
Abstract
Background:
Diabetic kidney disease (DKD) is a severe complication of diabetes mellitus and is associated with an increased risk of end-stage renal disease (ESRD) and cardiovascular events. Early diagnosis and monitoring of DKD are crucial for implementing appropriate interventions. This study aimed to investigate the relationship between serum renalase (RNLS) levels, DKD, and diabetic macroangiopathy in patients with type 2 diabetes mellitus (T2DM).
Objectives:
This study aims to evaluate the diagnostic value of serum renalase levels in DKD and diabetic macroangiopathy.
Design:
This is a retrospective case–control study.
Methods:
A total of 233 participants were recruited for the study, including 115 T2DM patients without DKD or diabetic retinopathy, and 118 T2DM patients with DKD. Serum RNLS levels were measured using an enzyme-linked immunosorbent assay. Kidney function parameters and diabetic macroangiopathy risk factors were evaluated in relation to serum RNLS levels.
Results:
Serum RNLS levels were significantly higher in DKD patients compared to T2DM controls (34.82 (31.68, 39.37) vs 30.52 (28.58, 33.16), p < 0.01). Multiple linear regression analysis indicated that kidney function parameters and carotid intima-media thickness were independently related to RNLS levels. The study population was divided into four groups: no DKD and no diabetic macroangiopathy, DKD without diabetic macroangiopathy, diabetic macroangiopathy without DKD, and both DKD and diabetic macroangiopathy. Analysis results showed that patients with both DKD and diabetic macroangiopathy had the highest RNLS levels. Receiver operating characteristic curve analysis demonstrated the diagnostic value of RNLS for DKD (0.76 (95% confidence interval (CI) = 0.70–0.82, p < 0.01)) and diabetic macroangiopathy (0.75 (95% CI = 0.66–0.84, p < 0.01)).
Conclusion:
Circulating RNLS levels were significantly increased in patients with DKD and diabetic macroangiopathy, suggesting that RNLS may serve as an early diagnostic marker.
Introduction
Diabetic kidney disease (DKD) is a major complication of diabetes mellitus and a leading cause of end-stage renal disease (ESRD).1,2 Although DKD is prevalent worldwide, therapeutic options are quite limited. Currently, DKD is mainly managed through a multifaceted approach, including glycemic control, blood pressure management, and the use of renoprotective agents. However, the incidence of DKD continues to exceed clinical capacity.3–7 The kidney function of DKD patients always declines rapidly accompanied by a high risk of cardiovascular and cerebrovascular accident, which is significantly faster than other chronic kidney diseases (CKD).8–10 Thus, early diagnostic markers for monitoring and predicting DKD are essential to enable timely and appropriate protective treatments.11,12
Currently, urinary albumin is the primary marker used for the early diagnosis of DKD in diabetes mellitus patients. However, its sensitivity and specificity are limited, and its contribution to early diagnosis is limited.13–15 It is necessary to develop more sensitive markers for early diagnosis of DKD. Recent studies have focused on exploring biomarkers associated with resistance to DKD, suggesting that individuals with a long duration of diabetes may have an enrichment of protective factors. Identifying these factors could lead to the development of new therapeutic targets for DKD.
Renalase (RNLS) is a flavin adenine dinucleotide-dependent amine oxidase primarily expressed in the kidneys, heart, liver, and skeletal muscle. It plays a key role in the degradation of circulating catecholamines. 16 Recent study shows that RNLS can act as a cytokine and perform cytoprotective properties independent of its enzymatic activity. 17 RNLS protects against acute kidney injury by activating protein kinase B (AKT), extracellular signal-regulated kinase (ERK), mitogen-activated protein kinase (MAPK), and inhibiting c-Jun N-terminal kinase. 18 RNLS also exerts protective effects in the development of DKD through inhibiting mesangial cell hypertrophy. 19 Additionally, genetic association studies have indicated that variants in the RNLS gene are associated with hypertension, coronary artery disease, stroke, type 1 diabetes mellitus, and CKD in humans.19–24 The serum concentration of RNLS is significantly higher in individuals with ESRD and coronary artery disease compared to healthy individuals. However, whether RNLS plays a role in early diabetic kidney injury and can serve as a diagnostic marker in the early stages of DKD and diabetic macroangiopathy remains uncertain.
