
Abstract
Background:
Ultrasound therapy is a non-invasive technique used to address a variety of health issues.
Objectives:
This systematic review and meta-analysis aim to assess the effectiveness of ultrasound therapy in alleviating pain associated with musculoskeletal diseases.
Design:
This study was conducted following PRISMA guidelines, with relevant articles identified through comprehensive searches in electronic databases.
Data sources and methods:
We conducted searches across multiple databases, including Scopus, PubMed, MEDLINE, ProQuest, Science Direct, CINAHL, AIM, and ELDIS. Two independent reviewers screened the titles and abstracts of the retrieved articles. We included randomized controlled trials (RCTs) and observational cohort studies published between 2010 and 2023 that evaluated ultrasound therapy for knee and shoulder skeletal disorders. The selected data were analyzed qualitatively and synthesized, with the risk of bias assessed using the RoB2 tool.
Results:
Initially, 117 articles were reviewed using the search strategy, and 10 trials that met the inclusion criteria were identified. In seven of these studies, the primary musculoskeletal disorder was osteoarthritis, while three studies focused on shoulder pain and impingement. Most studies indicated that ultrasound therapy significantly reduced pain. The meta-analysis showed that ultrasound therapy was significantly more effective than other interventions for knee disorders (I2 = 51%, Z = 2.65, p = 0.008). However, for shoulder disorders, both ultrasound and other intervention methods were found to be ineffective (I2 = 93%, Z = 0.73, p = 0.46).
Conclusion:
The current evidence supports the effectiveness of ultrasound therapy in reducing pain and aiding rehabilitation for knee conditions. However, there are mixed results regarding its efficacy for shoulder conditions, highlighting the need for further research in this area.
Introduction
Ultrasound therapy has become widely used in recent decades. 1 The production of ultrasound waves, through the absorption of mechanical energy, generates heat and induces therapeutic effects on tissues. For example, the application of heat relaxes muscles, enhances local blood flow, reduces inflammation, and promotes tissue regeneration. 2 In cases of chronic pain, the continuous mode is typically used to target tissues, with the heating of deep tissues, such as tendon or ligament insertion points, often alleviating pain.
Ultrasound therapy was traditionally used mainly for its thermal effects. However, there is a growing trend in its application for non-thermal effects, particularly in soft tissue reconstruction, wound healing and bone fracture recovery. Continuous ultrasound is primarily associated with thermal effects, while low-intensity pulsed ultrasound (LIPUS) is linked to non-thermal effects. 3 Ultrasound acoustic cavitation, which has non-thermal effects, enhances cell permeability and represents a potential mechanism for pain treatment. 4
In cases of acute and sub-acute soft tissue injuries, the primary objective is typically to avoid significantly increasing temperature, swelling or inflammation. Therefore, pulsed ultrasound therapy is preferred. Pulsed ultrasound settings provide therapeutic effects on soft tissue, cavitation and acoustic flow while minimizing heat generation.5,6 Beyond the biophysical effects of therapeutic ultrasound, LIPUS has been associated with a variety of benefits, including spasmolytic, anti-inflammatory, sympatholytic, tissue regulation and trophic effects. Additionally, LIPUS enhances microcirculation, increases cell membrane permeability, boosts protein biosynthesis, regulates muscle tone and improves cell metabolism. 7
While low-intensity ultrasound is often preferred for treating skeletal disorders, both continuous and pulsed methods can be used. However, some challenges have been identified regarding the use of ultrasound therapy as an adjunctive treatment. These challenges include the lack of standardized treatment protocols for various clinical situations, conflicting results regarding ultrasound’s efficacy in certain joints, and its comparative effectiveness with other physical treatments such as hyperthermia and laser therapy.8–10 This systematic review and meta-analysis aimed to assess the efficacy of ultrasound therapy in alleviating musculoskeletal pain. After identifying relevant randomized controlled trials (RCTs), we thoroughly analyzed the methodologies and scrutinized the findings to determine the significance of ultrasound in treating musculoskeletal diseases. A key feature of our systematic meta-analysis is the inclusion of studies that focus on ultrasound therapy as the primary treatment modality. This approach allows us to comprehensively evaluate ultrasound therapy without the confounding effects of other adjunctive therapies.
Methodology
Searched databases and eligibility criteria
This systematic review and meta-analysis included studies published between 1 January 2010, and 15 July 2023, that used ultrasound as a treatment for musculoskeletal disorders affecting the knee and shoulder. We analyzed all RCTs and observational cohort studies published during this period.
