
Abstract
Exhaled nitric oxide (NO) production, upregulated by inflammatory cytokines and mediators in central and peripheral airways, can be easily and non-invasively detected in exhaled air in asthma and other respiratory conditions as a promising tool for disease monitoring. The American Thoracic Society and European Respiratory Society released recommendations that standardize the measurement of the fractional exhaled NO (FeNO). In asthma, increased FeNO reflects eosinophilic-mediated inflammatory pathways and, as a biomarker of T2 inflammation can be used to identify asthma T2 phenotype. In this setting its measurement has shown to be an important tool especially in the diagnostic process, in the assessment and evaluation of poor adherence or predicting positive response to inhaled corticosteroids treatment, in phenotyping severe asthma patients and as a biomarker to predict the response to biologic treatments. The discovery of the role of NO in the pathogenesis of different diseases affecting the airways and the possibility to estimate the predominant site of increased NO production has provided new insight on its regulatory role in the airways, making it suitable for a potential extended use in clinical practice for different pulmonary diseases, even though its role remains less clear than in asthma. Monitoring FeNO in pulmonary obstructive lung diseases including chronic bronchitis and emphysema, interstitial lung diseases, obstructive sleep apnea and other pulmonary diseases is still under debate but has opened up a window to the role NO may play in the management of these diseases. The use of FeNO is reliable, cost effective and recommendable in both adults and children, and should be implemented in the management of patients with asthma and other respiratory conditions.
Keywords
Introduction
Endogenous nitric oxide (NO) is a gaseous molecule produced by residential and inflammatory cells in both large and peripheral airways playing an important role in regulating airway and vascular function. It is produced by three isoforms of NO synthases: neuronal nitric oxide synthase (NOS) (nNOS, NOS1), endothelial NOS (eNOS, NOS3), and inducible NOS (iNOS, NOS2) with different expression and pathophysiologic roles in the airways. The presence of NO in exhaled air was first described in 1991 by Gustafsson et al. 1 and, in 1992 NO was voted molecule of the year by the scientific journal Science. 2 Subsequently, researchers from the Karolinska Institute in Sweden (1993) were the first to report increased fractional exhaled NO (FeNO) levels in asthmatics by induced cell types during an inflammatory response. 3 This was soon followed by a number of publications reporting high FeNO in subjects with asthma. 4 Since then, a large amount of evidences has confirmed a role of endogenous NO as responsible for the physiological regulation of airways, thus its possible involvement in many pulmonary conditions. Moreover, the in-depth study of different inflammatory pathways and the development of techniques to detect FeNO using different flows offers the possibility to estimate the predominant site of increased FeNO production, making it suitable for a potential extended use in the clinical management of many conditions even though its role remains less established than in asthma. The identification and monitoring of biomarkers like FeNO in obstructive lung diseases including chronic bronchitis and emphysema, interstitial lung diseases (ILDs), obstructive sleep apnea (OSA) and other respiratory conditions might reflect the disease state and be helpful in understanding the underlying pathology though its role is still controversial and under debate. The aim of this narrative review is to resume the most important highlights on the usefulness of FeNO as a consolidated tool for assessment and management of bronchial asthma and to provide new insight about the role of FeNO in the regulation of the airways in different respiratory diseases including chronic obstructive pulmonary disease (COPD) and emphysema, ILDs, OSA and other pulmonary diseases to open up a window on its potential contribution as a surrogate biomarker of inflammation and as a method to detect disease activity, useful in the clinical management of these diseases. The use of FeNO is reliable, recommendable and cost effective in both adults and children, and should be implemented and encouraged when used in the diagnosis and management of patients with asthma and other respiratory conditions as shown in Figure 1.

Main respiratory diseases in which fractional exhaled nitric oxide assessment may have a potential role.
Exhaled NO assessment
The gold standard technique for the detection of FeNO uses a chemiluminescence reaction. The reaction between the NO in the breath sample and ozone determines the emission of electromagnetic radiation having wavelength between 600 and 3000 μm which, detected and amplified, provide a proportional signal of the concentration of NO. 5 The chemiluminescence equipment needs an external, highly sensitive source of NO to generate ozone, with detection thresholds of parts per billion (1:109 ppb) and a fast response time (0.5–0.7 s). 6 The chemiluminescence FeNO analyzers currently on the market are NOA 280i (Sievers, GE Analytical Instruments), Logan model LR2149 (Logan Research), NIOX (Circassia), and CLD 88 (Eco Medics).An electrochemical sensor is able to convert NO concentration into an electrical signal, in the presence of a buffer system and a catalytic sensor. A subsequent chemical reaction induces a quantifiable physical change in the sample directly proportional to the concentration of NO. Among electrochemical or infrared sensor devices commercially available there are: NIOX VERO (Circassia), Medisoft (Hypair), NObreath (Bedfont Scientific), and Vivatmo-PRO (Bosch). The NIOX VERO is portable, usable in both adults and children with a sensor to be replaced after 100–300 measurements. Patients should exhale for at least 10 s at a pressure ensuring a flow rate of 50 ± 5 ml/s. An electrochemical sensor evaluates the final 3 s of exhalation and subsequently express the result in a range of 5–300 ppb. NObreath requires 12 s of exhalation in adults and 10 in children. 6 The Medisoft device is semi-portable and can offer either off-line and on-line measurements, in a range of 0–600 ppb. The ‘Off-line’ measurement involves the analysis of a previously collected gas sample, while the ‘on-line’ one collects gas sample in real time. Recent research has shown a good correlation between some of these devices although FeNO absolute values may show clinically relevant differences. 7 Recently, a comparison between FeNO levels measured by different portable analyzers produced by different manufacturers was published. FeNO levels obtained using the NIOX MINO® and NObreath® were more variable than those measured using the NA623NP®. There were strong positive correlations in FeNO levels measured by the NA623NP®, NIOX MINO®, and NObreath® (p < 0.001). No significant differences were observed in FeNO levels obtained using the NIOX MINO® and NIOX VERO®. 8 The authors concluded that globally it seems that there may be significant differences in the FeNO measurements carried out with different instruments especially if from different manufacturers; this must be kept in mind in clinical practice and in the evaluation of studies especially in relation to the normal cut-offs considered. Optical sensors consisting of a laser light source that reacts with sample gas, a collection cell, and a sensing system that records signals in the mid-infrared absorption band (5.1–5.7 μm) have been developed. 9