In this study, we aimed to investigate the serum levels of RNLS in early-stage DKD patients and determine its potential as an early biomarker. We measured RNLS levels in 233 patients with type 2 diabetes mellitus (T2DM), both with and without DKD. Additionally, we assessed T2DM-related kidney function and cardiovascular disease (CVD) risk based on serum RNLS levels.
Methods
Participants and phenotype definition
This retrospective case–control study utilized patient records and existing clinical samples. We recruited 233 patients diagnosed with T2DM based on World Health Organization criteria: fasting plasma glucose ⩾7 mmol/L or 2 h plasma glucose after an oral glucose tolerance test ⩾11.1 mmol/L. Patients with type 1 diabetes mellitus, mitochondrial diabetes, maturity-onset diabetes of the young, and other special types of diabetes mellitus were excluded. Additionally, patients with known cancer, hemolytic disease, pregnancy, alcohol or drug addiction, mental disease, infections, and abnormal liver function were excluded.
Diagnosis of DKD
This study focuses on patients clinically diagnosed with DKD, utilizing key indicators such as estimated glomerular filtration rate (eGFR) and the 24-h urinary albumin excretion rate (uAER). Blood and urine samples were collected for analysis, with blood samples used to measure creatinine levels. The glomerular filtration rate (GFR) was estimated using the Modification of Diet in Renal Disease equation for the Chinese population: 25

For urine collection, patients discarded the first-morning urine around 8:00 a.m. and retained all subsequent urine samples, including daytime, nighttime, and the first-morning urine on the following day. After completing the 24-h urine collection, the total volume was measured using a graduated container, and a well-mixed 10 mL urine sample was taken for analysis within 1 h. During the 24-h urine collection period, patients maintained regular water intake, diet, and activities. Each collection was thoroughly mixed, stored at 2–8°C, and promptly delivered for accurate analysis. DKD was diagnosed as uAER ⩾ 30 mg/24 h or eGFR ⩽ 60 mL/(min × 1.73 m2) in patients with T2DM. Individuals with any history of CKD were excluded.
Diagnosis of diabetic macroangiopathy
Vascular ultrasound was employed for the comprehensive examination of bilateral carotid arteries. The carotid arteries were examined bilaterally at four specific locations: the common carotid arteries, the bifurcation, and the internal and external carotid arteries. Information regarding intima-media thickness (IMT), atherosclerotic plaques, and stenosis was meticulously recorded at each location. An atherosclerotic plaque was defined as a focal protrusion into the arterial lumen measuring 0.5 mm or 50% greater than the surrounding IMT value. Evaluation of significant artery stenosis followed conventional Doppler ultrasound criteria. Diagnoses of carotid atherosclerosis were established in the presence of plaques or significant stenosis. Computed tomography and/or magnetic resonance imaging were utilized to identify evidence of cerebrovascular disease.26,27 Patients with a history of diagnosed macroangiopathy (atherosclerosis, coronary heart disease, myocardial infarction, stroke, ischemic encephalopathy, and intracerebral hemorrhage) were also included.
Clinical measurements
The anthropometric characteristics, such as age, sex, height, body weight, waist circumference, and duration of T2DM, were recorded. Body mass index (BMI) was calculated as weight (kilograms) divided by the square of height (meters). Waist circumference was measured in the horizontal plane midpoint between the iliac crest and the lowest rib while standing. Blood pressure was measured twice by an experienced physician from the right arm after a 5-min sitting break, and the mean value was recorded. Fasting venous blood was collected, and serum samples were isolated and stored at −80°C. Serum creatinine, blood urea nitrogen, uric acid, and other serum concentrations of lipid and liver function indexes were analyzed by a Hitachi 7600-020 automated biochemical analyzer (Hitachi, Tokyo, Japan). Hemoglobin A1c (HbA1c) was evaluated by high-performance liquid chromatography with a Bio-Rad Variant II Hb testing system (Bio-Rad Laboratories, Hercules, CA, USA).
Serum RNLS measurements
Serum RNLS levels were detected by enzyme-linked immunosorbent assay (ELISA) using a human ELISA kit for RNLS (catalog #SEC845Hu; USCN Life Science Inc., Wuhan, China) following the assay procedure.
