
Abstract
Background:
Inferior vena cava (IVC) filters are commonly used intravascular devices designed to prevent fatal pulmonary embolism (PE), maintaining the IVC filter as centered as possible is fundamental for achieving its filtration function.
Objective:
This study aimed to characterize the tilt angles of IVC filter between the vascular access of internal jugular vein (IJV) and femoral vein (FV), as well as to identify factors associated with increased or decreased tilt angles between placement and retrieval.
Design:
This is a multicenter retrospective study.
Methods:
A multicenter retrospective study was conducted from October 2017 to March 2019. The primary outcome was the change in filter tilt between placement and retrieval. The secondary outcome was the identifications of factors associated with increased or decreased tilt angle. Relevant variables were analyzed using t-tests, Chi-square tests, Fisher’s exact tests, while multivariate logistic regression analysis was used to determine risk factors.
Results:
A total of 184 eligible patients were included in this study. The IJV group had a lower likelihood of tilt angle over 10° at the time of placement compared to the FVs group (0% versus 12.5%, p = 0.040). Among the 171 patients with a mean dwell time of 22.1 days, the IJV group had a higher likelihood of tilt angle over 10° than the FVs group (10.3% versus 2.3%, p = 0.080). The use of FVs access at placement was associated with a higher difference between placement and retrieval filter tilt angles (p < 0.01). Multivariate logistic regression analysis showed that hypertension [odds ratio (OR) 0.668; 95% confidence interval (CI) 0.328–1.358, p = 0.265], cardiologic artery disease (OR 0.537; 95% CI 0.136–2.130, p = 0.377), cerebral venous disease (OR 0.555; 95% CI 0.186–1.651, p = 0.290), filter types (OR 1.624; 95% CI 0.851–3.096, p = 0.141), and IVC filter thrombosis (OR 1.634; 95% CI 0.804–3.323, p = 0.175) were not associated with increased filter tilt angle. Right side (OR 0.434; 95% CI 0.202–0.930, p = 0.032) or bilateral lower extremity deep vein thrombosis (LEDVT) (OR 0.383; 95% CI 0.148–0.995, p = 0.049) were identified as protective factors.
Conclusion:
IJV access was associated with a lower filter tilt angle at the time of placement, while FVs access was linked to a higher difference between placement and retrieval tilt angles. Right side or bilateral LEDVT were identified as protective factors against increased IVC filter tilt angle.
Introduction
Inferior vena cava (IVC) filters are commonly used intravascular devices designed to prevent fatal pulmonary embolism (PE) in high-risk patients with deep vein thrombosis (DVT) by trapping clots within or cephalad to their struts.1,2 Therefore, maintaining the IVC filter as centered as possible is fundamental for achieving its filtration function. Since the introduction of the IVC filter in 1967, over 259,000 filters have been released in the USA by 2012, making them increasingly common.1,3 Although IVC filters can reduce the prevalence of PE, their potential complications are also well-documented. 4 Some related sequelae of filter placement, such as filter migration, fractures, thrombosis, and IVC wall or adjacent organs perforation, are not uncommon. Filter perforation has been reported with a prevalence of 0–41%, particularly in patients with conical IVC filters.1,4 However, the mechanism of penetration remains not well elucidated, and IVC filter tilt has been shown to be associated with the potential risk of penetration and filter retrieval outcome.1,2,5
IVC filters can be temporary or permanent,4,5 and are typically delivered through the vascular access of internal jugular veins (IJVs) or femoral veins (FVs), ideally in the infrarenal IVC. 5 The anatomic configuration of the IVC is considered a risk factor for filter tilt.6,7 Therefore, performing IVC ultrasound, computed tomography, or venography to identify potentially variant anatomy before the placement procedure may yield important clinical implications. As previously descripted,5–7 filter tilt, referring to an IVC filter at a certain angle along the longitudinal axis of the filter and IVC, may increase the complexity of retrieval attempts and lead to subsequent adverse events. 5 Nonetheless, specific guidelines concerning unambiguous angles for pathological filter tilt remain lacking in the literature, and most studies have defined it as an angle >15° or 20°.5–8 Grullon et al. 7 noted that when placed via the IJVs, the sheath tends to have a straighter angle to the IVC, potentially triggering off fewer filter tilts >20° and access site complications compared with FVs access. However, limited data is available on the relationship between vascular access, immediate filter tilt after placement, self-adjusted tilt before filter retrieval, and the implications of vascular access on adverse events.
