In addition, this is one of the many other alternative methodologies described in the literature.
There is an increasing preoccupation with adequate detergent removal after decellularization since many of these agents are cytotoxic and have deleterious effects on cell seeding after decellularization.32,33 Although there are reviews in the literature reporting a toxic effect of detergents on cells during cell seeding procedure post decellularization, 34 some researchers have obtained a successful extracellular matrix recellularization post decellularization with detergents solutions. Hassanein et al. 35 demonstrated a recellularization with multilineage cells post 0.1% SDS perfusion. Kojima et al. 36 performed a seeding method with primary rat hepatocytes and liver sinusoidal endothelial cells post decellularization protocol with 1% Triton X-100. As an alternative, some groups have been using mild detergents, such as Triton X-100, to obtain acellular liver scaffolds. Willemse et al. 15 produced acellular liver scaffolds from whole human livers after Triton X-100 action and pressure-controlled perfusion. Therefore, in the last years, researchers have been focusing on fast and useful protocols avoiding non-human-compatible detergents to produce acellular livers to overcome the shortage of organs.
Liver Extracellular Matrix before and after decellularization
A promising strategy developed by tissue bioengineering scientists to solve the shortage of livers involves the use of the whole liver-derived ECM. Originally considered an inert product or substrate of cells, it is understood today that the ECM has an important structural, biochemical, and biomechanical function. The ECM can impact adhesion, shape, and cell differentiation.37–40 Further evidence has shown that ECM-cell interactions regulate the activation of progenitor or mature liver cells in vitro. These interactions can occur through integrin pathway signaling, the main receptors on the hepatocyte surface able to mediate ECM-cell interactions.41,42 Laminin, collagen III, IV, and hyaluronic acid are important to maintain the undifferentiated state of liver progenitor cells. While fibronectin is a key component of ECM involved with the scavenging of TGFß. 43
With recent advances in liver tissue engineering, several hepatic differentiation strategies exploring extracellular matrix components have been used to generate hepatocytes or hepatic-like cells in vitro.43–48 In parallel, proteomics-based approaches are increasingly used to answer how decellularization impacts the ECM’s composition and its ability to sustain new cells.
The ECM’s organization is efficient so that it constitutes a broadly vascularized three-dimensional scaffold that supports all the cells of the liver. Moreover, it acts as a start point at the beginning of the process of regeneration and tissue repair. 37 The liver ECM consists of various macromolecules, such as fibrotic (collagen fibers, reticular fibers, and elastic fibers) and non-fibrotic (glycosaminoglycans, proteoglycans, and glycoproteins) components. 49 Notably, the liver ECM is primarily composed of larger quantities of type I collagen and smaller amounts of type III, IV, V, VI, VII, and VIII collagen, glycosaminoglycans (GAGs), fibronectin, laminin, entactin, and tenascin.49,50 While some major fibrillar collagens (I, III, V, and VI) contribute to ensuring structural integrity in the liver parenchyma, other components such as collagen IV are delimiting the basement membrane in association with laminin, entactin, and tenascin and efficiently promote cell adhesion. 38 The negatively charged GAGs are responsible for attracting cations, which in turn attract numerous water molecules ensuring hydration to the liver ECM. 51 In addition, GAGs and proteoglycans also regulate the ECM stiffness allowing nutrient diffusion.51–55 In association, these components originate an interconnected network that represents a three-dimensional reservoir of signaling molecules and growth factors.17,52,53 Nevertheless, these biomolecules are not equally distributed throughout the organ. They differ in specific regions of the tissue, such as portal triad, central space, the space of Disse and the Glisson’s capsule, a thin and semi-transparent connective tissue layer composed of type I, III, IV, V, and VI collagen surrounding the liver.38,50,55,56
It is well characterized that decellularization removes several components from the ECM, especially the more soluble ones, and may partially damage the remaining ones (Figure 1). Harsh methods, such as the use of acids, bases, or ionic detergents, remove a considerable amount of GAGs and growth factors.21,23 In terms of protein composition, collagens (especially I and III, but also IV, V, VI, XI, XII, XIV, and XVIII), fibrinogens, fibronectin, elastin, asporin, fibulin, and annexins (I, II, VI, VII, and XI) remain after liver decellularization with SDS, although their proportion is changed. 49 These compounds are essential to sustain cell adhesion and give support to the growth of cells in recellularization steps.57,58 Several studies imply that the ECM originated after the decellularization procedure retains signals and codes responsible for many ECM-cell interactions, including cell adhesion, stem cell differentiation, induction of epithelial-mesenchymal transition, and promotion of malignant behavior of hepatocellular carcinoma cells.57–62 The results obtained by Jaramillo et al. 59 confirmed this interplay between decellularized ECM and cells. They investigated the effect of health decellularized human liver ECM on hepatic differentiation of human-induced pluripotent stem cells (hiPSC). When compared to common substrates used in cell differentiation protocols (e.g. Matrigel and collagen I), the decellularized human ECM was the best to induce high expressions of hepatic markers in cultivated cells. For this reason, new tools were developed, and nowadays, a liver ECM powder has been used in cell culture60,62 and such as bioink in 3D bioprinting, 17 and optimal results have been founded. These are examples that certificate an efficient use of liver ECM obtained by decellularization process to study cell biology, bioengineering application in regenerative medicine, and to certificate bioartificial liver clinical use (Figure 1).

