
Abstract
Background:
Acute esophagogastric variceal bleeding (AEGVB) is a common complication of liver cirrhosis and hepatocellular carcinoma (HCC). It is unclear if older patients with cirrhotic HCC benefit from endoscopic treatment as secondary prophylaxis for AEGVB in short term.
Objectives:
We aim to investigate if endoscopic treatment as secondary prophylaxis for AEGVB reduces short-term mortality in older patients with cirrhotic HCC.
Design:
We retrospectively enrolled 138 consecutive patients over 60 years old with cirrhotic HCC and AEGVB from April 1, 2021 through December 31, 2022 in Emergency Room, Beijing You’an Hospital, Capital Medical University.
Methods:
A 1:1 propensity score matching (PSM) analysis was performed to adjust for confounding factors such as age, gender, Child-Pugh score in our statistical findings. Logistic regression and Cox regression analyses were used to investigate whether there was a significant negative association between endoscopic treatment and short-term mortality for AEGVB in older patients with cirrhotic HCC. Kaplan–Meier methodology was employed to compare overall survival over 6 weeks between the endoscopic treatment group and non-endoscopic treatment group.
Results:
In older patients with cirrhotic HCC and AEGVB, in-hospital mortality and 6-week mortality were significantly lower in the endoscopic treatment group compared to the non-endoscopic treatment group before PSM (5.33% vs 26.98%, p = 0.001 for in-hospital mortality; 12.00% vs 44.44%; p < 0.001 for 6-week mortality). These results remained consistent after PSM (4.76% vs 26.98%, p = 0.002 for in-hospital mortality; 9.52% vs 44.44%; p < 0.001 for 6-week mortality). Both logistic regression and Cox regression analyses found that endoscopic treatment contributed to reduced short-term mortality for AEGVB in older patients with cirrhotic HCC. Kaplan–Meier survival curves indicated that older patients undergoing endoscopic treatment had a higher short-term survival rate than those who didn’t receive endoscopic treatment in our cohort. However, there was no significant difference in short-term survival between patients receiving endoscopic variceal ligation and those treated with endoscopic injection sclerotherapy.
Conclusion:
Secondary prophylaxis of endoscopic treatment helps to reduce 6-week mortality for AEGVB in older patients with cirrhotic HCC. Therefore, endoscopic treatment is suggested to be employed as secondary prophylaxis in this special population in clinical practice.
Keywords
Background
Acute esophagogastric variceal bleeding (AEGVB) is a severe complication of liver cirrhosis, with a 6-week mortality rate reaching 20%, even with huge advancements in management strategies. 1 The standard care for AEGVB includes a combination of vasoactive drugs, prophylactic antibiotics, proton pump inhibitor, and endoscopic treatment. Among these treatments, endoscopic treatment is the first-line strategy for both primary and secondary prophylaxis of AEGVB. 2 In a prospective study with 276 cirrhotic patients who presented with AEGVB and managed with endoscopic variceal ligation (EVL), they found that age >65 years and coexistence of hepatocellular carcinoma (HCC) were two of the independent factors associated with 3-year mortality. 3 Since older patients with AEGVB have lower tolerance to hemodynamic changes and more co-morbidities, 4 their morbidity and mortality are higher than those in younger ones. 5 A study involving 61 older patients with variceal bleeding demonstrated that those treated with active endoscopic injection sclerotherapy (EIS) within 12 h had outcomes similar to those of younger patients nearly 35 years earlier. 6 Therefore, it’s urgent to clarify whether endoscopic treatment can improve survival outcomes in older patients.