Thus, the purposes of the present study are to investigate the effect of vascular access choice at the time of immediate filter placement and retrieval in patients with lower extremity DVT (LEDVT) based on the data from a multicenter randomized controlled trial (RCT), as well as to identify the possible risk factors associated with increased or decreased tilt angles between placement and retrieval.
Methods
Patients and study design
This retrospective cohort study was conducted using data from a multicenter RCT, 9 which was prospectively carried out in 188 LEDVT patients to evaluate the efficacy and safety of PE prevention for Octoparms (Kosell MedTech (Suzhou) Co., Ltd, Suzhou, China) filter compared to Celect (COOK Medical, Bloomington, Indiana) filter at 10 clinical centers from 6 provinces in mainland China from October 2017 to March 2019. 9
All patients aged >18 years who had undergone filters placement in the multicenter RCT were included. Four patients were subsequently excluded because the filters were placed in the suprarenal vein (the flowchart of this study has been shown in Figure 1). Of the remaining 184 eligible patients, 40 underwent IJV access for IVC filter placement and were divided into the IJV group, while 144 underwent FVs access and were divided into the FVs group. In the exploratory factor analysis of tilt angle changes between filters placement and retrieval, 13 were excluded because the filters were placed permanently or presented with incomplete records. A total of 69 patients who experienced increased tilt angle were divided into the increased tilt angle group, and 102 who underwent decreased tilt angle were divided into the decreased tilt angle group. The data concerning these eligible patients were obtained from the medical database system and/or case report form. The baseline demographics, presentation of LEDVT, laboratory and electrocardiogram (ECG) examinations, thrombus characteristics, thrombus limbs, concurrent PEs, comorbidities, risk factors for LEDVT, filter/IVC-relevant information, vascular access of placement, and conjunctive endovascular treatments were all analyzed.
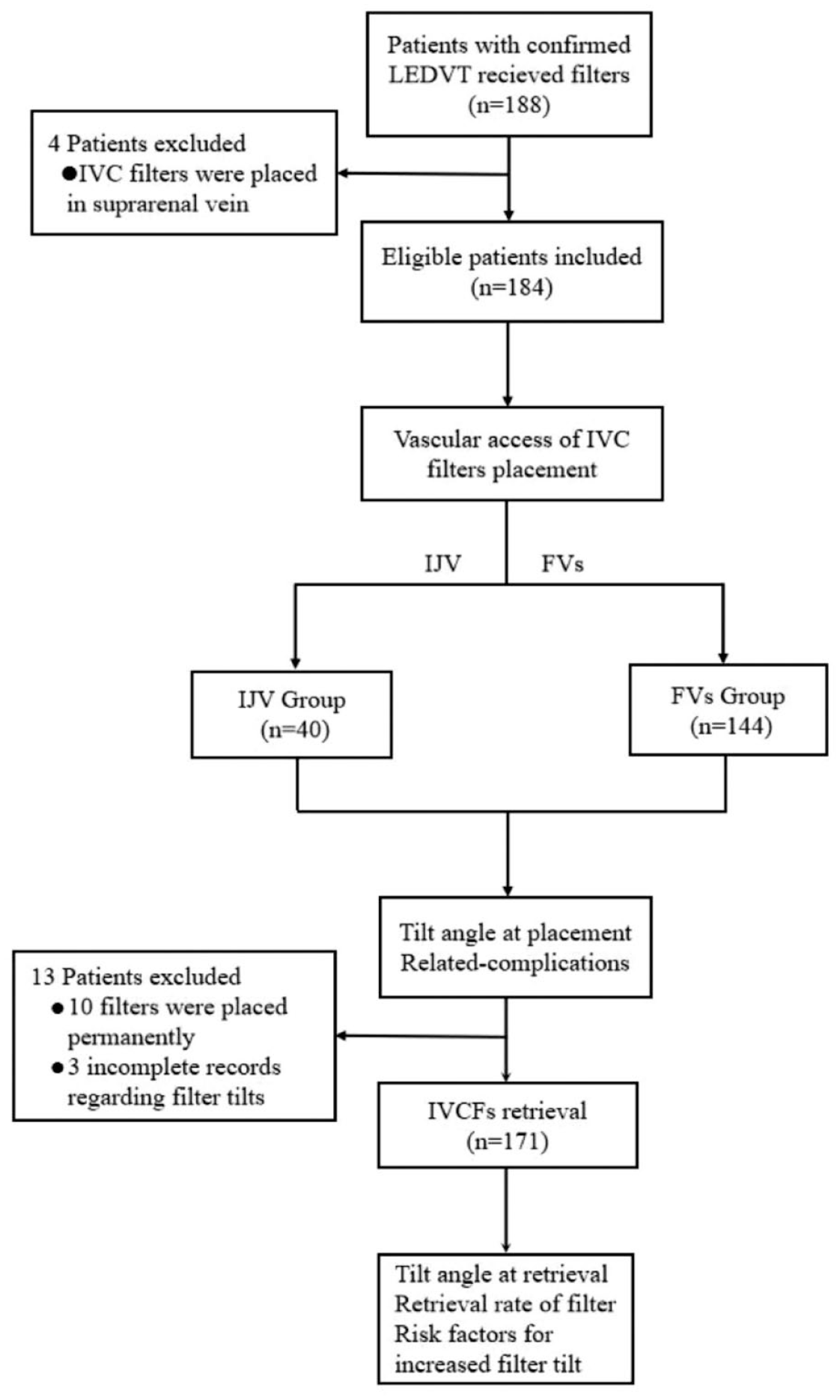
The study flowchart of the inclusion and exclusion criteria of LEDVT patients with IVC filters.
