
Abstract
It was demonstrated that octacalcium phosphate collagen composite achieved notable bone regeneration in bone defects in preclinical studies. On the basis of the research results, an investigator-initiated exploratory clinical trial was conducted after approval from a local Institutional Review Board. This clinical study was performed as a single-arm non-randomized intervention study. Octacalcium phosphate collagen composite was implanted into a total of 10 cases of alveolar bone defects after tooth extractions and cystectomy. Safety assessment was performed in terms of the clinical course and several consecutive laboratory examinations, and sequential radiographs were used for efficacy assessment. All participants uneventfully completed the clinical trial without major problems in their general condition. Postoperative wound swelling was observed, as also commonly seen in tooth extraction or cystectomy. Although no serious liver dysfunction, renal dysfunction, electrolyte imbalance, or abnormal urinalysis results were recognized, the number of white blood cells and C-reactive protein level temporarily increased after the operation. An increase in radiopacity in the octacalcium phosphate collagen composite–implanted site was observed in all cases. Finally, the border between the original bone and the octacalcium phosphate collagen composite–implanted site became indistinguishable. These results suggest that octacalcium phosphate collagen composite could be utilized safely in clinical situations in the future.
Introduction
As the restoration of bone defects is one of the critical themes in oral and maxillofacial surgery, 1 many bone substitute materials were developed to resolve this problem. 2 Calcium phosphate biomaterials are the principal bone substitute, and sintered ceramics of hydroxyapatite (HA) and β-tricalcium phosphate (β-TCP) have been widely used in clinical situations because they have no limitations, given their availability, excellent osteoconductivity, and relatively uniform quality.3,4 However, these bone regenerative properties were far beyond autologous bone grafting,5,6 and there is a demand to develop a substitute for autologous bone.
Octacalcium phosphate (OCP: Ca8H2(PO4)6 · 5H2O) is one type of calcium phosphate that has been suggested to be a precursor of biological apatite crystal in bone and tooth.7,8 If OCP were implanted into a bone defect, it would be irreversibly converted into the apatitic phase, 9 and it was shown to promote osteoblastic cell differentiation. 10 Moreover, the level of bone regeneration due to synthetic OCP was significantly higher than that for HA or β-TCP if implanted into a rodent calvarial bone defect. 11 Similarly, there have been an increasing number of studies using synthetic OCP that explained its bone regenerative properties and established approaches for using it in various bone defects.12–15
While OCP exhibits many desirable properties as a bone substitute, its intrinsic crystal characteristics prevent its molding by a sintering process, which has reduced the possibility of applying OCP clinically. To resolve the disadvantages of this material, OCP combined with atelocollagen for medical use (OCP/Col) was developed, and its bone regenerative properties were significantly better than those of OCP. 16 OCP/Col significantly enhanced bone regeneration more than sintered HA or β-TCP ceramic combined with collagen if implanted into a rodent critical-sized calvarial bone defect. 17 Likewise, notable bone regeneration using OCP/Col was confirmed in several canine experimental models, such as tooth extraction hole, critical-sized calvarial bone defect, artificial alveolar cleft, and mandibular bone defect.18–22
On the basis of these research results, an investigator-initiated exploratory clinical trial involving 10 patients was conducted for the first time in the world, according to Japanese ethical guidelines and regulations. After approval from the local Institutional Review Board (IRB), safety and efficacy were examined after the implantation of OCP/Col into bone defects, such as tooth extraction sockets or cyst holes. Safety evaluations were performed using systemic, local, and clinical laboratory findings, and efficacy assessments were performed by comparing the radiographic density of surgical sites to those of the surrounding host bone up to 1 year after implantation. Although part of the clinical course of the OCP/Col-treated patients has already been reported,23,24 a summary of this clinical trial is described here.
Materials and methods
Preparation of the material
The clinical batches were prepared aseptically in clean room facilities. As previously reported,22,23 OCP was prepared by direct precipitation, 25 and the sieved granules (particle sizes of 300–500 µm) were sterilized by heating at 120°C for 2 h. In the X-ray diffraction (XRD) pattern of the synthesized OCP that was recorded on a diffractometer (Mini Flex; Rigaku Electrical, Tokyo, Japan) at 30 kV and 15 mA, the primary (100) peak of OCP was identified at 2θ = 4.7. Collagen was prepared from NMP collagen PS (Nippon Meat Packers, Inc., Tsukuba, Ibaraki, Japan), a lyophilized powder of pepsin-digested atelocollagen isolated from the porcine dermis. OCP/Col was prepared from NMP collagen PS and OCP granules. OCP was added to the concentrated collagen and mixed, and the weight percentage of OCP in OCP/Col became 77%. The OCP/Col mixture was then lyophilized, and the disk was molded (9 mm in diameter, 1 mm thick). The molded OCP/Col underwent dehydrothermal treatment (150°C, 24 h) in a vacuum drying oven (Figure 1).

