
Abstract
Background:
For one of the most chronic medical conditions, osteoarthritis, uncertainties remain on the impact of injury chronology, the role of repeat injury on the incidence/progression of this disease and the need for knee arthroplasty.
Objectives:
To explore, in an older adult population, how nonsurgical knee injuries relate to osteoarthritis incidence/progression and the weight of independent risk factors for arthroplasty.
Design:
A cohort study design evaluates the long-term impact of injuries on knee osteoarthritis outcomes.
Methods:
Knees with no prior injury (n = 6358) and with at least one injury (n = 819) ⩽20 years before study inclusion were from the Osteoarthritis Initiative cohort. Sociodemographic, clinical and structural [X-ray, magnetic resonance imaging (MRI)] data at study inclusion and changes within 96 months were analysed. Statistics included a mixed model for repeated measurements, generalized estimating equations and multivariable Cox regression with covariates.
Results:
At inclusion, knees with prior injury demonstrated greater incidence and severity of osteoarthritis (p ⩽ 0.001). At 96 months, there was a greater increase in symptoms [Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain, p = 0.002], joint space width (JSW, p = 0.039) loss, medial cartilage volume loss (CVL, p ⩽ 0.001) and bone marrow lesion size (BML, p ⩽ 0.049). Knees with/without injury at inclusion but with new ones over time had a pronounced increase in symptoms (all WOMAC scores, p ⩽ 0.001), JSW loss, lateral (without) and medial CVL, lateral (without) and medial meniscal extrusion and medial BML (without; all p ⩽ 0.030). Levels of lateral and medial meniscal extrusion (without) and symptoms (with/without; all WOMAC scores, p ⩽ 0.001) were all accentuated with a repeated new injury. Risk factors associated with the highest knee arthroplasty occurrence are new meniscal extrusion and new injury (p ⩽ 0.001).
Conclusion:
This study highlights the importance of nonsurgical knee injury in older adults as an independent risk factor for knee osteoarthritis and arthroplasty. These data will be beneficial in clinical practice as they will help identify individuals at greater risk of significant disease progression and worst disease outcomes for a customized therapeutic approach.
Keywords
Introduction
Over the years, osteoarthritis, one of the most common chronic medical conditions, has become a major burden from both medical and financial points of view.1,2 Treatments remain mainly symptomatic, and intense research over the last decade has, unfortunately, not made any significant breakthroughs in discovering curative therapies.3–6 In this context, it is logical that efforts should be made to identify risk factors that will impact the incidence and progression of this natural chronic and degenerative disease to improve its outcome. Several cross-sectional and longitudinal studies have explored this subject, sometimes in the context of sports injury in young individuals, 7 while a possible association between a single acute knee injury and the development of osteoarthritis8–10 and even, in some cases, an accelerated form of the disease 11 was described. The meniscal lesions have also been reported to play a significant role in this pathology. 12 Studies in older adults have shown that a previous knee injury is potentially a significant risk factor for unilateral knee osteoarthritis based on symptoms and radiographic changes.13–16
While these studies highlighted the potential role of knee injury in osteoarthritis, many questions remain unanswered, particularly in older adults, where injuries are rarely sport related. The role of the chronological sequence of events over time, the number of injuries in the incidence and progression of osteoarthritis and disease outcomes such as knee arthroplasty have yet to be investigated further. When explored, this was mainly done using X-rays with minimal ability to identify early or new osteoarthritic changes, which remains a critical shortfall. Therefore, studies need to include a more comprehensive imaging exploration to bridge the missing link about how injury and related structural changes can impact osteoarthritis outcomes in a senior population. This could be done using magnetic resonance imaging (MRI), which has been demonstrated to be sensitive and reliable in identifying early (new) structural changes.
This study aimed to provide, in older adults, an in-depth exploration of the role of knee injury in the incidence and progression of the chronic disease, osteoarthritis, over an extended period (within 96 months) from a clinical and joint structural standpoint using both X-rays and MRI. Moreover, the impact of the number of knee injuries on the extent of the disease severity was fully explored. The role of injury on a disease outcome and joint replacement was comprehensively analysed by determining the relative weight of confounding risk factors, particularly at the structural level, which requires a long-term longitudinal evaluation. The Osteoarthritis Initiative (OAI) cohort was used as it provides an extensive and comprehensive longitudinal clinical and structural information data set of osteoarthritic knees. Furthermore, in this cohort, data included a vast amount of information from the years before inclusion, such as previous knee injury, which was documented yearly during the follow-up.
Methods
The reporting of this study conforms to the Strengthening the Reporting of Observation Studies in Epidemiology (STROBE) statement for reports of observational studies. 17
Study design
A cohort study design was used to evaluate the impact of an injury on the long-term incidence and progression of knee osteoarthritis at the clinical, joint structural and disease outcome levels.
Study setting
Knees were from participants of the OAI cohort (https://nda.nih.gov/oai/), a longitudinal database of knee osteoarthritis clinical, radiological and MRI data. Participants (n = 4796) of both sexes and aged 45–79 years were enrolled between February 2004 and May 2006 and followed for up to 108 months. The OAI cohort was divided into Progression (n = 1389), Incidence (n = 3285) and Control (n = 122) subcohorts. In the Progression cohort, participants were characterized as having symptomatic osteoarthritis (defined as frequent knee symptoms and tibiofemoral knee osteoarthritis – Kellgren-Lawrence grades ⩾2) at study inclusion. The Incidence cohort had characteristics that placed them at risk of developing symptomatic knee osteoarthritis, defined as the first occurrence during the study of frequent knee symptoms and definite tibiofemoral osteophytes in the same knee. Of note, no knee from the reference (nonexposed) Control subcohort was included in this analysis.
