
Abstract
Background:
Antilipidemic therapy adherence to medication among patients with dyslipidemia and type 2 diabetes mellitus (T2DM) remains suboptimal, particularly in developing countries. Poor adherence to lipid-lowering therapy is associated with a significantly higher risk of major adverse cardiovascular outcomes in this population than in the general population.
Objectives:
This study aimed to assess the level of non-adherence to antilipidemic medications and associated socio-demographic and clinical factors among patients attending comprehensive specialized hospitals (CSHs) in Northwest Ethiopia.
Design:
This multicenter, prospective, cross-sectional study was conducted at CSHs in Northwest Ethiopia from November 10, 2023 to January 30, 2024.
Methods:
Data were entered using EpiData version 4.6.0.0 and analyzed using STATA version 17.0. The Adherence in Chronic Diseases Scale was used to assess medication adherence. Multinomial logistic regression analysis was used to identify factors associated with non-adherence, and model fitness was checked before interpretation.
Results:
The study included 398 patients, yielding a response rate of 98.76%. Of these patients, 290 (72.9%) were classified as non-adherent to their antilipidemic medications. Factors significantly associated with medium and low medication adherence included female sex (adjusted odds ratio (AOR) for medium: 2.94, 95% confidence interval (CI): 1.61–5.38; AOR for low: 3.09, 95% CI: 1.66–5.76), unmarried status (AOR for medium: 2.83, 95% CI: 1.52–5.27; AOR for low: 2.72, 95% CI: 1.43–5.17), current smoking (AOR for medium: 3.25, 95% CI: 1.20–8.82; AOR for low: 6.54, 95% CI: 2.46–17.36), presence of comorbidities (AOR for medium: 3.01, 95% CI: 1.65–5.49; AOR for low: 2.41, 95% CI: 1.29–4.47), and polypharmacy (⩾5 medications) (AOR for medium: 3.00, 95% CI: 1.60–5.63; AOR for low: 4.87, 95% CI: 2.56–9.24).
Conclusion:
This study revealed a high prevalence of medication non-adherence among patients with T2DM with dyslipidemia in Northwest Ethiopia. Non-adherence was significantly associated with female gender, unmarried status, smoking, comorbid conditions, and polypharmacy. These findings emphasize the need for targeted strategies to improve adherence in high-risk populations to enhance lipid control and lower the likelihood of cardiovascular complications.
Introduction
Dyslipidemia is among the major risk factors of cardiovascular disease, mainly in atherosclerotic cardiovascular disease (ASCVD). Dyslipidemia can be caused by abnormality of one or more of the most common lipid profiles, high-density lipoprotein cholesterol (HDL-C) reduction, and elevation of low-density lipoprotein cholesterol (LDL-C), total cholesterol (TC), and triglycerides (TGs) from the target level.1,2 Dyslipidemia is responsible for approximately 4.4 million deaths annually worldwide, 56% of ischemic heart disease cases, and 18% of strokes. 3 Low-density lipoprotein (LDL) is the principal aspect of dyslipidemia. The principal aspect of dyslipidemia is LDL. The rise in LDL (bad cholesterol) and reduction in HDL (good cholesterol) may have detrimental effects, and controlling LDL-C is a cornerstone in the prevention and treatment of ASCVD. 4
Dyslipidemia is very common in type 2 diabetes mellitus (T2DM), affecting about 72%–85% of patients, and the exact mechanism of diabetes-related lipoprotein abnormalities is unclear. Because patients with impaired fasting glucose, impaired glucose tolerance, and T2DM have been shown to have lipoprotein changes, including an increase in triglycerides (TG), an increase in very low density lipoprotein (VLDL) particles, small dense LDL particles, and a decrease in HDL level, insulin resistance has been implicated in the pathogenesis of diabetic dyslipidemia rather than hyperglycemia. 5 There are currently over 500 million cases of T2DM worldwide, and its prevalence is projected to increase by the end of 2030. 6 When combined with other risk factors for coronary artery disease (CAD), such as T2DM, abnormalities in lipid profiles can significantly elevate the risk of developing CAD.4,7
Dyslipidemia is frequently misdiagnosed and poorly managed in high-risk populations, such as individuals with T2DM 8 ; however, rates of morbidity and death could be lowered with proper management.4,9 The superior success of statins over non-statin therapies in treating atherosclerosis is attributed to their ability to reduce mortality rates and their generally favorable tolerability profile.4,10 However, statins are not free of adverse effects, such as muscle pain, neuropathy, hepatic dysfunction, and rhabdomyolysis.11,12 When patients with dyslipidemia cannot meet their treatment goals, ezetimibe, hypertime, and fibrates have generally been used as complementary therapies to statins. 13 Intolerant patients to statins who do not achieve their therapeutic goal, like those who remain with constant elevation of triglyceride levels, other drug therapies like Cholesteryl Ester Transfer Protein inhibitors and Proprotein Convertase subtilisin/kexin type 9 inhibitors, are useful in reducing cardiovascular risk. 14
