
Abstract
Objective
Hysterectomy is associated with severe postoperative pain. The relative efficacy of pregabalin compared with other treatments for post-hysterectomy pain is unclear.
Methods
We searched the PubMed, Cochrane Library, and Web of Science databases for studies that compared the use of pregabalin and placebo for reducing pain in patients undergoing hysterectomy.
Results
This meta-analysis showed that pregabalin had limited pain-relieving effects at 2, 6, 24, and 48 hours after hysterectomy compared with placebo. Pregabalin significantly reduced postoperative nausea and vomiting. However, there was no significant difference in postoperative sedation or visual disturbances between patients treated with pregabalin and placebo.
Conclusions
Pregabalin is not clinically superior to placebo in terms of reducing pain intensity and morphine consumption in patients undergoing hysterectomy. However, the limitations of this meta-analysis mean that more high-quality randomized controlled trials are necessary to verify our pooled results.
Introduction
Hysterectomy causes significant postoperative pain, characterized by a combination of somatic and predominantly visceral pain. 1 Poorly managed acute postoperative pain may increase pain-related complications, delay out-of-bed activity, and affect quality of life.2–4 Enhanced recovery after surgery protocols have recently undergone rapid developments and have been widely applied in orthopedic, general, and cardiothoracic surgery.5,6 Numerous kinds of analgesics with different pharmacological mechanisms have been used to reduce postoperative pain.
Pregabalin is a structural analog of the inhibitory neurotransmitter gamma-aminobutyric acid and the main treatment for neuropathic pain. Its analgesic effect differs from that of other analgesics, including morphine, 7 nonsteroidal anti-inflammatory drugs, 8 and morphine-like drugs. 9 Previous studies showed that pregabalin could downregulate visceral hyperalgesia, in addition to reducing the severity of basic pain. 10
A previous meta-analysis indicated that pregabalin could decrease postoperative pain after spinal cord injury, 11 diabetic neuralgia, 12 and neuropathic pain; 10 however, the role of pregabalin following hysterectomy has yet to be defined. Asgari et al. 13 found that pregabalin played an important role in reducing postoperative pain after laparoscopic hysterectomy; however, another recent study questioned its efficacy and reported that it had limited ability to reduce pain intensity in hysterectomy patients. 14
The current meta-analysis aimed to determine if pregabalin was an effective treatment for managing acute postoperative pain following hysterectomy and to determine the risk of drug-related adverse effects.
Materials and methods
This meta-analysis was based on previously published studies and did not require ethical approval or patient consent. This systematic review and meta-analysis was performed in accordance with the Preferred Reporting Item for Systematic Review and Meta-analysis (PRISMA) guidelines.15,16
Search strategy
Two trained researchers (Jie Ni and Juan Jiang) independently searched the PubMed, Cochrane Library, and Web of Science databases, without restrictions on publication date, to identify relevant trials. We used a hierarchical approach based on titles, abstracts, and full texts to assess the relevance of the trials. The following search terms and their synonyms were used: “Trachelectomy (All Fields),” “Hysterectomy, Vaginal (All Fields),” “Hysterectomy” “pregabalin (All Fields),” “gamma-Aminobutyric Acid (All Fields),” and “3-(aminomethyl)-5-methylhexanoic acid (All Fields).” The researchers used the Boolean operators “and” or “or” to combine search terms. To ensure the comprehensiveness of the study, we also manually searched the reference lists of relevant articles to identify other trials.
Inclusion criteria and study selection
Trials were included if they met the following criteria: 1) patients underwent hysterectomy under general anesthesia or spinal anesthesia; 2) intervention group received pregabalin; 3) control group received placebo; 4) data available for at least one of the following outcomes: postoperative morphine consumption, pain intensity at rest or mobilization at 2, 6, 24, 48, and 72 hours following hysterectomy, and side effects (occurrence of nausea, vomiting, sedation and visual disturbances); and 5) comparative study. The reliability of the study selection was determined by Cohen’s kappa test with an acceptable threshold value of 0.61.17,18
Studies were excluded if they met the following criteria: 1) pregabalin compared with gabapentin without a control group; 2) design of the experiment not reasonable; 3) duplicate reports, systematic reviews and meta-analyses; and 4) animal experiments.