Exhaled NO measurement
Standardized procedures for measuring FeNO concentration were approved by the American Thoracic Society (ATS) and the European Respiratory Society (ERS). 10 The document was recently integrated by adding the evaluation of nasal NO measurement and introducing recommendations for NO dynamic models as extended NO analysis has been developed.11,12 According to the guidelines, FeNO measurement in adults occurs instantaneously during an expiratory maneuver. The subject should inhale to total lung capacity with purified air to limit contamination of the sample with potentially high NO levels in the surrounding environment. Then exhalation should be performed for 10 s at a pressure of 5–20 cmH2O, which ensures the closing of the soft palate to reduce the potential contamination from higher airways and paranasal sinuses. 13 An exhalation is considered adequate if a stable concentration level (plateau) is reached at a flow rate of 50 ml/s. An expiratory flow of 50 ml/s is recommended, considering that the region of interest of NO production is the lower respiratory tract. The plateau values, corresponding at the expiratory flow rate, vary considerably with the flow rate due to the diffusion of the NO into airways and transit time. For this reason, low speeds (<10 ml/s) result in higher levels. The measurement of FeNO at a single expiratory flow does not allow the identification of the site of NO production in the respiratory system. Therefore, mathematical models have been developed, extensively revised, 14 to calculate the production of pulmonary NO. The fractions of NO produced in the airway walls and alveolar region [concentration of alveolar nitric oxide (CANO)] can be calculated at different high flows. In addition, the association of mathematical calculations with NO measurements at high and low air flows can provide values of the concentration of the gas released by the air conduction system and the capacity of diffusion of NO. There is a possibility to modify expiratory flow rates by resistors in all chemiluminescence analyzers, whereas most electrochemical sensors are not suitable for the analysis of multiple streams except for Medisoft. The two-compartment model allowing the evaluation of NO dynamics in central and in more distal airways with mathematical models to calculate bronchial and alveolar NO parameters measuring NO at different exhalation flows seems to be theoretically plausible, even though, the feasibility to exhale at low flows in patients with obstructive lung diseases such as COPD or severe asthma may be limited. To address this issue, recent research proposed a suitable protocol for extended NO analysis to calculate CANO with a linear model obtained with elevated expiratory high flow rates in patients with asthma of differing severity including severe phenotypes. 15
Interpretation of FeNO measurement results
In clinical practice a FeNO value <25 ppb (<20 ppb in children) is considered normal, while values between 25 and 50 ppb (20 and 35 ppb in children) should be interpreted in the clinical context. Reference values for FeNO have been defined for healthy adults, older aging people and children.16–19 The upper limit of FeNO50 for healthy individuals, confirmed by a very large survey by the National Health and Nutrition Examination Survey, reported the fifth to 95th percentile values of FeNO being 3.5–39 ppb for subjects 12–80 years of age. 20 A recent review reported different studies in which the application of multiple regression modeling reported normal values of FeNO in never-smoking adults, ranging from 24 to 53 ppb. The data showed, in an unselected population, a distribution of FeNO skewed to the right, therefore the authors concluded that it is unlikely that reference values derived from a ‘normal’ population will be as helpful as cut points in patients with airway disease or respiratory symptoms. 21 FeNO values may be influenced by several conditions related to the patients like genetics, sex, height and weight, use of medications (corticosteroids, ACE-inhibitors), atopy, diet and smoking habits.22,23 Some foods are known to be capable of influencing FeNO values, with some enhancing, while others lowering FeNO. Nitrate-rich foods, especially leafy vegetables such as lettuce, spinach and kale, can increase FeNO.24,25 Chronic alcohol consumption and recent consumption of coffee were both related with lowering of FeNO values.26,27 Moreover, NO is produced by NOS, and alterations in NOS activity or expression may contribute to the pathophysiology of asthma. Genetic variations in NOS genes have been suggested as a potential contributor to altered NO production and airway inflammation in asthma patients. A large meta-analysis in 2023 28 concluded that several polymorph NOS gene variants appear to have influence on asthma prevalence or outcomes. However, current evidence is still affected by too many different factors such as ethnicity, study designs and disease variants to drive clear conclusions. The relationship between NOS gene mutations and FeNO levels is complex and may be influenced by other factors such as age, sex, and disease severity. Further research is needed to fully understand the relationship between NOS gene mutations and FeNO levels in patients with respiratory diseases. For these reasons, to avoid any analytic interference, it is strongly recommended to perform FeNO measurement before spirometric maneuvers and before consuming any food, beverage or cigarette smoking. The latter, in particular is one of the most important determinants of FeNO levels. Current smokers show lower levels of FeNO when compared to ex-smokers or non-smokers 29 and different mechanisms have been suggested such as a mechanism of downregulation of NO synthetase by NO from cigarette smoke, increased breakdown of NO or lack of tetrahydrobiopterin. 30 Also, viral respiratory infections can influence FeNO values 31 as represented in Table 1.