Patients with dyslipidemia follow medication regimens that are too complex, involve multiple medications with probable adverse drug events, which cause medication non-adherence. 15 In developing countries like Ethiopia, patients’ awareness and adherence to antilipidemic drugs to manage dyslipidemia in patients with T2DM are suboptimal. Patients are unlikely to achieve the desired therapeutic outcomes without strict adherence to prescribed treatment regimens and necessary lifestyle modifications. 16 In addition to poor glycemic control and cardiovascular risk, dyslipidemia has a greater economic burden. 17
Although several studies in Ethiopia have explored factors associated with medication non-adherence in patients with chronic conditions, data specifically addressing non-adherence among patients with dyslipidemia. Patients with T2DM are at substantially higher risk for cardiovascular events, and dyslipidemia is a key modifiable risk factor. Poor adherence to lipid-lowering therapy in this population is associated with a significantly higher risk of major adverse cardiovascular outcomes compared with the general population. Understanding adherence patterns in this population is essential, as lipid-lowering therapy plays a vital role in reducing cardiovascular risk, especially among individuals with T2DM. Therefore, this study aimed to assess the level of medication non-adherence and identify its predictors among patients with dyslipidemia attending comprehensive specialized hospitals (CSHs) in Northwest Ethiopia. The findings of this study may support efforts to improve lipid profile control, mitigate cardiovascular and diabetes-related risks, and reduce the burden of dyslipidemia and its complications.
Methods
Study design and study period
A multicenter, institution-based prospective cross-sectional study was conducted from November 10, 2023 to January 30, 2024.
Study setting
The study included patients diagnosed with dyslipidemia and coexisting T2DM who were receiving follow-up care at ambulatory clinics of selected CSHs in Northwest Ethiopia. There are five major CSHs in this region: the University of Gondar CSH, Debre Tabor CSH, Felege Hiwot CSH, Tibebe Ghion CSH, and Debre Markos CSH. A simple random sampling (lottery) method was used to select participating centers from a list of five CSHs in Ethiopia’s northwest region. Each CSH name was written on a slip of paper, and the slips were drawn blindly to ensure random selection. Three CSHs were chosen to ensure geographic and population diversity.
The University of Gondar CSH is located approximately 750 km from Addis Ababa and serves a population of over 7 million people in the Amhara region. Debre Markos CSH, located 300 km from Addis Ababa, serves an estimated population of 5 million people. Debre Tabor CSH is situated 667 km from Addis Ababa and 104 km from Bahir Dar, serving over 3 million people. Felege Hiwot CSH and Tibebe Ghion CSH are both located in Bahir Dar, the capital of the Amhara region, approximately 565 km from Addis Ababa, and collectively serve approximately 5 million people.
Inclusion criteria of study participants
Patients aged ⩾18 years with a confirmed diagnosis of dyslipidemia for more than 6 months and who were on antilipidemic therapy among patients with T2D, who attended and are attending ambulatory clinics of CSHs, and who signed the written informed consent were included in this study. Patients with cognitive impairment (confirmed diagnosis) were excluded from the study. Patients who were unwilling to participate in the study and did not sign the informed consent were excluded from the study.
Variables of the study
The dependent variable was the level of medication adherence (high, medium, and low adherence). The explanatory variables included the gender, age, body mass index (kg/m2), residence, marital status, educational level, employment status, social habits (smoking, alcohol consumption), number of drugs used, presence of comorbidity, antilipidemic drug prescribed, place of residence, previous medical and medication history, patterns of dyslipidemia, lipid abnormality status, HbAlc status, and duration of diabetes mellitus.