Schematic representation of the hepatic ECM composition before (a) and after (b) decellularization. The liver ECM consists of a three-dimensional network composed by various macromolecules, such as fibrotic (collagen fibers, reticular fibers, and elastic fibers) and non-fibrotic (glycosaminoglycans, proteoglycans, and glycoproteins) components. After decellularization, an acellular and non-immunogenic three-dimensional scaffold is originated. Although, it three-dimensional shape is preserved, the composition of ECM can be affected reducing some macromolecules such as glycosaminoglycans (GAG).
Liver scaffold preparation before transplantation
In general, terminal sterilization protocols are applied to avoid scaffold contamination and to follow preclinical use after liver scaffold obtention by decellularization. Besides, some substances used during decellularization protocols serve as disinfectants, and other chemical or physical methods can be used to perform scaffold sterilization. After sterilization methods application, the scaffold can be stored in solutions containing antibiotics agents until the transplantation procedure. Taking into account the procedures applied before human liver transplantation, liver scaffold perfusion has been performed before transplantation in preclinical cases during scaffold preparation steps. In this context, serum Ringer’s Lactate, PBS (Phosphate-Buffered Saline), and storage solutions such as Custodiol or HTK (Histidine-Tryptophan-Ketoglutarate) have been used to promote acellular liver scaffold perfusion before transplantation. The commonly used liver graft perfusion solutions are described in Table 1. In some cases, these solutions were used during ex vivo blood perfusion prior to transplantation, such as a blood diluent and such anticoagulant aims.63–69
Liver scaffold preparation (perfusion and storage) before transplantation.

HTK: Histidine-Tryptophan-Ketoglutarate; PBS: phosphate buffered saline; PV: portal vein.
In this regard, our group opened a new frontier in liver scaffold preparation. We previously showed that Custodiol, a common storage solution, can be used to promote acellular and recellularized liver scaffolds perfusion and storage before orthotopic and heterotopic transplantation. In addition, we demonstrated that Custodiol was an efficient tool to improve the hemocompatibility of decellularized liver scaffold. 69 Therefore, organ storage solutions can be important alternatives to promote the preservation and to extend liver scaffold’s lifespan.
Liver transplantation
The idea of replacing one organ with another has been applied since ancient times in Egypt, and since then, many studies have been established with this goal. The purpose of tissue regeneration investigation was funded at the beginning of the 90s when an important study became the hallmark in this stage of scientific development. This study, which was published in 1997, showed the creation of a heterotopic ear through chondrocytes that were cultivated in mice lacking the thymus. 70 Since then, innovative tools were developed aiming to solve human health problems. However, many problems involving liver transplantation remain unsolved.
According to Health Resources & Services Administra-tion, there are currently over 106,000 people on the USA transplant waiting list. While about 45,664 people are waiting for organ transplantation in Brazil according to the Brazilian Transplantation Registry. The only definitive treatment for some liver diseases, such as severe hepatic failure is transplantation. 71 However, the number of patients awaiting transplantation is increasing, and the numbers of donors and viable organs are very small. To address this issue, tissue bioengineering has been providing throughout its development new strategies in the study of bioartificial organs aiming to apply them in regenerative medicine. 72 Thanks to the unique features of organ-derived ECM, we can explore this functional biological scaffold through tissue engineering. A serious problem in the orthotopic and heterotopic transplantation performance of organs in general, including the liver, is the potential immunological rejection of the graft by the recipient. The use of bioengineered liver based on decellularized ECM is an efficient strategy to perform these transplants, since it is not immunogenic and preserves the essential characteristics of the organ, such as vasculature and shape, corresponding to a three-dimensional scaffold that can be used as a graft for treatment purposes of acute and chronic liver diseases. 73
One of the aims of tissue bioengineering is the attempt to perform transplantation of decellularized or recellularized hepatic scaffolds primary into animals with various hepatic lesions, such as cirrhosis and in the future to perform transplantation into humans. Non-clinical models are crucial to understanding if acellular liver scaffolds can be fully recellularized and assemble a liver after in vivo transplantation. On the other hand, if only recellularized liver scaffolds could be able to be functional and viable after in vivo transplantation, many questions regarding cell sources, cell quantity, cell delivery, and long-term bioreactor culture remain unclear and need to be solved.