We conducted a systematic search across multiple databases, including Scopus, PubMed, MEDLINE, ProQuest, Science Direct, CINAHL, AIM, and ELDIS, to identify relevant scientific articles and reports for further analysis. The search criteria excluded meta-analyses and systematic reviews, non-systematic reviews, scoping and narrative research, case reports, technical studies and studies not published in English. Only studies published in peer-reviewed journals were included. To minimize the effects of external variables, validity and reliability studies were excluded from the analysis.
The search strategy involved using a combination of several keywords in the specified databases. These keywords included ‘ultrasound’, ‘ultrasonic’ [mesh], ‘ultrasound therapy’, ‘sonotherapy’, ‘musculoskeletal’, ‘musculoskeletal and neural physiological phenomena’ [mesh], ‘musculoskeletal physiological phenomena’ [mesh], ‘musculoskeletal system’ [mesh], ‘musculoskeletal abnormalities’ [mesh], ‘musculoskeletal pain’ [mesh] and ‘musculoskeletal diseases’ [mesh]. This comprehensive approach aimed to capture relevant literature about ultrasound therapy in musculoskeletal disorders.
Review criteria
The systematic review followed the PRISMA guidelines for study selection and data extraction. 11 Two independent reviewers screened the titles and abstracts of articles identified through keyword searches in relevant databases, applying eligibility criteria. Abstracts were assessed for eligibility, and duplicates were manually removed. Disagreements were resolved with input from a third reviewer. Additionally, we conducted a manual search and explored gray literature to ensure the inclusion of eligible articles and avoid overlooking any relevant sources.
After removing duplicates and irrelevant records, and screening the abstracts of eligible studies, we identified a total of 117 relevant articles. Experimental studies, animal studies, case reports, reviews and technical studies were then excluded from the initial pool of articles. Following a comprehensive review of the full texts, we determined that 10 studies met the inclusion criteria and were selected for further analysis. The search and selection processes are outlined in Figure 1.

Flow charts for the identified, displayed and included studies.
Characteristics assessment
A qualitative assessment based on characteristics was conducted to evaluate details of previous studies, including the country and location of the study, age range and sample size. Additionally, technical aspects of the ultrasound therapy method were scrutinized, such as the frequency of ultrasound waves, the muscles targeted, intervention specifics, treatment duration, intensity, use of ultrasound imaging and the gold standard tool/method employed. These factors were assessed to gain a comprehensive understanding of the studies included in the analysis.
The Critical Appraisal Skills Programme (CASP) protocol was used to assess the quality of the RCT studies. 1 This checklist includes 11 queries addressing essential characteristics of the RCTs, such as the type of study, clarity of research questions, study design, applicability of results, accuracy of findings, use of participant data, assessment of benefits and consideration of investigation costs. Inter-examiner discrepancies were evaluated by calculating the agreement rate for each CASP checklist, ensuring consistency and reliability in the appraisal process.
Risk of bias assessment and quantitative data synthesis
The risk of bias assessment was conducted using the RoB2 tool, which is freely available in Excel format (https://www.riskofbias.info). Bias parameters such as the random sample selection, blinding of participants and personnel, outcome assessment and handling of incomplete data were evaluated and categorized as ‘low risk’, ‘high risk’ or ‘unclear risk’. 12
We conducted a quantitative analysis to identify trends in the characteristics among individual studies and compare them against expected standards. This approach helps provide insights into the overall quality and rigor of the included studies.
Results
Qualitative analysis and clinical usage
Table 1 presents the characteristics of the reviewed articles, detailing sample size, musculoskeletal disorder, type of pain, intervention, ultrasound therapy protocol and outcomes related to pain reduction. The studies involved adult participants, with the majority aged between 40 and 60 years. The average sample size across the studies was 65.0 ± 29.2, and the average treatment duration was 12.1 ± 6.2 days. Most of the reviewed studies reported improvements in pain reduction following ultrasound therapy.13–17
Characteristic of the included studies.

NR, not reported; STM, soft tissue mobilization; US, ultrasound.