Diagnosis and definition of IVC filter tilt angle and change
To distinguish the variations between IJV and FVs vascular access, the diagnosis of IVC filter tilt was determined by venography immediately after placement and before filter retrieval. Filter tilts were categorized into 0°–5°, 5°–10°, 10°–15°, and >15°, based on the angle between the longitudinal axis of the target vein and the filter on an antero-posterior cavogram. The filters used and filter tilt angle measurement were shown in Figure 2. The primary outcome was the change in filter tilt between placement and retrieval. The secondary outcome was the identification of factors associated with increased or decreased tilt angle, as well as retrieval rate. The filter dwell time was defined as the time from filter placement to filter retrieval, and decision and timing were individualized in each case by the referring interventional radiologist based on the patient’s condition. Increased IVC filter tilt angle was defined as a rise in angulation from placement to retrieval, and the decreased tilt angle was defined as a lower angle at the time of retrieval compared with initial placement. Obesity was defined as body mass index (BMI) > 28 kg/m2, according to a standard criterion from the Working Group on Obesity in China. Proximal LEDVT included thrombus in the common iliac vein, external iliac vein, common FV, proximal and distal segments of the FV, and/or popliteal vein, and isolated distal DVT included thrombus in distal veins, including the anterior tibial vein, posterior tibial vein, peroneal vein, gastrocnemius muscle vein, and soleus muscle vein.1,10

A schematic representation of the Octoparms filter, Celect filter and filter tilt angle measurement. (a) The Octoparms filter, (b) The Celect filter and (c) The filter tilt angle (X1 angle) is measured as the angle between the long-axis of the filter and the long-axis of the inferior vena cava.
Statistical analysis
Statistical analyses were performed using the SPSS statistical software package (version 23.0; SPSS statistical software, Chicago, Illinois, USA) and R statistical language software (version 4.2.1; R Foundation, Vienna, Austria). Continuous data are presented as mean ± standard deviation (SD), and categorical data are given as counts (percentage). When assessing the correlations between two groups and comparing continuous data, including age, IVC diameter, and time to filter retrieval, a t-test was used. The significance of categorical data was tested with a chi-square test or Fisher’s exact test. The relationship of filter tilt between placement and retrieval was evaluated with a pairing graph using the R software. When analyzing the risk factors for increased and decreased IVC filter tilt, a univariate analysis was performed to identify significant variables between the two groups, and multivariate analysis was performed while p < 0.2, controlling for any significant variables. Findings with a p < 0.05 (two-tailed) were deemed statistically significant.