Written informed consent was obtained from all participants. The OAI study was approved by the Institutional Review Boards at the University of California, San Francisco (OAI Coordinating Center; Approval Number 10-00532). Each of the four clinical sites also approved the study.
Participants
Analyses were made at the knee level (Figure 1). Of the 9348 knees that entered the OAI, 90 were without information on the presence of a prior injury and were therefore excluded. Knees were then divided based on the presence or absence of a reported injury before study inclusion. Of the 2573 knees with a prior injury, 914 were excluded due to previous knee surgery, 836 because they reported at least one injury more than 20 years prior to entering the OAI, and four had missing information regarding age at the time of injury or occurrence of knee surgery. Of the 6685 knees that had no prior injury, 320 knees with previous knee surgery were excluded, and seven others with missing information regarding the occurrence of such surgery. Included in this work were 6358 knees with no prior injury (no injury) from 4038 participants (both knees 2320, one knee 1718) and 819 knees from 721 participants (both knees 98, one knee 623) with at least one reported prior injury and no surgery in the 20 years before inclusion in the OAI study. Data from study inclusion and follow-up visits, up to 96 months after inclusion, were studied.
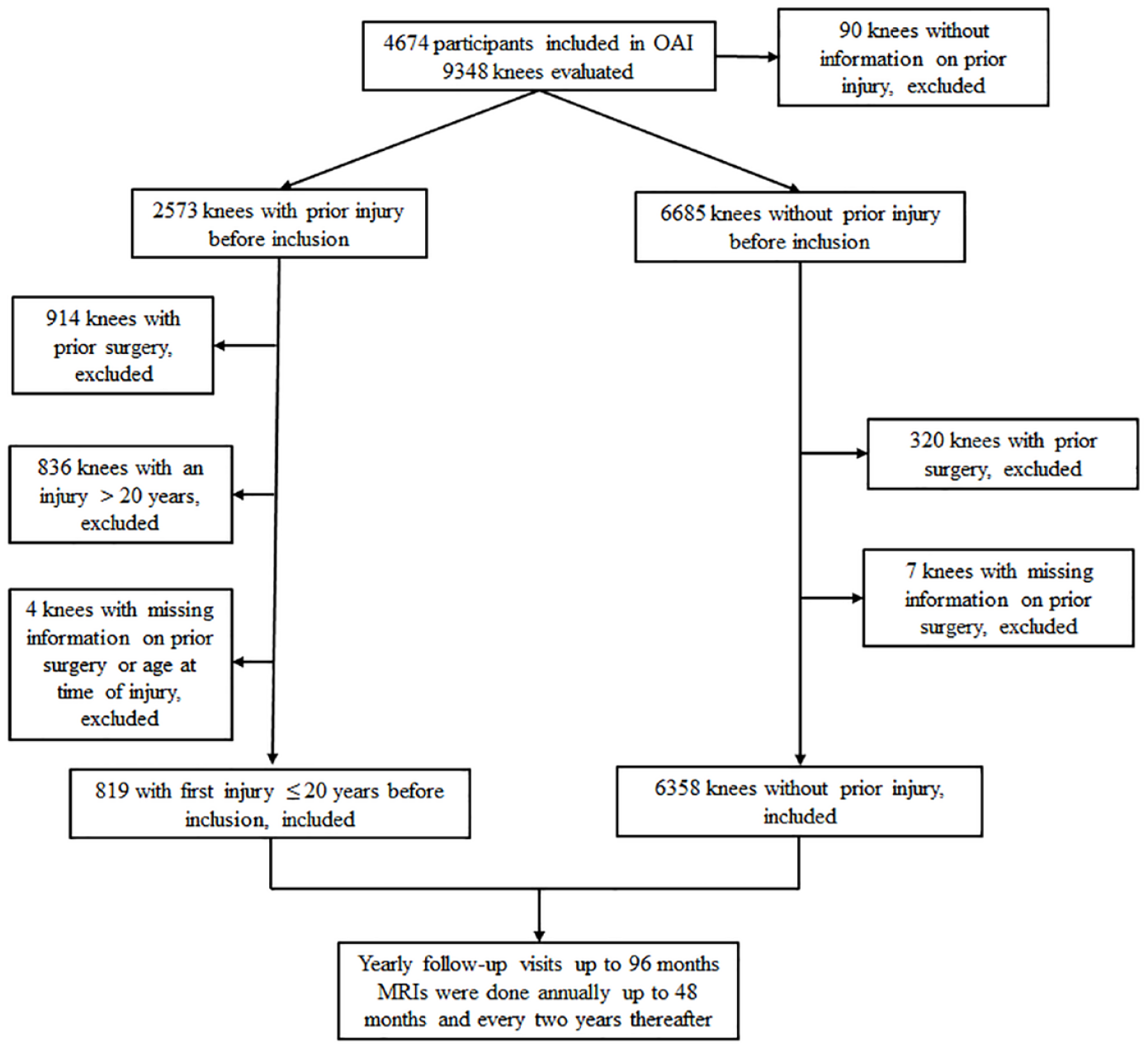
Flow chart of the study.
Variables
Sociodemographic and clinical characteristics
The sociodemographic and clinical data were from the OAI database. These included knee side, age, gender, Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores (pain, function, stiffness, total), 18 body mass index (BMI), age at first reported knee injury and physical activity scale for the elderly (PASE).