One of the biggest questions regarding basic research in hepatic transplantation is about the functionality and viability of ex vivo bioengineered liver after transplantation. Besides that, the choice of the type of transplantation should also be taken into account. The choice of transplantation should be very well studied since it will directly influence all the experimental stages throughout the research. There are two types of liver transplantation: orthotopic and heterotopic transplantation. Both types have been used in basic research since the 70s with different approaches regarding experimental models and surgical techniques. 74
Orthotopic transplantation
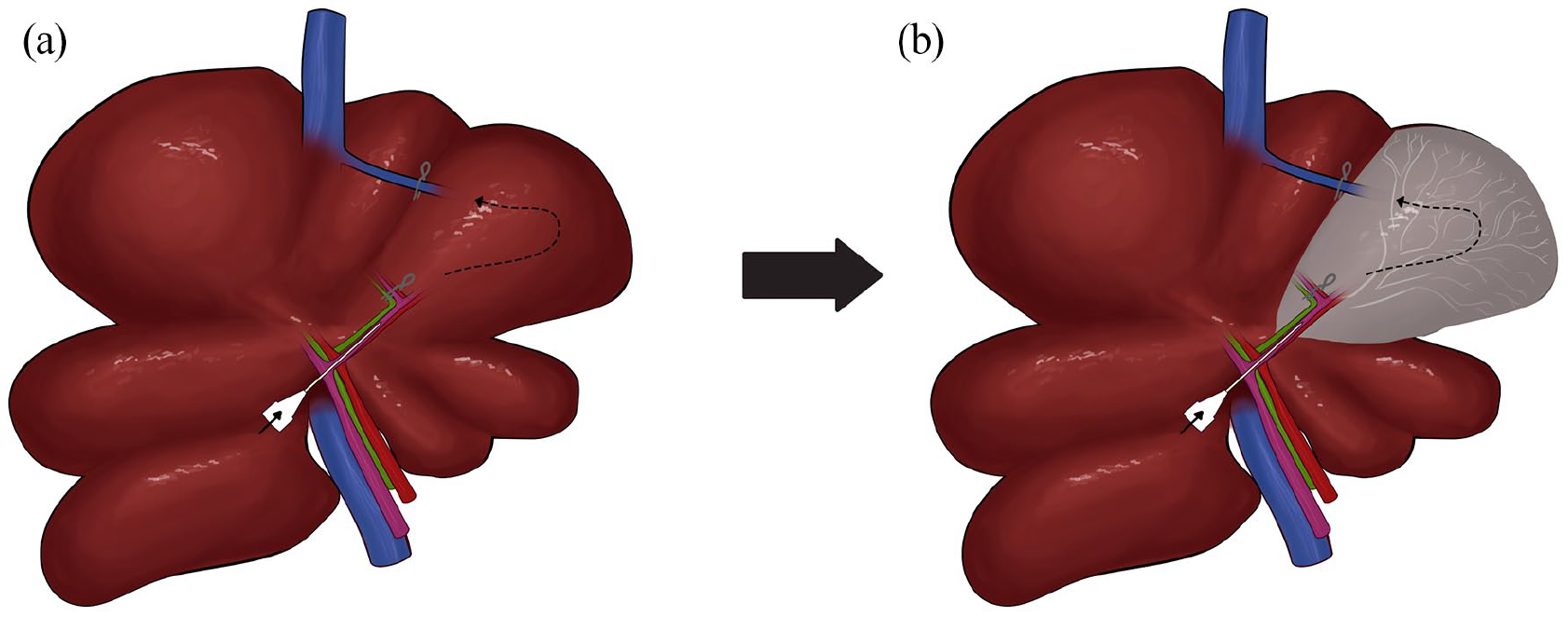
Orthotopic liver transplantation (OLT) is the only treatment for severe hepatic failure. This surgical technique consists of the complete removal of the damaged liver and replacing it with another one. 74 This technique is very challenging because it has some limitations such as oxygen supply and nutrients diffusion, which are essential for the proper function of the liver and the success of the surgery. Many researchers have been studying different strategies to improve the orthotopic transplantation experimental surgery. This procedure was established by Zimmerman et al. 75 and Kamada and Calne 76 after the development of the Cuff technique. Nowadays, it is already possible to decrease the probability of losing a transplanted organ and the consequent death of the animal.77,78 The success of this technique is mainly due to the reduction of the time of portal vein clamping and the reduction of bile damage in the graft.79,80 This type of transplantation consists of three stages: the first one is the performance of surgery on the donor, the second stage is the preparation of the graft, and the third one, which is the most complicated and most difficult to perform, is the surgical procedures to connect the graft into the recipient patient. The surgical procedures of this method can be seen in the studies carried out by Yokota et al. 77 Recently, several reports have used OLT to study immune regulations and responses in recipients animals post-surgery procedure. 81 Moreover, this surgical technique has been used to elucidate other events, such as mitochondrial protection and endoplasmic reticulum stress. 82 Qu et al. developed a novel technique to perform anastomosis for suprahepatic vena cava (SHVC) reconstruction in OLT. This technique consists of attaching the magnetic rings to the donor’s and recipient’s SHVC. 83 However, there are some limitations to this technique, such as a short SHVC of some rats and magnetic rings interfering with the scan during magnetic resonance image evaluation. Furthermore, other steps such as the re-arterialization must be performed to improve this novel model for OLT studies. Orthotopic liver transplantation was described a long time ago, and it is well elucidated. So far, there are no published studies that apply this surgical technique to transplant an ECM-originated bioartificial liver using liver disease models. Since total orthotopic transplantation using an acellular scaffold is not a good strategy. Other surgical alternatives can circumvent this surgical approach. One of them is the auxiliary orthotopic transplantation, in which the whole acellular liver scaffold or parts of it can be transplanted in an auxiliary way using the vasculature of the recipient animal, after leaving behind a part of the native liver (Figure 2). Besides an acellular liver scaffold, the recellularized liver can also be used in this context. Zhang et al. 63 performed orthotopic transplantation of acellular liver in healthy mice. In this work, the authors performed a partial orthotopic transplantation of acellular liver previously obtained by 1% SDS, 0.05% Trypsin, and 0.002% EDTA decellularization step. Even though step-by-step descriptions regarding surgical procedure, no recipient survival times, and post transplantation analysis were described.