Results
Patients and baseline characteristics
Of the 184 eligible patients in this study, the mean age was 58.47 ± 14.97 years, and 51.6% (95/184) of them were male. The majority of the included patients were of Han ethnicity (96.7%) and married (95.1%), and obesity was noted in 20.7% (31/184) of patients. Regarding the symptoms and signs of LEDVT, more than 65% of them suffered from limb pain and swelling. Time from symptoms onset to admission ⩽7 days and D-dimer value was <10 μg/ml in both groups were presented in 38.6% (71/184) and 81.0% (149/184), respectively. The leading abnormal laboratory test was hematocrits, presenting in 48.4% (89/184) of patients, and abnormal ECG test accounted for 53.3% (98/184) of patients. Concerning thrombus distribution, the majority of the included patients were afflicted with proximal LEDVT (84.2%) and left limb involvement (63.6%). Concurrent PE identified by CT venography was noted in 45.7% (84/184) of these patients. The most common comorbidities and risk factors for LEDVT patients were hypertension (28.3%) and a history of major surgery (32.1%). As for IVC or filter-relevant information, the filters used were conical IVC filters, including Octoparms (50.5%) and Celect (49.5%), and all were placed in the infrarenal vein (100%) via the vascular access of IJV (21.7%) or FVs (78.3%). IVC diameters was 20.33 ± 3.25 mm. When it comes to endovascular treatments, percutaneous aspiration (PAT), percutaneous angioplasty (PTA) and percutaneous stent (PTS) were noted in 17 (9.2%), 38 (20.7%) and 8 (4.3%) of these patients. According to vascular access, these included patients were divided into the IJV group and the FVs group. The baseline demographics, presentation of LEDVT, laboratory and ECG examinations, thrombus characteristics, concurrent PE, comorbidities, risk factors for LEDVT, IVC and filter-relevant information, and conjunctive endovascular treatments for patients who received IVC filters were summarized in Table 1.
Baseline demographics, presentation of LEDVT, laboratory examination, thrombus characteristics, concurrent PE, comorbidities, risk factors for LEDVT, IVC and filter-related information, endovascular treatments for patients who received IVC filters.

Continuous data are presented as the means ± SDs; categorical data are given as the counts (percentage).
Fisher exact.
A total of 34 patients lacked BMI values.
Proximal LEDVT included thrombus in the common iliac vein, external iliac vein, common FV, proximal and distal segments of the FV, and/or popliteal vein.
IDDVT included thrombus in distal veins, including the anterior tibial vein, posterior tibial vein, peroneal vein, gastrocnemius muscle vein, and soleus muscle vein.
BMI, body mass index; CAD, cardiologic artery disease; CVD, cerebral venous disease; ECG, electrocardiogram; IDDVT, isolated distal deep vein thrombosis; IVC, inferior vena cava; LEDVT, lower extremity deep vein thrombosis; PAT, percutaneous aspiration; PE, Pulmonary embolism; PTA, percutaneous angioplasty; PTS, percutaneous stent; FV, femoral vein; SD, standard deviation; VTE, Venous thromboembolism.
Filter tilt change at the time of placement and retrieval
The tilt of IVC filter following filter placement were observed in all eligible patients (184/184), and tilt angles ranged from 0.2° to 19.2°. Frequency and comparison of tilt stratified by vascular access are listed in Table 2. Of these 184 patients, the filter tilt angles of 0°–5°, 5°–10°, 10°–15°, and >15° were noted in 110 (64.3%), 56 (32.7%), 15 (8.2%), and 3 (1.8%) patients, respectively. These findings showed that filter tilt angles of the IJV group focused on under 10°, such as 0°–5° (70%) and 5°–10° (30%), while the FVs group tended to have more patients with IVC filter tilt angles over 10°, presenting in 10°–15° (10.4%) and >15° (2.1%). This demonstrates that the IJV group had a lower likelihood of tilt angle of over 10° measured at the time of placement compared to the FVs group (0% versus 12.5%, p = 0.040).
Removal rate, time and filter tilt angle at the time of placement and retrieval via IJV or FV access, and related complication.

Continuous data are presented as the means ± standard deviations; categorical data are given as the counts (percentage).
Fisher exact.
FVs, femoral veins; IJV, internal jugular vein; IVC, inferior vena cava; PE, Pulmonary embolism.
With a mean filter dwell time of 22.1 days (range, 4–190 days), 10 filters were placed as permanent filters, and three had missing tilt data. Of the remaining 171 filters, the filter tilt angles at the time of retrieval of 0°–5°, 5°–10°, 10°–15°, and >15° were noted in 109 (63.7%), 55 (32.2%), 5 (2.9%), and 2 (1.2%) of patients, respectively. The IJV group had a higher likelihood of tilt angle over 10° than that in the FV group (10.3% versus 2.3%, p = 0.080). The use of IJV access at placement was not significant statistically (p > 0.05), while FVs access was associated with a higher difference between placement and retrieval filter tilt angles (p < 0.01). The transitions of filter tilt angles concerning IJV access [shown in Figure 3(a)] and FVs access [shown in Figure 3(b)] at the time of placement and retrieval are shown. The retrieval rate was 92.7% (171/184), 2.3% (4/171) patients experienced incident PE and 32.7% (56/171) suffered from filter-related thrombosis at the time of retrieval, the differences between the two group were not statistically significant (p > 0.05).