Risk of bias quality analysis and summary
Figure 2 presents a summary review of the qualitative evaluation of the included studies using the CASP tools for RCTs. All the reviewed articles effectively focused on the central issue, assigned patients to treatments randomly, selected large sample sizes, and precisely reported the treatment effects. However, it remains unclear if all clinically important outcomes were considered in these articles. Additionally, other qualitative parameters varied among the evaluated studies, with detailed information shown in Figure 2. High-risk bias domains were blinded for participants and personnel. In all the evaluated articles, selection bias and the blinding of participants and personnel regarding the treatment protocols were reported at rates of 100% and 60%, respectively.

The assessment of the studies included in the analysis was conducted through CASP tools designed for RCTs, which consist of 11 quality criteria. A green-coded circle denotes that the survey adequately fulfilled the corresponding quality criterion. A yellow-coded indication suggests that the study only partially fulfilled the individual quality criterion. A red-coded indication suggests that the study did not meet the specific quality criterion. (a) Did the trial address the focused issue? (b) Was the patient assignment to treatments random? (c) Were all patients properly accounted for in the conclusion? (d) Were patients, health workers and study personnel blinded to treatment? (e) Were the groups similar at the start of the trial? (f) Were the groups treated equally regarding the conditions of the experimental intervention? (g) Was the treatment effect significantly large? (h) Was the estimation of the treatment effect precise? (i) Can the results be applied in the current review context? (j) Were all clinically important outcomes considered? (k) Are the benefits worth the harms and costs?
Figure 3 presents a Funnel plot that illustrates the risk of bias for the evaluated studies. This plot shows higher precision due to larger sample sizes (y-axis) against the study results (x-axis). Greater symmetry in the plot indicates lower bias. The acceptable symmetry observed in the Funnel plot suggests a low risk of bias among the reviewed studies.

Funnel plot for publication bias.
Table 2 highlights the findings of the quantitative analysis, showing trends in characteristics between individual studies and the expected standard.
Quantitative analyses of the included studies.

Meta-analysis
For the meta-analysis, we excluded one shoulder-related article 13 and two knee-related articles15,20 because their results were unavailable for statistical analysis. Ultimately, we analyzed seven articles: two focused on shoulder-related issues and five on knee-related issues. The overall meta-analysis results indicated that the efficacy of ultrasound was significantly better than the intervention (I2 = 74%, Z = 2.42, p = 0.02). Subgroup analysis revealed that ultrasound was significantly more effective than the intervention for knee disorders (I2 = 51%, Z = 2.65, p = 0.008), whereas both methods were ineffective for shoulder disorders (I2 = 93%, Z = 0.73, p = 0.46) (see Figure 4).
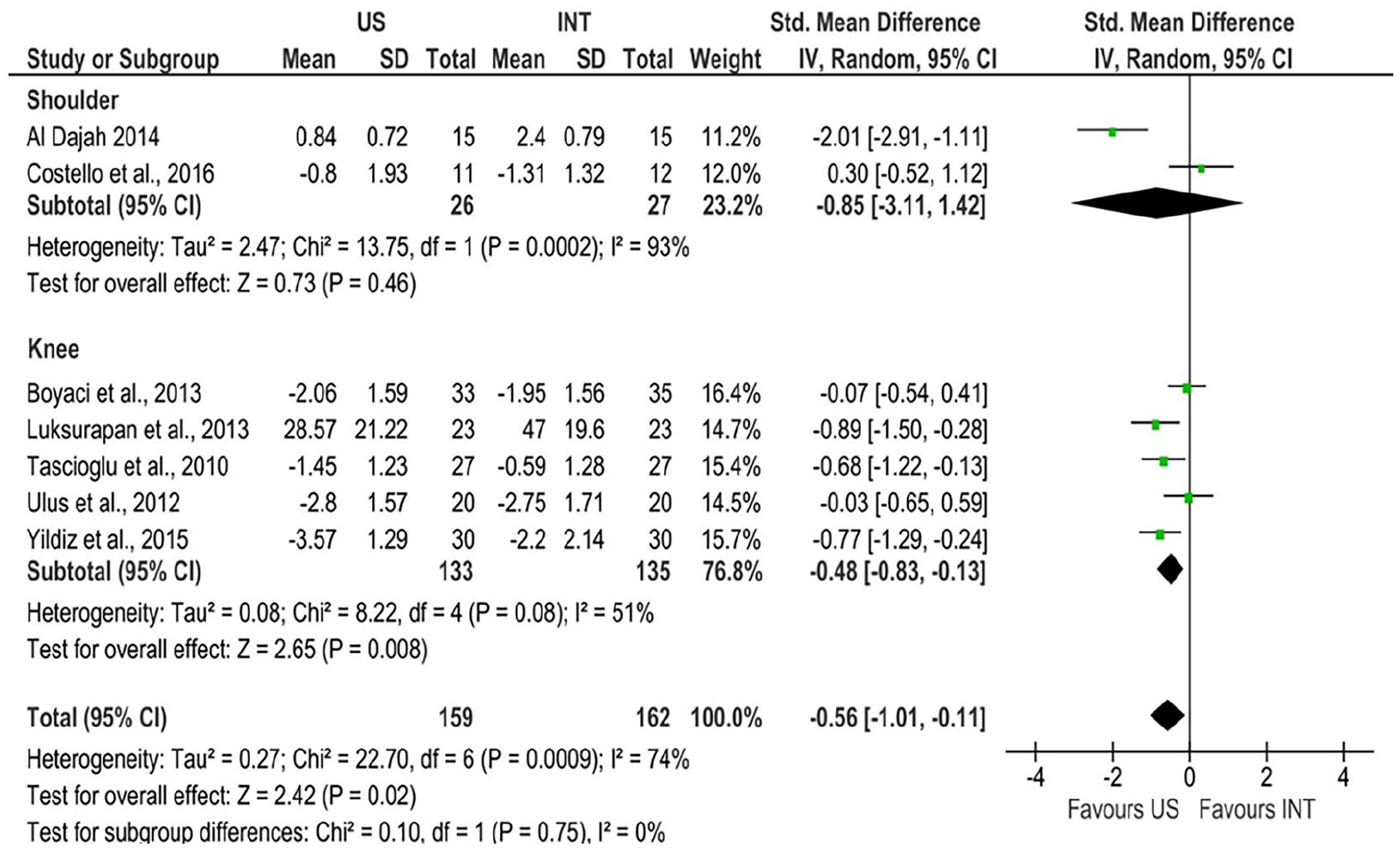
Forest plot results for comparing the results of US and INT in knee and shoulder disorder.
Discussion
Ultrasound therapy is commonly used to treat various musculoskeletal disorders, including myofascial syndrome, 17 back pain, 24 hip, 25 acute ankle sprains 26 and knee osteoarthritis. 27 In this systematic review and meta-analysis, we focused on examining the effects of ultrasound on pain reduction and rehabilitation in the shoulder and knee.