The appearance of OCP/Col disks and XRD of OCP/Col: (a) the disks were molded to 9 mm in diameter and 1 mm thick and (b) XRD patterns of OCP/Col before implantation.
After two OCP/Col disks had been inserted into a sterilized conical tube (1.5 mL; 509-GRD-SC, Quality Scientific Plastics, USA), the tube was packed in a Fisherbrand instant sealing sterilization pouch (9 cm × 13 cm; Fisher Scientific, Pittsburgh, PA, USA). The packaged OCP/Col was then sterilized using gamma-ray irradiation (5 kGy) to a ready-to-use form. After sterilization, the XRD pattern derived from OCP/Col exhibited a collapsed and reduced primary (100) peak with a shift from 4.7° to 5.3° at 2θ, as previously reported. 16 In addition, the OCP/collagen itself had little radiopacity, as previously reported.17,23
Design of the clinical trial
The official scientific title of the study is “Bone regenerative therapy by octacalcium phosphate (OCP) collagen com-posites,” which was registered as JPRN-UMIN000004655 in the University Hospital Medical Information Network in Japan (UMIN) and the International Clinical Trials Registry Platform Search Portal of the World Health Organization. The protocol of the clinical trial was submitted and approved by the research ethics committee of Tohoku University Graduate School of Dentistry under reference number 20-27. The principal investigator and promoter were Dr Shinji Kamakura (DDS, PhD) and the Department of Oral and Maxillofacial Surgery, Tohoku University Hospital, Sendai, Japan.
The main purpose of this clinical trial was a safety verification of OCP/Col if implanted into a total of 10 cases of tooth extraction socket and cyst hole (Table 1). And considering the ethical aspect of the study patients, this clinical trial is performed by a single-arm non-randomized intervention study after consultation with the local IRB. The number of the subject patient was established with discussion of local IRB by referring the previous study which was injected into bone substitute in dental sockets and evaluated safety and efficacy of the device. 26 The safety verification was evaluated in terms of the clinical course and several consecutive laboratory examinations. The second clinical evaluation focused on bone regeneration in the bone defects after tooth extractions and cystectomy by radiographic examination. These selection criteria were applied to the candidates. The examinees were aged 20–65 years, including both inpatients and outpatients. The period with no effects and the treatment period were specified. In cyst cases, the longest diameters of radiographic examination were below 5 cm. In tooth extraction cases, the extraction socket must be covered by primary closure. In addition, the following patients were excluded from this study: (1) patients suffering from severe hepatopathy, renal disorders, and heart disease, who would affect the safety evaluation in this trial; (2) patients using allergy drugs; (3) patients who were pregnant, possibly pregnant, nursing, or considering pregnancy; (4) patients who had participated in other clinical trial programs within 3 months prior to study entry; and (5) others, namely, patients who were unfit for the study as determined by the principal investigator or sub-investigators.
List of the patients.