Determination of sample size
The sample size was calculated using a single population proportion formula based on the assumptions of a 95% confidence level, a 5% margin of error, and a proportion (p) of 50.0%, as the rate of medication non-adherence among patients with dyslipidemia in Ethiopia is currently unknown. Therefore, n = [(Z1 − α/2) 2 * p * (1 − p)]/d², n = [(1.96) 2 (0.5) (1−0.5)]/(0.05) 2 = 384; using a contingency of 5%, that is, 384 *10% = 19; the calculated sample size was 384 + 19 = 403. Where d = margin of error, p = proportion of the sample population, Za/2 = the value under a standard normal table using a 95% confidence interval (CI), and n = the total sample size. Proportional allocation of samples to the total population of each CSH ambulatory clinic was applied. The lottery method was used, and Debre Tabor, Felege Hiwot, and Debre Markos CSHs were selected (Figure 1):
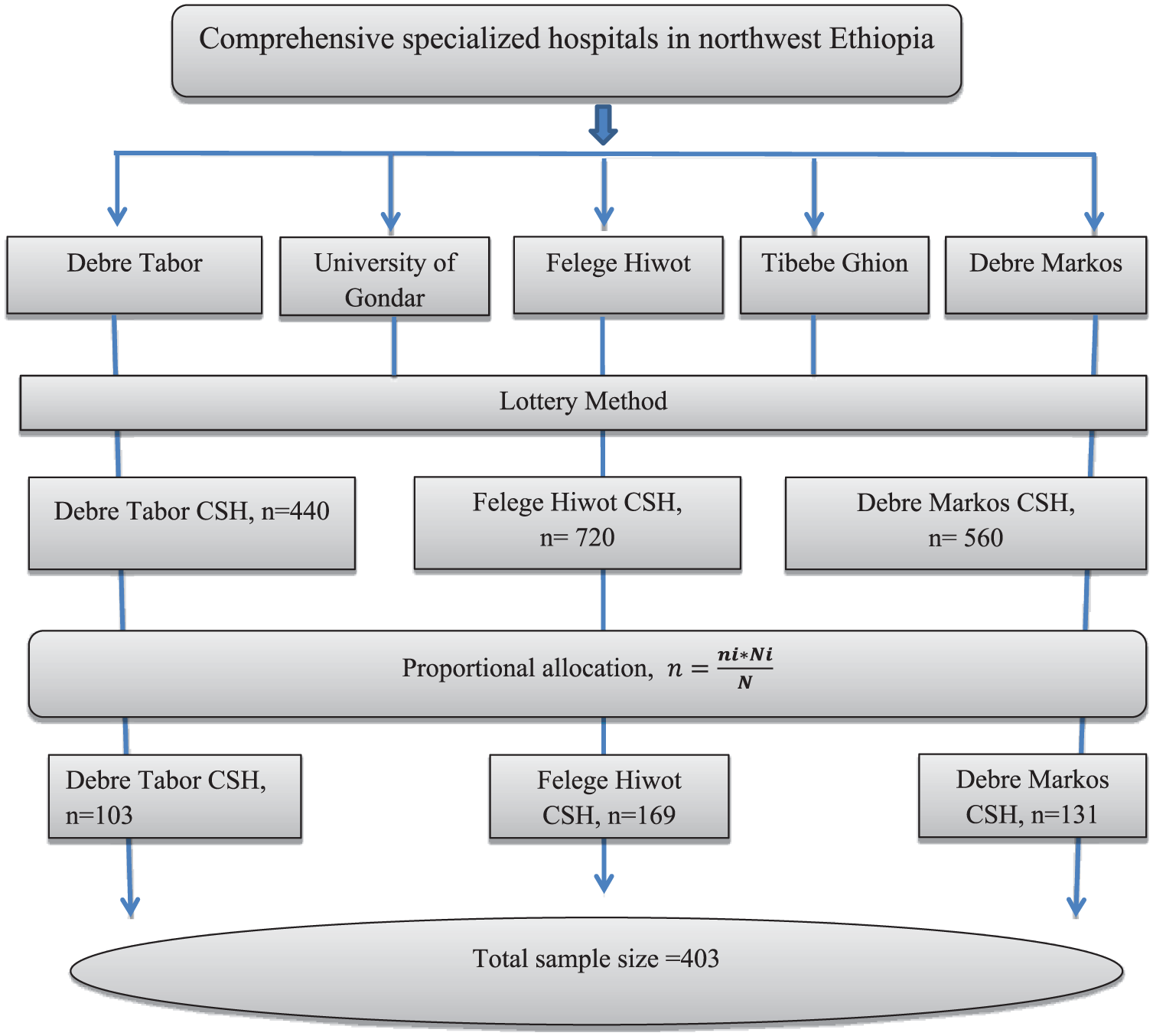
Diagrammatic representation of the sampling procedure.