Data extraction
All potentially relevant studies retrieved from the literature search were imported into Endnote X9 (Clarivate Analytics, Philadelphia, PA, USA), and duplicate studies were excluded by the software. The two above researchers read the titles and abstracts of each article to rule out those that did not meet the requirements. The same researchers then read the full texts of the remaining articles to further exclude trials that did not meet the selection criteria. Any disagreements were resolved by discussion with a third researcher (Rui-fang Sun).
Quality assessment
We assessed the quality of each included trial according to the Cochrane risk of bias tool for randomized trials. 19 We assessed the following items: generation of random sequence, concealment of allocation sequence, blinding of participants, incomplete outcome data, selective outcome reporting, and other sources of bias. For each included study, each type of bias was rated as high, low, or unclear and entered into the risk of bias table. The risk of bias was examined by two reviewers concurrently, and discrepancies were resolved by consensus.
Outcome measures and statistical analysis
The efficacy and safety of pregabalin compared with placebo for treating postoperative pain after hysterectomy were assessed using categorical and continuous data, and relative risks (RRs) and standard mean differences (SMDs) with 95% confidence intervals (CIs), respectively, were calculated before data pooling. Pain scores were measured by visual analogue scale, with 100 mm for the most severe pain and 0 mm for no pain at all. Pooled analyses for all outcomes were carried out using the random effects model considering the underlying variables across the included trials. Heterogeneity among the included trials was assessed using the I2 and Q statistics with I2 > 50% or P < 0.10 indicating significant heterogeneity. 20 The robustness of the pooled results was assessed using sensitivity analysis. Moreover, subgroup analysis for the efficacy of outcomes was conducted based on pregabalin dose, risk of bias, and hysterectomy category between subgroups evaluated using the interaction P-value, which assumed that the data in each subgroup were normally distributed. 21 The quality of the evidence was assessed according to each outcome using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) method, which grades the evidence as high, moderate, low, or very low quality. Sensitivity analysis was carried out by removing one study at a time (leave-one-out) to identify sources of heterogeneity. Publication bias was assessed using funnel plots and Egger’s and Begg’s test results. 22 The inspection level for pooled results was two-sided, and P < 0.05 was considered statistically significant. STATA software (Version 12.0; StataCorp, TX, USA) was used to conduct all analyses in this study.
Results
Search results
The flowchart of the study search and selection process is shown in Figure 1. A total of 628 articles (database = 625, other sources = 3) were identified through the literature search and manual searching. The titles and abstracts of 453 articles were reviewed after duplicates were removed. A total of 439 studies were excluded after reviewing the titles and abstracts and the full texts of the remaining 14 studies were reviewed. Fourteen studies13,14,19,23–33 were finally included in the current meta-analysis. The general characteristics of the included studies are shown in Table 1.

Flow diagram of study selection.
General characteristics of the included studies.

a1, postoperative morphine consumption; 2, pain intensity with rest at 2 hours; 3, pain intensity with rest at 6 hours; 4, pain intensity with rest at 24 hours; 5, pain intensity with rest at 48 hours; 6, pain intensity with rest at 72 hours; 7, pain intensity with mobilization at 2 hours; 8, pain intensity with mobilization at 6 hours; 9, pain intensity with mobilization at 24 hours; 10, nausea; 11, vomiting; 12, sedation; 13, visual disturbances.
Quality assessment
All studies had a low risk of bias regarding the blinding of outcome assessment, incomplete outcome data, and selective reporting. Nine studies had a low risk of bias regarding the blinding of participants and personnel. One study 21 did not mention allocation concealment and blinding of participants and personnel. Five studies3,19,20,23,26 had an unclear risk of other bias, and one study 20 had a high risk of other bias. The quality assessment for each study and the results of the included studies are shown in Figure 2.