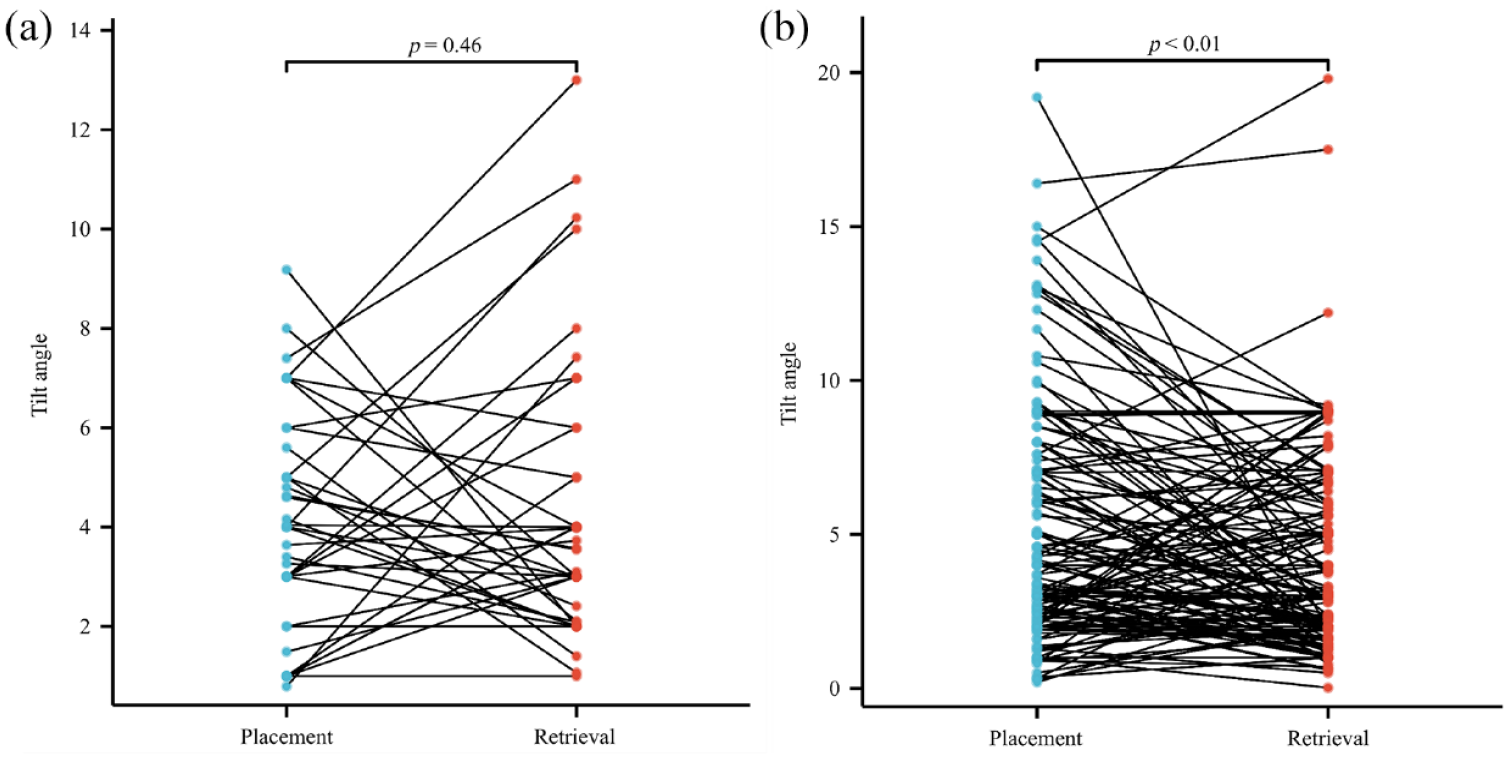
The distributions of filter tilt angle at the time of placement and retrieval for both IJV and FVs access groups. (a) In the IJV group, there was no statistically significant difference between filter tilt angles at the time of placement and retrieval (p = 0.46) and (b) FVs access was associated with a higher difference between placement and retrieval filter tilt angles (p < 0.01).