HCC ranks the sixth among the most common cancers and the third leading cause of cancer-related death worldwide. 7 The majority of HCC cases originates from liver cirrhosis. 8 More than 50% of patients with HCC have esophageal varices and about 50% of these patients undergo AEGVB, which are associated with poorer survival outcomes. 9 AEGVB patients with HCC have higher 5-day treatment failure and 6-week mortality rates compared with those without HCC. 10 Furthermore, HCC predicts and elevated risk of in-hospital mortality from AEGVB in patients with liver cirrhosis. 11 A Taiwanese study nearly 30 years ago revealed that EIS decreased short-term mortality due to esophageal variceal bleeding in cirrhotic HCC patients, whereas the long-term survival benefits of EIS were not observed because the survivors subsequently experienced complications such as hepatic failure and tumor growth. The mean survival times for the cohort were <3 months. 12 Nowadays, the overall survival rates have been significantly improved with the discovery of early-stage HCC, the advent of immunotherapy, and new tyrosine kinase inhibitors for HCC patients with reduced bleeding risk. 13 Thus, eradication of varices in cirrhotic HCC patients should contribute to their long-term survival theoretically. Currently, there is a significant lack of data on the benefits of endoscopic treatment for older cirrhotic HCC patients with AEGVB. Therefore, it is of great interest to clarify the clinical features, prognosis, and especially the importance of endoscopic treatment for short-term mortality in older patients with HCC and AEGVB, which may help to improve the survival rate of older patients.
In this study, we aim to investigate the clinical characteristics and prognosis of older cirrhotic HCC patients with AEGVB and clarify whether endoscopic treatment will contribute to reduced short-time mortality in a Chinese retrospective cohort.
Methods
Study cohort
Patient information in this retrospective single-center study was derived from a previous cohort that included patients over 18 years old with acute gastrointestinal bleeding (AGIB) admitted to the Emergency Room (ER), Beijing You’an Hospital, Capital Medical University from April 1, 2021 to December 31, 2022. Only the first admission was included for patients who had multiple admissions due to AGIB during the previous study period. Only patients with liver cirrhosis were included for data analysis. In this study, we excluded patients in the cirrhotic AGIB cohort who: (i) were lost to follow-up; (ii) were discharged against medical advice in ER; (iii) did not undergo endoscopy within 6 months prior to admission and refused it after admission; (iv) had non-variceal bleeding; (v) were younger than 60 years old; (vi) did not have HCC. Finally, 138 patients were enrolled in the present study and then followed up for 6 weeks. All-cause death was recorded. The primary endpoint was 6-week mortality. The second endpoints were in-hospital mortality and 6-week rebleeding.
Clinical, laboratory, and radiological parameters
HCC was diagnosed on the basis of historical data, pathology, or imaging studies such as computed tomography and/or magnetic resonance imaging. 14 HCC staging was performed using the Barcelona Clinic Liver Cancer (BCLC) classification. 15 Liver cirrhosis was diagnosed with medical history, physical examination, laboratory tests, imaging studies, and liver biopsy. AEGVB is defined as clinical signs of bleeding (hematemesis, melena, or hematochezia) originating from the gastrointestinal tract. This condition must be confirmed by endoscopy, which should reveal esophagogastric varices within 6 months. We recorded the following items: shock index, etiology of cirrhosis, underlying diseases, grades of ascites, stages of hepatic encephalopathy, Child-Pugh class, in-hospital death, 6-week death, 6-week rebleeding, endoscopy, endoscopic treatment, and HCC-related contents. The following laboratory parameters were included: hemoglobin (Hb), platelet (PLT), alanine aminotransferase (ALT), aspartate aminotransferase (AST), creatinine, total bilirubin (TB), albumin, prothrombin time (PT), blood urea nitrogen (BUN), creatinine kinase-MB (CK-MB), Troponin I (TnI), and myoglobin. Child-Pugh classes were estimated based on the degree of hepatic encephalopathy, ascites, TB, albumin, and PT. Grade of ascites and stages of hepatic encephalopathy were diagnosed according to the criteria by the Chinese Society of Hepatology, Chinese Medical Association. 16
Treatment received
All enrolled patients received treatments including antibiotics, vasoactive drugs (Octreotide or Terlipressin), and proton pump inhibitor. Some patients received various treatments based on their conditions, including the Sengstaken–Blakemore tube and/or endoscopic treatments such as EVL, gastric variceal ligation, EIS, or tissue adhesive injection for gastric varices.