Factors influencing FeNO production.
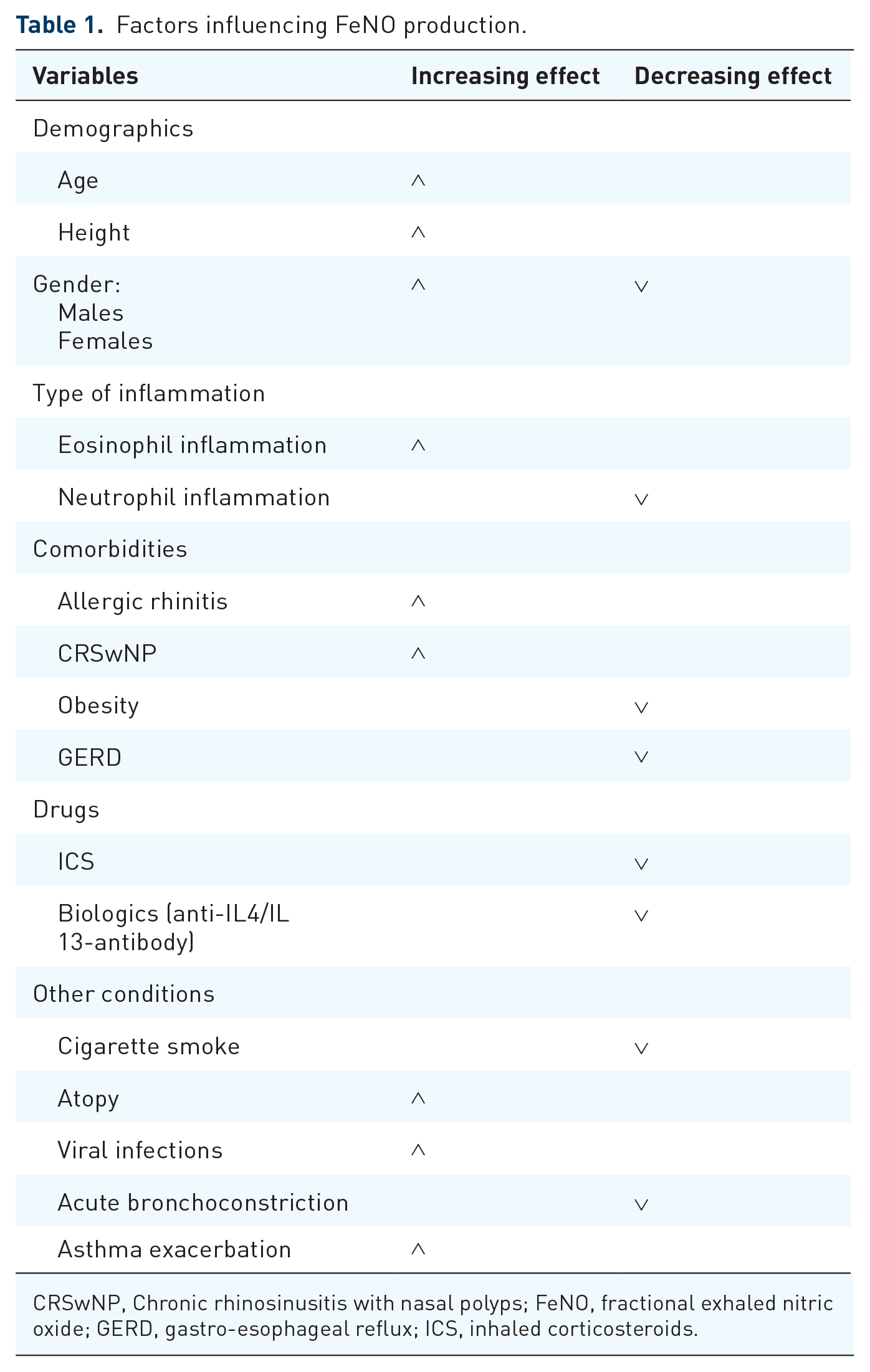
CRSwNP, Chronic rhinosinusitis with nasal polyps; FeNO, fractional exhaled nitric oxide; GERD, gastro-esophageal reflux; ICS, inhaled corticosteroids.
Main clinical applications of FeNO: State of art
Asthma
Asthma diagnosis
High FeNO values in patients with relevant symptoms and in combination with other diagnostic options may help in confirming the diagnosis of asthma and, National Institute of Clinical Excellence (NICE) and ERS guidelines recommend supplementing the asthma diagnostic algorithm with FeNO testing in combination with lung function assessment.32,33 According to current literature, increased FeNO levels (cut-off of 40 ppb in adults and 35 ppb in children) are associated with a higher probability of asthma diagnosis, while in range values do not exclude asthma. 31 In a study conducted by Karrasch et al., 34 high FeNO levels showed higher specificity than sensitivity and a positive predictive value for asthma, being an important tool in ruling in asthma diagnosis. Although disease prevalence in the population is known to influence the predictive value of the test, the cited study, analyzed populations with widely differing asthma prevalence (9–80%) and found no significant differences in the accuracy of FeNO to diagnosing asthma. FeNO measurement may also be used as a rule-in test for detecting Cough-Variant Asthma (CVA) in adult patients with chronic cough35,36 and may be useful to predict bronchial hyperactivity in young adults with CVA being an alternative to the use of bronchial provocation tests which can be time-consuming and expensive 37 (Table 2).