WOMAC and PASE score changes over time were calculated as the difference between the value at follow-up and the value at study inclusion.
Data sources/measurement
Injuries prior to inclusion were documented from the OAI question: Have you ever injured either of your knees so badly that it was difficult for you to walk for at least two days? If yes: How old were you when you injured your knee? The answers (yes/no) and the age at injury were recorded to calculate the duration between injury (age at study inclusion minus age at injury) and study inclusion. The occurrence of a first knee injury ⩽20 years prior to inclusion was categorized as no injury/injury, and data were analysed accordingly. The cutting point of 20 years was selected as it was felt to be recent enough for the participant to remember the event reliably.
At each visit following inclusion, participants were also asked the question: Since your last annual visit to the OAI clinic about 12 months ago, have you injured your (right/left) knee badly enough to limit your ability to walk for at least two days? Knees were further stratified based on the answer to this question (new injury/no new injury). This allowed for the assessment of the total number of injuries that occurred over time. The time of the first new injury was determined as being the annual visit, in months, at which it was first reported. The time to first new injury was thus assessed as the average of months elapsed since study inclusion in the report of a new injury.
BMI, PASE and WOMAC (pain, stiffness, function, total) scores were obtained from the OAI AllClinicalxx data sets.
Imaging characteristics
MRI acquisitions, Kellgren–Lawrence (KL) grades and joint space width (JSW) measurements were all from the OAI. MRIs were done annually up to 48 months and every 2 years thereafter.
MR images were acquired from the 3.0 T apparatus (Magnetom Trio, Siemens) at the four OAI clinical centres using a double-echo steady-state imaging protocol. KL grades and JSW measurements were from the OAI central reading (https://nda.nih.gov/oai/). Study inclusion KL grades (0–4; files: kXR_SQ_BU01) were centrally scored. Study inclusion and follow-up medial JSW (files: kxr_qjsw_duryeaxx) were blindly measured from bilateral, weight-bearing, fixed-flexion posterior–anterior knee X-rays.19,20
For the purpose of this study, we elected to use very stringent definitions to separate normal (KL = 0) from OA (KL ⩾1) knees. This is in accordance with a number of previous reports in this field.21–23
Fully automated and validated quantitative MRI technologies were used to assess the cartilage volume and the BMLs, and a validated scoring method for a meniscal extrusion. Cartilage volume was determined as previously described 24 and analysed for the global tibiofemoral (femur and plateau) knee and their respective medial and lateral compartments. BMLs were assessed 25 in the same MRI sequences as for the cartilage, quantified in each of the medial and lateral compartments of the knee, and expressed as a percentage of the lesion in the bone volume. The meniscal extrusion was defined as partial/complete meniscal extrusion at any segments of the medial or lateral meniscus 26 and reported as the percentage of knees with a medial or lateral extrusion.
Relative changes in JSW, BML and cartilage volume were calculated as the difference between the value at the time of the follow-up and the value at study inclusion, divided by the value at study inclusion. Changes in meniscal extrusion were reported as the percentage of the number of knees that developed a new extrusion over the course of the follow-up period. The time to new extrusion was determined as being the MRI visit, in months, at which it was first observed, thus being the average of months elapsed since study inclusion to the report of a new extrusion.
Knee arthroplasty was any partial or total knee replacement (V99E(R/L)KTLPR) as reported in the OAI database and previously described. 27 As the date of knee replacement (V99E(R/L)KDATE) and the number of days from study inclusion to knee arthroplasty (V99E(R/L)KDAYS) were recorded in the OAI database, it was possible to accurately calculate the average time to knee arthroplasty for all knees who had this procedure.
Study size
We studied 9348 knees from 4674 participants from the OAI (Figure 1). As reported in the ‘Participants’ section, the population included were 6358 knees with no prior injury (no injury) and 819 knees with reported first injury in the 20 years prior to enrolling into the OAI (injury). Data from study inclusion (inclusion) and follow-up visits, up to 96 months after inclusion, were studied.
Statistical analysis
Descriptive statistics, including frequencies and percentage of knees for categorical variables and measures of central tendency (means) and dispersion (standard deviations) for continuous variables, were calculated to characterize knees with and without a reported injury prior to study inclusion in the OAI.
For comparison of characteristics between injury and no injury groups and since all knees were analysed individually, to avoid potential correlations for each knee within the same subject to have an impact on the assessment of the contralateral knee, we performed a knee-based longitudinal analysis using logistic regression with repeated measures (generalized linear mixed model) to adjust for correlations between knees within-person over time and between knees, with age, gender and BMI at study inclusion as covariables.
To test the variation through time of continuous variables, a mixed model for repeated measurements (MMRM) adjusted for correlation between knees within-person was employed with the selected continuous variables at 96-month follow-up as a response; injury, follow-up and injury by follow-up as fixed factors; subject and error terms as random factors; age, gender, BMI and medial meniscal extrusion at study inclusion as covariates; as well as the selected continuous variable at study inclusion. For the categorical variables, a generalized estimating equation (GEE) adjusted for correlation between knees within-person was performed with selected categorical variables at 96-month follow-up as a response; injury, follow-up and injury by follow-up as fixed factors; subject and error terms as random factors; age, gender, BMI and medial meniscal extrusion at study inclusion as covariates; as well as the selected continuous variable at study inclusion. The within-patient covariance matrix was assumed to be unstructured.