Statistical analyses
The study was conducted and reported in accordance with the STROBE statement (Supplemental material). 28 Statistical analyses were performed using SAS (version 9.3; SAS Institute, Cary, NC, USA). A sample size of 118 cases and 115 controls provided 80% power to detect a between-group difference in serum RNLS levels. This was determined using a two-sided t test with a significance level of 0.05, as calculated by G*Power 3.1 software (Universitäd Kiel, Germany). Data are presented as the mean ± standard deviation or median with interquartile range according to the normality test. Differences in frequency distribution were analyzed by the Chi-square test. Differences in quantitative results among groups were assessed by the Mann–Whitney U test or Kruskal–Wallis test. The association between serum RNLS levels and clinical characteristics was analyzed using Spearman rank correlation analysis, while multiple linear regressions were conducted to identify relationships, adjusting for confounding factors. A two-tailed significance level was set at p < 0.05.
Results
Clinical characteristics
A total of 115 T2DM patients without DKD and diabetic retinopathy (DR) and 118 T2DM patients with DKD were recruited for this study. The clinical characteristics of the groups, classified by DKD status, are presented in Table 1. There was no difference in sex distribution, age, waist circumference, HbA1c, total cholesterol, low-density lipoprotein cholesterol, and blood urea nitrogen between the DKD and non-DKD groups. However, the DKD group had higher BMI, systolic blood pressure (SBP), diastolic blood pressure (DBP), triglycerides, uric acid, serum creatinine, AER, and carotid IMT compared to the non-DKD group. Meanwhile, the DKD group had a shorter duration of diabetes, lower high-density lipoprotein cholesterol, alanine aminotransferase (ALT), aspartate aminotransferase (AST), and eGFR than the non-DKD group.
Clinical characteristic.

Data are shown as median (interquartile range)
p Values <0.05 are shown in bold.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; DKD, diabetic kidney disease; eGFR, estimated glomerular filtration rate; HbA1c, hemoglobin A1c; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; IMT, intima-media thickness.
Serum RNLS levels in DKD case–control groups
In our study, the serum RNLS level in T2DM patients was 32.67 (29.73, 36.46) ng/mL, indicating a relatively stable concentration. DKD patients had higher levels of RNLS compared to the control group (34.82 (31.68, 39.37) vs 30.52 (28.58, 33.16), p < 0.0001) (Figure 1(a)). This difference remained significant after adjusting for age, sex, BMI, duration of T2DM, and HbA1c (p < 0.0001). Further adjustments for triglycerides, total cholesterol, ALT, AST, SBP, DBP, and eGFR still showed a significant difference (p = 0.0192). There was no significant difference in serum RNLS levels between males and females (32.66 (30.06, 36.36) vs 32.90 (29.52, 36.49), p = 0.8260) (Figure 1(b)).
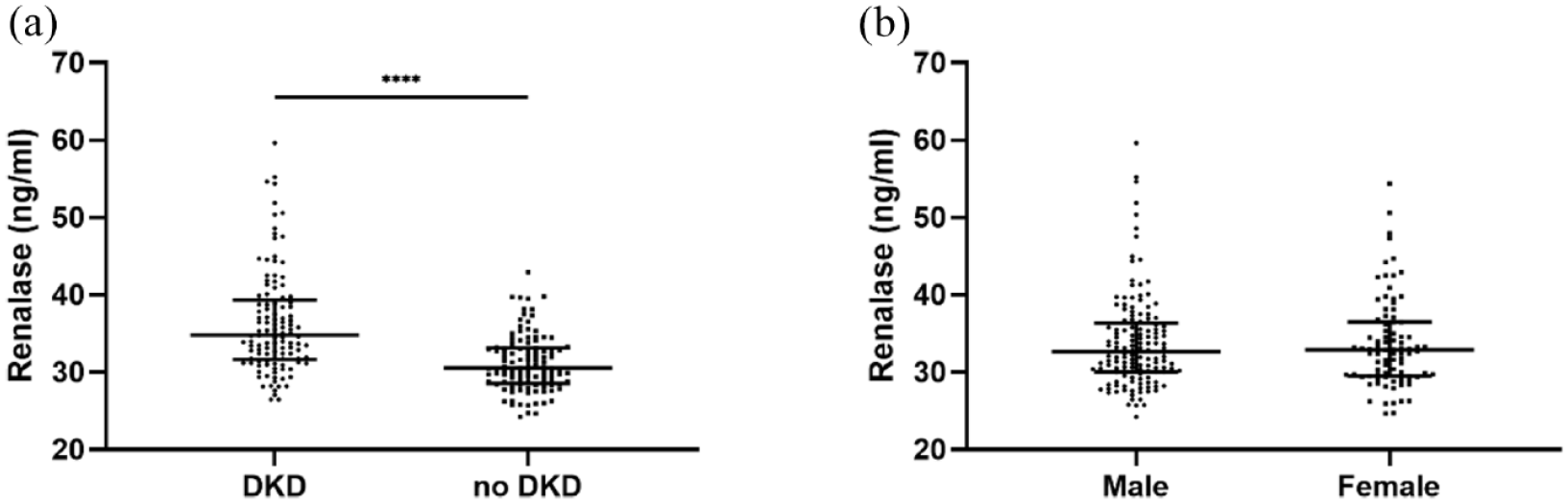
Serum RNLS levels in T2DM patients. (a) Comparison of serum RNLS levels between DKD patients (n = 118) and control group (n = 115) (p < 0.0001). (b) Comparison of serum RNLS levels between male (n = 144) and female (n = 89) groups (p = 0.8260). p Values were calculated by the Mann–Whitney U test. The median is presented as middle black solid line; the upper and lower quartiles are presented by the top and bottom lines, respectively.