where n = total sample size to be selected, N = total population, Ni = total population of patients with T2DM and dyslipidemia at each CSH ambulatory clinic, and ni = sample size from each CSH ambulatory clinic.
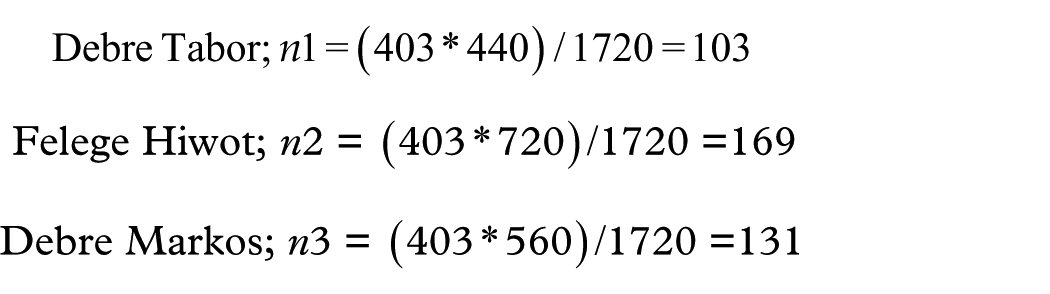
The total calculated sample size was 403 (n1 + n2 + n3), but the current study included 398 patients selected through a stratified sampling technique, resulting in a response rate of 98.76% (398/403). Five participants withdrew from the study due to their unwillingness to participate.
Data collection procedure and quality control
Following a review of the previous literature, a questionnaire was prepared.16,18–29 After receiving 1 day of training on the study’s objectives, data collection tools, and ethical considerations, fifth-year pharmacy students served as data collectors. The supervisor conducted regular oversight throughout the study. A pretest was conducted on 5% of patients at the Tibebe Ghion Comprehensive Specialized Hospital 7 days before the actual data collection, to ensure clarity and logical sequence. Cronbach’s alpha was measured to assess the tool’s reliability and consistency for medication adherence, yielding a value of 0.83, which falls within an acceptable range. Patients who are 18 years and above have had a dyslipidemia diagnosis for more than 6 months, and who have at least one antilipidemic drug are included in this study. Patients with cognitive impairment (confirmed diagnosis) were excluded from the study. During their outpatient visit, patients were evaluated using their medical charts to determine eligibility for the study. Socio-demographic variables and clinical characteristics were extracted from both medical charts and interviews of each patient.
Medication adherence of diabetic dyslipidemia patients was determined using the Adherence in Chronic Diseases Scale, which consists of seven (7) questions. The responses of patients were rated out of 4 (0–4 points) and the total sum of adherence for each patient ranges from 0 to 28 they were classified as follows; a total score >26 points is considered as high adherence, medium adherence with a score of 21–26 and with a score of <21 points as low medication adherence. The medication adherence tool is available free of charge on the website of Nicolaus Copernicus University. 30
Operational definitions
Dyslipidemia: Defined as the presence of at least one of the four lipid abnormalities (HDL, LDL, TG, and TC) in the serum lipid profile. 31 The diagnosis was based on clinical records and the current prescription of lipid-lowering medication during the data collection period. The diagnostic criteria followed the guidelines of the American Diabetes Association and National Cholesterol Education Program Adult Treatment Panel III, which define dyslipidemia based on elevated LDL-C, low HDL-C, or elevated triglycerides.
Low levels of HDL-C: HDL-C level ⩽40 mg/dl (⩽1.03 mmol/l) in men and ⩽50 mg/dl (⩽1.29 mmol/l) in women. 32
High LDL-C levels: expressed as LDL-C level ⩾100 mg/dl (⩾2.59 mmol/l). 32
High level of TC (Hypercholesterolemia): defined as TC level ⩾200 mg/dl (⩾5.17 mmol/l). 32
High level of TGs (Hypertriglyceridemia): defined as TG level ⩾150 mg/dl (⩾1.70 mmol/l). 32
Body mass index (BMI): defined as healthy weight (BMI = 18.5–24.9 kg/m2), overweight (BMI = 25–29.9 kg/m2), and obese with a BMI of 30 kg/m2 or greater. 33
Hypertension: High blood pressure, that is, systolic blood pressure ⩾140 mmHg or diastolic blood pressure ⩾90 mmHg, 34 and other comorbidities were defined as a documented previous diagnosis using evidence-based diagnosis methods.