Ethics
This study was approved by the Clinical Research Ethics Committee of Beijing You’an Hospital, Capital Medical University following the declaration of Helsinki (Number LL-2023-143-K). The clinical data used in this study were anonymized to protect patient confidentiality. The need for consent was waived by the ethics committee for the retrospective nature of the study. This study was conducted and reported in accordance with the STROBE statement. 17
Statistical analysis
Quantitative variables were presented as medians with interquartile range and group differences were assessed using the Student’s t test. Qualitative variables were reported as frequency and percentage, and the Chi-square test was used to perform the difference comparison. If the variables did not meet normal conditions, non-parametric tests would be performed. Cumulative survival rates were estimated by the Kaplan–Meier method. Univariable and multivariable Cox regression analyses were performed to identify prognostic factors associated with overall survival. Propensity score matching (PSM) analysis in a 1:1 ratio was employed to reduce the confounding effect of factors affecting prognostic survival including age, gender, Child-Pugh class, Hb, PLT, APTT, hypertension, DM, coronary heart disease, smoking history, drinking history, and chronic kidney disease. p-Value of <0.05 was deemed statistically significant. All statistical analyses were performed with R software version 4.2.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Clinical characteristics of older cirrhotic HCC patients with AEGVB
We collected electronic records of 2071 episodes of AGIB in ER. Based on the including/excluding criteria, we finally enrolled 138 older cirrhotic HCC patients with AEGVB who were followed up for 6 weeks (Figure 1). The rates of in-hospital mortality and 6-week mortality in the whole cohort were 15.22% and 26.81%, respectively. Additionally, 15.95% of the cohort experienced a recurrence of gastrointestinal bleeding.

Schematic diagram of patient selection procedure.
To minimize the confounding effects of factors influencing prognostic survival such as age, gender, Child-Pugh class, and medical history, we conducted PSM analysis at a 1:1 ratio. This process resulted in 63 matched patients in each group. The baseline clinical characteristics of patients before and after PSM are summarized in Table 1. Patients who did not receive endoscopic treatment exhibited higher levels of TB, creatinine, ALT, and AST compared to those who did. Nevertheless, no significant differences were observed between the two groups in terms of demographics, etiology of liver cirrhosis, Child-Pugh class, comorbidities, HCC-related markers, and anti-tumor treatments.
Clinical characteristics of AEGVB in older patients with liver cirrhosis and HCC before and after PSM.
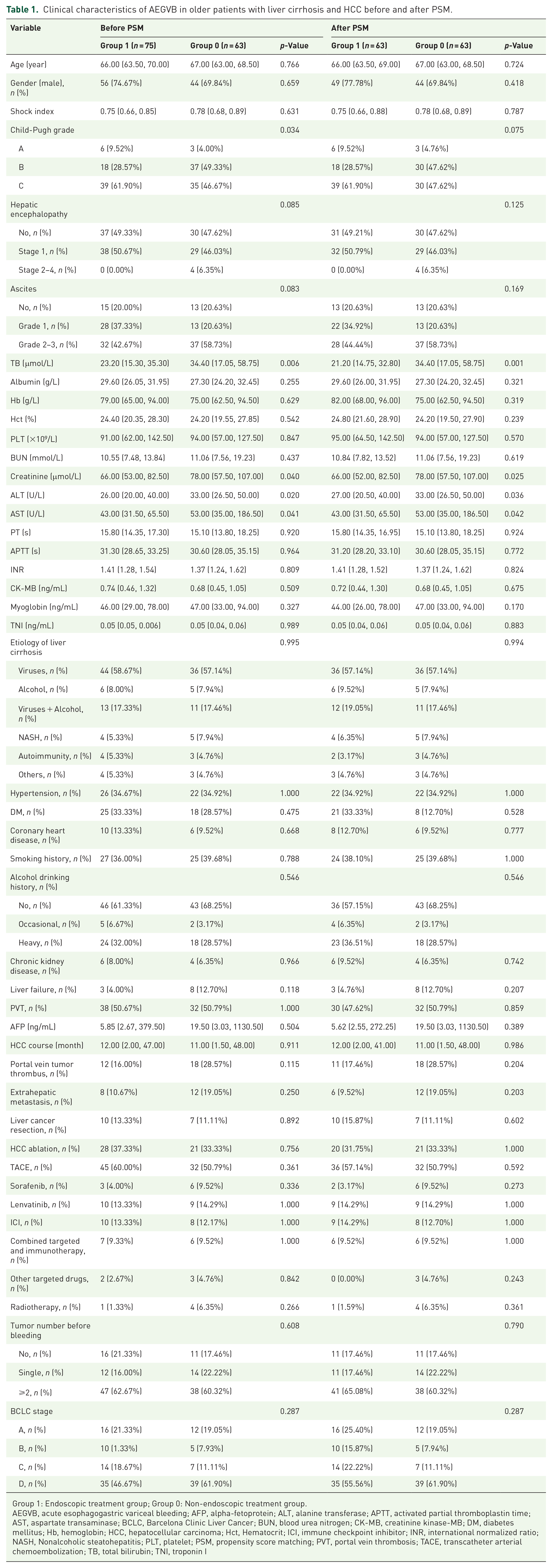
Group 1: Endoscopic treatment group; Group 0: Non-endoscopic treatment group.
