
Abstract
Background:
Epidemiological studies have suggested that vitamin D deficiency is associated with the development of type 2 diabetes (T2DM) and is related to diabetes complications. This study was undertaken to determine the relationship between diabetes complications and cardiovascular risk factors with vitamin D3 and its metabolites: 1,25-dihydroxyvitamin D3 (1,25(OH)2D3), 25-hydroxyvitamin D3 (25(OH)D3), 24,25-dihydroxyvitamin D3 (24,25(OH)2D3); and 25-hydroxy-3epi-vitamin D3 (3epi25(OH)D3).
Methods:
750 Qatari subjects, 460 (61.3%) with and 290 (38.7%) without T2DM, who were not taking vitamin D3 supplements, participated in this cross-sectional, observational study. Plasma concentrations of vitamin D3 and its metabolites were measured by liquid chromatography tandem mass spectrometry analysis.
Results:
T2DM subjects had lower concentrations of all vitamin D3 metabolites (p < 0.001) except 3epi25(OH)D3 (p < 0.071). Males had higher concentrations of all vitamin D3 metabolites (p < 0.001). In the T2DM subjects, lower 25(OH)D3 was associated with retinopathy (p < 0.03) and dyslipidemia (p < 0.04), but not neuropathy or vascular complications; lower 1,25(OH)2D3 was associated with hypertension (p < 0.009), dyslipidemia (p < 0.003) and retinopathy (p < 0.006), and coronary artery disease (p < 0.012), but not neuropathy; lower 24,25(OH)2D3 concentrations were associated with dyslipidemia alone (p < 0.019); 3epi25(OH)D3 associated with diabetic neuropathy alone (p < 0.029). In nondiabetics, 25(OH)D3, 1,25(OH)2D3 and 24,25(OH)2D3 were associated with dyslipidemia (p < 0.001, p < 0.001, p < 0.015, respectively) and lower 1,25(OH)2D3 was associated with hypertension (p < 0.001). Spearman’s correlation showed 1,25(OH)2D3 to be negatively correlated to age and diabetes duration.
Conclusions:
Different diabetes complications were associated with differing vitamin D parameters, with diabetic retinopathy related to lower 25(OH)D3 and 1,25(OH)2D3 levels, hypertension significantly associated with lower 1,25(OH)2D3, while dyslipidemia was associated with lower 25(OH)D3, 1,25(OH)2D3 and 24,25(OH)2D3. While 25(OH)D metabolites were lower in females, there was not an exaggeration in complications.
Background
Accumulating evidence suggests that vitamin D deficiency increases the risk of type 2 diabetes (T2DM).1,2 Deficiency of vitamin D is associated with both insulin resistance and beta cell dysfunction. 3 As long ago as 1980, impaired insulin secretion was demonstrated in isolated perfused rat pancreas in the setting of vitamin D deficiency. 4 Later reports suggested that vitamin D deficiency could contribute to metabolic syndrome and T2DM.5,6 Vitamin D appears to exert its antidiabetic effect through modulation of hepatic glucose and lipid metabolism versus activation of calcium and the adenosine monophosphate–activated protein kinase (AMPK) pathway, and through promotion of beta cell function and survival. 7
A large prospective study of women, with 20 years of follow up, reported an inverse relationship between vitamin D concentrations and the onset of diabetes. 8 Vitamin D deficiency in T2DM has also been correlated with microvascular complications of retinopathy, neuropathy and nephropathy,9,10 though there is still some debate.