Medication adherence was categorized as high (total score >26 points), medium adherence (21–26), and low adherence (score <21 points). 30
Data management and statistical analysis
The collected data were entered into the EpiData (version 4.6.0.0) and then exported to STATA version 17.0 for analysis. Descriptive statistics, including frequency, percentage, mean, median, interquartile range (IQR), and standard deviation, were used to summarize patients’ socio-demographic, clinical, and medication-related characteristics. Categorical values were reported as frequencies with percentages, and continuous variables were reported as means with standard deviations (±SD) or medians with IQR based on the distribution. Outliers and multicollinearity of the variables were checked before running the regression model. The assumption of multicollinearity was checked by the variance inflation factor and tolerance test, and no significant multicollinearity was observed.
The dependent variable was ordinal (high, medium, and low adherence) and initially analyzed using an ordinal logistic regression model. However, after testing the model’s assumptions, the test of parallel lines (proportional odds) was violated (p < 0.05), preventing further use of this model despite meeting the other assumptions. Because of this, a multinomial logistic regression model, which can be run without considering the rank of the response category, was chosen for analysis. In this multinomial logistic regression model, high adherence to medications was set as the reference category, while medium and low adherence were treated as alternative categories.
Bivariate and multivariate multinomial logistic regression analyses were conducted to identify statistically significant variables. Variables with p-values less than 0.25 in the bivariate multinomial logistic regression analysis showing significant associations with either medium or low adherence were selected as candidates for the multivariate multinomial logistic regression to control for potential confounding effects. Lastly, statistically significant variables were established at p-value <0.05 in a multivariate multinomial logistic regression model, and an adjusted odds ratio (AOR) with a 95% CI was reported to measure the strength of association.
Model fit was assessed using the likelihood chi-square test (χ2 = 151.804, df = 30, p < 0.001), which was significant, indicating that the full model provides a significantly better fit than the null model. The model’s goodness-of-fit was evaluated using the Pearson chi-square test (χ2 = 760.269, df = 716, p = 0.122) and the deviance chi-square test (χ2 = 680.903, df = 716, p = 0.823), both of which were not significant, indicating an adequate model fit. Both tests indicated that the model fits the data set effectively. Therefore, these numerical figures showed that the overall model adequately described the data. Nagelkerke’s (pseudo R2) showed how much the independent variables explain the response variable (practice adherence score) by 35.8% in the model. The overall percentage of accuracy rate (predictor variables’ percentage of prediction on the response variable category) of the multinomial logistic regression model was very good at 57.5% in the present study.
Results
Socio-demographic characteristics of the study participants
A total of 398 participants were included in the study, resulting in a response rate of 98.76% (398 out of 403). Among them, 225 (56.5%) were male, and 151 (37.9%) were between the ages of 28 and 50. The median age of the participants was 56 years, with an age range of 28–76 years. Nearly half, 185 individuals (46.5%), were classified as overweight, while 155 (38.9%) were considered obese. In terms of education, 128 participants (32.2%) had completed secondary school. Most participants, 224 (56.3%), lived in urban areas, and 248 (62.3%) were employed in government, private, or self-owned businesses. In addition, 74 participants (18.6%) reported smoking, and 64 (16.1%) reported alcohol use (Table 1).
Socio-demographic characteristics of the study participants (n = 398).

Clinical, vital signs, and laboratory findings of the study participants
In the present study, over half of the participants (59.5%) had comorbid conditions aside from dyslipidemia and diabetes. Hypertension was the most common comorbidity, reported in 262 individuals (65.8%), and followed by ASCVD in 250 participants (62.8%). Lipid profile analysis indicated that approximately 263 participants (66.1%) had uncontrolled lipid abnormalities. Elevated LDL-C was present in 234 participants (58.8%), while high TC (hypercholesterolemia) was observed in 269 individuals (67.6%). In addition, the majority of participants, 280 (70.35%), had HbA1c levels above 7%, indicating poorly controlled diabetes (Table 2).
Clinical and laboratory findings of the study participants at comprehensive specialized hospitals’ ambulatory clinics in Northwest Ethiopia (n = 398).

ASCVD, atherosclerotic cardiovascular disease; CKD, chronic kidney disease; HbA1c, glycated hemoglobin; HTN, hypertension; IHD, ischemic heart disease.