To measure the association between the occurrence of a knee arthroplasty over time, a multivariable Cox regression analysis, with a robust sandwich covariance matrix estimated to account for correlation between knees within-person, was performed with the following variables: new meniscal extrusion (time-dependent variable), new injury (time-dependent variable), meniscal extrusion at study inclusion, injury at study inclusion, age, gender and BMI. The hazard ratio (HR) and associated 95% confidence interval (CI), as well as p-values, were calculated.
Statistical analyses were performed using SPSS (IBM SPSS Statistics 26.0, IL, USA) and SAS software, V.9.4 (SAS Institute, Cary, NC, USA). For all analyses, statistical tests were two-sided, and a p-value < 0.050 was considered significant.
Results
Demographic, clinical and imaging characteristics of knees at study inclusion
Table 1 shows that most of the 6358 knees without previous injury at study inclusion and 819 with injury in the 20 years prior to OAI enrolment were from the Incidence subcohort. The first injury, on average, occurred at 7.1 ± 6.0 years (mean ± standard deviation) before study inclusion. In both no-injury and injury groups, most participants were slightly overweight (BMI over 27 kg/m2), predominantly female, moderately active with a similar physical activity level (PASE score) and had a similar cartilage volume and BML size. Compared with the no-injury group, the injury knees were slightly younger, had a smaller JSW, more pronounced levels of symptoms (WOMAC scores), a greater number of KL grade scores 2–4 and incidence of medial meniscal extrusion.
Demographic, clinical and imaging characteristics of knees at study inclusion.

BMI, body mass index; BML, bone marrow lesion; JSW, joint space width; OAI, Osteoarthritis Initiative; PASE, Physical Activity Scale for the Elderly; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Data are mean ± standard deviation, percentage (%) or number of knees (n).
First injury occurred ⩽20 years prior to study inclusion. Knees may have one or more injuries. Knees with prior surgery were excluded.
Comparison of characteristics between injury and no injury groups was performed using a generalized linear mixed model adjusted for age, gender, BMI at study inclusion and for correlation between knees within-person.
Number of knees studied in the group.
Calculated as difference (in years) between age at study inclusion and age at first injury.
WOMAC questionnaire was self-administered: higher WOMAC scores indicate more symptoms and greater functional impairment.
Meniscal extrusion scored as absence or presence of a partial or complete extrusion in any of the three segments of medial or lateral meniscus.
The p-values in bold indicate statistical significance (p < 0.050).
Based on the number of injuries encountered before inclusion in the study and identified from the participant questionnaire, the majority of knees (90%) had only one injury, and the others (more than one), except for a few, had only two or three injuries (Supplemental Table S1). The group having suffered less than one injury showed a longer time period from the first injury to inclusion, a higher WOMAC pain score and a greater cartilage volume in both medial and lateral compartments, which reached statistical differences in the latter.
In knees with osteoarthritis (KL 1–4) at study inclusion (Table 2), the injury group showed higher WOMAC scores, percentage of knees with more severe KL (2–4) grades and incidence of medial meniscal extrusion, a slightly smaller JSW and a lower cartilage volume in the medial compartment.
Demographic, clinical and imaging characteristics of knees with osteoarthritis a at study inclusion.

BMI, body mass index; BML, bone marrow lesion; JSW, joint space width; OAI, Osteoarthritis Initiative; PASE, Physical Activity Scale for the Elderly; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Data are mean ± standard deviation, percentage (%), or number (n) of knees.
Knee osteoarthritis: knees with KL 1–4.
First injury occurred ⩽20 years prior to study inclusion. Knees may have one or more injuries. Knees with prior surgery were excluded.
Comparison of characteristics between injury and no injury groups was performed using a generalized linear mixed model adjusted for age, gender, BMI at study inclusion and for correlation between knees within-person.
Number of knees studied in the group.
Calculated as difference (in years) between age at study inclusion and age at first injury.
WOMAC questionnaire was self-administered: higher WOMAC scores indicate more symptoms and greater functional impairment.
Meniscal extrusion: scored as absence or presence of a partial or complete extrusion in any of the three segments of medial or lateral meniscus.
The p-values in bold indicate statistical significance (p < 0.050).
As expected in knees with no osteoarthritis (KL = 0; Supplemental Table S2), the injury group showed mild WOMAC scores but significantly more pronounced than the non-injury group, and knees had a minimal increase in cartilage volume in the lateral compartment.
Changes at 96 months in clinical and imaging characteristics
The main findings for the changes at 96 months were that the injury group (injury prior to study inclusion) had a worsening of the WOMAC scores and, in the medial compartment, a greater loss in JSW and cartilage volume, an increase in the incidence of meniscal extrusion and BML size (Table 3; results of changes at other times over the follow-up are presented in Supplemental Table S3).
Changes at 96 months in clinical and imaging characteristics according to history of knee injury before study inclusion.

BMI, body mass index; BML, bone marrow lesion; JSW, joint space width; PASE, Physical Activity Scale for the Elderly; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Data are mean ± standard deviation and percentage (%) in each group; n, number of knees.
Δ: difference between value at 96 months and study inclusion value.
Δ%: relative difference (Δ divided by study inclusion value).
First injury occurred ⩽20 years prior to study inclusion. Knees may have one or more injuries. Knees with prior surgery were excluded.