In the reviewed RCT studies on therapeutic interventions such as STM, laser therapy and hyperthermia compared to ultrasound for shoulder muscle relief, evidence indicated that ultrasound therapy has no significant effect on shoulder joints.18,19,28 A study by Costello et al. 18 examined the immediate impacts of STM compared to therapeutic ultrasound among patients with neck and arm pain showing neural mechanical sensitivity. Outcomes were gathered immediately before and after the treatment, as well as during a follow-up period of 2–4 days. The study showed that STM significantly reduces shoulder pain compared to ultrasound therapy, which did not result in significant pain reduction. In another study, 29 the authors evaluated the short-term effectiveness of high-intensity laser therapy (HILT) versus ultrasound therapy in treating subacromial impingement syndrome in 70 patients. They found that participants experienced a more substantial reduction in pain and improvement in joint movement and muscle strength in the affected shoulder after undergoing 10 treatment sessions of HILT compared to those receiving ultrasound therapy over 2 consecutive weeks. 29 Additionally, another investigation studied 37 athletes (8 women, 29 men; age range 19–43 years) with symptomatic supraspinatus tendinopathy. The participants were divided into three groups: one received hyperthermia at 434 MHz, another received continuous ultrasound treatment at 1 MHz with an intensity of 2 W/cm² three times a week, and the third performed pendular swinging and stretching exercises for 5 min twice daily. The study reported that patients who underwent hyperthermia experienced significantly greater pain relief compared to those receiving ultrasound therapy or performing exercises. 30 Rahman and Uddin 13 investigated the efficacy of ultrasound therapy with pregabalin, an anticonvulsant, on the pain behavior of 70 stroke patients with shoulder pain. They found that both treatments improved shoulder pain, but pregabalin yielded better results. Additionally, therapeutic ultrasound provided added benefits when administered alongside pregabalin compared to using ultrasound alone. Petterson et al. 31 conducted a double-blind, randomized, multi-site, placebo-controlled study to assess the efficacy of low-intensity continuous ultrasound (LICUS) treatment for chronic upper neck and shoulder pain. In the study, 33 participants with upper trapezius myofascial pain were randomly assigned to receive treatment with either active (n = 25) or placebo (n = 8) devices. Participants self-applied LICUS (3 MHz, 0.132 W/cm2, 1.3 W, 4 h) if their pain rating was equal to or greater than 3, with a total energy of 18,720 J per treatment. The study found that LICUS treatment significantly decreased pain in patients with upper trapezius myofascial pain in the neck and shoulder. In a study by Balci et al., 32 30 patients diagnosed with shoulder adhesive capsulitis were enrolled in a prospective, double-blind, RCT. The study revealed that adding ultrasound to a combination of physical therapy modalities did not provide any additional benefits for treating adhesive capsulitis. Similarly, Ebadi et al. 33 evaluated the potential benefits of ultrasound (3 MHz, 1.5 W/cm2) as an adjunct to exercise and manual therapy in rehabilitating primary adhesive capsulitis in 50 patients. Their findings indicated that continuous ultrasound, when combined with a regimen of semi-supervised exercise and mobilization, did not offer any additional effects compared to placebo ultrasound, as assessed by outcome measures. Previous research highlights the need for further investigations into the use of ultrasound therapy for pain reduction and rehabilitation of shoulder disorders.