Reference values and clinical interpretation of FeNO in asthma diagnosis and treatment.
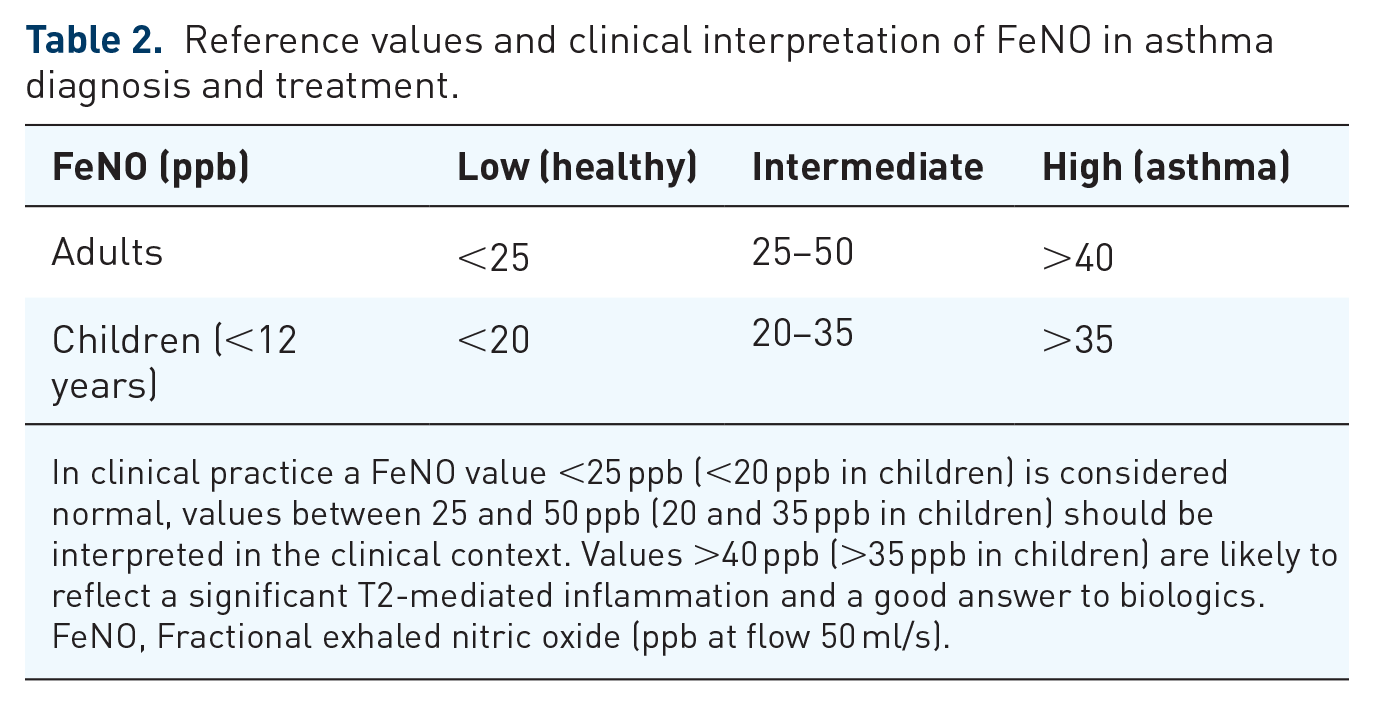
In clinical practice a FeNO value <25 ppb (<20 ppb in children) is considered normal, values between 25 and 50 ppb (20 and 35 ppb in children) should be interpreted in the clinical context. Values >40 ppb (>35 ppb in children) are likely to reflect a significant T2-mediated inflammation and a good answer to biologics.
FeNO, Fractional exhaled nitric oxide (ppb at flow 50 ml/s).