Vitamin D3 (cholecalciferol) is endogenously produced by UV-B irradiation of 7-dehydrocholesterol, while ergosterol is derived from the diet (primarily from mushrooms and fungi) and converted to previtamin D2 (ergocalciferol) by UV-B light, though both are hydroxylated to 25(OH)D3 and 25(OH)D2, respectively, by multiple 25-hydroxylases in the liver (Figure 1). 11 25(OH)D is transported to the kidney and converted to either the active 1,25(OH)2D by 1 alpha hydroxylase, or to 24,25(OH)2D, which is also active, by the 24 alpha hydroxylase present in the renal tubular cells (Figure 1). 12 It has recently been reported that extrarenal tissues may also convert 25(OH)D to 1,25(OH)2D, although, notably, activation in renal and non-kidney tissues is regulated differently with macrophage production of 1,25(OH)2D through the type 2 interferon response. 13 1,25(OH)2D binds to the vitamin D receptor (VDR) but, to exert its effect (which may take several hours), it heterodimerizes with the retinoid X receptor; 12 however, reports suggest alternative, more rapid mechanisms of action through binding to membrane VDR or through the 1,25D-membrane-associated, rapid response steroid-binding protein receptor with activation of protein kinases A and C. 14 Obesity can exacerbate vitamin D deficiency through decreased bioavailability due to deposition of vitamin D in the body fat compartments. 15 In many countries, vitamin D2 is available as a pharmaceutical and a supplement to counter vitamin D deficiency. 16
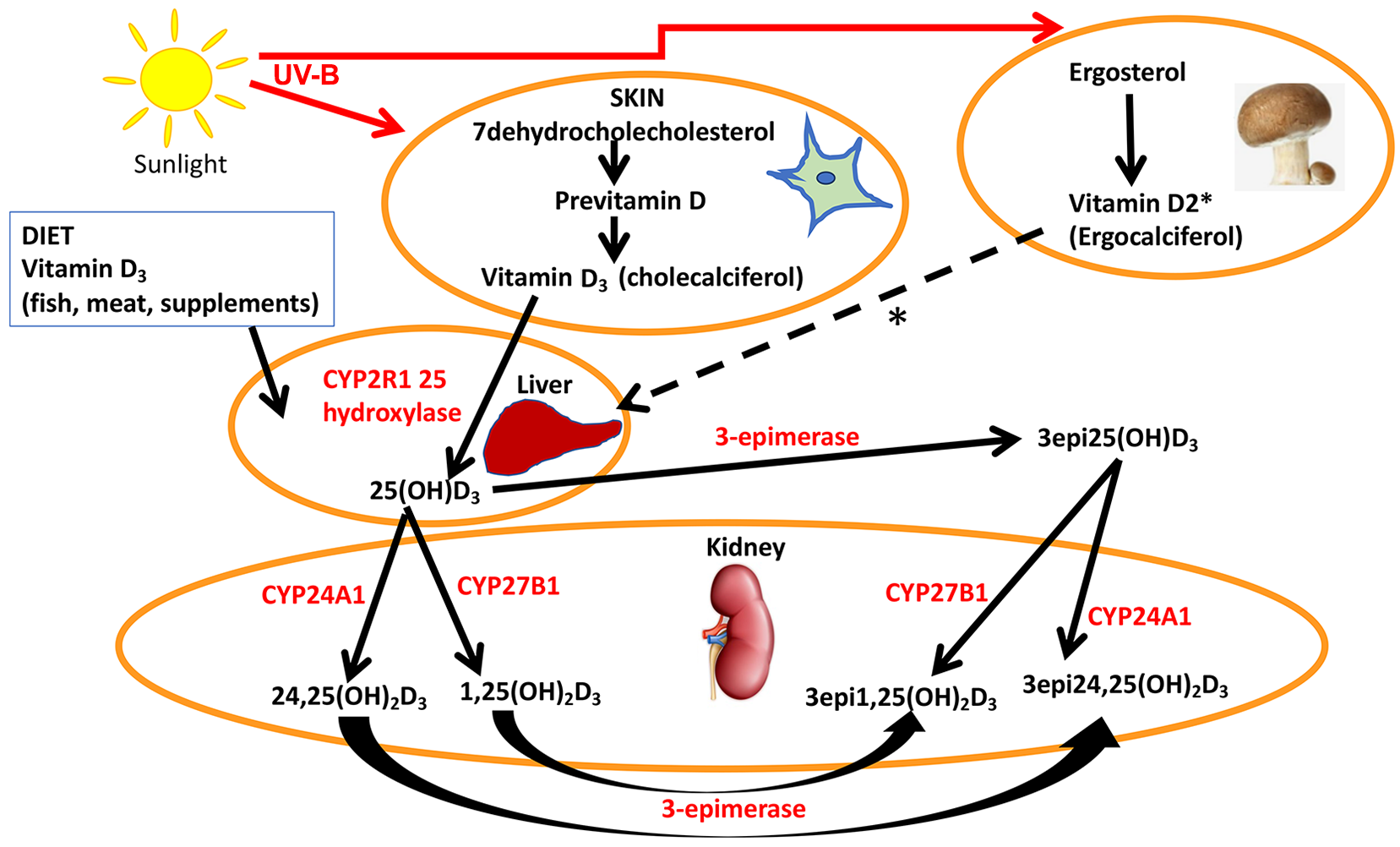
A simplified schematic representation of the synthesis and metabolism of vitamin D.