Possible risk factors for increased IVC filter tilt angle at the time of retrieval
A total of 69 (40.4%) patients experienced increased filter tilt angles, and 102 (59.6%) suffered from decreased filter tilt angles at the time of retrieval when compared with placement. Except thrombus limbs, the remaining baseline demographics, concurrent PE, comorbidities and risk factors, IVC and filter-relevant information, and endo-vascular treatments were not statistically significant (p > 0.05), as shown in Table 3. Following the univariable analysis, the significant variables (p < 0.2) that predicted the probability of increased tilt angle were as follows: thrombus limbs [including left (p = 0.006), right (p = 0.046) and bilateral (p = 0.146)], comorbidities [including hypertension (p = 0.190), cardiologic artery disease (CAD) (p = 0.192), cerebral venous disease (CVD) (p = 0.102)], filter types (p = 0.111), and IVC filter thrombosis (p = 0.127). The multivariate logistic regression analysis showed that hypertension [odds ratio (OR) 0.668; 95% confidence interval (CI) 0.328–1.358, p = 0.265], CAD (OR 0.537; 95% CI 0.136–2.130, p = 0.377), CVD (OR 0.555; 95% CI 0.186–1.651, p = 0.290), filter types (OR 1.624; 95% CI 0.851–3.096, p = 0.141), and IVC filter thrombosis (OR 1.634; 95% CI 0.804–3.323, p = 0.175) were not associated with increased filter tilt angle. Right side lower (OR 0.434; 95% CI 0.202–0.930, p = 0.032) or bilateral LEDVT (OR 0.383; 95% CI 0.14 8–0.995, p = 0.049) were identified as protective factors for increased IVC filter tilt angle, as presented in Table 4.
Baseline demographics, thrombus characteristics, concurrent PE, comorbidities and risk factors, IVC and filter-related information, endovascular treatments for patients who received IVC filters for patients with increased/decreased tilt angle.

Continuous data are presented as the means ± SDs; categorical data are given as the counts (percentage).
Fisher exact.
BMI, body mass index; CAD, cardiologic artery disease; CVD, cerebral vascular disease; FVs, femoral veins; IDDVT, isolated distal deep vein thrombosis; IJV, internal jugular vein; IVC, inferior vena cava; LEDVT, lower extremity deep vein thrombosis; PAT, percutaneous aspiration; PE, pulmonary embolism; PTA, percutaneous angioplasty; PTS, percutaneous stents; SD, standard deviation; VTE, venous thromboembolism.
Multivariate regression analysis of risk factors for increased filter tilt angle after placement in LEDVT patients.

CAD, cardiologic artery disease; CI, confidence interval; CVD, cerebral vascular disease; IVC, inferior vena cava; LEDVT, lower extremity deep vein thrombosis; OR, odds ratio.
Discussion
The increased use of IVC filter has been accompanied by a rise in the number of filter-related complications.2–4 The risk factors for IVC filter tilt tend to be multifaceted, with vascular access being recognized as a considerable risk. Ideally, the filter should be inserted without any filter tilt.6,11 However, the changes in IVC filter tilt during the time of placement and retrieval, as well as the factors for increased filter tilt, have not been fully elucidated. In this retrospective cohort study, using data from a multi-center RCT, we compared the IVC filter tilt degree and change according to the vascular access of IJV and FVs. Our findings demonstrated that an IVC filter approach via the FVs was associated with a statistically significant frequency in tilt angle over 10° at the time of immediate placement compared with the IJV approach. However, FVs access underwent a significant overall tilt change than IJV at the time of retrieval, and IJV had a slightly higher prevalence of tilt angle over 10° compared to FVs access. The distributions of IVC filter tilt angles tend to be paralleled finally. A logistic regression analysis based on baseline demographics, thrombus characteristics, concurrent PE, comorbidities, risk factors for LEDVT, IVC and filter-relevant information, and con-junctive endovascular treatments was performed between patients who underwent increased and decreased tilt angles to investigate the relevant risk factors, indicating that compared with left side LEDVT, right side (OR 0.434; 95% CI 0.202–0.930, p = 0.032) or bilateral LEDVT (OR 0.383; 95% CI 0.148–0.995, p = 0.049) were identified as protective factors for developing an increased IVC filter tilt angle.