Patterns of dyslipidemia, antilipidemic drug therapy, and level of adherence
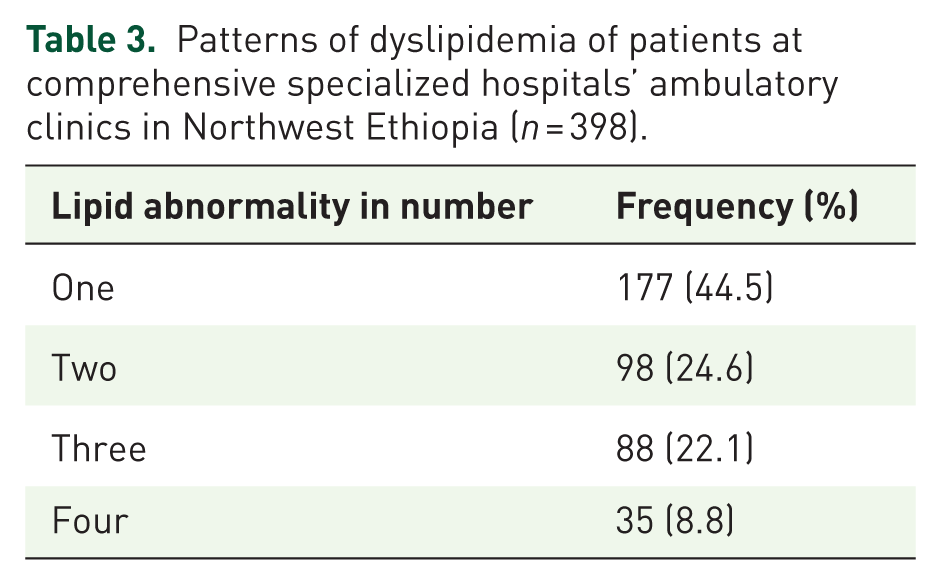
The most common patterns of dyslipidemia observed were low HDL-C in 278 participants (69.8%) and high LDL-C in 234 participants (58.8%) (Figure 2). About 177 (44.5%) of the study participants had one lipid abnormality, and 35 (8.8%) had all four lipid abnormalities (Table 3). More than one-third (36.9%) of participants were taking moderate-intensity statins (Figure 3). In the present study, the level of medication non-adherence was 290 (72.9%), and 108 (27.1%) and 140 (35.2%) of the study participants were high adherent and low adherent to their medications, respectively (Figure 4).

Lipid abnormality of patients at comprehensive specialized hospitals’ ambulatory clinics in Northwest Ethiopia (n = 398).
Patterns of dyslipidemia of patients at comprehensive specialized hospitals’ ambulatory clinics in Northwest Ethiopia (n = 398).

Antilipidemic drug therapy of the study participants at comprehensive specialized hospitals’ ambulatory clinics in Northwest Ethiopia (n = 398).

Medication adherence level of the study participants at comprehensive specialized hospitals’ ambulatory clinics in Northwest Ethiopia (n = 398).
Multinomial logistic regression analysis of factors associated with medication adherence
Bivariate multinomial logistic regression analysis identified several variables with a p-value <0.25 that were potentially associated with either medium or low levels of medication adherence. These included age, gender, place of residence, marital status, employment status, smoking and alcohol habits, presence of comorbid conditions, number of medications taken, history of medication use, use of lipid-lowering agents, and duration of diabetes.
Subsequent multivariable multinomial logistic regression analysis revealed that female gender, unmarried status, smoking habit, presence of comorbidities, and the use of five or more medications were significantly associated with both medium and low adherence to medications. In addition, diabetes duration greater than 10 years, history of medication use for ⩾1 year, unemployment, and alcohol consumption were significantly associated with medium adherence. Furthermore, age between 28 and 50 years was significantly associated with low adherence.
When compared to patients with high adherence to medications, female participants had significantly higher odds of both medium (AOR = 2.94; 95% CI: 1.61–5.38; p < 0.001) and low adherence (AOR = 3.09; 95% CI: 1.66–5.76; p < 0.001). Unmarried individuals demonstrated increased odds of medium (AOR = 2.83; 95% CI: 1.52–5.27; p = 0.001) and low adherence (AOR = 2.72; 95% CI: 1.43–5.17; p = 0.002) compared to their married counterparts. Current smokers exhibited significantly higher odds of medium (AOR = 3.25; 95% CI: 1.20–8.82; p = 0.020) and low adherence (AOR = 6.54; 95% CI: 2.46–17.36; p < 0.001) relative to non-smokers. Patients with comorbid conditions had greater odds of medium (AOR = 3.01; 95% CI: 1.65–5.49; p < 0.001) and low adherence (AOR = 2.41; 95% CI: 1.29–4.47; p = 0.005). Taking five or more medications was associated with increased odds of medium (AOR = 3.00; 95% CI: 1.60–5.63; p = 0.001) and low adherence (AOR = 4.87; 95% CI: 2.56–9.24; p < 0.001) when compared to those on fewer medications (1–4 medications).