Association between serum RNLS levels with anthropometric and biochemical traits
We further analyzed the association between serum RNLS levels and clinical traits. There was no correlation between serum RNLS levels and age (r = 0.03, p = 0.6753), BMI (r = 0.12, p = 0.0614), SBP (r = −0.03, p = 0.6877), DBP (r = −0.01, p = 0.9345), ALT (r = 0.14, p = 0.0619), and AST (r = 0.07, p = 0.2929) (Figure 2(a)–(f)). Regarding kidney function-related traits, serum RNLS was negatively correlated with eGFR (r = −0.31, p < 0.0001) (Figure 3(a)). Serum RNLS was positively correlated with AER (r = 0.39, p < 0.0001), serum creatinine (r = 0.28, p < 0.0001), and uric acid (r = 0.14, p = 0.0319) (Figure 3(b)–(d)).
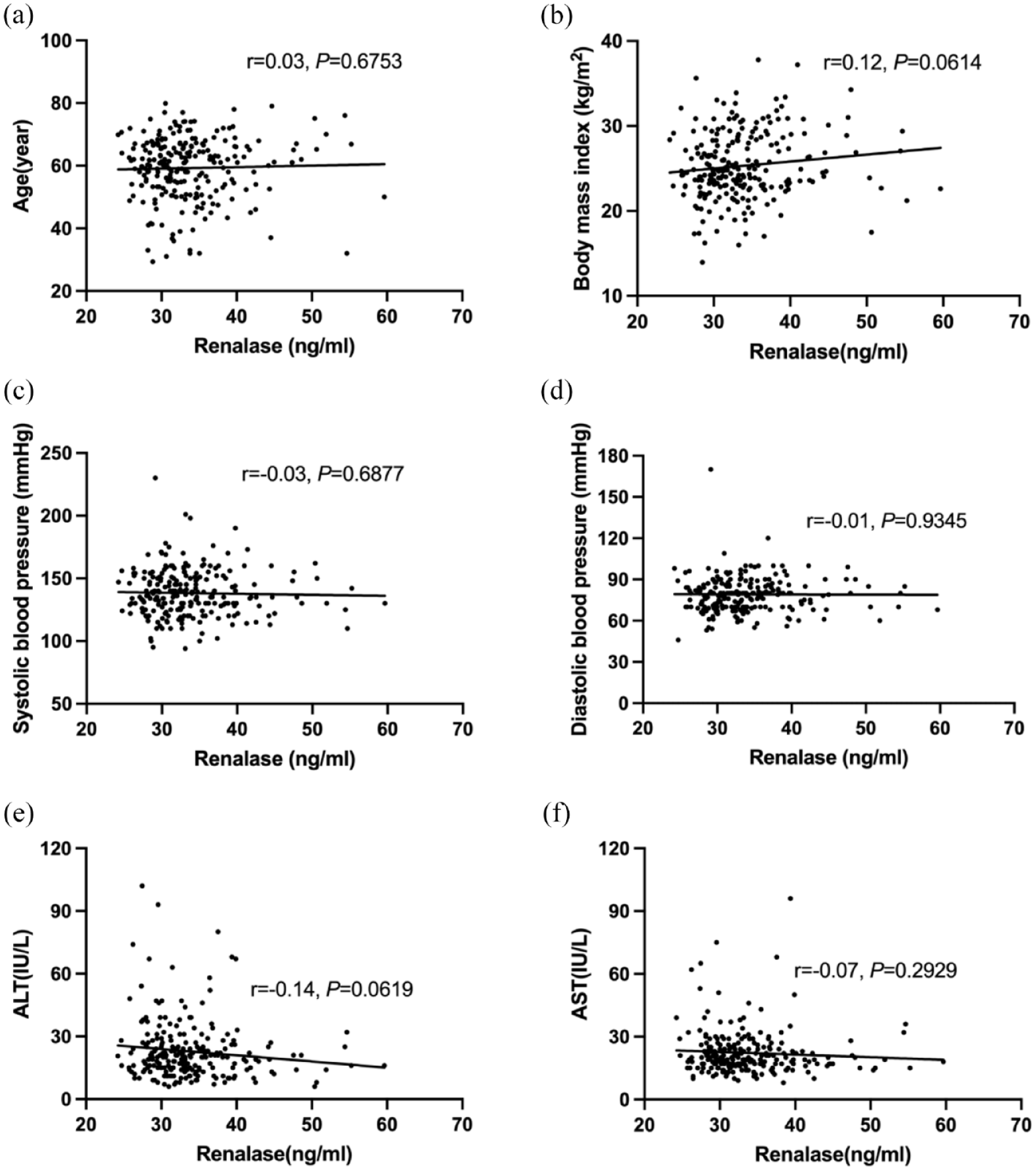
Relationship between serum RNLS levels with basic clinical characteristics. (a) Relationship between serum RNLS levels with age, body mass index (b), systolic blood pressure (c), diastolic blood pressure (d), alanine aminotransferase (e), and aspartate aminotransferase (f) in T2DM patients (n = 233).

Relationship between serum RNLS levels and kidney function-related traits. (a) Comparison between RNLS levels with estimated glomerular filtration rate, log-transformed albuminuria (b), serum creatinine (c), and uric acid (d) in T2DM patients (n = 233).
Given the association between serum RNLS levels and kidney function, we aimed to investigate the correlation between these traits and serum RNLS levels in our study. We stratified the study population into tertiles (low RNLS levels, from 24.23 to 30.52 ng/mL, n = 77; middle RNLS levels, from 30.58 to 34.61 ng/mL, n = 78; high-RNLS levels, from 34.62 to 59.64 ng/mL, n = 78). The traits corresponding to the RNLS tertiles were analyzed after adjusting for age, sex, BMI, HbA1c, and duration of T2DM (Table 2, Figure 4). A significant difference was