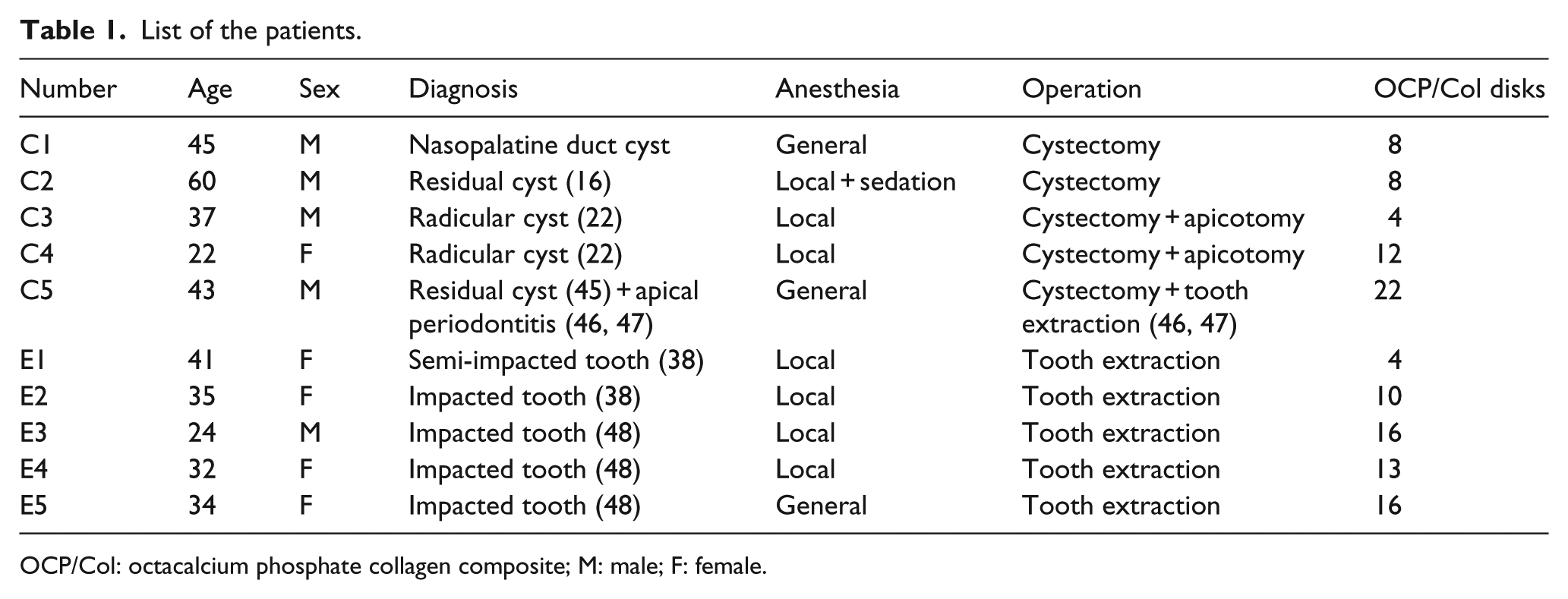
OCP/Col: octacalcium phosphate collagen composite; M: male; F: female.
The candidates also underwent laboratory examinations, such as blood and urine tests and a cardiac function test, before the operation. In addition, a pulmonary function test was performed on patients for whom an operation under general anesthesia was planned (Table 2). Finally, 10 patients who did not meet the exclusion criteria and signed the formal consent form were included in this study. These 10 patients included 5 males and 5 females, and 5 cyst and 5 extraction socket cases. The ages of the patients ranged from 22 to 60, with an average of 37.3 years (Table 1).
List of the laboratory examinations.

The examinations were performed before the operation and 1 day, 1 week, and 1, 3, 6, 9, and 12 months after it. The items marked with an asterisk are limited to sets of data from the preoperative assessment.
AST: Aspartate transaminase;
GOT: Glutamic oxaloacetic transaminase;
ALT: Alanine transaminase;
GPT: Glutamic pyruvic transaminase;
ALP: Alkaline phosphatase;
LDH: Lactic acid dehydrogenase;
GTP: Glutamyl transpeptidase;
BUN: Blood urea nitrogen;
HCV: Hepatitis C virus.
Surgical procedure
All extracted teeth were impacted or semi-impacted mandibular wisdom teeth under general and local anesthesia. Incisions were made medially and distally in the gingiva around the tooth. Full-thickness flaps were raised in the periosteal region. The wisdom teeth were extracted using an elevator with root amputation and/or the removal of surrounding bone. After extraction, the sockets were rinsed with saline solution, and the OCP/Col disks were implanted into them. Finally, the operation wounds were closed by suturing the flap with biodegradable sutures.
In the cyst cases, the operations were performed under general and local anesthesia with/without sedation. After gingival incisions had been made medially and distally around the cystic lesion, full-thickness periosteal flaps were raised. Cystectomy with apicotomy and/or tooth extraction was accomplished with the removal of overlying bone, if necessary. After cystectomy, the cyst holes were rinsed with saline solution, and the OCP/Col disks were implanted into them. Finally, the operation wounds were closed by suturing the flap with biodegradable sutures. To prevent infection, antibiotics were administered orally for 3–7 days postsurgically with or without an intravenous drip during the operation in all cases. In addition, postoperative analgesics were administered orally for 3–7 days.