AEGVB, acute esophagogastric variceal bleeding; AFP, alpha-fetoprotein; ALT, alanine transferase; APTT, activated partial thromboplastin time; AST, aspartate transaminase; BCLC, Barcelona Clinic Liver Cancer; BUN, blood urea nitrogen; CK-MB, creatinine kinase-MB; DM, diabetes mellitus; Hb, hemoglobin; HCC, hepatocellular carcinoma; Hct, Hematocrit; ICI, immune checkpoint inhibitor; INR, international normalized ratio; NASH, Nonalcoholic steatohepatitis; PLT, platelet; PSM, propensity score matching; PVT, portal vein thrombosis; TACE, transcatheter arterial chemoembolization; TB, total bilirubin; TNI, troponin I
Endoscopic treatment and prognosis in older cirrhotic HCC patients with AEGVB
In the non-endoscopic treatment group, 58.73% of the patients underwent endoscopy after being admitted. Regarding endoscopy, there were no significant differences in esophageal varices degree, gastric varices, red sign, and portal hypertension gastropathy between the two groups. Although a higher proportion of patients in the endoscopic treatment group received Sengstaken–Blakemore tube, there was no significant difference between the two groups. In the endoscopic treatment group, 73.44% of the patients underwent EIS which ranked the first and only 21.33% received EVL. The rates of in-hospital mortality and 6-week mortality in the endoscopic treatment were 5.33% and 12.00%, respectively, significantly lower than those in the non-endoscopic treatment group (26.98% and 44.44%, p < 0.001). Older patients in the endoscopic treatment group experienced a lower incidence of rebleeding compared to those in the non-endoscopic treatment group. However, this difference was not statistically significant (13.33% vs 19.05%, p = 0.497; Table 2).
Endoscopy, treatment, and short-term prognosis of AEGVB in older patients with liver cirrhosis and HCC before and after PSM.

Group 1: Endoscopic treatment group; Group 0: Non-endoscopic treatment group.
AEGVB, acute esophagogastric variceal bleeding; EIS, endoscopic injection sclerotherapy; EVL, endoscopic variceal ligation; GOV, gastroesophageal varices; HCC, hepatocellular carcinoma; ICU, intensive care unit; IGV, isolated gastric varices; PSM, propensity score matching.
During 6 weeks after admission, 28 (44.44%) patients died in the non-endoscopic treatment group. Among them, 16 (57.14%) died from AEGVB at admission or rebleeding and 12 (42.86%) from non-AEGVB such as HCC and other complications of end-stage liver cirrhosis. However, only nine (12.00%) patients died in the endoscopic treatment group, among which four (44.44%) died from bleeding and five (55.56%) from non-bleeding causes (Figure 2). Then we further analyzed whether there was a significant difference in bleeding-related 6-week mortality. We found that the proportion of deaths within 6 weeks due to bleeding was significantly higher in the non-endoscopic treatment group (23.81%) compared to the endoscopic treatment group (4.76%; p = 0.002).

Causes of death in older cirrhotic HCC patients between non-endoscopic treatment group and endoscopic treatment group.