Although the relationship between vascular access and filter tilt has been previously documented,6,7,12 the interactions of vascular access on IVC filter placement remain controversial. In a retrospective cohort study of 78 patients, Choi et al. 6 reported no significant difference in filter tilt between the vascular access of IJVs and FVs. In a larger study that included 13003 patients evaluating the association between IJVs and FVs access, Grullon et al. 7 demonstrated that the IJV approach might allow for more precise placement and less tilt. Our present study results are consistent with the findings by Grullon et al. 7 ; patients who underwent IJV approach had a lower likelihood of tilt angle over 10° compared to FVs at the time of placement, which was likely attributable to potential differences in the anatomy of the IJVs and FVs accesses. Anatomically, the IJV access provides a straighter approach to the IVC than FVs, which transition to the iliac veins, enabling the deployment of the filter with a smaller angle between the IVC and the delivery sheath.6,8,13 In addition, when placing a filter via the IJV access, a small pull force was spontaneously created as the distal tiny hooks in the legs were first introduced and trapped or hooked in the IVC wall. However, when using the FVs access, the filter head was released first, and the hooks were not entirely hooked within the IVC wall. Hence, the tilt angles changed over time as the abdominal pressure changed during the retrieval procedure. Noteworthy, prior studies6,7 mainly focused on IVC filter tilt over 20° at the time of placement, and the significance of filter tilt during the time of placement and retrieval is not as well studied. In our study, we used a multi-center RCT database to quantify angle distributions with 0°–5°, 5°–10°, 10°–15°, and >15° to investigate the transition of IVC filter tilt at the time of placement and retrieval, which seemed that the tendency observed at placement continued through the time of retrieval.
Interestingly, this study found that patients who underwent filter placement via IJV had a slightly higher likelihood of tilt angle over 10° than those via FVs at the time of retrieval, although the final angle distributions were not significantly different. IVC filter tilt may occur due to various factors, such as operator error, differential IVC axial morphology, or specific types of filters.5,6 As mentioned in our previous study, 8 the Octoparms and Celect filters showed similar efficacy and safety in preventing PE and had lower filter tilt. The IVC axial morphology and proportion of filter types did not differ between the two groups in this study. The potential explanation for this tendency is not clearly understood, but it is hypothesized that both filters used may have self-adjusting and self-centering capacities. Moreover, the present study further evaluated potential risk factors for patients with increased or decreased filter angle. Multivariant logistic regression analysis revealed that compared to left side LEDVT, right side or bilateral LEDVT tend to be protective factors for developing an increased IVC filter tilt angle. As proposed by Goldman et al., 8 obesity may trigger IVC filter tilt through the compression of the IVC and increased abdominal IVC pressures. This interpretation seems to be in line with the findings that right side or bilateral LEDVT could reduce the incidence of increased filter tilt angle from a hemodynamic perspective. It is assumed that blood flow in the bilateral or right limb is greater than that in the left limb, mainly attributed to the nature barrier of Cockett syndrome, which means that thrombi could reduce the influence of blood flow on the IVC filters. However, the underlying pathogenesis for developing increased filter tilt angle has not been well elucidated, and these hypotheses are speculative. Further studies are needed to confirm these assumptions and provide a better understanding of the factors influencing IVC filter tilt angle changes.
BMI has been identified as a significant factor that influences the formation of IVC filter tilt. Goldman et al. 8 used the Vascular Quality Initiative 2 registry database to examine the effects of extreme obesity on filter placement outcomes and revealed that morbidity of increased tilt correlated with a BMI > 40/kg/m2. Similarly, Grullon et al. 7 found that BMI demonstrated a statistically significant contribution to filter tilt. However, this study was conducted in a Chinese population, where the mean BMI is generally lower than that of Europeans. Therefore, we used a standard criterion from the Working Group on Obesity in China, defining obesity as a BMI of 28 kg/m2 or higher. No significant differences were found between the IJV and FVs access or between the increased and decreased filter tilt angle population in this study. Although no differences were identified, the rate of BMI in patients with FVs access was poorly represented, and the results should be interpreted with caution. Further research in the Asian population is needed to confirm these findings and better understand the role of BMI in IVC filter tilt in diverse populations.
Conjunctive endovascular strategies could also be a factor for potential IVC filter tilt. 14 Park et al. 15 demonstrated that implementing the original push wire technique through FVs approach led to a significantly increased incidence of IVC filter tilt. In contrast, employing a bent stiff wire via IJV access resulted in a higher prevalence of filter tilt. These findings highlight the importance of considering the interrelationship between distinct techniques and vascular access, as they can significantly impact the propensity for filter tilt occurrences. In the present study, PAT, PTA, and PTS techniques were all analyzed, but there were not enough cases to show a significant difference in terms of filter tilt at the time of placement and retrieval, as well as the increased IVC filter tilt. This factor may be worth studying in the future with large sample sizes to better understand the impact of various endovascular strategies on filter tilt.