Additional associations were observed for medium adherence: participants with a diabetes duration greater than 10 years had higher odds of medium adherence (AOR = 1.85; 95% CI: 1.01–3.37; p = 0.046). A history of medication use for ⩾1 year was associated with higher odds of medium adherence (AOR = 2.13; 95% CI: 1.13–4.01; p = 0.019). Unemployed individuals were more likely to exhibit medium adherence (AOR = 1.94; 95% CI: 1.07–3.51; p = 0.006). Alcohol consumption was associated with significantly lower odds of medium adherence (AOR = 0.34; 95% CI: 0.14–0.83; p = 0.018), indicating a potential protective association. Lastly, patients aged 28–50 years were more likely to have low adherence, with nearly 2.78 times greater odds compared to older individuals (AOR = 2.78; 95% CI: 1.29–5.98; p = 0.009) (Table 4).
Bivariate and multivariable multinomial logistic regression analyses of factors associated with medication non-adherence level of patients with dyslipidemia at comprehensive specialized hospitals’ ambulatory clinics in Northwest Ethiopia (n = 398).

Bold = statistically significant (p < 0.05); 1 = reference.
Unmarried = divorced, separated, widowed, or single. AOR, adjusted odds ratio; CI, confidence interval; COR, crude odds ratio; N/B, high adherence to medications is the reference category in this model.
Discussion
Medication non-adherence poses a major challenge in the management of patients with T2DM and dyslipidemia, substantially elevating their risk of cardiovascular complications. 16 Addressing the multifactorial causes of medication non-adherence is crucial for improving clinical outcomes in patients with T2DM and dyslipidemia. Non-adherence to prescribed therapies can result in suboptimal disease control, increased risk of complications, and greater healthcare expenditures. Individuals with T2DM face a markedly elevated risk of cardiovascular events, with dyslipidemia representing a key modifiable contributor. Poor adherence to lipid-lowering therapy in this population has been linked to a significantly higher incidence of major adverse cardiovascular events compared to the general population. 17 A multidisciplinary approach involving physicians, nurses, and clinical pharmacists, combined with patient-centered interventions, can enhance medication adherence and help reduce cardiovascular events.4,9 This study aimed to evaluate the level of medication non-adherence and identify its associated factors among dyslipidemia patients with diabetes attending ambulatory clinics at CSHs in Northwest Ethiopia.
The findings reveal a high prevalence of medication non-adherence, with 72.9% of patients exhibiting either medium or low adherence to their prescribed lipid-lowering medications. This study finding is in line with the previous studies, 26 but higher than other studies conducted so far.25,35 The higher non-adherence rate in our study population could be attributed to various factors, including socioeconomic challenges, limited health literacy, and inadequate patient education about the importance of medication adherence in managing dyslipidemia.
The multivariable multinomial logistic regression analysis revealed several factors that were significantly associated with medium and low adherence to medications. Female gender, being unmarried, having a smoking habit, the presence of comorbidities, and a higher number of prescribed medications (⩾5) were all found to increase the odds of both low and medium adherence compared to high adherence. Gender emerged as a significant factor associated with medication non-adherence, with female patients showing higher odds of both medium and low adherence compared to males (AOR: 2.94, 95% CI (1.61–5.38)) and (AOR: 3.09, 95% CI (1.66–5.76)), respectively. This finding aligns with previous research that has identified gender disparities in medication adherence across various chronic conditions.22,36–38 The reasons for this disparity may be multifaceted, potentially involving differences in health-seeking behaviors, socioeconomic factors, and competing responsibilities that disproportionately affect women in these settings. Interventions from both the public and healthcare professionals should target cultural, socioeconomic, and psychosocial factors such as caregiving responsibilities, differences in health literacy, and healthcare access, focusing on females. This approach can help reduce medication non-adherence and ultimately improve medication optimization and overall female health.