Influence of liver disease severity on 6-week mortality in older cirrhotic HCC patients with AEGVB
Given that liver disease severity affects patient prognosis, we examined whether endoscopic treatment reduced 6-week mortality in patients with varying degree of liver disease severity. Out of 57 patients in Child A/B, 24 (42.1%) received non-endoscopic treatment, while 33 (57.9%) underwent endoscopic treatment. Only four patients (7.02%) died within 6 weeks from bleeding, with two (8.33%) in the non-endoscopic treatment group and two (6.06%) in the endoscopic treatment group (p = 1.000). A total of six participants (10.53%) experienced all-cause death within 6 weeks, with four (16.67%) from the non-endoscopic treatment group and two (6.06%) from the endoscopic treatment group (p = 0.395). There were no statistically significant differences between two groups for either outcome although 6-week mortality due to bleeding or all cause seemed higher in non-endoscopic treatment group than that in endoscopic treatment group. However, the results differed significantly for patients in Child C. Among 69 patients in Child C, 39 (56.52%) were in non-endoscopic treatment group and 30 (43.48%) in endoscopic treatment group. 6-Week death due to bleeding occurred in 14 cases (20.29%), with non-endoscopic treatment group showing a higher proportion (33.33% vs 3.33%; p = 0.002). All-cause death within 6 weeks occurred in 28 cases (40.58%), with non-endoscopic treatment group having a higher proportion (61.54% vs 13.33%; p < 0.001).
Univariable and multivariable logistic regression analysis for 6-week mortality in older cirrhotic HCC patients with AEGVB
We analyzed predictors of 6-week mortality in older cirrhotic HCC patients with AEGVB through univariable analysis. Variables with a significance level of p < 0.05 (Table 3) were selected for further multivariable regression analysis. We found that endoscopic treatment (odds ratio (OR), 0.031; 95% confidence interval (CI), 0.020–0.232; p = 0.003), Child-Pugh score (OR, 2.467; 95% CI, 1.328–5.789; p = 0.013), albumin (OR, 0.785; 95% CI, 0.608–0.971; p = 0.036), PLT (OR, 1.053; 95% CI, 1.025–1.096; p = 0.002), PT (OR, 0.575; 95% CI, 0.350–0.810; p = 0.007), APTT (OR, 1.742; 95% CI, 1.270–2.726; p = 0.003), and tumor number before bleeding (OR, 21.954; 95% CI, 3.829–272.523; p = 0.003) were significantly associated with 6-week mortality in this patient group. Among them, endoscopic treatment is crucial for reducing 6-week mortality.
Univariable and multivariable logistic regression analysis for 6-week mortality of AEGVB in older patients with liver cirrhosis and HCC.

AEGVB, acute esophagogastric variceal bleeding; AFP, alpha-fetoprotein; ALT, alanine transferase; APTT, activated partial thromboplastin time; AST, aspartate transaminase; BCLC, Barcelona Clinic Liver Cancer; BUN, blood urea nitrogen; CK-MB, creatinine kinase-MB; DM, diabetes mellitus; EIS, endoscopic injection sclerotherapy; HCC, hepatocellular carcinoma; ICU, intensive care unit; OR, odds ratio; PLT, platelet; TB, total bilirubin; TNI, Troponin I.
Cox regression analysis for short-term survival in older cirrhotic HCC patients with AEGVB
Table 4 presents the results of the univariate and multivariate Cox regression analysis. The 6-week mortality was significantly associated with several factors: endoscopic treatment (hazard ratio (HR), 0.104; 95% CI, 0.029–0.367; p < 0.001), Child-Pugh score (HR, 1.797; 95% CI, 1.281–2.520; p = 0.001), TB (HR, 1.005; 95% CI, 1.001–1.010; p = 0.018), PLT (HR, 1.015; 95% CI, 1.006–1.024; p = 0.007), creatinine (HR, 1.013; 95% CI, 1.003–1.022; p = 0.007), APTT (HR, 1.126; 95% CI, 1.063–1.192; p < 0.001), CK-MB (HR, 0.796; 95% CI, 0.664–0.955; p = 0.014), and tumor number before bleeding (HR, 4.202; 95% CI, 1.298–13.606; p = 0.017).
Univariable and stepwise multivariable COX regression analysis for 6-week mortality of AEGVB in older patients with liver cirrhosis and HCC.