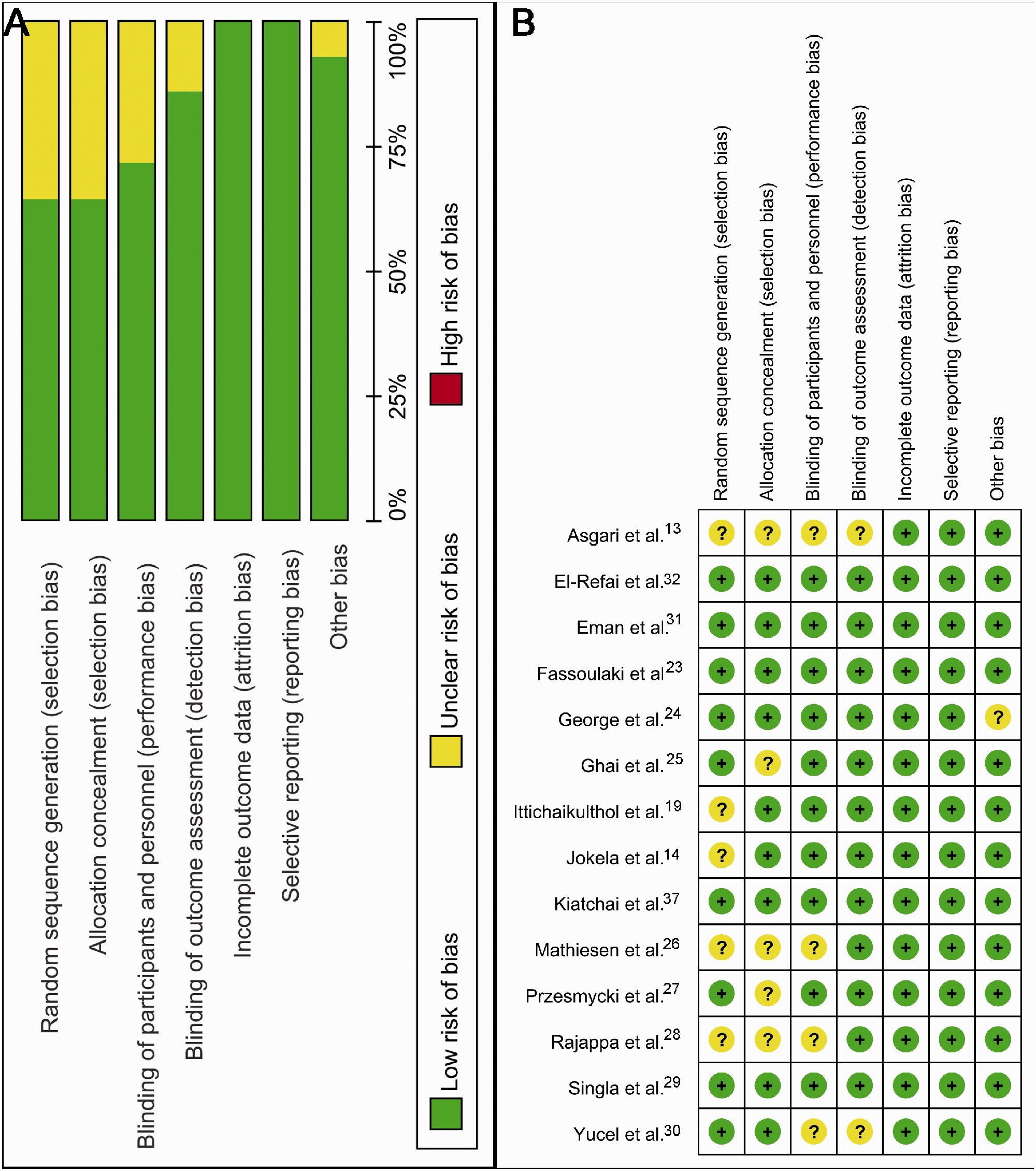
Risk of bias summary for the included studies.
Results of meta-analysis
Postoperative morphine consumption
Trials involving 118 patients reported postoperative morphine consumption as an outcome (Table 2). Compared with the control group, the pregabalin group had a significantly lower postoperative morphine consumption (P < 0.001).
Summary of meta-analysis results.

CI, confidence interval.
Pain intensity with rest following hysterectomy
Compared with the control group, the administration of pregabalin was associated with a significant reduction in pain intensity with rest at 2 hours (P = 0.002; Table 2). The pain intensity with rest at 6 hours is shown in Table 2. Pooled analysis showed that pregabalin also relieved pain intensity with rest at 6 hours (P < 0.001; Table 2), 24 hours (P < 0.001; Table 2), 48 hours (P = 0.001; Table 2), and 72 hours (P = 0.104; Table 2) after hysterectomy.