observed in eGFR (β ± SE = −14.92 ± 4.59, p = 0.0013), serum creatinine (β ± SE = 8.58 ± 3.00, p = 0.0046), and carotid IMT (β ± SE = 0.05 ± 0.02, p = 0.0165) across the serum RNLS tertiles. However, no significant differences were found in blood pressure, blood lipid levels, liver function, and AER.
Multiple linear regression analysis of clinical traits with RNLS tertiles.

p Values < 0.05 are shown in bold.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; eGFR, estimated glomerular filtration rate; HDL-C, high-density lipoprotein cholesterol; IMT, intima-media thickness; LDL-C, low-density lipoprotein cholesterol; RNLS, renalase.

Heatmap showed the clinical characteristics in three groups divided by RNLS tertile. Each cell in the figure showed the relative levels of clinical traits among groups.
Relationship between RNLS concentration and diabetic macroangiopathy
Given that high-RNLS levels were associated with higher carotid IMT, we further explored the association between serum RNLS levels and diabetic macroangiopathy. In our study, patients with diabetic macroangiopathy exhibited significantly higher levels of carotid IMT compared to controls (p < 0.001) (Figure 5(a)). Similarly, patients with diabetic macroangiopathy also showed elevated levels of RNLS compared to controls (p < 0.001) (Figure 5(b)). Considering the influence of DKD on serum RNLS levels, we categorized the study population into four groups: (1) no DKD and no diabetic macroangiopathy, (2) DKD without diabetic macroangiopathy, (3) diabetic macroangiopathy without DKD, and (4) both DKD and diabetic macroangiopathy. The results revealed that patients with both DKD and diabetic macroangiopathy had the highest levels of RNLS (Figure 5(c)). Tertile analysis further indicated that the high-RNLS group exhibited the highest incidence of cardiovascular disease.