The p-values were calculated from mixed model for repeated measurements (MMRM) adjusted for correlation between knees within-person with selected continuous variable at 96-month follow-up as response, injury, follow-up and injury by follow-up as fixed factors, subject and error terms as random factors, and age, gender, BMI and medial meniscal extrusion at study inclusion as covariates, as well as the selected continuous variable at study inclusion. For meniscal extrusion, p-values were calculated from generalized estimating equation (GEE) adjusted for correlation between knees within-person with selected categorical variable at 96-month follow-up as response, injury, follow-up and injury by follow-up as fixed factors, subject and error terms as random factors, and age, gender, BMI and medial meniscal extrusion at study inclusion as covariates as well as the meniscal extrusion at study inclusion.
Number of knees studied in the group.
WOMAC questionnaire was self-administered: higher WOMAC scores indicate more symptoms and greater functional impairment.
New meniscal extrusion after study inclusion. Meniscal extrusion: scored as absence or presence of partial or complete extrusion in any of the three segments of the medial or lateral meniscus.
The p-values in bold indicate statistical significance (p < 0.050).
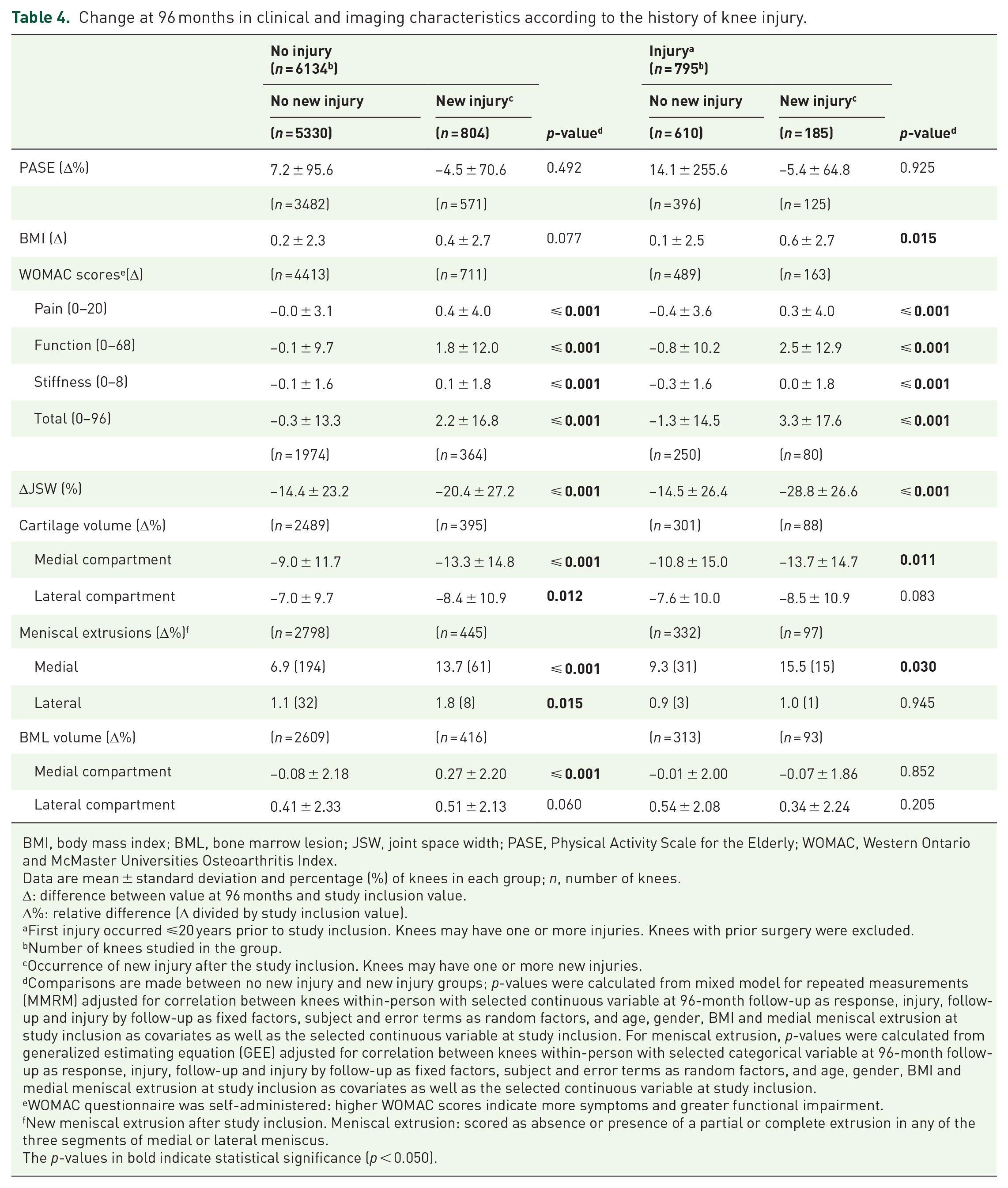
The changes at 96 months were further analysed to identify and discriminate the role of injury on osteoarthritis outcomes based on whether the injury was encountered before (no injury and injury) and after (no new injury and new injury) inclusion into the study (Table 4 and Supplemental Table S4). On average, the first new knee injury occurred at 50.0 ± 27.8 months after study inclusion. Notably, the percentage of knees with new injury in the injury group (23%) was about double compared with the no-injury group (13%). The occurrence of new injuries between visits and within each group was in a similar range (new injury 24–48 months, 218; 48–72 months, 182; and 72–96 months, 175) and injury group (new injury 24–48 months, 40; 48–72 months, 44; and 72–96 months, 29; Supplemental Table S4). In knees that had no injury before study inclusion, those experiencing a new injury after inclusion had a greater increase in WOMAC scores, loss of JSW, medial BML size and loss of cartilage volume and incidence of meniscal extrusion in both compartments. These changes were progressive over time for the finding regarding the loss of JSW and cartilage volume and incidence of meniscal extrusion in the medial compartment. In knees with injury at study inclusion, those who experienced a new injury had similar findings as those found in the no injury group, with the exception of an increase in BMI, and no differences were found in some of the structural alterations, including the loss of cartilage volume and the incidence of meniscal extrusion in the lateral compartment, and BML size in the medial compartment. Of note, a meniscal extrusion in the lateral compartment was found only in a few knees.