Asthma control, response to treatments and adherence
Being a T2-mediated biomarker 38 related to airway eosinophilic inflammation FeNO was investigated as a promising marker able to predict asthma exacerbations and poor asthma control.39,40 Moreover, its rapid reduction after anti-inflammatory treatment makes it a suitable tool to predict therapeutic efficacy of treatments. Many studies had previously investigated these aspects but, actually, a recent meta-analysis concluded that the correlation between FeNO levels and asthma control is weak. 41 These results may be partly explained by clinical characteristics of the patients: FeNO levels correlates with asthma control only in patients not regularly treated with ICS; 42 moreover sino-nasal comorbidities frequently correlated with asthma may influence FeNO levels independently. 43 Some asthma phenotypes are characterized by eosinophilic inflammation (T2 phenotypes) which are sensitive to glucocorticoids; in these patients FeNO (directly related to eosinophilic inflammation) has been reported to be an ideal tool in monitoring the clinical response to inhaled or systemic corticosteroid treatments especially in steroid-naïve patients, with high levels of FeNO associated with a good response to treatment.40,44 Moreover, elevated high FeNO levels before starting ICS treatment may predict improvements in lung function either in adults and children, 45 reduction of symptoms 46 and a better quality of life. 47 FeNO assessment has also been proposed for therapeutic strategies based on personalized treatment regimen according to FeNO levels44,48,49 (combined impact of exhaled nitric oxide) due to the rapid response to anti-inflammatory treatments together with a rapid increase in case of worsening of asthma control and exacerbations.39,50 A meta-analysis including data from three Cochrane reviews51,52 concluded that a strategy based on FeNO levels for tailoring asthma therapy resulted in significant attenuation of exacerbations in adults and children when compared to a guideline-based strategy, without increasing ICS dose. 44 FeNO has also been examined as a tool for the identification of non-adherence to treatment, helping to distinguish ‘difficult to treat’ versus actual severe asthma patients. Patients not adhering to treatment tend to have high FeNO values53–58 and therefore like all other asthmatics who do not respond to therapy, would undergo to the so-called ‘FeNO suppression test’. 59 Globally, recent evidence-based recommendations suggest that FeNO testing is indicated to optimize asthma treatment, in particular to control exacerbations and titrating ICS therapy and should be introduced in the management of asthma, from diagnosis to follow-up 60 as summarized in Figure 2. Overall, literature evidence underlines FeNO utility in the diagnosis of asthma, prediction of ICS response and evaluation of the risk of exacerbation/loss of control and lung function impairment, although the clinical use of a single biomarker in asthma has to be carefully weighted according to the goals it is demonstrated to satisfy in clinical trials and real-life experiences. Moreover, several factors may influence the measure of FeNO as mentioned before (the variability over time, corticosteroids intake, comorbidities, environmental exposure or habits). Among positive aspects FeNO has been shown to be easy-to-measure, reliable and cost-effective, useful both in adults and children. Therefore, the use of FeNO in combination with other diagnostic tests and biomarkers is highly suggested to increase the specificity of the outcomes and, as an integrated tool, may be useful for routine clinical practice (Figure 3).
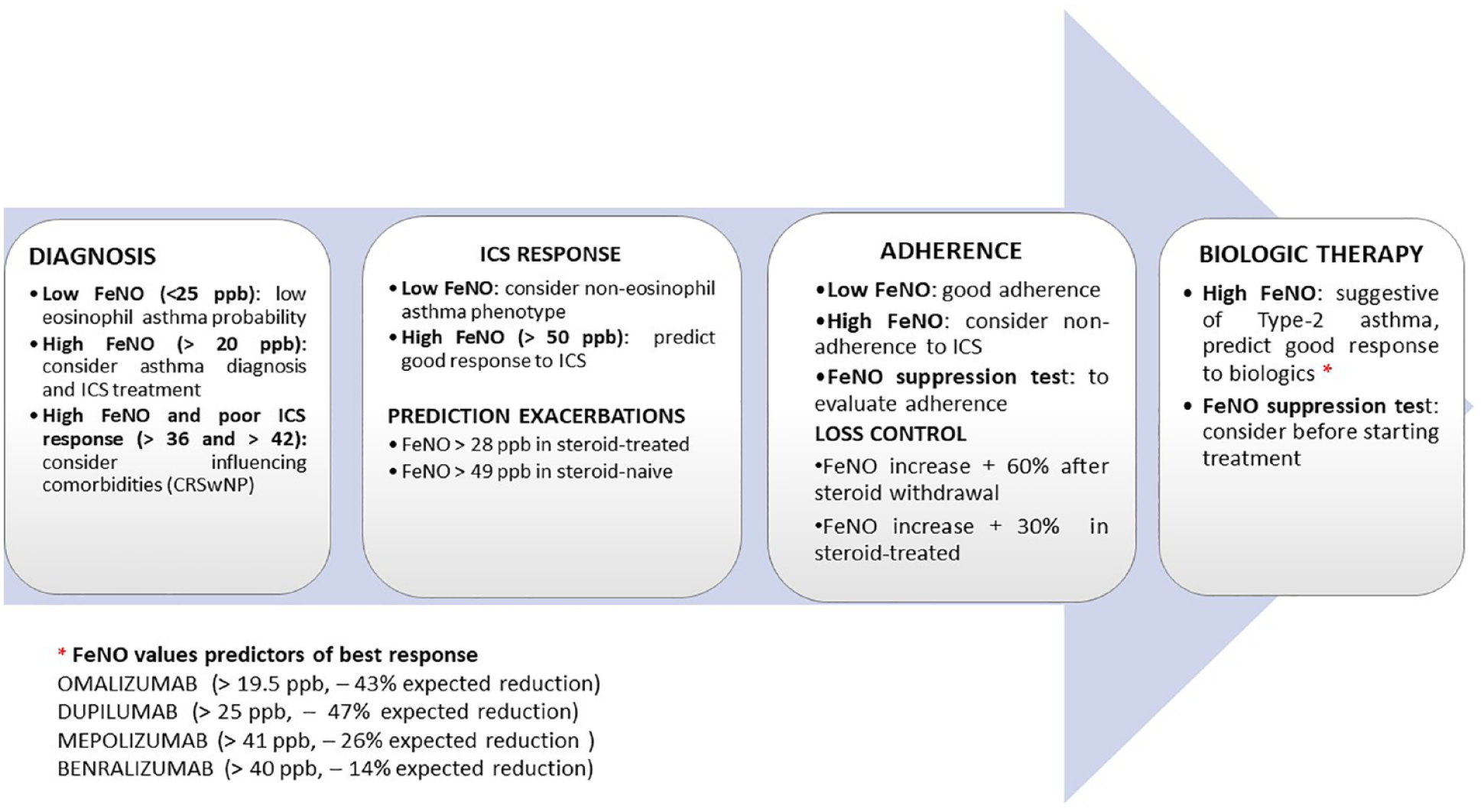
Usefulness of fractional exhaled nitric oxide measurement in the management of asthma and severe asthma.