Postoperative clinical and radiographic assessment
Safety assessment was performed by examining the clinical course, the presence or absence of adverse events, and sequential clinical laboratory results (hematologic test and urinalysis) (Table 2). Analysis of the clinical condition and other examinations were performed before the operation and 1 day, 1 week, and 1, 3, 6, 9, and 12 months after it. Efficacy assessment was performed using radiographs, such as intraoral and panoramic radiography, and computed tomography (CT). Intraoral and panoramic radiography was conducted before the operation and 1 day, 1 week, and 1, 3, 6, 9, and 12 months after it. The operated region was scanned by CT (SOMATOM Definition Flash, SIEMENS, Germany) at 35 mA, 120 KV, 0.6 mm thickness, before the operation and 3, 6, and 12 months after it. And the Hounsfield Unit (HU) values of the centers of the lesion were measured. The X-ray images were independently examined by three doctors specialized in oral and maxillofacial surgery. Under the restriction of the study design, bone biopsy was prohibited in this clinical trial. Thus, bone regeneration by implantation of OCP/Col was qualitatively assessed by comparing radiographs before and 12 months after the implantation of OCP/Col.
Results
Macroscopic views
All participants uneventfully completed the clinical trial without major problems in their general condition, but postoperative swelling and pain was detected in most cases as also commonly seen in tooth extraction or cystectomy. And, each one case of pus discharge and wound dehiscence was observed. In this clinical trial, 4–22 disks of OCP/Col were implanted into the bone defect after cystectomy or tooth extraction. As many OCP/Col disks as possible were implanted to occupy the bone defect (Figure 2). Hemostasis in the OCP/Col-implanted site was satisfactory, and no implanted OCP/Col deviated from the bone defect during the operation, except that the case of pus discharge.

Macroscopic view before and after implantation of OCP/Col: (a) after tooth extraction, the extraction socket (*) was evident and (b) the disks of OCP/Col sponge were implanted into the extraction socket.
In terms of the local conditions after the implantation of OCP/Col, no postoperative bleeding was observed. No spontaneous pain was observed the day after the operation under conditions of using internal analgesics. However, within a week, oppressive pain was observed in seven cases. In all cases, the operative wound was swollen the day after the operation. Although the swelling in six cases decreased from 2 days after the operation, in the remaining four cases, the swelling of the operative wound continued for about 1 week.
In one case after cystectomy (C4), spillage of excessively implanted material and mild pus discharge from the operative wound were observed 1 week after the operation, although swelling and oppressive pain of the operative wound was not remarkable. Because the infected area seemed to be superficial, it was treated by removal of the spilled material and local irrigation with additional prescription of antibiotics for 5 days. Thereafter, the wound resolved without any difficulties. In another case (E1), it was caused by insufficient closure of the wound during the operation. It was controlled by local irrigation with additional prescription of analgesics for five times. Thereafter, the wound was healed without any difficulties.
Clinical laboratory findings
In the clinical laboratory examinations, no serious liver dysfunction, renal dysfunction, electrolyte imbalance, or abnormal urinalysis results were recognized without transient slight deviation from the normal range, especially immediate after operation. And it was confirmed no liver dysfunction, renal dysfunction, electrolyte imbalance, or abnormal urinalysis results existed at the end of this study. Although the number of white blood cells increased the day after the surgery, it almost recovered to within the normal limits after 1 week, at which level it was then maintained (Figure 3). In most cases, an increase in C-reactive protein (CRP) was observed the day after surgery, and it was maintained within the normal limits after 1 month. Although high CRP values were indicated in one case (E3) 1 day (10.5 mg/dL), it would be caused by many relief incisions for the ablated mucogingival flap made to assure the primary closure of the wound. Thus, severe facial and local swelling occurred and indicated high CRP values, although the general condition has no problem. After 1 week, facial and local swelling and CRP values (1.7 mg/dL) were reduced and the general condition has still no problem. After 1 month, the patient caught a bad cold and had fever (37.9°C = 100.2°F). The CRP values increased to 5.6 mg/dL, although the local condition was no problem. Three months later, the general and local condition was good, and the CRP values remained within normal limits (0–0.2 mg/dL).

Chronological change in the number of white blood cells (WBC). Although the number of WBC increased the day after surgery, it almost recovered to within the normal limits (gray zone) after 1 week, at which level it was maintained thereafter.