Change at 96 months in clinical and imaging characteristics according to the history of knee injury.
BMI, body mass index; BML, bone marrow lesion; JSW, joint space width; PASE, Physical Activity Scale for the Elderly; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Data are mean ± standard deviation and percentage (%) of knees in each group; n, number of knees.
Δ: difference between value at 96 months and study inclusion value.
Δ%: relative difference (Δ divided by study inclusion value).
First injury occurred ⩽20 years prior to study inclusion. Knees may have one or more injuries. Knees with prior surgery were excluded.
Number of knees studied in the group.
Occurrence of new injury after the study inclusion. Knees may have one or more new injuries.
Comparisons are made between no new injury and new injury groups; p-values were calculated from mixed model for repeated measurements (MMRM) adjusted for correlation between knees within-person with selected continuous variable at 96-month follow-up as response, injury, follow-up and injury by follow-up as fixed factors, subject and error terms as random factors, and age, gender, BMI and medial meniscal extrusion at study inclusion as covariates as well as the selected continuous variable at study inclusion. For meniscal extrusion, p-values were calculated from generalized estimating equation (GEE) adjusted for correlation between knees within-person with selected categorical variable at 96-month follow-up as response, injury, follow-up and injury by follow-up as fixed factors, subject and error terms as random factors, and age, gender, BMI and medial meniscal extrusion at study inclusion as covariates as well as the selected continuous variable at study inclusion.
WOMAC questionnaire was self-administered: higher WOMAC scores indicate more symptoms and greater functional impairment.
New meniscal extrusion after study inclusion. Meniscal extrusion: scored as absence or presence of a partial or complete extrusion in any of the three segments of medial or lateral meniscus.
The p-values in bold indicate statistical significance (p < 0.050).
In addition, comparisons were also carried out according to the number of new injuries (one and more than one), and analyses were made on knees for whom that information was available for all time points. Data showed that a small number of knees that had a new injury experienced more than one injury over the years (Supplemental Table S5). For those, most of the knees experienced two to three injuries. Knees with multiple new injuries (more than one) but no injury at study inclusion experienced an increase in the incidence of medial meniscal extrusion. A worsening of symptoms (all WOMAC subscores) was found for knees with and without injury at study inclusion.
Risk factors associated with the occurrence of knee arthroplasty
Knee arthroplasty occurred at an average of 61 months after study inclusion, which is similar whether knees experienced an injury before or after study inclusion (Supplemental Table S6). Data showed that knees with or without a previous injury at study inclusion and with no new one at 96 months had a low incidence of knee arthroplasty (about 3–4%). However, for both no-injury and injury groups, for those who suffered a new injury, the incidence of knee arthroplasty was increased by about 2.7 times compared with those without new injury (10.6% compared with 3.9%).
The impact of several independent risk factors (at study inclusion and during follow-up) on the occurrence of a knee arthroplasty over time was further studied. Data demonstrated (Table 5) that new meniscal extrusion and new injury had the highest HRs, followed by the presence of meniscal extrusion at study inclusion, age and BMI (all p ⩽ 0.001).
Independent risk factors associated with the occurrence of knee arthroplasty. a

BMI, body mass index, CI, confidence interval; HR, hazard ratio.
Occurrence of a knee arthroplasty at any time after study inclusion (see Supplemental Table S6).
Multivariable Cox regression model with a robust sandwich covariance matrix estimate to account for correlation between knees.
New meniscal extrusion after study inclusion. Meniscal extrusion: scored as absence or presence of a partial or complete extrusion in any of the three segments of medial or lateral meniscus.
Occurrence of one or more new injury at any time after study inclusion.
First injury occurred ⩽20 years prior to study inclusion. Knees may have one or more injuries. Knees with prior surgery were excluded.
The p-values in bold indicate statistical significance (p < 0.050).
Discussion
This cohort study extends on a previous report 28 in providing new information from an older population about the role of knee injury as a risk factor for osteoarthritis incidence and progression over a prolonged period. This study also aimed at documenting knee structural changes that can predict a major osteoarthritis hard outcome, knee arthroplasty, to classify these patients for tailoring decisions and treatments, thus improving their quality of life.
Our data showed that knees that experienced a nonsurgical injury in years (± 20) prior to study inclusion, about 7 years on average, had an increased incidence and severity of knee osteoarthritis development, including greater symptoms and structural changes. Moreover, a new injury after inclusion was demonstrated to be a major factor favouring osteoarthritis development at both symptomatic and structural levels, as well as being among the most important independent risk factors for knee arthroplasty. Importantly, those changes were found to be more severe in knees having repeated new injuries.
Structural changes in the knee having an injury before study inclusion had a higher incidence level of medial meniscal extrusion, cartilage volume loss, and BMLs providing, among others, an explanation of how an injury could be linked to knee osteoarthritis.