While vitamin D deficiency is a global issue, 17 cultural norms dictating full-body coverage in parts of the world such as the Middle East magnify the issue of vitamin D deficiency in these regions. 18
In Qatar, T2DM is a particularly serious health issue affecting approximately 20% of the population, a figure 2–3 times higher than the world average. 19 As a consequence, the burden associated with diabetes complications in Qatari patients is tremendous. A total of 43% of patients referred to dialysis have diabetic nephropathy. 20 A significant proportion of the total patient population presenting with cardiac pathologies in Qatar have T2DM: 57% of patients presenting with acute heart failure, and 30% of atrial fibrillation patients. 21
The aim of this study was specifically to answer the question as to whether vitamin D deficiency was associated with diabetes retinopathy. In addition, given the pervasively low vitamin D status in the Middle East, we hypothesized that full-body coverage for women would lead to lower vitamin D parameter concentrations compared to men and lead to increased diabetes complications.
Methods
Study population
A total of 750 Qatari patients, 460 (61.3%) with T2DM, were recruited from the Hamad outpatient clinic, along with 290 (38.7%) nondiabetic participants, who were relatives accompanying the T2DM patients to their clinic visits from July 2013 to July 2015, as part of a study investigating gene expression and genomics in individuals with diabetes (Table 1). None of the diabetic patients were taking vitamin D3 supplements, though all had been prescribed vitamin D2 supplements.
Demographic data and vitamin D3 levels in the control (n = 290) and type 2 diabetic (n = 460) groups.

BMI, body mass index; HbA1c, glycosylated hemoglobin A1c; 1,25(OH)2D3, 1,25-dihydroxyvitamin D3; 25(OH)D3, 25-hydroxyvitamin D3; 24,25(OH)2D3, 24,25-dihydroxyvitamin D3; 3epi25(OH)D3, 25-hydroxy-3epi-vitamin D3; IQR, interquartile range.
Inclusion criteria were male or female Qataris, aged 30 years or older. The diagnosis of T2DM was made according to the WHO guidelines; 22 for inclusion in the T2DM group, at least one of the following was required: fasting plasma glucose >7 mmol/L, HbA1c >6.5%, or a diagnostic glucose tolerance test. Inclusion in the nondiabetic control group required a normal glucose tolerance test. Patients were excluded from the study if they had a diagnosis of type 1 diabetes or any active form of diabetes, such as gestational diabetes or diabetes secondary to steroid treatment. All diabetes patients had retinal photography, a clinical foot examination, blood pressure measurement and urine analyzed for the albumin:creatinine ratio collected at their outpatient visit. Dyslipidemia was defined as a total cholesterol greater than 190 mg/dl (>4.9 mmol/L) and/or fasting triglycerides greater than 150 mg/dl (>1.7 mmol/L) untreated, or if patients were under treatment.
The study was approved by Weill Cornell IRB (IRB# 13-00063) and all participants provided written informed consent. The conduct of the trial was in accordance with ICH GCP and the Declaration of Helsinki.
Study design
Following an overnight fast, blood samples were collected, and weight and blood pressure were measured at the baseline visit. Fasting venous blood was collected into fluoride oxalate and serum gel tubes. Samples were separated by centrifugation at 2000 g for 15 min at 4°C, and the blood, serum and plasma aliquots were stored at −80°C within 1 h of collection. Overnight urine samples were collected, and aliquots were stored at −80°C until batch analysis. Blood pressure was measured using an automated device (NPB-3900; Nellcor Puritan Bennett, Pleasanton, CA, USA) during each study visit. Blood pressure measurements were performed after the participants had been seated quietly for at least 5 min and with the right arm supported at heart level. Three readings were taken, each at least 2 min apart, and then the average of the readings was calculated.