Radiographic findings
The operated region was scanned by CT before the operation and 3, 6, and 12 months after it, and the HU values of the centers of the lesion were measured. However, the CT data of C1 at 12 months was not taken for our technical error. For the tooth extraction cases, the CT values at pre-ope were excluded because the center of the lesion was occupied by the impacted tooth. OCP/Col itself has little radiopacity, and the CT value of the OCP/Col before implantation was from 130 to 140 HU. 23 The average HU values of the centers of the lesion detected at pre-ope, 3M, 6M, and 12M were 44.6, 299.7, 486.1, and 398.9, respectively (Table 3).
HU values of the bone defect.

CT: computed tomography; HU: Hounsfield Unit.
The average HU values increased between the preoperative and 6 months and they plateaued after 6 postoperative months.
The CT data of C1 at 12 months was not taken for our technical error.
Note: For the tooth extraction cases (E1~E5), the CT values at pre-Ope were excluded, because the center of the lesion was occupied by the impacted tooth. So, the column of CT values at pre-Ope of the tooth extraction cases (E1~E5) are shaded.
In this study, all cases qualitatively demonstrated an increase in radiopacity in the OCP/Col-implanted site. By adopting E3 as a representative case, the radiographic healing process was indicated if OCP/Col were implanted into the bone defect (Figure 4). The day after the implantation of OCP/Col, the extraction socket was clearly distinguished, and there was no increase in radiopacity in the OCP/Col-implanted site because OCP/Col itself had little radiopacity. After 1 month, the border of the extraction socket had become broader and unclear. In addition, the radiopacity in the OCP/Col-implanted site was increased throughout the defect. After 3 months, the border of the extraction socket became almost indistinguishable, and the radiopacity in the whole extraction socket was clearly increased. After 6 months, a trabecular-like structure was observed in the defect, and a cortical bone-like structure was indicated in part of the upper border of the extraction socket. After 12 months, the difference in the radiopacity between the OCP/Col-implanted site and the original bone became almost indiscernible. In the distal part of the second molar region, the newly formed bone was augmented near the cemento-enamel junction. In addition, the cortical bone-like structure was clearly indicated in part of the upper border of the extraction socket.

Radiographs after OCP/Col implantation. Before the operation (pre), the impacted wisdom tooth was observed. Radiopacity was not observed in the operated region the day after the operation (1D). After 1 month (1M), the border of the extraction socket became broader and unclear. After 3 months (3M), the border of the extraction socket became almost indistinguishable, and the radiopacity in the whole extraction socket clearly increased. After 6 months (6M), a cortical bone-like structure was indicated in part of the upper border of the extraction socket. After 12 months (12M), the difference in radiopacity between the OCP/Col-implanted site and the original bone became almost indiscernible.
Discussion
As bone regenerative material, OCP/Col has many prominent properties. First, OCP/Col achieved sufficient bone regeneration without exogenous cell transplantation and cytokines. 16 Then, OCP/Col significantly reinforced bone regeneration more than β-TCP collagen composite and HA collagen composite, whereas the implanted OCP/Col was significantly resorbed more than β-TCP Col or HA Col. 17 Moreover, the OCP/Col-derived bone would be remodeled and exhibited outer cortical and inner cancellous structures as well as original bone. 20 Finally, OCP/Col is easy to use and has no need for a complicated operation or management system.
The present report is the first to summarize the clinical evaluation of OCP/Col. Because the main purpose of this clinical trial was investigation of a safety verification of OCP/Col after implantation of tooth extraction socket and cyst hole, it was performed by a single-arm non-randomized intervention study on a small group. And this study design was consulted with the local IRB considering the ethical aspect of the study patients. Nevertheless, it should be performed with a comparative study, which includes a control cohort, such as autologous bone or other commercially available bone substitutes to secure the safety and efficacy of implantation of OCP/Col. However, these evidences were demonstrated in this clinical trial as follows.