A proposed strategy for auxiliary orthotopic transplantation of ex vivo bioengineered liver in rats. The acellular or recellularized liver (whole or partial) could be transplanted orthotopically (a) in an auxiliary manner, connecting the hepatic artery (HA) and portal vein (PV) (b). This strategy is interesting for studying liver disease models and assessing the capacity of liver scaffolds to improve animal health.
Until now, no other descriptions of ex vivo bioengineered liver orthotopic transplantation was published. One possible reason may be the complex surgical procedure to perform bioengineered liver anastomosis to allow recipient vessel connection, blood, and oxygen supply. This can probably explain the fact that there are no reports in the literature about the use of this strategy in liver disease models such as fibrosis/cirrhosis or hepatocellular carcinoma. These are open questions in the organ bioengineering field concerning ex vivo bioengineered orthotopic liver transplantation, which should be answered in the near future.
Heterotopic transplantation
Another approach for transplantation is called heterotopic liver transplantation (HLT). Many teams of scientists have adopted this technique since its establishment. 84 Heterotopic transplantation is the implant of an organ in a different anatomical region without removal or substitution of the native organ of the animal. 74 This technique was established as an alternative to orthotopic transplantation, and the transplanted liver mostly functions just as an auxiliary organ. This type of transplantation is widely used as an alternative in the treatment of chronic and acute hepatic failure. In order to perform this surgical strategy, different venous and arterial pathways can be taken in the animal models. Aller et al. 74 describe some of these pathways. The study of which veins and vessels are to be used to establish blood flow, as well as oxygen and nutrients input, should be prioritized since these factors will directly reflect the success of the transplantation. The surgical procedures of this method can be found in the studies of Schleimer et al. 84 and Qiao et al. 85 In addition, we described a step-by-step surgical methods to perform acellular liver scaffold transplantation. 68 Ex vivo bioengineered liver heterotopic transplantation was firstly reported by Uygun et al. 86 to implant decellularized and recellularized liver scaffolds in healthy recipient rats. They performed a unilateral nephrectomy and used arterial and renal vein to establish recipient and scaffold vessels connection, as shown in Figure 3. The generated results show us that this strategy has great applicability in tissue engineering. Even though successful recellularization of the scaffold, the graft viability was 8 h post-transplantation. Possibly, this short-term graft viability can be explained just by the fact that anastomosis is performed to promote a connection between the recipient and the graft. To perform an efficient anastomosis that allows continues blood flux to ensure nutrients distribution is not considerate an easy procedure and, in many cases, it requires microsurgery abilities and surgical microscope use. The weak flow of nutrients can promote cell death and results in short term graft viability. Shortly after, Baptista et al. 30 reported the second ex vivo bioengineered liver transplantation. In this work, the authors performed a partial scaffold transplantation (right lobe of the acellular scaffold) allowed by end-to-side anastomosis between the portal vein and vena cava of the scaffold and superior mesenteric vein and vena cava of the recipient Sprague-Dawley rat. In this case, differently from Uygun et al., the site for transplantation was the abdominal cavity, and because of that, this type of transplantation can be also called “ectopic transplantation.” This smart surgical strategy was efficient to study the mechanical properties of the scaffold vasculature after transplantation. Unfortunately, after vascular clamps removal, the blood flux was interrupted by clotting formation, and the graft was only viable for 60 min. Bruinsma et al. 64 performed recellularized and heparinized liver scaffolds heterotopic transplantation in recipient female Lewis rats. In this work, they removed the right kidney to allow graft transplantation. The proximal and distal inferior vena cava of the recipient rat were anastomosed with the portal vein and superior vena cava of the liver scaffold, respectively. The graft was viable for 24 h. Although successful, scaffold heparin mobilization the transplantation did not allowed long term graft viability after transplantation. Yang et al. 87 reported a partial heterotopic transplantation of caudate and middle lobes in recipient mice. The partial scaffold was connected to recipient mice through end-to-end fashion anastomosis between portal vein and renal artery of the recipient, while inferior vena cava was anastomosed with right renal vein of the recipient mice. The transplanted scaffold was evaluated 20–40 days after transplantation. More recently, Takeishi et al. 88 produced a bioengineered human liver scaffold to perform heterotopic auxiliary graft transplantation in recipient rats. The liver graft previously recellularized with a mix of human derived iPS cells was transplanted into immunocompromised and retrorsine-hepatectomy-preconditioned rats. The recipient animals were sacrificed at 4 days after transplantation and according to the authors the causes of mortality were poor blood flow into the graft, portal vein thrombosis and intestinal ischemia. Meng et al. 65 achieved the highest tax of ex vivo bioengineered liver survival post-transplantation (8 days) in recipient rats. After re-endothelization with immortalized endothelial cells perfused with gelatin-hydrogel, the ex vivo bioengineered liver was transplanted. In this work, they performed end-to-side fashion anastomosis between the abdominal aorta and inferior vena cava of recipient Sprague Dawley rats and portal vein and inferior vena cava of the scaffold, respectively. According to the authors, the active blood flux was observed in the ex vivo bioengineered liver and no internal bleeding was detected prior to rat abdomen closure. Even after 8 days post-transplantation, the blood flux was still detected. Until now, this report is the longest survival time reported involving ex vivo bioengineered liver transplantation. 