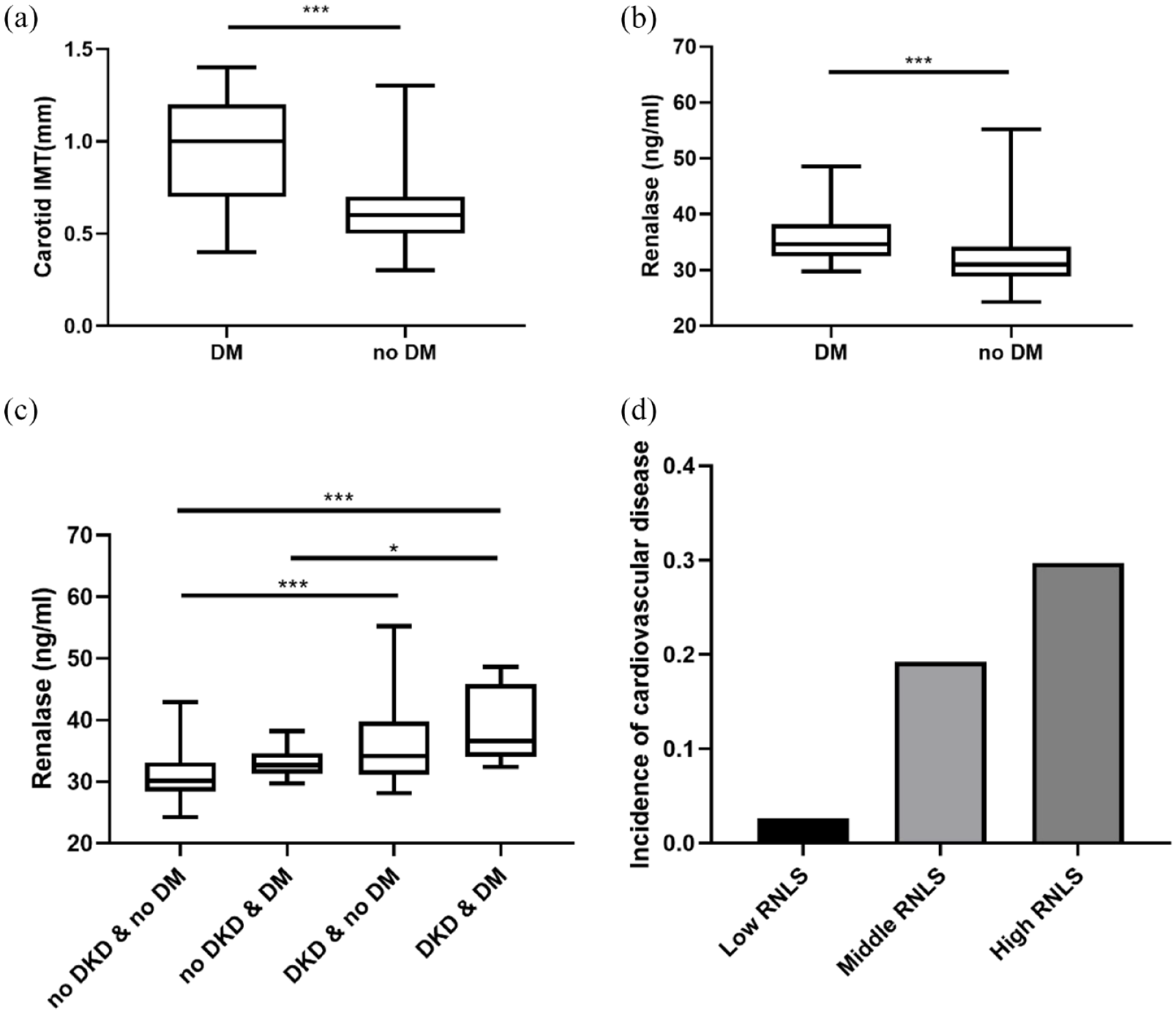
Association between serum RNLS levels with DM. (a) Comparison of carotid IMT levels and RNLS (b) in DM and control group. (c) Comparison of serum RNLS levels in the study population divided by DKD and DM. (d) Incidence of DM disease in RNLS level tertiles.