Serum vitamin D and metabolite measurements
Serum vitamin D concentrations were quantified using isotope-dilution liquid chromatography tandem mass spectrometry (LC-MS/MS). A total of 25µl of internal standards (d6-1calcitriol (1.5 ng/ml), d6-25OHD3 (50 ng/ml) and d6-epi-25(OH)D3 (20 ng/ml)) was added into each microcentrifuge tube containing 250 µl of calibration standards, quality control or serum samples, and kept for 30 min to reach binding equilibrium. The samples were diluted with 250 µl of pretreatment solution (isopropanol and water; 50:50 v/v) and left to stand for at least 15 min to displace binding protein.
Pretreated samples of 300 µl were loaded onto ISOLUTE® supported liquid extraction (SLE+) columns (Biotage), followed by elution with 1.8 ml of n-heptane (2 × 900 µl) into a collection tube already containing 200 µl of 0.25 mg/ml PTAD solution in ethyl acetate and heptane (8:92 v/v). The eluate was evaporated to dryness using turbovap under nitrogen gas heated at 38°C. Once dried, 50 µl of reconstituted solution consisting of methanol and deionized water, 70:30 v/v, and 0.006% methylalamine were added into all tubes. The derivatized extracts were transferred into LC insert vials and 10 µl from each was injected into the LC-MS/MS system. Data for the 25(OH)D3 and metabolite validation are shown in Supplemental Table 1.
Diabetes-related complications
Coronary artery disease (CAD) was defined as a history of myocardial infarction or angina, confirmed by coronary angiography. Peripheral arterial disease (PAD) was defined as a history of claudication or rest pain with evidence of artery stenosis on ultrasound or lower limb angiography. Stroke was defined as a sudden onset neurological deficit lasting more than 24 h.
Diabetic retinopathy was diagnosed by fundoscopy. Diabetic neuropathy (DN) was diagnosed based on the vibration perception threshold (Neurothesiometer NU-1, Horwell, UK) of the great toe being >25 V.
Study outcomes
Statistical analyses
A pilot study of 270 diabetes patients was previously undertaken in this population based on previous literature 9 that suggested that 460 total patients, of whom 40% had retinopathy, would be required at α = 0.05 to detect a standard deviation difference of 0.27 in mean vitamin D levels with 80% power, considered a small to moderate-sized effect.
Data trends were visually and statistically evaluated for normality. Non-parametric tests (Mann–Whitney U) were applied to data that violated the assumptions of normality when tested using the Kolmogorov–Smirnov test. Bonferroni correction was applied to account for multiple testing. Statistical analysis was performed using SPSS for Windows, version 24.0. All values are given as mean ± SD or as mean with 95% confidence interval (CI) unless specified. Correlations between vitamin D and its metabolites were undertaken with Spearman’s correlation.
Results
Baseline characteristics
Diabetes patients were older than controls (median age (range) 55.2 (9.9) and 46.1 (10.8) years, respectively, p < 0.001)) and diabetes patients had a greater body mass index (BMI) than controls (median age (range) 32.4 (44) and 30.1 (34.8) years, respectively, p < 0.001)), and concentrations of 25(OH)D3, 1,25(OH)2D3, 24,25(OH)2D3 were significantly different to controls (p < 0.001), though 3epi25(OH)D3 did not differ (p < 0.071) (Table 1). The diabetes complications for the T2DM cohort are shown in Table 2.
The relationship of vitamin D

1,25(OH)2D3, 1,25-dihydroxyvitamin D3; 25(OH)D3, 25-hydroxyvitamin D3; 24,25(OH)2D3, 24,25-dihydroxyvitamin D3; CAD, coronary artery disease; IQR, interquartile range; PAD, peripheral arterial disease.
Vitamin D metabolite measurements
Vitamin D3 concentrations are lower in T2DM
Concentrations of 25(OH)D3, and its active form 1,25(OH)2D3, and its metabolite 24,25(OH)2D3 were lower in the T2DM patients (median (ng/dl) 6.45, 0.02 and 0.29, respectively) compared with nondiabetic controls (median (ng/dl) 8.82, 0.04 and 0.38, respectively: p < 0.001), but 3epi25(OH)D3 did not differ (p = 0.07) (Table 1).