65 Yanagi et al. 89 developed two methods (in vivo and ex vivo) for growing in vitro generated liver buds using orthotopic and heterotopic liver transplantation. Furthermore, they established a new method for orthotopic surgery entitled “the orthotopic transplantation on the transected parenchyma of the liver.” In agreement with the authors, this new procedure resulted in a superior growth of transplanted liver buds in comparison with heterotopic transplantation. More recently, the same authors published a new procedure to realize orthotopic transplantation using a fetal or 3D bio-printed liver bud in rats and porcine. 90

A proposed strategy for heterotopic transplantation of ex vivo bioengineered liver in rats. After performing a nephrectomy in the left kidney (a), the acellular or recellularized liver could be transplanted heteropically, connecting the hepatic artery (HA) to the renal artery (RA) and the portal vein (PV) to the renal vein (RV) (b).
Heterotopic transplantation in recipient large animals
According to surgical techniques adaptations other recipient animals have been explored representing a step to evaluate the clinical use of transplantable liver scaffolds. Ko et al.
66
were the first to report vascularized ex vivo bioengineered liver transplantation in a large animal model. After CD31-antibody immobilization, they transplanted ex vivo bioengineered liver harvested from piglets (5–8 kg) in recipient Yorkshire pigs (60–80 kg). They heterotopically implanted the ex vivo bioengineered liver after performing left nephrectomy following anastomosis between the renal artery and renal vein of the recipient pigs with the portal vein and inferior vena cava of the ex vivo bioengineered liver. The graft was viable to support blood flux up to 24 h post-transplantation. Mao et al.
91
obtained livers from pigs (10 kg) and performed heterotopic transplantation of a ex vivo bioengineered porcine liver post
Ex vivo bioengineered liver transplantation overview.

Bile duct reconstruction during transplantation
The liver is composed of complex vascular networks, including the bile duct. The biliary system is essential to provide normal liver functions, including concentration, transportation, storage, and secretion of bile acids. 93 Many groups have demonstrated that the bile duct is an important way to improve cell distribution and allow attachment into liver scaffold parenchyma.36,94–97 For this reason, the bile duct preservation during donor surgical steps following surgical reconstruction and recipient animal connection is a crucial step and could improve survival time post-transplantation and contribute to ex vivo bioengineered liver functionality. 71 To address this issue, surgical strategies such as choledochoduodenostomy to promote the connection between the bile duct of the ex vivo bioengineered liver and the duodenum of the recipient rat could be performed. 84 This surgical strategy was recently adopted by Takeishi et al. 88
Resection and partial hepatectomy before transplantation
As time passes, new strategies have been developed, aiming to improve the results of heterotopic and orthotopic transplantation, and researchers have been performing partial liver transplantation. In this context, the candidate liver first undergoes partial hepatectomy, which can vary from 10% to 90% removal of the hepatic lobes. 98 Our group previously showed that resections and partials hepatectomies before transplantation are useful surgical tools to investigate acellular liver scaffold recellularization after in vivo transplantation. 68 Ono et al. 99 have shown success in partial heterotopic transplantation in rats after performing partial hepatectomy of 30% of the graft. Wang et al. 100 have shown a modification of the partial heterotopic transplantation with hepatectomy in the host and its effects in the regeneration of the grafted liver. Currently, other strategies have been described to allow ex vivo bioengineered liver transplantation. Recently, the acellular liver scaffold obtained by decellularization with sodium lauryl ether sulfate was transplanted in recipient rats after lobectomy. 101 This process is schematically depicted in Figure 4. Naeem et al. 101 performed a left lateral lobe removal and subsequently left lateral acellular liver scaffold lobe transplantation in control rats. The graft was evaluated 30 days post-transplantation. Histological analysis confirmed neovascularization and whole recellularization after transplantation. Hepatocytes, immune cells, and stellate cells were identified into the scaffold. Furthermore, the surgical procedure of transplantation did not impact the recipient’s serological parameters. Shimoda et al. 67 performed acellular liver scaffold transplantation after resection in recipient pig livers. Pigs weighing 20–25 kg were submitted to partial hepatectomy, and then, the left median or left lateral lobe of the acellular liver scaffold was transplanted. The scaffold was evaluated 1, 10- and 28-days post-transplantation. Histological analysis confirmed different cell type infiltration, including albumin, CD31, CK19, and EpCAM positive cells. Moreover, the authors suggest that acellular liver scaffold could promote regeneration and neo cell organization after liver resection.