Flow diagram of treatment decisions based on fractional exhaled nitric oxide measurement at initial evaluation of patients with suspected asthma.
Severe asthma
Severe asthma is defined by the ATS/ERS guidelines on the basis of the treatment needed to achieve asthma control. Recent studies have shown the association of severe asthma with the degree of eosinophilic inflammation 61 and with an increased expression of iNOS which is the major player responsible for the production of FeNO. iNOS expression is mediated by IL-13, one of the most important inflammatory cytokines involved in TH2 inflammatory response. The utility of FeNO measurement in the management of severe asthma is still debated, especially in light of the ICS inhibitor action on iNOS. However, a recent study reported elevated FeNO levels in 50% of severe steroid-dependent asthmatics. Moreover, high concentrations of FeNO and eosinophils in blood and sputum that characterize severe late-onset asthma, predominantly non-atopic, were found to be associated with the severity of asthma. Further research has shown that, in severe asthmatics, elevated FeNO values correlated with increased airway reactivity, increased sputum eosinophilia, atopy, hyperventilation, reduced perception of symptoms, increased airflow obstruction, more pronounced air-trapping and higher emergency room visits. 62 All this evidence suggests that FeNO is a reliable biomarker for identifying patients with severe asthma. According to the Global Initiative for Asthma (GINA) guidelines, to evaluate the asthma phenotype a FeNO ⩾ 20 ppb is considered the cut-off for Type 2 inflammation in severe asthma and may be used together with blood (⩾300 cells/μl) and sputum (⩾3%) eosinophil count. Reference values may be used as general guidance, taking into account that they may be subject to change significantly in patients. FeNO values >50 ppb (>35 ppb in children) are associated with eosinophilic inflammation of the airways and may predict response to anti-inflammatory therapy or a loss of control of the disease 39 suggesting the opportunity for treatment with ICS. Instead, a FeNO < 25 ppb (<20 ppb in children) is correlated with lower eosinophilic inflammation and corticosteroid response. Measures >30 ppb have been associated with uncontrolled asthma, while a value between 16 and 25 ppb defines the smallest clinically significant difference (an increase of up to 60% in baseline). During an exacerbation, FeNO can increase by more than 50% and up to 150 ppb following exposure to an allergen or acute infection. FeNO in association with patients’ symptoms monitoring may aid clinicians in gradually decreasing oral corticosteroids (OCS) dose in case of good responses to Type-2 targeted therapy, though the ERS/ATS guidelines suggest that FeNO should be avoided in guiding OCS-therapy in adults with severe asthma. 63 More recently, FeNO, being a biomarker of T2 inflammation, has been proposed as a predictor of response/efficacy to treatment with biological agents.64–67 In particular, FeNO ⩾ 25 ppb, together with eosinophilic counts ⩾150 cells/μl, is predictive of therapeutic efficacy of Dupilumab (an IL-4/IL-13 antagonist) in severe asthmatics on high doses of ICS.68,69 Also, treatment with Tezepelumab, a humanized antibody targeting thymic stromal lymphopoietin, which acts in an upstream position in the inflammatory cascade and modulating both the Th1 and TH2 pathways, has demonstrated persistent reductions in FeNO levels and blood eosinophil count 70 which promises to be a therapeutic strategy in severe uncontrolled asthma patients irrespective of the asthma T2 phenotype.71,72 It is important to underline that FeNO levels are primarily controlled by IL-13-induced upregulation of NOS in the airway epithelium; for this reason, FeNO seems not to be a reliable prediction marker for the efficacy of Mepolizumab and Benralizumab.73,74 In the DREAM study FeNO failed to show a pharmacodynamic response during Mepolizumab treatment and did not demonstrate as a predictive biomarker for reductions in exacerbation rates. 75 This suggests that FeNO is not responsive to modulation through the IL-5 pathway and is potentially more relevant to different aspects of the T2 inflammatory response (IL-13). However, a small study on Benralizumab in real life found that the responder could be predicted by FeNO at 40 ppb in Type 2 asthma. 76 Recently, an Italian Consensus paper supported the use of FeNO in the diagnosis and management of asthma and severe asthma and to titrate treatment with ICS and biologics. 13 Globally, the current evidence suggests FeNO as a reliable biomarker in the identification of asthmatic patients with a more severe behavior, though the heterogeneity of the disease needs an integration of different tools to completely characterize specific phenotypes.