Gender differences in vitamin D3 concentrations
In T2DM, concentrations of 25(OH)D3, 1,25(OH)2D3, 24,25(OH)2D3 and 3epi25(OH)D3 were all lower in females versus males (p < 0.01) (Table 2).
Concentrations of 25(OH)D3, 1,25(OH)2D3, 24,25(OH)2D3 were also lower in nondiabetic females versus nondiabetic males (p < 0.01) (Table 3). Despite the lower vitamin D parameters in females, there was no difference in diabetes complications between males and females (data not shown).
The relationship of vitamin D3 and its epimers to complications in the group of nondiabetic control participants (n = 290).

1,25(OH)2D3, 1,25-dihydroxyvitamin D3; 25(OH)D3, 25-hydroxyvitamin D3; 24,25(OH)2D3, 24,25-dihydroxyvitamin D3; IQR, interquartile range.
Relationship of vitamin D3 metabolite concentrations with diabetic complications
In this T2DM Qatari cohort, lower concentrations of 1,25(OH)2D3 (p < 0.006) and lower levels of 25(OH)D3 were weakly associated with diabetic retinopathy (p < 0.031), as shown in Table 2.
Spearman’s correlation showed 1,25(OH)2D3 to be negatively correlated to age and diabetes duration (R2 –0.301, p < 0.01; –0.16, p < 0.01, respectively); 25(OH)D3 was negatively correlated to age (R2 –0.08, p < 0.024), with no correlation evident for 24,25(OH)2D3 or 3epi25(OH)D3.
There was no difference in the frequency of diabetic complications between males and females.
Relationship of vitamin D3 metabolite concentrations with cardiovascular complications
In this T2DM Qatari cohort, lower concentrations of 1,25(OH)2D3 were associated with hypertension (p < 0.009), dyslipidemia (p < 0.003) and coronary heart disease (p < 0.01). Lower levels of 25(OH)D3 were weakly associated with dyslipidemia (p < 0.041) and low concentrations of 24,25(OH)2D3 were associated with dyslipidemia (p < 0.02), as shown in Table 2.
Relationship of vitamin D3 metabolite concentrations in nondiabetic participants
In nondiabetic participants, concentrations of 25(OH)D3, 1,25(OH)2D3 and 24,25(OH)2D3, but not 3epi25(OH)D3, were lower in females versus males (p < 0.01) (Table 3).
Lower concentrations of 1,25(OH)2D3 were associated with hypertension (p < 0.001) and dyslipidemia (p < 0.001). Lower levels of 25(OH)D3 were associated with dyslipidemia (p < 0.001), as were low concentrations of 24,25(OH)2D3, as shown in Table 3.
eGFR and vitamin D3 concentrations
We considered the possibility that 25(OH)D3 metabolite concentrations were merely reflecting the eGFR in these patients. However, the lack of correlation between eGFR and 1,25-dihydroxyvitamin D (1,25(OH)2D3), 25-hydroxyvitamin D
Correlation of eGFR with levels of vitamin D and its epimers in patients with diabetes.

eGFR, estimated glomerular filtration rate; 1,25(OH)2D3, 1,25-dihydroxyvitamin D3; 25(OH)D3, 25-hydroxyvitamin D3; 24,25(OH)2D3, 24,25-dihydroxyvitamin D3.
Discussion
This study was specifically powered on retinopathy, and both 25(OH)D3 and the active form 1,25(OH)2D3 were highly associated with diabetic retinopathy. The association of vitamin D with diabetes complications is controversial and unclear, with some studies suggesting that it is associated with microvascular complications9,10 and others that it is not. 23 An association specifically with diabetic retinopathy was reported,9,24 and low concentrations of vitamin D have been associated with development of microvascular complications in T2DM, 25 which is in accord with the results reported here, and may, in fact, be predictive of diabetic complication risks. 26 This discrepancy between studies may be due to measuring total vitamin D rather than the D3 form specifically, and perhaps contributed to by having less precise measurement of vitamin D levels than the gold standard measurement employed here. Of note, vitamin D deficiency is not related to seasonal variability in the Middle East, likely due to the population remaining covered throughout the year. 27
Only low 3epi25(OH)D3 levels were found with DN and otherwise 3epi25(OH)D3 did not relate to any other complication. Little is known about the epimers of vitamin D, and the assumption has been that they are biologically less potent.28,29 It is therefore unclear if this is a random chance observation or of specific significance that needs further clarification on the role of vitamin D epimers in disease, and specifically in diabetes.