One of the study’s aims was to explore whether a past injury could be an independent predictive risk factor for osteoarthritis incidence and progression. We restricted to events that occurred within 20 years prior to inclusion to ensure reliable information. An individual remembering having a knee injury before such a period would have been challenging and could have compromised the findings. Moreover, knees that had surgery due to injuries were excluded, and information is available in the literature regarding their association with osteoarthritis.29–33
This work showed that knees experiencing a nonsurgical injury(ies) in the 20 years prior to inclusion definitively had a greater incidence of radiological osteoarthritis (KL score ⩾1), which were of a more severe grade (higher score), a finding in line with the smaller JSW and a smaller cartilage volume in the medial compartment seen in that group. Moreover, as reported, these knees also had an increased incidence of medial meniscal extrusion, which could be responsible for greater disease severity and symptoms. 34
The role played by an injury occurring after study inclusion, a new injury, was also an important question that needed to be explored. To this end, the cohort was followed for 96 months after study inception, allowing for a longitudinal appreciation of the clinical and structural changes over time. Knees with a history of injury at study inclusion presented over time a greater increase in the severity of both symptoms and structural changes and, more specifically for the latter, in the medial compartment. More severe structural alterations in the medial compartment were expected and supported the notion that this compartment is within the first to be altered in older adult osteoarthritis patients.35,36 Moreover, new knee injury(ies) exacerbated the extent of symptoms and structural changes. Hence, knees with no injury at inclusion but experiencing new injuries showed higher osteoarthritis structural alterations in both medial and lateral meniscal extrusion and cartilage volume loss, as well as an increased medial BML size. These data concur with studies reporting that a medial meniscal lesion is a strong risk factor for the occurrence of lateral lesions,37,38 in addition to those reporting that meniscal extrusion and BML predict incident and progressive knee osteoarthritis.26,28,39–41 The increased BML size may have been a direct consequence of a bone injury, a meniscal extrusion and a possible rupture of the anterior cruciate ligament.42–45 Of note, knees with a history of injury at inclusion showed an increase in BMI and meniscal extrusion incidence and cartilage volume loss only in the medial compartment. The increased BML size in the medial compartment in the group having no injury at inclusion but with new injury on knees over time extends on previous observations. 28 It could explain, at least in part, a link with a knee arthroplasty through a more pronounced worsening in disease symptoms and loss of cartilage, which are both known to be associated with BML.28,46 The increase in BMI may have been an additional contributing factor to an increased risk for a worse disease outcome in these participants. Globally, these findings strongly suggest that the occurrence of new injury is a strong risk factor for inducing osteoarthritis and exacerbating a pre-existing osteoarthritic condition in those with a prior injury, which will negatively impact the disease outcome.
Another important question was to explore whether the number of injuries could have influenced the above findings. Data indicate that repeated new injuries are a greater risk than a single new injury for worsening of osteoarthritic symptoms and progression of structural damage, as demonstrated by a higher loss of JSW and greater incidence of meniscal extrusions. As noted in the ‘Results’ section, the number of knees showing lateral meniscal extrusions is small; therefore, caution should be exercised in interpreting these data. These findings on new injuries contrast with those regarding the impact of injury encountered before study inclusion. The difference could be ascribed to having a better accuracy of the collected information in this study and the fact, as mentioned in the text, that knees with surgery were excluded from the study cohort and could have been more prone to experience multiple injuries.
New meniscal extrusion followed by a new injury and meniscal extrusion at study inclusion were the strongest independent risk factors for knee arthroplasty. This finding concurs with the data that about twice as many meniscal extrusions were found in knees with a new injury, particularly in those experiencing multiple new injuries. However, as the number of knees having meniscal extrusion, particularly in the lateral compartment, was low, it prevented us from evaluating their impact on knee arthroplasty. Although of moderate importance but reaching statistical significance, age and BMI were also associated with knee arthroplasty supporting and expanding previous reports.1,13
The findings of this study are new as it relates to knee injuries in an older adult population, are not associated with a sports injury and are obviously part of real-life events in a population at risk of or with knee osteoarthritis. Moreover, data of repeated new injury being associated with greater worsening in severity of symptoms and structural modifications have, to our knowledge, not been reported previously in such a cohort, even in cases of accelerated knee osteoarthritis. 10 The use of MRI data, in which the exams were conducted at regular intervals during the follow-up, strengthened this work, as this methodology is very sensitive to knee structural alterations and their changes, which could be detected before other imaging-based technologies. 47
Data from this work bring into perspective and reinforce the important role that prevention could play in reducing the risk of subsequent knee osteoarthritis. Not forgetting that in some cases, a single knee injury could be a risk factor for the development of accelerated knee osteoarthritis, an aggressive form of rapidly progressive and destructive knee osteoarthritis. 10 In addition, data will be beneficial in clinical practice, as they will assist in identifying individuals at greater risk of a significant disease progression and worst disease outcome. Thus, any condition that has a destabilizing effect on the knee, such as meniscal tear/extrusion, malalignment and overweight, to name a few, need to be managed accordingly.
We acknowledge that there are limitations. As our primary variable was the history of a knee injury associated with an increased risk for osteoarthritis, one could, at first sight, believe that it was already studied. Previous studies8,9,48 may have overestimated this relationship as people with symptomatic osteoarthritis may more likely remember a past injury or interpret early osteoarthritic symptoms as indicative of a past joint injury.