A proposed strategy for transplantation of ex vivo bioengineered liver after partial hepatectomy. In this strategy, first, a portion of the liver median lobe is removed through a partial hepatectomy (a). The acellular or recellularized liver can then be connected to the removed portion of the lobe (b).
This bioengineering strategy relies on the ability of the acellular liver lobe to regenerate and reach a liver mass post-transplantation. 72 In this context, there are beneficial effects of performing partial hepatectomy followed by transplantation of the acellular liver lobe scaffold. First, the recipient’s resected liver activates endogenous signaling to allow hepatocyte hypertrophy and hyperplasia. 102 Besides hepatocytes, cholangiocytes, Kupffer cells, liver sinusoidal endothelial cells, and stellate cells are also responsible for providing various signals that initiate and propagate liver regeneration.103,104 Second, the liver lobe scaffold is an ideal scaffold that contains an efficient nutrient-rich environment that facilitates cell attachment, and viability. Furthermore, in the scaffold, the cells find space to interact with each other and establish cell to cell and cell to ECM interactions. In particular, the interrelationship between cells and ECM contributes to a homeostatic rate of ECM degradation and synthesis where the cells can deposit matrix while proliferating. Taken together, the presence of a three-dimensional environment favorable to tissue development provides the ideal clues for the receptor’s cells to migrate to the scaffold, assembling a newly regenerated liver tissue. 104 It is noteworthy to mention that these benefits can also be extended in case of liver disease. Under this circumstance the liver regeneration is minimal, and the acellular liver lobe scaffold can be an efficient strategy used to induce regeneration. In this case, the acellular ECM acts as a reservoir of growth factors such as HGF, known to be a potent regeneration inducer ready to receive bipotent liver progenitor cells (oval cells) that, through ECM stimuli, will initiate the process of cell differentiation and proliferation, assembling a new liver tissue.105,106 In addition, the transplanted scaffold can ensure liver mass that will provide functional metabolic support until the recipient’s liver can restore its functions.92,107,108
Aiming to use this approach in the human clinic in the future, this bioengineering strategy can be an efficient tool to increase the limit of liver resections during hepatectomies procedures. 109 Furthermore, the successful results obtained by literature support that acellular liver lobe transplantation can induce liver regeneration and therefore minimize the risk of postoperative liver failure in humans.
In vivo liver engineering
New bioengineering strategies based on decellularization have been created. In vivo liver engineering represents a new way to apply clinical tools in regenerative medicine and consist of a liver lobe decellularization method in live animals. This approach was reported firstly by Pan et al. 110 They developed a new surgical technique to generate inferior right lobe isolation and to establish a by-pass circulation after portal vein and inferior vena cava cannulation. Perfusion of 1% SDS and 1% Triton X-100 for 30 min each was used to promote inferior right lobe decellularization. After single liver lobe decellularization step, they perfused mature hepatocytes within the bioengineered lobe and reestablished the blood circulation for 6 h in vivo. 110 More recently, Wang et al. 111 improved the surgical technique and investigated three different protocols to perform in vivo liver lobe perfusion and decellularization. 112 To promote a successful in vivo partial liver lobe decellularization, the left lateral lobe was perfused with 1% SDS and 1% Triton X-100 for 1 h or only with 1% SDS or 1% Triton X-100 for 2 h, respectively. According to the authors, in vivo decellularization with 1% SDS only for 2 h was able to promote efficient cell remotion while the main ECM proteins were preserved. In this work, they established new strategies to avoid chemical detergent contamination and to study short-term physiological perfusion. Furthermore, they established a 7 days survival model to study in vivo liver bioengineering. 112 A summary of the studies exploring in vivo bioengineering strategies is described in Table 3 and the surgical approach is depicted in Figure 5. This technique can be successfully translational to clinical in the future to treat liver diseases such as tumor areas in the liver without performing resection steps. In addition, this is currently a useful and homeostatic method to study hepatic recellularization in vivo. In comparison to common ex vivo bioengineering methods, in vivo liver engineering has advantages such as the capacity to investigate cell recruitment and attachment into decellularized liver lobe under physiological blood circulation that ensures optimal amounts of nutrients and oxygen, besides does not require anastomosis between the recipient and the graft. In this regard, some important vessels, such as the hepatic artery and the bile duct, are naturally preserved and do not need to be reconstructed like in ex vivo bioengineering methods.110–112 Furthermore, in vivo bioengineering strategies are also promising because they eliminate the need for another organ for transplantation. In this case, the animal/patient’s liver is used to induce post-decellularization regeneration, and therefore there is no need for replacement. However, many hurdles and pitfalls regarding in vivo bioengineering remain. The surgical technique steps to avoid chemical detergent contamination during lobe perfusion, time of decellularization, techniques to close vessels and prevent blood loss at the final of operation, strategies to prevent blood clots, kidney failure, and long-term survival time are some of the open questions and could be solved in the next years.