The metabolite 24,25(OH)2D3 was highly associated with dyslipidemia, and may just reflect 25(OH)D3 concentrations that were also highly associated with dyslipidemia; however, 24,25(OH)2D3 may not be an inactive metabolite, as it has been shown to induce non-genomic signaling pathways and to suppress Apo A-1 in Hep G cells, 30 and it may have a physiological role in growth plate formation; 11 therefore, a direct effect on lipid metabolism cannot be excluded.
Hypertension specifically was associated with lower 1,25(OH)2D
Dyslipidemia was significantly associated with lower 25(OH)2D
Lower 1,25(OH)2D3 levels were found with CAD, though this was not seen for 25(OH)D3, 24,25(OH)2D3 or 3epi25(OH)D3. Vitamin D has been associated epidemiologically with CAD, though a systematic review concluded that there was no effect on vascular function. 33 This study was not powered for this outcome and, therefore, future studies are needed to determine if this is a true association, although vitamin D3 supplements seem to be of limited therapeutic impact. 33 It is of note that no vitamin D3 metabolite was associated with either PAD or stroke; however, vitamin D has been associated with increased risk of PAD 34 and stroke in some studies. 35
The lower 25(OH)D3 concentrations in the Qatari T2DM females versus males are also in accord with other studies, 36 though this is not a universal finding. 9 However, despite the lower vitamin D levels in women, they did not have a higher rate of diabetes.
The strength of this study was the number of participants, all of whom were vitamin D3 supplement naive, and the use of state-of-the-art measurement of vitamin D3 metabolites in this homogeneous population. However, this was a cross-sectional observational study that could not address the underlying causality or mechanisms, and interventional vitamin D3 studies are needed. All of the participants were Qatari, but the controls without T2DM were recruited from the relatives that accompanied the patients to clinic, which may have resulted in a source of bias. Vitamin D deficiency is not related to seasonal variability in the Middle East, likely due to the population remaining covered throughout the year, 27 and therefore would not have been a confounder.
Conclusion
These data showed that both 25(OH)D3 and the active form 1,25(OH)2D3 were highly associated with diabetic retinopathy for which the study was powered, but in addition a relationship between 1,25(OH)2D3 concentrations and hypertension and CAD was found: 25(OH)D3 and 24,25(OH)2D3 levels were associated with dyslipidemia, giving further support to the evidence that vitamin D metabolites may have a role in the development of diabetes as well as cardiovascular complications.
Supplemental Material
R1_Supp_Table_1_Vit_D_Metabolites – Supplemental material for Association of vitamin D3 and its metabolites in patients with and without type 2 diabetes and their relationship to diabetes complications
Supplemental material, R1_Supp_Table_1_Vit_D_Metabolites for Association of vitamin D3 and its metabolites in patients with and without type 2 diabetes and their relationship to diabetes complications by Alexandra E. Butler, Soha R. Dargham, Aishah Latif, Haira R. Mokhtar, Amal Robay, Omar M. Chidiac, Amin Jayyousi, Jassim Al Suwaidi, Ronald G. Crystal, Charbel Abi Khalil and Stephen L. Atkin in Therapeutic Advances in Chronic Disease
Footnotes
Author contributions
AEB researched the data and wrote the manuscript. SRD performed the statistical analysis. AL and HRM performed the vitamin D measurements. AR, OMC, AJ and JAS researched the data. RGC, SLA and CAK designed the study and contributed to the discussion. SLA is the guarantor of this work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Dr. Abi Khalil’s lab is funded by the Qatar National Research Fund (QNRF), NPRP Grant 9-169-3-024. The funding source did not have a role in the design of the study, decision to publish or writing of the manuscript.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Ethical approval
The study was approved by Weill Cornell IRB (IRB# 13-00063) and all participants provided written informed consent. The conduct of the trial was in accordance with ICH GCP and the Declaration of Helsinki.
Consent to publish
All authors agree to publish this work.
Availability of data and materials
All data are available upon reasonable request by contacting the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.