Because all participants uneventfully completed this clinical study, it is suggested that the systemic safety after OCP/Col implantation in tooth extraction socket or cyst hole has been substantiated, although this trial was performed on only a small group. When OCP/Col was implanted into the bone defect, no postoperative bleeding was observed and hemostasis in the operative site was satisfactory. This suggests that OCP/Col would be a biomaterial that can be used safely. Since collagen is used as a hemostatic agent, 27 this collagen composite material might obstruct bleeding from bone defects during and after operations. The operative wound in all cases was swollen the day after the operation, and in the remaining four cases, swelling continued for about 1 week. However, these findings would also be observed in the clinical course of third molar surgery.28,29
In this study, each one case of pus discharge and wound dehiscence was observed. In the case of local infection (C4), the excessive OCP/Col implantation (12 disks) for the defect initiated the spillage of a part of material and it seemed to be caused by the superficial infection around them. Therefore, it should be considered that the excessive implantation of OCP/Col for the bone defect would cause the spillage of the material and the local infection. In case of local wound dehiscence (E1), it was caused by insufficient closure of the wound during the operation. It should be considered it is generally accepted that primary closure was needed to achieve predictable results, if bone grafts or bone substitute materials were applied to the bone defect. 30
It is reported that the implanted materials would be removed if pus discharge or local wound dehiscence progressed. 31 In this study, mild pus discharge from the operative wound and slight local wound dehiscence were observed in one case each, they were managed by local irrigation or observation, and healed without any difficulties. This suggests that OCP/Col might be associated with tolerance of slight bacterial contamination or mild mechanical disruption.
Even though no serious liver dysfunction, renal dysfunction, electrolyte imbalance, or abnormal urinalysis results were recognized in the clinical laboratory examinations, the number of white blood cells and CRP level were temporarily increased after the operation. A previous report indicated that increases in white blood cells and CRP were observed with the appearance of postoperative complications if third molar surgery was performed. 32 However, these data would have been collected after the onset of postoperative complications, not immediately after an operation. Therefore, the safety of OCP/Col implantation should be assured.
Because CT values are proportional to bone mineral density, it was used to evaluate bone healing in this study. In this study, the CT values of normal bone ranged from 100 to 600 HU in cancellous bone. The CT values of OCP/Col ranged from 130 to 140 HU. 23 Before implantation of OCP/Col in cyst cases, the average CT values of the bone defect was 44.6 HU. At 3 months after implantation of OCP/Col, the average CT values of the bone defect was increased to 299.7 HU. It suggests that OCP/Col is converted into hard tissue, such as cancellous bone, within 3 months of its implantation. It was increased to 486.1 HU after 6 months and decreased to 398.9 HU after 12 months. The discrepancies between these trends among each case might have been related to the local conditions at each site. Also, it might be correlation that the bone regeneration by OCP/Col tended to reach a plateau at 6 months. 19
The radiopacity in the defects at 12 months after implantation of OCP/Col was higher than that the day after the operation. This suggests that the implantation of OCP/Col would be effective for the restoration of bone defects. In terms of the radiographic findings, there was no increase in radiopacity in the OCP/Col-implanted site immediately after the operation, as OCP/Col itself had little radiopacity.17,23 Subsequently, the radiopacity in the OCP/Col-implanted site gradually increased by the apatitic conversion of OCP and new bone formation. 16 The essential feature in this material was that the increase in radiopacity in the bone defect was elicited from the margin of the bone defect and also the implanted OCP/Col. 16 Finally, the border between the original bone and the OCP/Col-implanted site became indistinguishable, and OCP/Col-derived bone was remodeled into outer cortical and inner cancellous structures, like original bone. 20 This suggests that this material would be a bone substitute with the properties of physiological remodeling.
This clinical study was limited to qualitative assessment by radiographic examination because bone biopsy was prohibited under the restriction of the study design. However, it was considered that the radiopacity in the OCP/Col-implanted site reflected newly formed bone, referring to our previous studies.17,18,21 In addition, it is necessary to discuss whether the implantation of OCP/Col would be notable for conventional treatment. On the basis of research achievements including this study, sponsor-initiated multicenter clinical trials of OCP/Col for bone defects in the oral and maxillofacial area (UMIN000018192) were recently conducted as multicenter clinical trials at several facilities in Japan, including Tohoku University, which will be the primary trial facility. This material with its many outstanding bone regenerative properties would be expected to be utilized in clinical situations in the future.
Footnotes
Acknowledgements
The authors thank Dr Seishi Echigo, Emeritus Professor of Tohoku University, for his excellent assistance in this study.
Declaration of conflicting interest
The authors (S.K. and O.S.) have obtained a patent for OCP/Col (#5046511) in Japan.
Funding
This study was supported, in part, by grants-in-aid for Scientific Research on Priority Areas (17076001) and Scientific Research (B) (19390490, 20300165, and 23390450) from the Ministry of Education, Science, Sports and Culture of Japan.