Receiver operating characteristic curve analysis
To evaluate the diagnostic value of serum RNLS levels for DKD and diabetic macroangiopathy, receiver operating characteristic (ROC) curve analyses were conducted. For DKD diagnosis, the area under the curve (AUC) of the ROC curve was 0.758 (95% confidence interval (CI) = 0.697–0.819, p < 0.0001) (Figure 6(a)), with a specificity of 78.30% and sensitivity of 62.70%. The cut-off value for serum RNLS in diagnosing DKD was determined to be 33.36 ng/mL. For diabetic macroangiopathy, the AUC of the ROC curve was 0.749 (95% CI = 0.660–0.838, p = 0.0001) (Figure 6(b)), with a specificity of 78.26% and sensitivity of 60.63%. The cut-off value for serum RNLS in diagnosing diabetic macroangiopathy was found to be 32.44 ng/mL.

ROC curve analysis. (a) ROC curve analysis of the prediction of diabetic kidney disease in the T2DM patients. (b) ROC curve analysis of prediction of diabetic macroangiopathy in T2DM patients.
Discussion
In the present study, we examined serum RNLS levels in patients with T2DM and observed significantly higher levels in those with early DKD. We found no significant associations between serum RNLS levels and age, sex, SBP, or DBP. However, serum RNLS levels were significantly associated with kidney function-related traits. Additionally, we observed higher IMT levels in the higher serum RNLS group. Subgroup analysis further indicated that serum RNLS may play a crucial role in both DKD and diabetic macroangiopathy, suggesting its potential as a diagnostic marker for early DKD and related cardiovascular diseases.
RNLS, a secreted flavoprotein, serves dual roles as both an enzyme and a cytokine, protecting cells against apoptosis.18,29 Population studies have demonstrated that serum RNLS levels are significantly elevated in CKD patients, particularly in those with ESRD, and show a strong inverse relationship with eGFR. These findings strongly suggest that RNLS plays a role in the decline of kidney function.30–32 However, there has been few data revealing serum RNLS levels in the early stages of DKD. In the present study, we focused on early-stage DKD characterized by slightly impaired kidney function, principally manifested as microalbuminuria or macroalbuminuria. From the DKD case–control population in T2DM patients, we found that RNLS levels were significantly increased in early DKD. This finding suggests a role for RNLS in early DKD despite relatively normal kidney function. The protective function of RNLS on organs has long been recognized. Secreted RNLS in plasma functions as an anti-apoptotic factor, binding with its receptor PMCA4b and stimulating calcium efflux through the activation of the Phosphoinositide 3-kinase and MAPK pathways, inducing the expression of Bcl-2 and inhibiting caspase-3 mediated apoptosis. Thus, RNLS protects from acute kidney injury and cardiac ischemia. 33 Recent studies have shown that RNLS can significantly ameliorate renal interstitial fibrosis through inhibiting the ERK pathway, lowering the expression of p21, and attenuating albuminuria, glomerular hypertrophy, mesangial expansion, and extracellular matrix accumulation.19,34 Besides, RNLS can also exert anti-inflammatory and hemodynamic improvement effects.35,36 Thus, RNLS may act as a compensatory mechanism in the early stages of the disease, protecting the kidney from damage. RNLS may also be a biomarker of DKD even if eGFR remains normal, and may actively participate in the regulation of tissue damage.
In previous studies, RNLS had been claimed to be a monoamine oxidase that can degrade catecholamines; as a result, lowering blood pressure and improving hemodynamics. Xu et al. reported that supplementation with exogenous recombinant RNLS can lower blood pressure, and Desir et al. reported that interference with RNLS gene expression could increase blood pressure by 13 mmHg. It seems that serum RNLS levels were inversely associated with blood pressure. However, there was also debate on the function of RNLS as a monoamine oxidase oxidizing catecholamine substrates, as it shared only 13% similarity with monoamine oxidase.37–39 In our study, we did not observe a significant association between serum RNLS levels and blood pressure. This result is consistent with several other studies that have reported no relationship between RNLS and blood pressure in adults with normal kidney function, heart transplant recipients, and patients undergoing peritoneal dialysis.40–42 Besides, paradoxical results were also observed between RNLS gene polymorphisms and hypertension occurrence.43,44 We speculated that T2DM patients with DKD had higher blood pressure levels, which might require more RNLS to help lower blood pressure, thereby masking the inverse relationship between RNLS and blood pressure. Additionally, blood pressure regulation is complex, with many other factors potentially playing major roles. Furthermore, the patient’s medication regimens also need to be considered. Taken together, whether RNLS functions as a monoamine oxidase remains disputed, and the mechanism by which RNLS participates in DKD through blood pressure regulation requires further exploration.