AEGVB, acute esophagogastric variceal bleeding; AFP, alpha-fetoprotein; ALT, alanine transferase; APTT, activated partial thromboplastin time; AST, aspartate transaminase; BCLC, Barcelona Clinic Liver Cancer; BUN, blood urea nitrogen; CI, confidence interval; CK-MB, creatinine kinase-MB; DM, diabetes mellitus; Hb, hemoglobin; HCC, hepatocellular carcinoma; Hct, Hematocrit; HR, hazard ratio; ICU, intensive care unit; ICI, immune checkpoint inhibitor; INR, international normalized ratio; NASH, Nonalcoholic steatohepatitis; PLT, platelet; PT, prothrombin time; PVT, portal vein thrombosis; TACE, transcatheter arterial chemoembolization; TB, total bilirubin; TNI, Troponin I.
Kaplan–Meier analysis showed that 6-week mortality rate was significantly higher in the non-endoscopic treatment group compared to the endoscopic treatment group (long-rank test, p < 0.0001; Figure 3).

Overall survival in non-endoscopic treatment group versus endoscopic treatment group in older cirrhotic HCC.
We also analyzed the survival rate difference between patients treated with EVL and those treated with EIS. Six patients who were only treated with tissue adhesive injection for gastric varices but neither with EVL nor EIS and two patients with both EVL and EIS were excluded. Ultimately, we included 14 patients treated with EVL and 53 patients with EIS in our analysis. We found there was no significant difference in survival rate between these two patient groups (long-rank test, p = 0.21; Figure 4).

Overall survival in EVL group versus EIS group in older cirrhotic HCC patients with AEGVB without PSM.
Discussion
Several studies suggest that combining ligation with cyanoacrylate may be preferred as secondary prophylaxis for HCC patients with esophageal and gastric varices. 18 To the best of our knowledge, for older cirrhotic HCC patients with AEGVB, this is the first retrospective cohort study that examines the relationship between second prophylaxis of endoscopic treatment and reduced short-term mortality. The in-hospital mortality rate was 15.22%, while the 6-week mortality rate for the entire cohort was 26.81%. However, endoscopic treatment as second prophylaxis significantly lowers in-hospital mortality to 5.33% and 6-week mortality to 12.00%, both of which are markedly lower than the rates in patients who did not receive endoscopic treatment.
The in-hospital mortality rate for HCC patients with AEGVB can reach 54.3% if they had a model for end-stage liver disease (MELD) score >12.9, higher-grade esophageal varices, active bleeding during the initial endoscopy, an increased need for blood transfusion, prolonged hospital stays, and decompensated liver disease with significant comorbidities. 19 In our cohort, the in-hospital mortality rate for AEGVB among older cirrhotic HCC patients was 15.22%, lower than the previously reported rate of 20.5%. 20 Moreover, endoscopic treatment can lower the in-hospital mortality rate to as low as 5.33%, suggesting that it is an effective as second prophylaxis for short-term survival in older cirrhotic HCC patients with AEGVB. Notably, our analysis showed that endoscopic treatment was considerably associated with 6-week mortality in older cirrhotic HCC patients with AEGVB, as indicated by both logistic regression and Cox regression analyses.
In this study, there were 69 (54.76%) patients in Child C after PSM. We found that for patients in Child A/B endoscopic treatment didn’t significantly influence both all-cause and bleeding-related 6-week mortality. However, for patients in Child C, both 6-week mortality due to bleeding and all-cause mortality were much higher in non-endoscopic treatment group than those in endoscopic treatment group. These results indicate that endoscopic treatment ameliorates 6-week mortality especially for patients in Child C. Therefore, older cirrhotic patients with HCC in Child A/B may suffice with hemostasis using vasoactive drugs in the short term. In contrast, those in Child C likely require additional treatment beyond vasoactive drugs to achieve effective hemostasis. It will be important to perform endoscopic treatment in this special subgroup, which should help to reduce at least their short-term mortality. Kawai et al. found that HCC patients in Child A/B had better overall survival than those in Child C who received emergency EVL following variceal rupture. 21 Our results also demonstrated that even though endoscopic treatment could reduce 6-week mortality in older HCC patients with AEGVB, 6-week mortality was higher in Child C patients compared to Child A/B patients.