In vivo liver engineering studies.

SDS: sodium dodecyl sulfate;
Schematic representation of an in vivo decellularization strategy. With the animal’s abdominal cavity open, the arterial and biliary vasculatures are clamped in the left lateral lobe (LLL) entrance as well as the venous branch that connects this lobe to the superior vena cava (a). A cannula is inserted in the portal vein ramification directly before the entrance of the LLL, and decellularization agents can then be perfused to remove cellular content selectively from this lobe (b).
Animal models to test ex vivo bioengineered liver functionality post-transplantation
Regarding the introduction of liver scaffolds into orthotopic and heterotopic transplantation or in vivo engineering, the chosen animal model should also be well studied. Some authors described the limitations of performing transplantation in mice due to their liver size and the arteries and vessels, which usually cannot be identified by naked eyes. 113 In addition, besides mice, small animals such as rats need surgeons with more experience in performing microsurgeries and microsurgical microscopes for transplantation purposes. These traits are minor when transplantation is performed on pigs or other large animals. Once the choice of animal model was well studied for liver scaffold transplantation inquiry, the liver disease model should also be chosen. To study the transplanted liver scaffold functionality in animals with liver disease, one should choose a pathological model and then induce this pathology into the animals before performing transplantation.113,114 The main animal models used to address ex vivo bioengineered liver functionality post-transplantation are described in Table 4. Many models can be selected, such as Wilson’s disease, 116 genetic or chemical induction of hepatocellular carcinoma, 117 fibrosis/cirrhosis,118–120 ionizing radiation-induced lesion, 121 hepatic alcoholic steatosis, 122 among others. 115 Our group has shown success in the chemical-induced cirrhosis model by intraperitoneal administration of carbon tetrachloride (CCl4).119,123–125 However, other substances can be used to induce this pathological process.126,127 Delire et al. 128 have described the results of the disease induction by CCl4 administration and other two substances: thioacetamide (TAA) and dimethylnitrosamine (DMN). According to these authors, the substance that best induces the pathological model occurring in humans is TAA. In addition, this substance has lower animal death indices when compared to DMN administration, which is highly toxic to animals leading to high mortality rate.
The main disease models used to test ex vivo bioengineered liver functionality post-transplantation.

ALB: albumin; ALT: aspartate aminotransferase; AST: aspartate transaminase; CCL4: carbon tetrachloride; i.p: intraperitoneally; TB: total bilirubin.
To address functionality evaluation, Jiang et al. 129 transplanted ex vivo bioengineered liver repopulated with 106 mesenchymal stromal/stem cells in mice models of fulminant hepatic failure model induced by CCl4. After left lobe 2-mm incision, the transplanted ex vivo bioengineered liver was efficient in rescuing liver functions of recipient animals treated with CCl4 30 days after transplantation. More recently, Nobakht Lahrood et al. 130 transplanted a liver patch from decellularized sheep liver reseeded with human bone marrow stromal cells, human endothelial, and hepatoma cells (Huh7) in acute liver failure recipient mice obtained by CCl4 sublethal dose administration. The scaffold functionality was observed 48 and 72 h post-transplantation decreasing aspartate transaminase (AST) levels and increasing albumin (ALB) levels in recipient animals’ serum. Li et al. 131 transplanted bioengineered hepatic tissues in the omentum majus of recipient mice treated with CCl4 7 days before transplantation. The authors observed that recellularized liver graft was able to improve the recipient’s serological parameters (decreasing AST, total bilirubin levels, and increasing albumin ALB levels) and also ameliorated native liver fibrogenesis. Taken together, these studies demonstrated that ex vivo bioengineered livers are powerful tools in regenerative medicine to treat liver diseases. An overview of current organ bioengineering approaches available to treat liver disease is presented in Figure 6.