Marital status emerged as a significant predictor of medication non-adherence, with unmarried individuals showing higher odds of both medium and low adherence compared to their married counterparts (AOR: 2.83, 95%CI (1.52, 5.27)) and (AOR: 2.72, 95% CI (1.43, 5.17)), respectively. This study’s findings were consistent with the previous studies in Lebanon, 23 Australia, 39 and Finland. 38 This association could be explained by the potential lack of social support and reminders that married individuals might receive from their partners, which can play a crucial role in maintaining medication adherence. 40
Our study findings revealed that the presence of comorbidities and the number of prescribed medications were significantly associated with increased odds of non-adherence. Patients with comorbidities (AOR: 3.01, 95% CI (1.65–5.49)) and (AOR: 2.41, 95% CI (1.29–4.47)), respectively, and those with polypharmacy (AOR: 3.00, 95% CI (1.60–5.63)) and (AOR: 4.87, 95% CI (2.56–9.24.90)), respectively, were more likely to exhibit non-adherence than their counter parts. These findings are in line with the existing literature,19,22,35,37,41 highlighting the challenges faced by patients managing multiple health conditions simultaneously. The increased pill burden and potential side effects associated with polypharmacy may contribute to reduced adherence among these patients.
Lifestyle factors, particularly smoking habits, demonstrated a strong association with medication non-adherence. Patients who smoked had significantly higher odds of both medium and low adherence compared to non-smokers (AOR: 3.25, 95% CI (1.20–8.82)) and (AOR: 6.54, 95% CI (2.46–17.36)), respectively. The association between smoking habits and lower adherence is likely due to the potential impact of nicotine addiction on self-care behaviors. 42 This finding is consistent with previous studies23,39; while alcohol consumption was associated with lower odds of medium adherence,23,43 it warrants further investigation into the complex relationship between alcohol use and medication-taking behaviors. Employment status emerged as a factor influencing medium adherence, with unemployed patients showing higher odds of medium adherence compared to employed individuals. This finding highlights the potential impact of socioeconomic factors on medication adherence and underscores the need for interventions that address financial barriers to treatment adherence. This was in line with the existing literature.18,24,39
Patients with a prolonged duration of diabetes (>10 years) had higher odds of medium adherence to medications compared to those with a shorter duration of diabetes, with an (AOR: 1.85; 95% CI (1.01–3.37)). Patients with a medication use history of 1 year or more had higher odds of medium adherence compared to high adherence than those with a shorter medication use history (AOR: 2.13; 95% CI (1.13, 4.01)). This recommends that while awareness of long-term medication use may improve adherence to some extent, it does not necessarily translate to high adherence. Younger patients (28–50 years) showed higher odds of low adherence compared to older age groups (AOR: 2.78; 95% CI (1.29–5.98)), which may reflect differences in perceived risk and the importance of medication adherence across age groups.21,38 Unemployed patients had higher odds of medium adherence compared to high adherence than employed patients (AOR: 1.94; 95% CI (1.07, 3.51)).
Despite the availability of highly efficacious antilipidemic medications, non-adherence is a prevalent public health concern that contributes to significant healthcare costs and detrimental health treatment outcomes. 44 Treatment adherence of patients with dyslipidemia can contribute to therapy efficacy and better treatment outcomes. 45 The findings highlight the intricate relationship between socio-demographic, lifestyle, and clinical factors in shaping medication adherence behaviors. To address this issue, multifaceted interventions targeting modifiable risk factors, such as smoking cessation programs, simplification of medication regimens, and enhanced patient education, should be implemented in patients with dyslipidemia in all healthcare settings.
Strengths and limitations of the study
This study’s strengths include the application of robust statistical analyses, the comprehensive assessment of multiple contributing factors, and its multicenter design, which collectively enhance the generalizability and relevance of the findings. However, the cross-sectional nature of the study limits the ability to infer causal relationships. Furthermore, the reliance on self-reported data introduces the potential for recall bias and social desirability bias, which may affect the accuracy of responses and should be acknowledged as methodological limitations.
Conclusion and recommendations
The present study revealed a high burden of non-adherence to medications among patients with dyslipidemia and identified various modifiable risk factors that can be targeted to improve adherence. To address the various factors contributing to non-adherence from multiple perspectives, healthcare providers, including physicians, nurses, and clinical pharmacists, should integrate tailored adherence-enhancing strategies. Such strategies may include patient education, effective communication, medication simplification, and the provision of social support. They should also have a motive in medication prescribing, rational drug use, and lowering lipid abnormalities of patients to the target level. Healthcare institutions should establish a systematic approach to implement medication adherence monitoring and interventions, such as using pill counts, self-reported measures, or electronic monitoring devices.