Previous studies have suggested that RNLS levels are related to age 45 ; however, no significant correlation was found in this study. This discrepancy may be due, in part, to the lower average age of patients in our cohort compared to those in previous studies. Additionally, the incidence of heart and kidney diseases increases with age, which could contribute to higher serum RNLS levels observed in older populations. As for other traits, we found a nominal association of serum RNLS with BMI and alanine transaminase. This may be due to the limitation of our sample size, which needs further verification in a larger population. Notably, among the traits studied, serum RNLS was significantly associated with renal functional indicators, even in the early stages of DKD. Additionally, RNLS was relatively stable in serum, suggesting its potential diagnostic value for early DKD. Therefore, we evaluated its diagnostic value using ROC curve analysis.
DKD is a major cause of CKD and is associated with an exceptionally high rate of cardiovascular diseases.46,47 RNLS, as a mediator connecting the kidneys and cardiovascular system, warrants significant attention. Studies have shown that, compared to its predictive value for hypertension, RNLS has a higher prognostic value for ischemic heart disease. As a cytokine, RNLS secretion increases in response to elevated HIF1a expression, thereby protecting organs from ischemic damage. Currently, using ultrasound to measure carotid IMT is a convenient test that can screen high-risk populations for CVD.
Our study demonstrated that the carotid IMT was thicker in the high serum RNLS group, indicating that elevated RNLS levels also suggest a high risk of cardiovascular events, primarily due to ischemic damage. Further analysis indicated that the percentage of T2DM patients with diabetic macroangiopathy was significantly higher in the high-RNLS group, reinforcing RNLS’s role in identifying high-CVD risk populations. To further clarify the role of RNLS levels in diabetic macroangiopathy and DKD patients, we conducted a subgroup analysis. The results showed significantly increased RNLS levels in patients with diabetic macroangiopathy or DKD, with the highest levels observed in patients with both conditions. This suggests that elevated RNLS levels predict the possibility of DKD accompanied by diabetic macroangiopathy. Previous studies have analyzed the predictive value of RNLS for cardiovascular events in CKD patients and obtained similar results. However, given the high incidence of diabetic macroangiopathy in DKD, it is crucial to analyze and predict cardiovascular events specifically in T2DM patients.
This study had some limitations. First, our sample size was relatively limited, which may have resulted in insufficient analysis of weak metabolic effects. Additionally, the control group in this study only included patients without DKD and DR, lacking patients solely with DKD or those analyzed in conjunction with DR. This may introduce a certain degree of bias. Second, the main focus of this study’s cardiovascular disease assessment was on the carotid artery, and data on ultrasound measurements of the lower extremity arteries were lacking. Moreover, this was an observational study, and data on the progression of DKD and CVD in individuals with high-RNLS levels were not available. Further, longitudinal studies are needed to elucidate the role of RNLS in the progression of DKD and CVD.
Conclusion
Circulating RNLS levels were found to be significantly elevated in patients with DKD and diabetic macroangiopathy, indicating that RNLS may have potential as an early diagnostic marker for these conditions. This finding suggests that monitoring RNLS levels could aid in the early detection and management of DKD and diabetic macroangiopathy, potentially improving patient outcomes.
Supplemental Material
sj-docx-1-taj-10.1177_20406223241286677 – Supplemental material for The early diagnostic value of serum renalase level in diabetic kidney disease and diabetic macroangiopathy: a retrospective case–control study
Supplemental material, sj-docx-1-taj-10.1177_20406223241286677 for The early diagnostic value of serum renalase level in diabetic kidney disease and diabetic macroangiopathy: a retrospective case–control study by Li Jin, Wensu Wang, Rong Zhang, Jianguo Shen, Yangyang Li and Yi Zhang in Therapeutic Advances in Chronic Disease
Footnotes
Acknowledgements
We extend our gratitude to all the staff and study participants at Shanghai Jiao Tong University Affiliated Sixth People’s Hospital for their invaluable contributions and dedicated participation.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.