In Western countries, EVL is widely recommended as a standard endoscopic treatment for the secondary prevention of esophageal variceal bleeding. 2 In contrast, most Chinese endoscopists prefer endoscopic intervention within 1 week after hemostasis of AEGVB using EVL, EIS, and tissue adhesive injection as the main strategies for secondary prophylaxis. 22 The guidelines in Japan, another Asian country, recommend that both EVL and EIS can be used to treat esophageal varices. 23 A recent study showed that both EIS and EVL were applicable to emergency endoscopic treatment for AEGVB. 24 Prophylactic EIS can reduce bleeding and enhance survival rates in certain patients with HCC and varices.25–27 Nearly 35 years ago, Hosking et al. 6 pointed out that early endoscopy and EIS were essential treatments in older patients with AEGVB in order to obtain optimum results. In our retrospective study, both EVL and EIS were used for secondary prophylaxis in older cirrhotic HCC patients with AEGVB. Sixteen patients (21.33%) from the endoscopic therapy group underwent EVL and 55 (73.33%) received EIS. Previous studies have compared the effects of EIS with EVL.28,29 EIS has been demonstrated a lower recurrence rate of EGV than EVL because EIS has the potential to occlude the blood flow to esophageal varices by the injection of a sclerosing agent. What’s more, a Japanese team reported that EIS even could improve liver functions and prognosis in patients with Child-Pugh grade A/B, but EVL didn’t have such an impact. 30 However, our results indicated no significant difference in survival rates between patients treated with EVL and EIS, likely due to the small size of our cohort. Further prospective trials with a larger case number are needed to clarify the differences between EVL and EIS in older cirrhotic HCC with AEGVB.
Several studies indicate that using endoscopic treatment for primary prevention enhances the prognosis of patients with HCC and EGV. Primary prevention of AEGVB was associated with a lower mortality rate in patients with HCC. 31 Recently, a randomized controlled trial found that EVL is more effective than Propranolol in preventing AEGVB among patients with HCC and medium-to-large EVs. Furthermore, EVL not only reduced the risk of AEGVB but also improved overall survival in patients with BCLC stage A/B HCC. 32 Our study focused on older cirrhotic HCC patients with AEGVB, a distinct demographic, and we demonstrated that secondary prevention can enhance their short-term prognosis. Nevertheless, it remains uncertain whether secondary prevention positively affects the long-term prognosis of this group.
To date, this study represents the inaugural investigation into the potential of endoscopic treatment as a secondary prophylaxis for AEGVB in older cirrhotic HCC patients. Our findings indicate that secondary prophylaxis of endoscopic treatment is an effective strategy for reducing short-term mortality in this special population. However, it is crucial to acknowledge that the study’s limitations stem from its single-center, retrospective design, which may affect the generalizability of our findings. Secondly, our data were obtained from a specialized tertiary hospital for liver diseases affiliated with a medical university, which may be unable to represent scenarios in general hospitals. Thirdly, the number of cases was relatively limited, therefore, we did not perform the calculation and justification of the sample size selected for this study, which may cause a degree of selection bias and influence the statistical outcomes. Finally, only short-term mortality was investigated in the current study. It’s still unclear whether second prophylaxis of endoscopic treatment helps to prolong survival of older cirrhotic HCC patients with AEGVB in a long period. Therefore, larger prospective trials with long-term prognosis in this special population are warranted in future.
Conclusion
We herein characterized AEGVB occurring in older cirrhotic HCC patients, showing that short-term mortality rate was notably lower in the endoscopic treatment group than that in the non-endoscopic treatment group. We recommend that endoscopic treatment is employed as a secondary prophylaxis and for the eradication of EGV in old HCC patients. However, due to the limited number of cases included in this study and its retrospective design, further prospective trials with larger sample sizes are needed.
Supplemental Material
sj-doc-1-taj-10.1177_20406223251356824 – Supplemental material for Endoscopic treatment as secondary prophylaxis ameliorates short-term mortality for acute esophagogastric variceal bleeding in older patients with cirrhotic hepatocellular carcinoma
Supplemental material, sj-doc-1-taj-10.1177_20406223251356824 for Endoscopic treatment as secondary prophylaxis ameliorates short-term mortality for acute esophagogastric variceal bleeding in older patients with cirrhotic hepatocellular carcinoma by Qi Li, Ruifeng Liu, Shenghui Zhou, Lingna Lyu, Chunlei Fan and Huiguo Ding in Therapeutic Advances in Chronic Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.