Another potential limitation is assessing the time of injury as probed per the participant’s questionnaire. The longer the duration from time to injury to study inception, especially if an intraarticular surgical procedure had been done, could have impacted (positively or negatively) its association with future knee osteoarthritic symptoms and damage. However, we felt that no skewness was expected, as participants with a surgical procedure associated with such trauma and those with an injury beyond 20 years were excluded.
In addition, the type of injury, and not simply its occurrence, could have been a factor impacting the probability of osteoarthritis incidence and progression and is relevant information that is not captured by the questionnaire. Such information, especially injury implying shear force, might have been very informative as they have been demonstrated to yield an osteoarthritis phenotype labelled as ‘mechano-inflammatory’, which is prone to more cartilage damage versus a pure compressive force which in contrast is promoting its repair. 49
Additional structural changes that can be associated with injury, such as synovitis, joint malalignment and instability, were not investigated in this study and may have been possible additional contributing factors.28,50–53
A limitation of the OAI database resides in the lack of information on the disease duration. It was, therefore, impossible to predict the time between injury occurrence and subsequent knee osteoarthritic symptoms/radiological onset nor to identify confounding factors that may influence the rate of post-traumatic osteoarthritis appearance.
Per the study design, we defined the progression of osteoarthritis using continuous variables (symptoms and structure) modifications over time and not predetermined cut-offs such as using plain radiography and KL grade changes as already reported.48,54 Although the absence of a cut-off may make the clinical relevance of the structural progression of osteoarthritis more challenging to interpret, such a design was mainly done to gain statistical power. However, it is agreed that any osteoarthritic clinical and structural progression factors over a long period of time are most likely deleterious. In contrast, we have chosen a ‘hard’ outcome, knee arthroplasty, in which data support all our findings except the injury history prior to study inclusion, which could have been due to statistical power. Moreover, the chosen outcome also raises its limitation since the need for surgery is a known issue concerning procedure indication and access, such as socioeconomic, comorbidities and patient preferences, to name a few.
Medication usage (analgesics, NSAIDs, intraarticular injections of steroids and hyaluronan) was excluded in this study, recognizing that such may confound knee symptom intensity upon database entry and change over time. Unfortunately, the OAI database does not permit which treatment, if any, was provided at the time and after the injury, which in turn may potentially mitigate the incidence and progression of osteoarthritis over time. However, as we have already explored the effect of medication on knee OA progression/knee replacement through two large case–control studies27,28 and since no causal relationship was found, such information was not deemed to be relevant in this study.
Finally, our study was performed on a single longitudinal cohort, the OAI, using individuals from the United States. The inclusion of participants for the studied (Progression and Incident) subcohorts was based on the probability that osteoarthritis may occur over time according to specific risk factors. This may not entirely mirror what is expected from the general osteoarthritis population, for instance, in other countries, and thus may impact the generalizability of our results. Other similar analyses performed on different data sets from another country yielding similar results would further enhance the confidence of our findings.
Conclusion
In summary, this study provides new findings in support of nonsurgical knee injury in an older population being associated with the incidence/progression of this chronic degenerative disease – knee osteoarthritis and the occurrence and increased risk of knee arthroplasty. The meniscal extrusions, and more particularly new ones, and new injuries were found to be highly associated and independent risk factors for the incidence of knee arthroplasty, as well as recent and repeat injury being of great consequence for more severe osteoarthritis symptoms and structural damages. Also associated with new injury was an increase in BML size, a factor known to intensify the severity of disease symptoms and disease progression, which are key factors for a worse disease prognosis. Our findings are clinically relevant and support the role of prevention to counteract or reduce the occurrence of post-traumatic knee osteoarthritis harmful events, a condition known to reduce the quality of life in older adults. Moreover, these data introduce a novel source of decision support in precision medicine that will help to improve the identification of individuals at greater risk of significant disease progression and worst disease outcome for a customized treatment plan.
Supplemental Material
sj-docx-1-taj-10.1177_20406223231169715 – Supplemental material for Risk factors for the long-term incidence and progression of knee osteoarthritis in older adults: role of nonsurgical injury
Supplemental material, sj-docx-1-taj-10.1177_20406223231169715 for Risk factors for the long-term incidence and progression of knee osteoarthritis in older adults: role of nonsurgical injury by Jean-Pierre Pelletier, Patrice Paiement, Marc Dorais, Jean-Pierre Raynauld and Johanne Martel-Pelletier in Therapeutic Advances in Chronic Disease
Footnotes
Acknowledgements
The authors would like to thank the Osteoarthritis Initiative (OAI) participants and the Coordinating Center for generating the OAI cohort’s clinical and radiological data and making them publicly available. The OAI is a public–private partnership comprised of five contracts (N01-AR-2-2258; N01-AR-2-2259; N01-AR-2-2260; N01-AR-2-2261; N01-AR-2-2262) funded by the National Institutes of Health, a branch of the Department of Health and Human Services, and conducted by the OAI Study Investigators. Private funding partners include Merck Research Laboratories; Novartis Pharmaceuticals Corporation, GlaxoSmithKline; and Pfizer, Inc. Private sector funding for the OAI is managed by the National Institutes of Health Foundation. This manuscript was prepared using an OAI public use data set and does not necessarily reflect the opinions or views of the OAI investigators, the NIH or the private funding partners. None of the authors are part of the OAI investigator team. A special thanks to ArthroLab Inc., Montreal, Canada, for providing the magnetic resonance imaging data, and to Santa Fiori for preparing the manuscript.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.