There is some evidence that ultrasound therapy can positively affect knee musculoskeletal disorders. However, studies using ultrasound therapy alone are rare, and its efficacy is usually evaluated in combination with other interventions. For instance, Yang et al. 15 examined the impact of ultrasound on knee osteoarthritis in 87 patients (15 men and 72 women). The patients were randomly divided into an ultrasound group and a placebo group. The study found that ultrasound treatment significantly improves joint symptoms, reduces joint swelling, enhances joint mobility and diminishes inflammation in osteoarthritis patients. Luksurapan and Boonhong 23 conducted a study comparing the effects of phonophoresis (PH) with piroxicam and ultrasound therapy in 46 patients aged 58.91 ± 10.50 years with mild-to-moderate symptomatic knee osteoarthritis. Both groups received treatment using an ultrasound program with the stroking technique, continuous mode, 1 W/cm², for 10 min per session, five times a week for 2 weeks. The piroxicam group was treated with 4 g of 0.5% piroxicam gel (equivalent to 20 mg of the drug), while the ultrasound therapy group used a non-drug coupling gel. Both groups showed significant improvements in the visual analog scale (VAS) and total Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores after treatment (p < 0.001). The piroxicam group demonstrated more significant reductions in the VAS pain score (p = 0.009) and improvements in the WOMAC score, though the latter was not statistically significant (p = 0.143). Additionally, Boyaci et al. 22 compared the efficacy of three different deep heating modalities – PH, ultrasound and short-wave diathermy (SWD) – in knee osteoarthritis. Patients were randomly assigned to one of three groups: Group 1 (n = 33) received PH, Group 2 (n = 33) received ultrasound and Group 3 (n = 35) received SWD. Each modality was administered 5 days a week for 2 weeks, totaling 10 sessions. The results indicated that all three modalities were effective, with no significant difference in efficacy among them. Based on these studies, ultrasound therapy has not shown any significant side effects. However, when compared to other physical methods, ultrasound therapy does not demonstrate superior benefits. Therefore, ultrasound therapy can be considered as an additional or alternative treatment option. For example, the ultrasound pulse mode might be more suitable for acute and sub-acute bone conditions due to its lesser thermal effect.14,16,20,21
Ultrasound has been primarily focused on diagnosis, with fewer applications and investigations into long-term rehabilitation and pain reduction treatment protocols. Previous studies have employed various protocols for ultrasound therapy, including different irradiation modes (continuous or pulsed), treatment durations, sessions, irradiation intensities and frequencies. Standardization across diverse clinical conditions is essential. This systematic review and meta-analysis can prove valuable for clinicians aiming to enhance and establish practical standards for ultrasound therapy in pain reduction. It encourages considering ultrasound therapy’s application in clinical practice and aims to contribute to its development and refinement.
Conclusion
Ultrasound therapy is a safe and effective method for reducing pain and rehabilitating knee and shoulder disorders. The available evidence strongly supports the efficacy of ultrasound in treating knee diseases. However, the literature review reveals some conflicting results regarding the effectiveness of ultrasound therapy for shoulder issues, highlighting the necessity for further research in this specific area.