Non-asthmatic eosinophilic bronchitis
Non-asthmatic eosinophilic bronchitis (NAEB) is characterized by chronic dry cough, sputum eosinophilia and good response to glucocorticoids similarly to bronchial asthma. However, in contrast to asthma, NAEB presents no airflow obstruction and airway hyperresponsiveness. It has been hypothesized that the difference of inflammatory cells location, inflammatory mediators and airway remodeling might result in pathogenesis of NAEB and asthma. Compared with asthmatics, in fact, inflammatory cells mainly infiltrate bronchial mucosa in subjects with NAEB thus explaining the absence of airway hyperresponsiveness, as less inflammatory mediators exert their action on smooth muscle. 77 Some reports indicate that, in patients with NAEB, FeNO levels are significantly elevated when compared to those of patients with other causes of chronic cough. 78 According to a meta-analysis, FeNO seems to be less precise in predicting NAEB in non-asthmatic patients with chronic cough. However, the same study highlighted the reliability of FeNO values between 30 and 40 ppb in identifying asthmatics with chronic cough responsive to corticosteroids, hence implying not to neglect the clinical utility of FeNO in these patients. 35 A recent systematic review of guidelines and expert panel report on the management of chronic cough due to asthma and non-asthmatic eosinophilic bronchitis (NAEB) in adults and adolescents, suggest that non-invasive measurement of airway inflammation may be useful and the presence of eosinophilic airway inflammation is likely to be associated with a more favorable response to ICS especially in patients with chronic cough due to asthma. 79
COPD and related comorbidities
Fractional exhaled nitric oxide in COPD
The clinical value of FeNO in COPD patients despite its potential benefit as a non-invasive monitoring biomarker of airway inflammation during routine outpatient visits (easy and standardized test, with low intra-subject variability) is still debated with smoking habits, disease severity and ICS use being important factors influencing FeNO levels. According to a previous meta-analysis, COPD induces a slight increase in NO, with higher levels in former smokers than in current smokers; globally no association has been found between the levels of FeNO and COPD flare-ups 80 even though in a recent large prospective observational study of 226 COPD patients, an association was reported between increased FeNO and the risk of COPD exacerbations. 81 Recent evidence underlines that FeNO at a flow of 50 ml/s (FeNO50) is related to sputum eosinophilia in COPD,82,83 and may be considered as a marker of T2 inflammation in the central bronchial airways. Moreover, the persistently elevated FeNO50 in stable COPD has been found to be associated with an increased risk of exacerbations 81 and to predict inhaled and systemic steroid responsiveness in stable and disease exacerbations, respectively.84,85 However, chronic airflow limitation in COPD is the result of either small airway disease and lung parenchyma destruction, 86 which may not be captured by FeNO50. In this setting the extended NO analysis allows the assessment of pulmonary NO dynamics in the central bronchial and more distal airways (small airways and the alveolar/acinar region). 11 A recent, interesting study investigated for the first time the CANO during COPD exacerbations finding an increased CANO in both stable and disease exacerbation, remaining unchanged during convalescence and lung function improvement, while FeNO50 reflecting central airway production was found to be elevated only during exacerbations and suppressed in convalescence. The authors also found that CANO was correlated with circulating eosinophils suggesting a possible upregulation of iNOS/nNOS activity in distal airways, but not correlated with airflow limitation markers of small airway dysfunction/alveolar integrity. 87 They concluded that CANO and bronchial NO parameters, reflecting nitrative stress at different anatomical sites, can be successfully measured in stable patients with severe airflow limitation and during COPD exacerbation using a feasible extended NO analysis. Moreover, central and peripheral airway NO, is differentially regulated in stable and exacerbated COPD suggesting CANO as a marker for detecting the constantly elevated nitrative stress in distal airways, while bronchial NO to monitor inflammatory activity during an exacerbation. The activity of NOS isoenzymes such as nNOS expression has been previously shown to be linked with the severity of airflow limitation in COPD; 88 therefore modulation of nitrative stress pathways in peripheral airways may be a potential therapeutic goal even though possible clinical application of CANO should be further explored in certain aspects, including its role in predicting disease progression or exacerbation development. Patients with COPD have a predominantly neutrophilic airway inflammation, although new scientific evidence shows that a proportion of COPD patients present with an eosinophilic airway inflammation. In these patients a significant direct correlation between FeNO and blood eosinophil count in stable disease, especially in GOLD E patients with frequent exacerbations was reported. 89 FeNO was also shown, in the same phenotype of patients, to predict response to ICS treatment during stable disease 90 and to systemic corticosteroid treatment in patients suffering an acute exacerbation. 85 In conclusion, in this specific COPD phenotype, FeNO, as eosinophilic surrogate biomarker, may have an important role, being an easier and useful tool to identify those patients who are most likely to benefit from ICS.
FeNO in alpha-1 antitrypsin deficiency
Alpha-1 antitrypsin (AAT) deficiency is a genetic disorder that, in the homozygotic form of the disease, is considered an important risk factor for developing COPD. Severe AAT deficiency (PiZZ: homozigous genotype) is characterized by lower FeNO levels compared to healthy non-smokers and COPD patients, due to the predictable pulmonary function impairment in these patients.91,92 On the other hand, patients with a lower reduction of plasma AAT levels (PiMZ: heterozygous genotype) show increased FeNO levels, and an inverse correlation with plasma AAT levels. 93 In these patients FeNO measurement may be important to monitor the progression of airway inflammation toward possible COPD development. 94
FeNO in pulmonary arterial hypertension and cardiovascular diseases