The present study has several important limitations that merit discussion. First, along with all retrospective analysis of a multicenter database, this study is subject to inherent limitations of reporting bias and inability to obtain certain case specifics. Additionally, the RCT database used was not initially designed to investigate filter tilt, we substituted filter tilt angles of 0°–5°, 5°–10°, 10°–15°, and >15° for a definition of tilt as angle over 20°, it is our hope that detailed tilt angle classifications will help promote the understanding of the implications of vascular access. Second, the present study only assessed the lateral filter tilt and not the anteroposterior tilt, it included only Octoparms and Celect filters, so extrapolation to other conical and non-conical filters is unclear. Third, the dwelling time of IVC filters, ranging from 4 to 190 days, was empirical and may affect the findings. Fourth, there was missing data on BMI for patients from one of the centers. Although the study showed no difference, further studies would be helpful to confirm the results. Fifth, this was a retrospective study using data from an RCT with controlled variables to assess filter tilt, but the sample size was relatively small for assessment; many risk factors described in literatures potentially related to filter tilt had very low event rates; thus, findings could not be statistically compared. In the future, studies with larger sample sizes that include more factors and exclude confounding factors are needed to overcome these limitations and provide a more comprehensive understanding of IVC filter tilt and its associated risk factors.
Conclusion
The incidence of IVC filter tilt angle over 10° at the time of placement could be limited by using the IJV access, while FVs access was associated with a higher difference between placement and retrieval tilt angles. Compared to left side LEDVT, right side or bilateral LEDVT were identified as protective factors against increased IVC filter tilt angle. Future study with a larger sample size and a randomized, controlled trial is needed to confirm the findings.
Footnotes
Acknowledgements
Thanks to all the investigators from 10 centers in the mainland of China who participated and executed the trial: Wanyin Shi, Liang Chen, Wensheng Lou, Guoping Chen, Jinhua Song, Haobo Su, Yumei Xiang, Yan Li, Tao Wang (Nanjing First Hospital, Nanjing Medical Univesity); Jianlong Liu, Xuan Tian, Wei Jia, Peng Jiang, Zhiyuan Chen, Yunxin Zhang, Chenyang Tian, Jinyong Li, Ying Zhang (Beijing Jishuitan Hospital); Gaojun Teng, Gang Deng, Yonglin Qin, Zhibin Bai, Guofeng Zhao, Qi Zhang, Youhua Xue, Lan Gao, Yahong Huang, Zhiping Shen, Sen Lin, Shuguang Zhao, Yue Yang, Yunfang Wang (Zhongda Hospital, Southeast University); Caifang Ni, Yonghai Jin, Pengfei Duan, Baorui Fan, Chao Yang, Lingfang Sun, Qian Ye (The First Affiliated Hospital of Soochow University); Hao Xu, Qingqiao Zhang, Hongtao Liu, Ning Wei, Zhikang Gao, Wenliang Wang, Bin Shen, Duntao Lv, Jing Yang, Yanan Liu, Buqiang Zhuang, Yan Li, Yanfeng Cui, Jinchang Xiao, Xun Wang (The Affiliated Hospital of Xuzhou Medical University); Zhen Li, Hui Cao, Zhouyang Jiao, Shirui Liu, Peng Xu, Zhaohui Hua, Mingxing Li, Zhiwei Wang (The First Affiliated Hospital of Zhengzhou University); Shuiting Zhai, Kun Li, Mingzhe Cui, Kai Liang, Xiaoming Fu, Weixiao Li, Rutao Xu, Dongbin Zhang (Henan Provincial People’s Hospital); Yanrong Zhang, Xiangdong Liu, Haitao Li, Yunsong Li, Liang Li, Jianing Zhao, Xianchao Zhang, Yujie Zhang, Liyuan Liu (The Third Hospital of Hebei Medical University); Hua Xiang, Lin Sun, Ding Li, Peng Yan, Qing Wang, Zhiyong Fang, Xin Xie, Yan Xiao, Shang Ouyang (Hunan Provincial People’s Hospital); Weizhu Yang, Hang Xie, Leye Yan, Zhen Chi, Kun Ke, Junqing Lin, Ning Huang, Na Jiang, Hui Zheng, Xin Lin (Fujian Medical University Union Hospital).