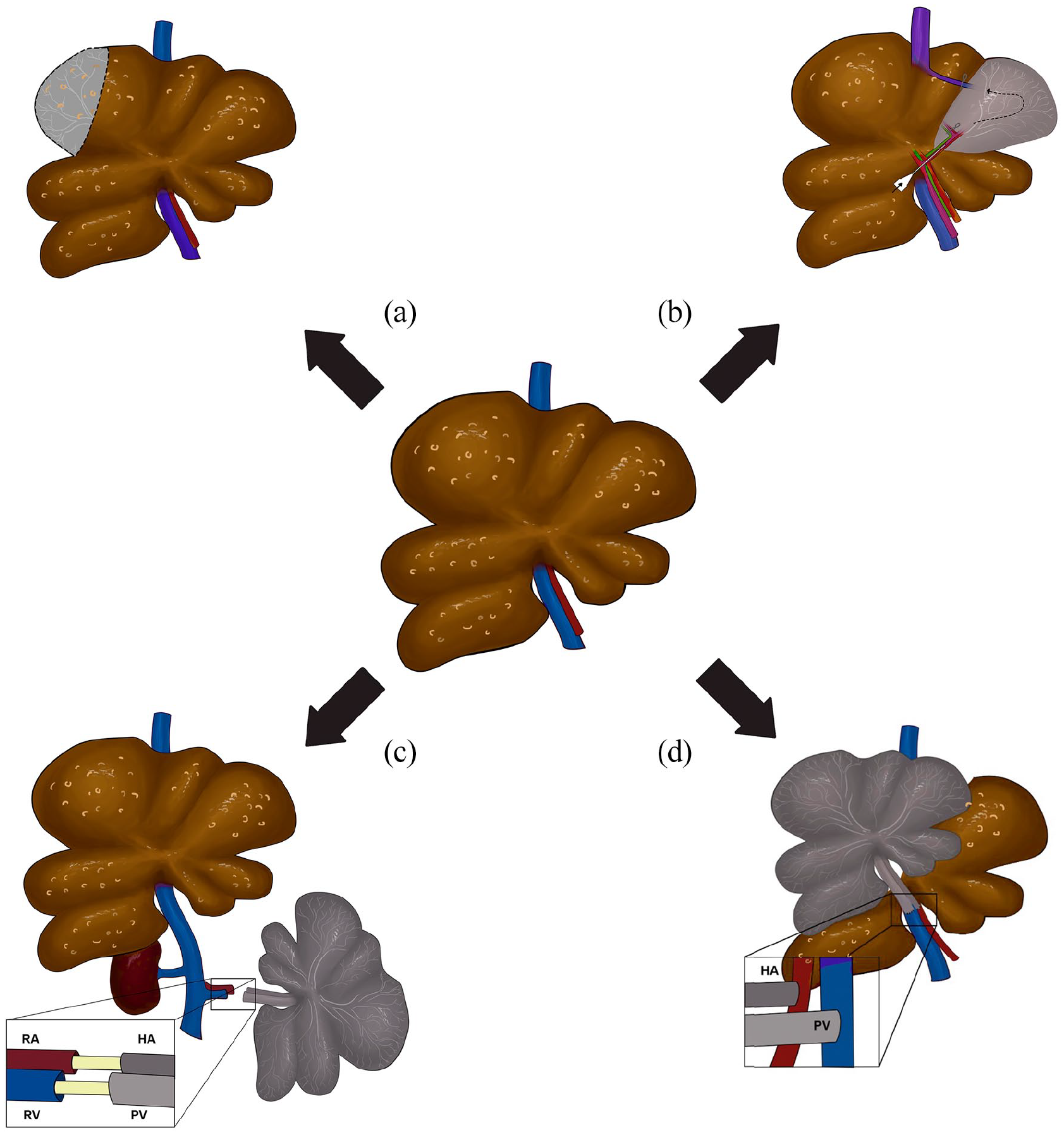
Available strategies to explore ex vivo bioengineered liver transplantation and in vivo decellularization in diseased livers. Partial hepatectomy followed by bioengineered liver lobe transplantation (a); in vivo decellularization (b); heterotopic bioengineered liver transplantation (c) and orthotopic bioengineered liver transplantation (d).
As far as we know, a few descriptions of ex vivo bioengineered liver transplantation in the recipient liver disease model were published.129–131 Probably, it can be explained by the difficulty of reaching long-term survival taxes after transplantation. A substantial number of animal models with liver disease already have a high mortality rate during the time of induction, which hinders their surgical performance resulting in short-term survival taxes. In addition, this negative scenario impact on functionality evaluation of the liver scaffolds post-transplantation. These current limitations and hurdles show the real reason and importance of studying liver bioengineering. In addition, it reflects the morbidity of patients with liver disease, and represents a real scenario of the possible difficulties and pitfalls that we will have to face to allow the use of bioengineered livers in the future. Considering the main reason to promote clinical translation, these studies are fundamental to creating feasible alternatives to liver shortage and transplantation. These basic models are crucial to elucidate bioengineered liver applications in liver diseases with any etiology, such as metabolic liver disease, biliary atresia, and acute and chronic liver disease.
Conclusions
Liver scaffolds based on native ECM are a strategy with huge potential in regenerative medicine to meet the growing demand for organs. Through the decellularization technique, the liver ECM can be obtained and then transplanted in preclinical models in a vastly pathological condition of the liver. The choice of the type of transplantation and liver disease model should be prioritized in the studies to establish tests that prove the reestablishment of liver function. In agreement, surgical techniques involving bile duct preservation and reconstruction and procedures that are more clinically reliable are necessary. Studies exploring acellular liver scaffolds transplantation should also be considered. We believe that ex vivo bioengineered liver transplantation represents a considerable advance in tissue engineering, and it has a great impact of applicability in the human clinic, assisting mainly in life improvements of patients with serious liver disease.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by: National Center of Science and Technology for Regenerative Medicine/INCT-REGENERA grant No 465656/2014-5, National Research Council/CNPq grant No 401816/2016-8, and Rio de Janeiro Research State Foundation /FAPERJ grant No E-26/202.963/2017, Brazilian National Council for Scientific and Technological Development (CNPq) grant No 465656/2014-5, and the Coordination for the Improvement of Higher-Level Personnel (CAPES) and FAPERJ for the scholarship support.