Pain intensity with mobilization following hysterectomy
Compared with the control group, the administration of pregabalin was associated with a reduction in pain intensity during mobilization at 2 hours (P = 0.003; Table 2), 6 hours (P < 0.001; Table 2), and 24 hours (P < 0.001; Table 2) after hysterectomy.
Side effects
Pooling data showed that pregabalin significantly decreased the occurrence of nausea (P < 0.001; Table 2) and vomiting (P < 0.001; Table 2), as shown by forest plots. However, there was no significant difference between the pregabalin and control groups in terms of the occurrence of sedation (P = 0.129; Table 2) and visual disturbances (P = 0.349; Table 2).
Subgroup analysis, sensitivity analysis, and publication bias
The results of subgroup analyses are shown in Table 3. In terms of the primary outcome of postoperative morphine consumption, there was a significant difference between patients treated with laparoscopic hysterectomy and abdominal hysterectomy (P = 0.002). There was no significant difference between studies with a low risk of bias and those with an unclear/high risk of bias or between studies with different doses of pregabalin (75 mg, P < 0.001; 150 mg, P = 0.005; 300 mg, P = 0.036; 600 mg, P = 0.001).
Subgroup analysis in terms of morphine consumption.

CI, confidence interval.
The results of sensitivity analysis for postoperative morphine consumption are shown in Table 3. None of the included studies was identified as a source of heterogeneity.
The assessment of publication bias using Egger’s and Begg’s tests showed no potential publication bias among the included trials.
GRADE assessment
The GRADE framework revealed low qualities of evidence for postoperative morphine consumption and pain intensity with rest at 2, 24, 48, and 72 hours, and moderate quality of evidence for pain intensity with rest at 6 hours following hysterectomy (Supplementary material S1).
Discussion
The current meta-analysis demonstrated that pregabalin reduced pain scores with rest following hysterectomy by 1.06 points at 2 hours, 0.23 at 6 hours, 0.44 at 24 hours, and 0.69 points at 48 hours, based on a 110-point visual analog scale. However, these reductions were not clinically significant. Pregabalin use also reduced morphine consumption, but this was also not clinically important, especially at doses <150 mg. The quality of evidence for these effects was low or moderate.
The results of this study contradicted previous meta-analyses assessing the use of pregabalin for the management of acute pain in hysterectomy patients. 6 Notably, previous meta-analyses included trials that applied abdominal hysterectomy, and two trials with large samples were missed. In comparison, the present meta-analysis included patients who received either abdominal or laparoscopic hysterectomy. Moreover, we also used the GRADE framework to assess the quality of evidence in relation to the final outcomes to provide guidance for policy makers.
Hamilton et al. 34 conducted a meta-analysis and found no evidence to support the routine use of gabapentinoids for the management of acute pain following total knee arthroplasty. The current meta-analysis found little pain reduction in the pregabalin group, and limited opioid-sparing effects compared with the control group (P < 0.001). Subgroup analysis showed that pregabalin 75 mg had no significant effect on pain intensity from 2 to 72 hours after hysterectomy.
This study had some potential limitations. First, the test power was limited by the sample size. Only 14 studies were included in this meta-analysis, all of which had relatively small sample sizes (n < 100). However, they were all randomized controlled trials, which are considered highly reliable, and all had evidence-based study designs. The GRADE framework therefore indicated that the evidence was of moderate quality, and the main reason for the lower grade was the small sample sizes. Second, the included studies were performed in different patient groups, using different pregabalin doses and different follow-ups, and in various clinical settings, thus increasing the risk of heterogeneity. Finally, the number of included trials was too small (<10 for most outcomes) to conduct an additional analysis of publication bias. However, the systematic review and meta-analysis was carried out in strict adherence to the PRISMA guidelines, to improve the quality of the study.
Conclusion
Pregabalin appeared to be more effective than placebo in reducing pain and morphine consumption in patients undergoing hysterectomy. However, the results were not clinically significant due to the limitations of this meta-analysis, and further high-quality randomized controlled trials are necessary to verify our pooled results.