An altered NO signaling in the pulmonary endothelium due to the decreased expression and dysfunction of eNOS contributes to the increased vascular smooth muscle tone and vascular remodeling, leading to the development and progression of pulmonary arterial hypertension (PAH). NO deficiency of the pulmonary vasculature can be assessed by detecting FeNO, a non-invasive biomarker that may be useful to correlate with changes in pulmonary hemodynamics and predicting therapies response. It has been shown that patients with PAH may have lower,95–98 similar97,99–101 or elevated FeNO levels compared to health 102 and that patients who respond to therapy replacing NO (phosphodiesterase Type 5 inhibitors, prostacyclin and endothelin receptor antagonists, other pharmacological strategies) show higher FeNO levels compared to those who do not, suggesting a role of FeNO in monitoring response to therapy.97,103–107 However, this remains controversial as some studies failed to confirm this correlation.108–111 Several experimental and human studies highlighted the involvement of the reduced endothelial NO signaling in the pulmonary vasculature in PAH patho-mechanisms; however, studies on both bronchial and alveolar NO showed ambiguous results, likely related to unstandardized measurement protocols, low number of patients, different PAH etiologies and confounding analytical and physiological factors. 112 Interestingly, a recent study evaluating the clinical value of FeNO in the diagnosis of PAH in patients with acute exacerbation of COPD (AECOPD) demonstrated that FeNO levels at admission can act as an indicator for PAH diagnosis in AECOPD patients. 113 Additionally, FeNO has been assessed in heart failure with ambivalent outcomes.114–116 In stable ischemic heart disease FeNO was found to be inversely associated with some of risk markers of atherosclerosis (triglycerides and hemoglobin A1c) implying endothelial dysfunction resulting in a decreased production and increased degradation of NO. 117
Interstitial lung diseases
The possibility to obtain multiple-flows assessment of FeNO may provide a reliable measurement of bronchial and alveolar production of NO, supporting its potential value as a biomarker in peripheral lung diseases, such as ILDs. Recent research proposed FeNO as a marker of severity of idiopathic pulmonary fibrosis (IPF) and systemic sclerosis-associated ILD. Patients affected by ILD have been reported to have an elevated high flow FeNO and CANO values compared to healthy controls, indicating a potential role of nitrosative stress in lung fibrosis. The significant difference of CANO levels between idiopathic ILDs and connective tissue disease (CTD)-associated ILD is interesting, and may be proposed as a differential diagnosis tool between the two entities, suggesting that NO is also implicated in lung inflammation associated with rheumatological diseases. 118 A recent systematic review on the assessment of extended FeNO analysis in the management of patients with ILDs (ILDs associated with systemic sclerosis, idiopathic pulmonary fibrosis, granulomatous ILDs, eosinophilic pneumonia) reported that multiple-flow FeNO analysis, and CANO in particular, demonstrated a suggestive potential in discriminating idiopathic ILDs from connective-ILDs, and in estimating survival and disease progression in terms of forced vital capacity (FVC) deterioration, suggesting its possible implementation in the clinical management of IPF due to its reproducibility, repeatability and non-invasive nature. 119
Obstructive sleep apnea
OSA is a sleep disorder characterized by airway and systemic inflammation. Many studies have investigated FeNO patterns in these patients, reporting slightly, but still significantly higher levels of FeNO than healthy controls, especially evident in non-smokers and not consistently related to the severity of the disease.120–122 Obesity, being a risk factor for OSA and, independently, for airway inflammation has been the objective of studies, although, conflicting results were found comparing FeNO values in obese OSA patients with healthy obese subjects.123–125 Some studies investigated alveolar NO reporting lower levels in OSA patients compared to healthy subjects with a significant increase after continuous positive airway pressure (CPAP) treatment,126,127 while other studies found elevated alveolar NO levels in OSA with a positive correlation with the apnea-hypopnea index (AHI), nocturnal desaturation and BMI, linking distal airway inflammation to intermittent hypoxia. No differences were found in bronchial NO. 128 nNO seems to have a greater value than FeNO reflecting upper airway inflammation in OSA patients. 122 Interestingly, CPAP treatment has been shown to reduce/normalize high FeNO values in OSA patients, suggesting its potential role as a biomarker of compliance and response to therapy129,130 although some studies failed to find this correlation. 127 Overall, even though FeNO seems to have a limited screening potential for sleep disordered breathing, 131 a composite index including BMI, age, carboxy-hemoglobin saturation, neck circumference, FEF50/FIF50 and FeNO has shown to be predictive for OSA, 132 hence new investigations are needed to overcome methodological limitations and better characterize airway inflammation and oxidative stress in these patients, which may aid in understanding the complex pathophysiology of OSA. 133
Conclusions and future perspectives
FeNO is an easy-to-measure, reliable and cost-effective marker of T2 airway inflammation recommended in both adults and children, for asthma diagnosis and monitoring, especially in combination with other diagnostic tests and biomarkers and in the appropriate clinical setting, considering its high variability over time. The use of FeNO may be considered for the identification of precise asthmatic phenotypes and for the consequent development of titrating-therapy strategy aimed at the individual. Of note, FeNO is not completely satisfactory in differentiating Type 2 asthma phenotypes, especially in the context of severe asthma choice of biologic therapies. As there is no currently universal shared algorithm for biomarker application in asthma and severe asthma management, an integrated approach including clinical molecular phenotyping is aimed to see if combination of different markers including FeNO can increase diagnostic accuracy and make decisions more reliable in the whole approach of asthma management and in routinely clinical practice, after the advent of personalized medicine.
The possibility to estimate the predominant site and distinguish the bronchial from the distal airways production of increased fraction of exhaled NO, moreover, opens a window in the monitoring of nitrative stress at different anatomical sites within the airways, making it now suitable for a potential extended use also in the management of other respiratory diseases including COPD and ILDs, though its role is still less clear and hence less established than in asthma. In this field, CANO has demonstrated a potential in discriminating idiopathic ILDs from CTD-ILDs and in estimating survival and disease progression in terms of lung function deterioration, suggesting its possible implementation in the clinical management of IPF, also due to its reproducibility, repeatability and noninvasive nature. These promising findings need to be confirmed by larger, prospective and multicenter studies to better investigate the dynamics of FeNO parameters throughout the clinical course of disease and to evaluate the influence on CANO in related comorbidities and during antifibrotic treatment.